
Abstract
Background
No prior meta-analysis has directly compared restenosis or revision rates between Draf IIb and Draf III in chronic rhinosinusitis (CRS) or evaluated how Type 2 versus non-Type 2 endotypes influence these outcomes.
Methods
Following PRISMA guidelines, PubMed, MEDLINE, Embase, and ClinicalTrials.gov were searched on 5 January 2025 for studies reporting restenosis or revision after Draf IIb or Draf III in adults with CRS. Random-effects meta-analyses of proportions (Freeman–Tukey transformation; Hartung–Knapp CIs), pooled restenosis and revision rates, with subgroup analyses by procedure type and endotype.
Results
Thirty-eight studies met inclusion criteria (restenosis n = 1550; revision n = 1305). The pooled restenosis proportion across procedures was 9% (95% CI: 5-14%) and the pooled revision proportion was 9% (95% CI: 5-13%). Restenosis was lower after Draf IIb than Draf III (0.8% vs. 12%), with revision rates showing a similar pattern (2% vs. 10%). Type 2 CRS demonstrated higher pooled rates of restenosis (8% vs. 1%) and revision (12% vs. 3%) compared with non-Type 2 CRS.
Conclusions
Draf IIb is associated with lower pooled restenosis and revision rates than Draf III in CRS. Type 2 inflammatory endotype confers substantially higher risk of adverse frontal sinus outcomes. Incorporating endotype into procedural decision-making may improve prognosis. Prospective, endotype-stratified studies are needed to refine indications for Draf IIb versus Draf III and optimize adjunctive management strategies.
Keywords
Introduction
Management of chronic frontal rhinosinusitis poses (CRS) significant challenges, as the frontal recess is narrow and anatomically variable, limiting surgical access and complicating postoperative care.1–5 Although intranasal corticosteroids, saline irrigations, and systemic therapies remain the first-line treatment, many patients ultimately require surgery to re-establish frontal sinus drainage.6,7
The Draf classification describes progressively extensive approaches for frontal sinus disease. Draf IIb enlarges the frontal ostium unilaterally between the lamina papyracea and nasal septum, while Draf III (endoscopic modified Lothrop procedure [EMLP]) creates a common drainage pathway by resecting the frontal sinus floor bilaterally with parts of the nasal and frontal septum.8–10 Despite surgical advancements, postoperative restenosis, neo-ostium scarring, and mucocele formation remain common causes of surgical failure, often requiring revision procedures.11–13
In addition to surgical factors, recent evidence highlights the role of immunologic endotypes in CRS pathophysiology. Type 2-driven inflammation, characterized by tissue eosinophilia and cytokine pathways including IL-4, IL-5, and IL-13, has been associated with higher recurrence rates and less favorable surgical outcomes than non-Type 2 disease.14–16 However, there is limited data directly comparing outcomes of Draf IIb and Draf III in CRS stratified by endotype.
Previous reviews, such as Hirayama et al., 17 have examined frontal sinus surgery broadly; however, no meta-analysis has specifically evaluated whether surgical extent and underlying inflammatory endotype interact to influence prognosis in CRS. The objective of this systematic review and meta-analysis was therefore to compare outcomes of Draf IIb and Draf III in CRS, focusing on restenosis and revision rates, and to assess whether surgical success differs between Type 2 and non-Type 2 disease.
Materials and Methods
Study Design and Registration
In accordance with PRISMA 2020 guidelines, a comprehensive literature search was conducted on 5 January 2025. The study protocol was prospectively registered in PROSPERO (ID 632674). 18 An information specialist librarian contributed to the development of the search strategy, including Medical Subject Headings (MeSH) and database-specific indexing terms.
Population, Comparison, Intervention, Outcome (PICO)
We included studies involving adult patients diagnosed with chronic rhinosinusitis (CRS) undergoing Draf IIb or Draf III procedures. The primary outcomes were frontal sinus restenosis and the need for revision surgery. Eligible study designs included randomized controlled trials, cohort studies, and case series; all primary research relevant to the PICO criteria was included. Studies were excluded if Draf IIb or Draf III procedures were performed for indications other than CRS, or if they were conference abstracts, commentaries, animal studies, lacked full-text access, or did not clearly report CRS patient numbers.
Information Sources and Search Strategy
A comprehensive search strategy was developed using standardized keywords and appropriate Boolean operators (Appendix A). Searches were conducted in PubMed, the Cochrane Library, AMED, Embase, CINAHL, and MEDLINE via Ovid from database inception to 5 January 2025. Only studies published in English were included. Grey literature sources such as ClinicalTrials.gov and WHO ICTRP were not searched.
Data Screening and Extraction
Four authors (Y.H., D.L., M.S., and N.N.) independently conducted study selection according to the predefined eligibility criteria. Screening occurred in two stages: an initial review of titles and abstracts, followed by full-text assessment. Reference lists of eligible studies were also screened to identify additional relevant publications. Any disagreements were resolved through discussion. Screening was managed using Google Sheets.
Data extraction was performed by two authors (D.L. and N.N.) using a standardized data extraction form. Extracted variables included study characteristics (author, year, design), patient demographics, intervention details (procedure type, comparator, follow-up duration), reported outcomes, study limitations, and conflicts of interest. When studies reported CRS patient proportions without corresponding subgroup outcome data, corresponding authors were contacted for clarification.
Endotype data—proportions of patients with Type 2 and non-Type 2 CRS, classified according to EPOS 2020 19 were extracted when available. When not explicitly provided, Type 2 endotype classification was inferred based on clinical surrogates defined by EPOS 2020 (eg, studies exclusively evaluating CRSwNP). Where explicit labels were absent from summary tables, endotype-specific data was isolated via full-text review, deduction of population subsets from explicitly defined complementary groups, and back-calculation of raw patient numbers from reported percentages. Studies lacking sufficient context to confidently separate endotype-specific data were excluded from this analysis.
Risk of Bias Assessment
Our review included studies with different designs, which required the use of multiple quality assessment tools. Risk of bias was carried out independently by Y.H., N.N. and D.L. Risk of bias was independently evaluated by Y.H., N.N., and D.L. using the JBI case series checklist, as it provides the most appropriate framework for assessing uncontrolled study designs. 20
Statistical Analysis
We performed meta-analyses of proportions using a random-effects approach, applying the Freeman–Tukey double-arcsine transformation to accommodate proportions near 0 or 1, with pooled estimates back-transformed to the original scale. Confidence intervals (CIs) for the summary effect were computed using the Hartung–Knapp method.
Between-study variance was estimated using the DerSimonian–Laird method, and heterogeneity was quantified using the I2 and H statistics. Subgroup meta-analyses were fitted without assuming a common between-study variance, and differences were assessed using between-subgroup Q-tests.
To assess small-study effects and potential publication bias for revision surgery and restenosis, we constructed DOI plots and calculated the Luis Furuya-Kanamori (LFK) index. Absolute LFK values within ±1 were interpreted as no asymmetry, values between ±1 and ±2 as minor asymmetry, and values > ± 2 as major asymmetry. All analyses were conducted in R version 4.4.0 (R Foundation for Statistical Computing) using the meta, metafor, and metadat packages. Results are reported as pooled proportions with 95% CIs, with two-sided p < .05 considered statistically significant.
Results
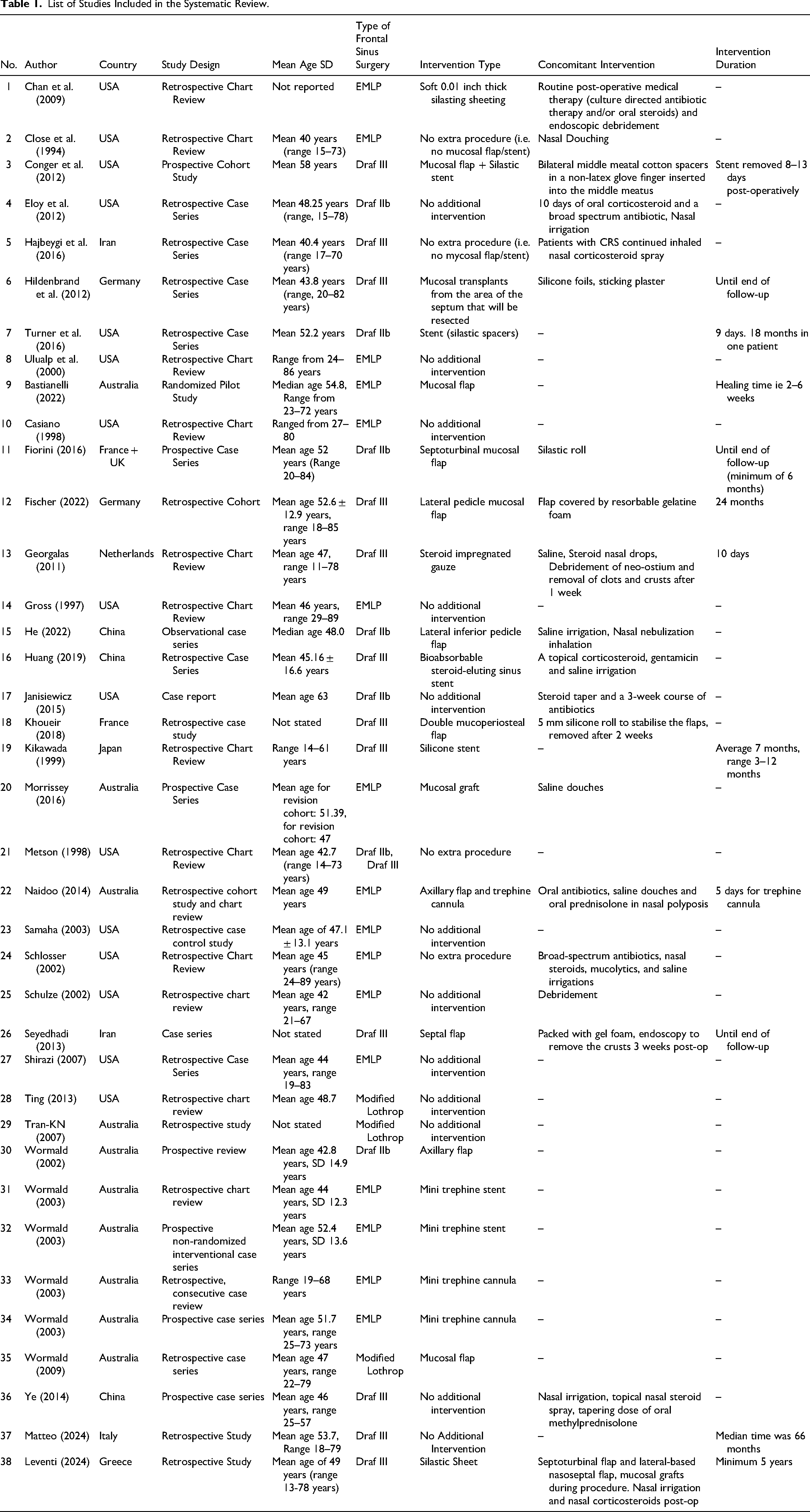
A total of 172 studies were identified through database searches and reference screening (Figure 1). Following abstract screening for PICO relevance, 98 studies were assessed for full-text review. 60 studies were excluded because the interventions did not involve Draf procedures CRS patients as population or relevant outcomes were not reported (Table A1). This resulted in 38 studies that fulfilled the eligibility criteria and were considered in the final systematic review and meta-analysis (Table 1).
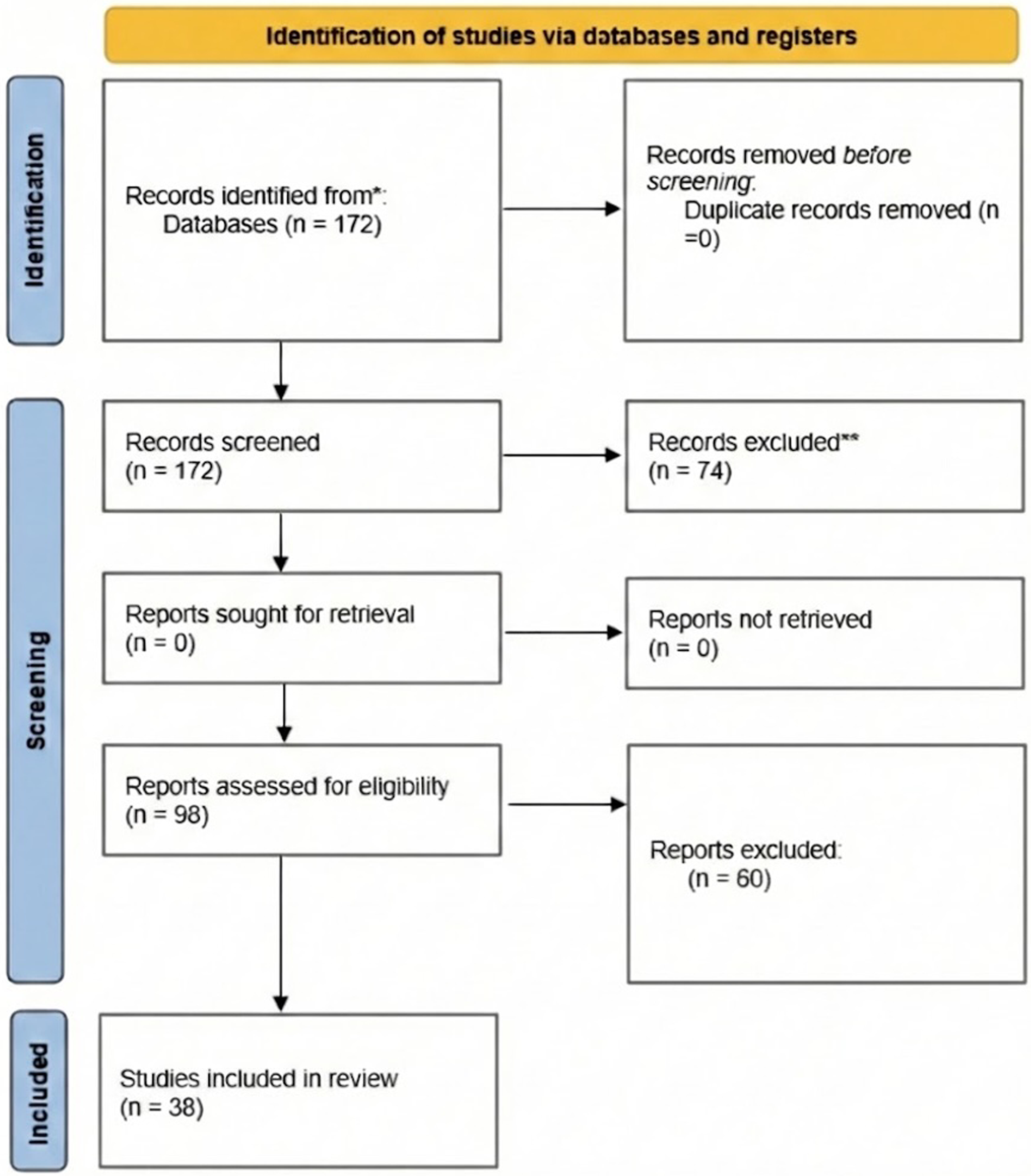
PRISMA flow diagram.
List of Studies Included in the Systematic Review.
Pooled Analysis
Restenosis
A total of 36 studies reporting restenosis outcomes following Draf IIb or Draf III procedures were included in the analysis.11,21–55 Across these studies, 1550 patients were evaluated, of whom 207 developed restenosis. The pooled weighted proportion of restenosis across Draf IIb and Draf III procedures was 0.09 (9%) (95% CI: 0.05-0.14), with substantial heterogeneity (I2 = 79.2%) and an overall effect p < .001. A prediction interval ranged from 0% to 38% (Supplementary Figure S7). The LFK index for the overall analysis was 0.26, indicating no evidence of asymmetry (Supplementary Figure S1).
Revision Procedures
Revision outcomes were reported in 30 studies, encompassing a total of 1305 patients who had undergone Draf IIb or Draf III procedures. Of these, 164 patients required revision surgery. When data from both procedure types were pooled, the weighted revision proportion was 0.09 (9%) (95% CI: 0.05-0.13). Considerable between-study variability was observed (I2 = 70.4%), and the overall effect was statistically significant (p < .001). The prediction interval ranged from 0% to 32% (Supplementary Figure 8). The LFK index for the overall revision analysis was 0.09, indicating no evidence of asymmetry (Supplementary Figure 2).
Draf IIb Versus Draf III
Restenosis
To evaluate outcomes by procedure type, studies were analyzed separately for Draf IIb and Draf III. In the Draf IIb subgroup (6 studies), only 3 cases of restenosis were reported among 121 patients, whereas the Draf III subgroup (30 studies) reported 204 cases among 1434 patients. The pooled restenosis proportion was 0.008 (0.8%) (95% CI: 0.00-0.10) for Draf IIb and 0.12 (12%) (95% CI: 0.07-0.17) for Draf III. Heterogeneity was moderate among Draf IIb studies (I2 = 42.1%) and high among Draf III studies (I2 = 79.4%). The subgroup difference was statistically significant (p < 0.049) (Figure 2). The LFK index for the Draf IIb subgroup was 3.82, indicating major asymmetry, whereas the Draf III subgroup had an LFK index of 0.19, indicating no evidence of asymmetry (Supplementary Figures 3 and 4).
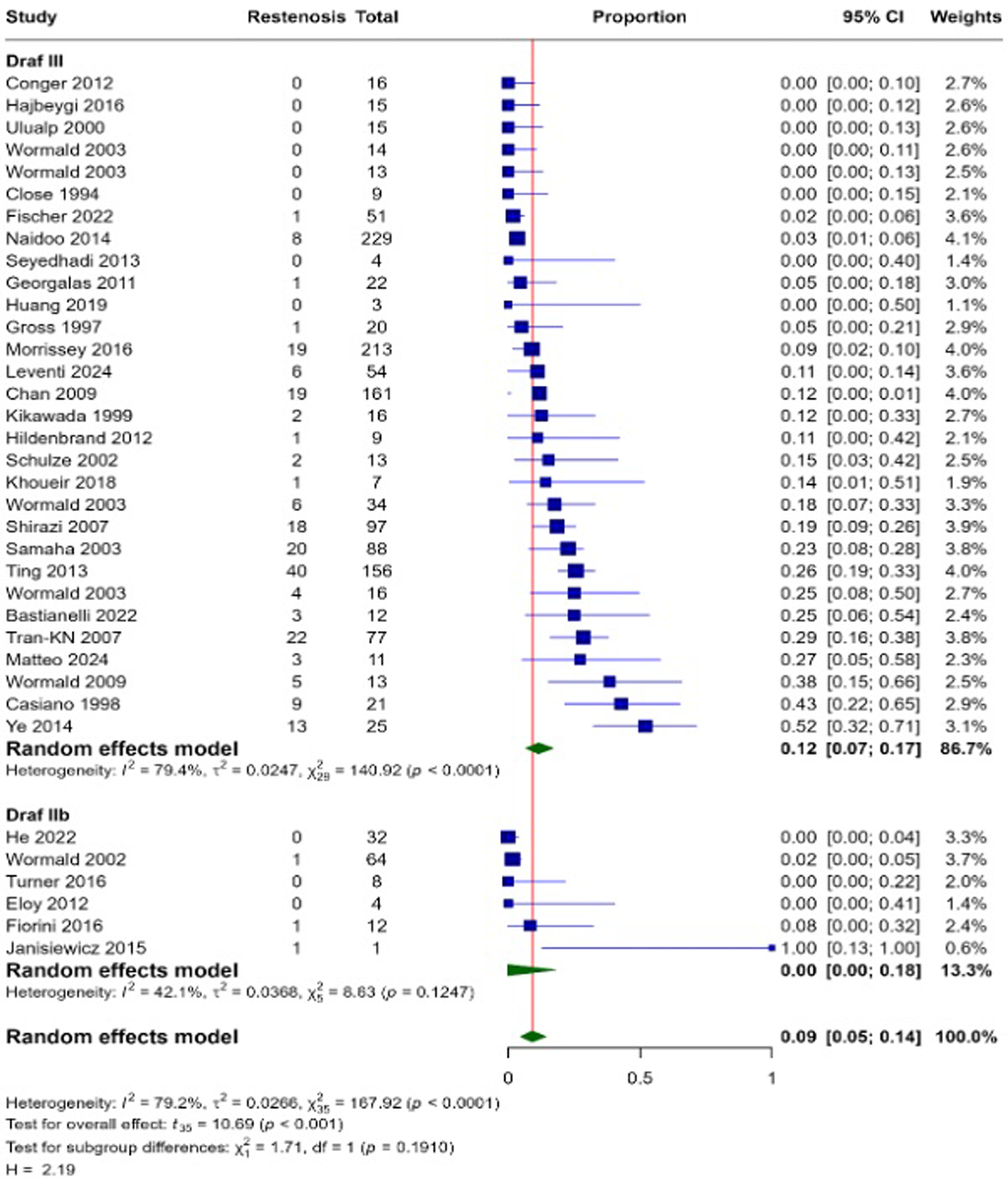
Proportional meta-analysis of restenosis outcomes comparing Draf IIb and Draf III across single-arm studies.
Revision Surgery
Revision outcomes were reported in four studies for Draf IIb and 26 studies for Draf III. The Draf IIb subgroup included 112 patients, of whom four required revision surgery, whereas the Draf III subgroup comprised 1193 patients with 158 revisions. The pooled revision proportion was lower for Draf IIb at 0.02 (2%) (95% CI: 0.00-0.09) compared with 0.10 (10%) (95% CI: 0.05-0.15) for Draf III. Heterogeneity was absent among Draf IIb studies (I2 = 0%) but substantial among Draf III studies (I2 = 75.6%). The subgroup difference did not reach statistical significance (p = .050) (Figure 3). The LFK index for the Draf IIb subgroup was 1.51, indicating minor asymmetry, whereas the Draf III subgroup had an LFK index of 0.28, indicating no evidence of asymmetry (Supplementary Figures 5 and 6).
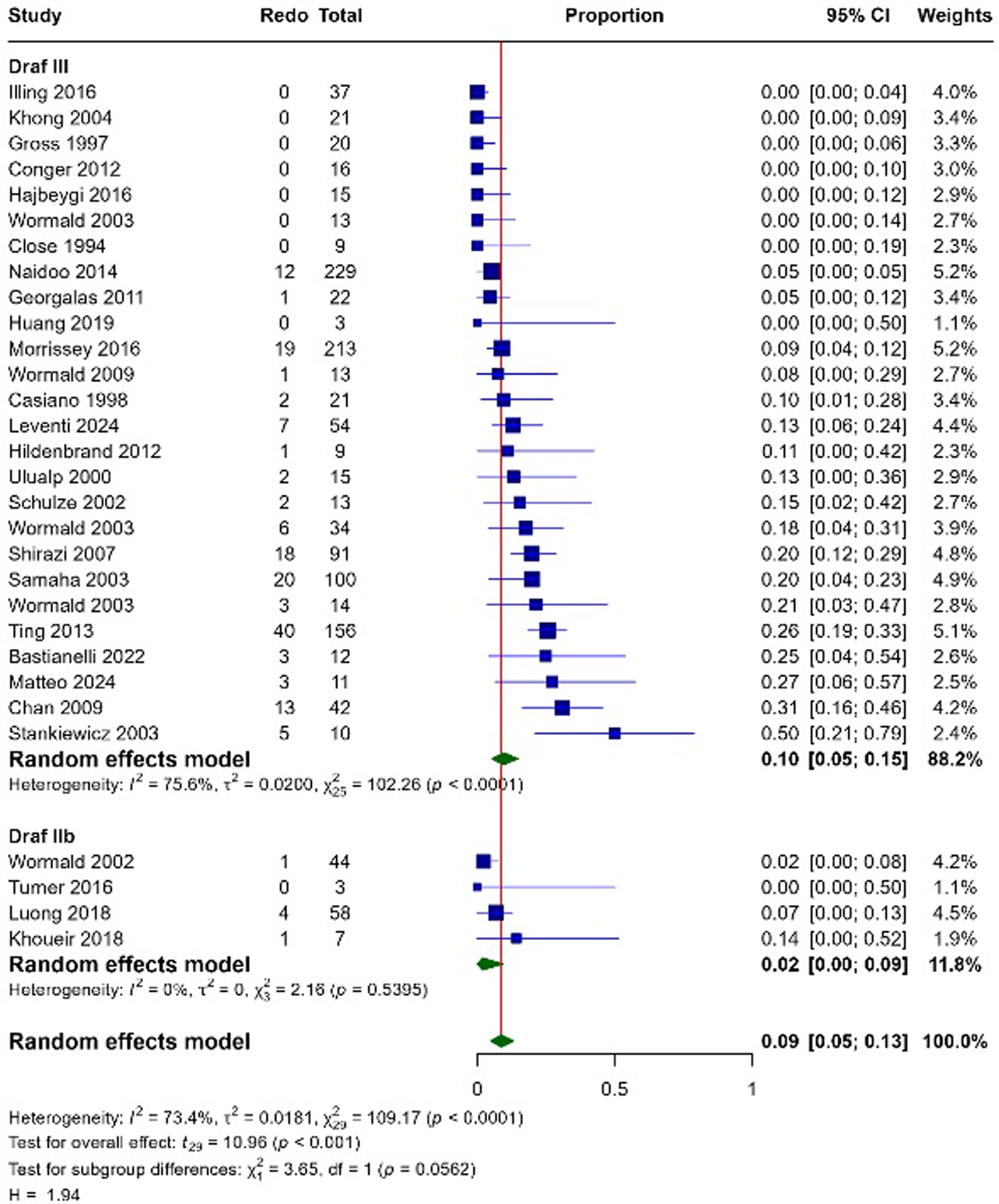
Proportional meta-analysis comparing revision outcomes between Draf IIb and Draf III across single-arm studies.
Type 2 CRS Versus Non-Type 2 CRS
To assess whether inflammatory endotype influenced surgical outcomes, a subgroup analysis was conducted comparing restenosis and revision rates between patients with Type 2 CRS and those with non-Type 2 CRS. This analysis was performed irrespective of the specific Draf procedure undertaken, allowing evaluation of endotype effects across all included surgical cohorts.
Restenosis
Eighteen studies reported restenosis outcomes for patients with Type 2 CRS, comprising a total of 479 individuals, of whom 67 developed restenosis. This corresponded to a pooled restenosis proportion of 0.08 (8%) (95% CI: 0.01-0.20), with high heterogeneity (I2 = 80.8%). Sixteen studies reported outcomes for non-Type 2 CRS, with 39 cases of restenosis among 589 patients. The pooled restenosis proportion in this group was 0.01 (1%) (95% CI: 0.00-0.05), with moderate heterogeneity (I2 = 43.4%). The between-group comparison demonstrated a statistically significant difference (p = .012) (Figure 4).
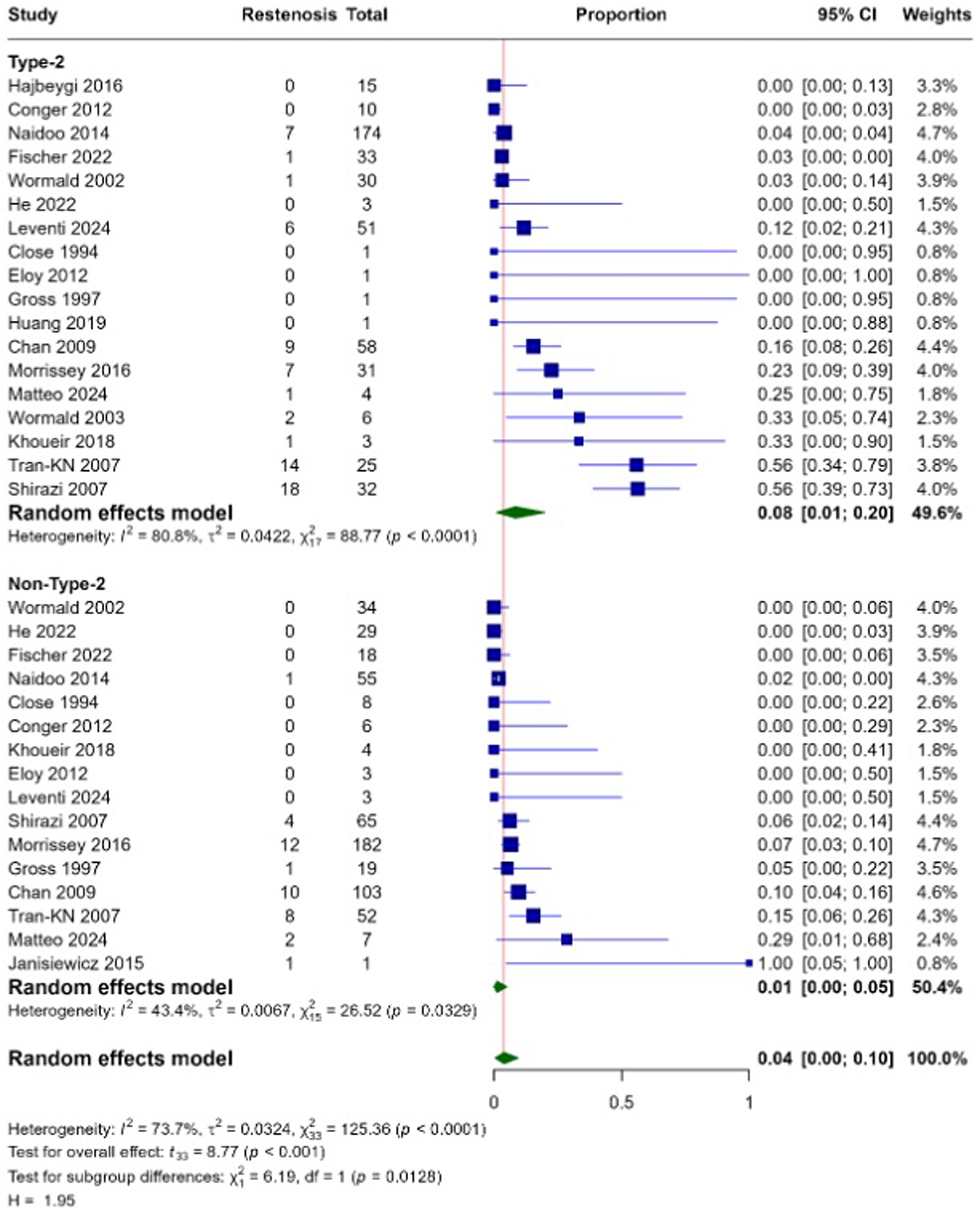
Pooled meta-analysis of restenosis proportions in type 2 versus non-type 2 CRS.
Revision
Revision rates were also evaluated in relation to CRS endotype. Six studies reported outcomes for patients with Type 2 CRS, comprising 115 individuals, 27 of whom required revision surgery. This yielded a pooled revision proportion of 0.12 (12%) (95% CI: 0.01-0.29) with low heterogeneity (I2 = 16.6%). For non-Type 2 CRS, five studies including 137 patients contributed data, among whom 32 required revision surgery. The pooled revision proportion in this group was 0.03 (3%) (95% CI: 0.00-0.25), with high heterogeneity (I2 = 80.8%). The comparison between subgroups demonstrated a statistically significant difference (p = .040) (Figure 5).
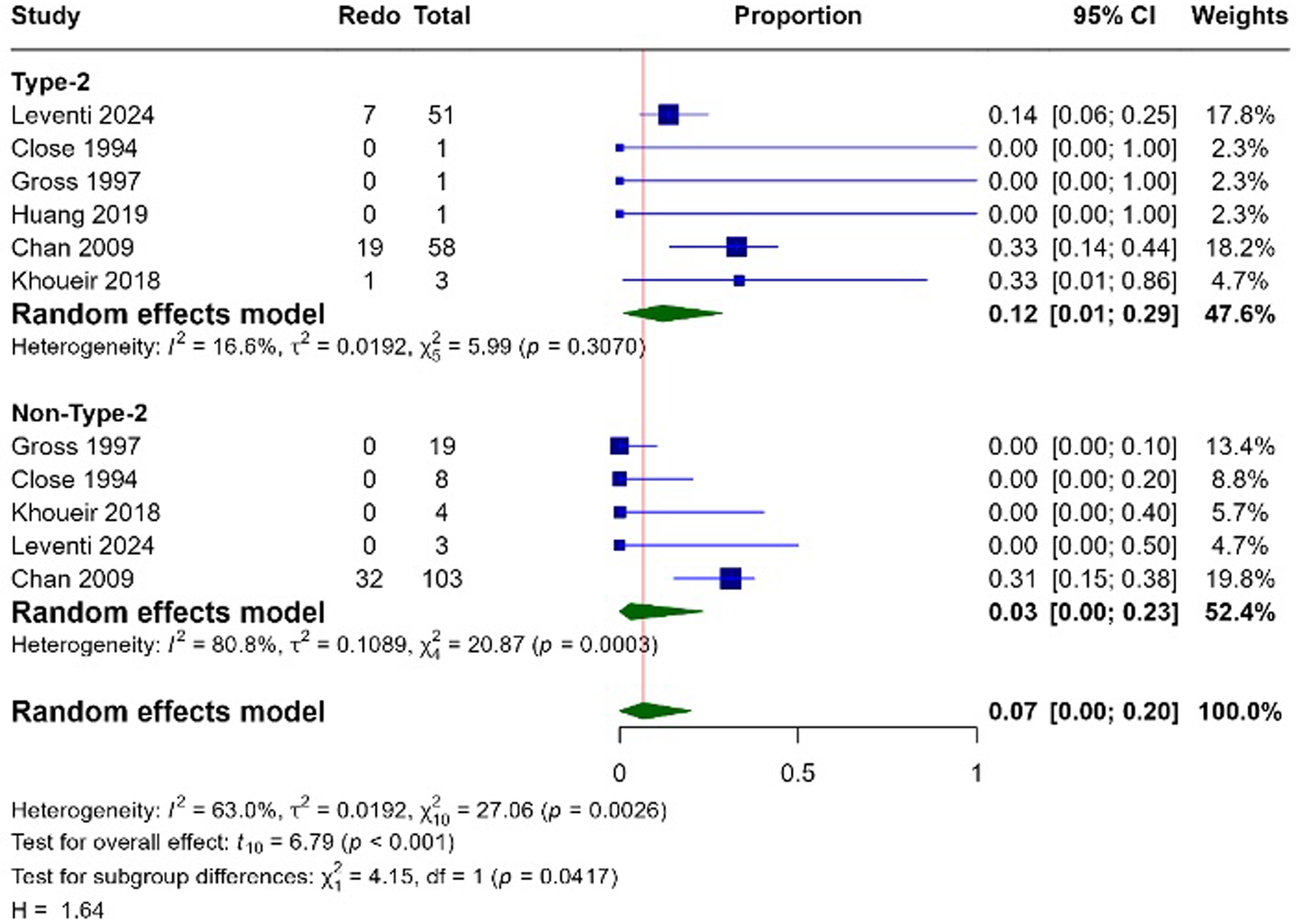
Proportional meta-analysis comparing revision outcomes between type 2 and non-type 2 CRS.
Draf IIb v Draf III in Type 2 CRS
Within the type 2 CRS subgroup, outcomes were further analyzed according to the type of Draf procedure performed.
Restenosis
Only three studies reported on Draf IIb, with 1 out of 34 patients having restenosis. The yielded pooled outcome proportion was 0.00 (0%) (95% CI: 0.00–0.01) and heterogeneity of I2 = 0%. In comparison, fifteen studies provided data for Draf III. Across these studies, a total of 445 patients were evaluated, with 66 developing restenosis. The pooled outcome proportion of 0.11 (11%) (95% CI: 0.02–0.25) and heterogeneity of I2 = 83.8% was seen. The test for subgroup differences showed a statistically significant difference between Draf IIb and Draf III with p-value <.01 (Figure 6).
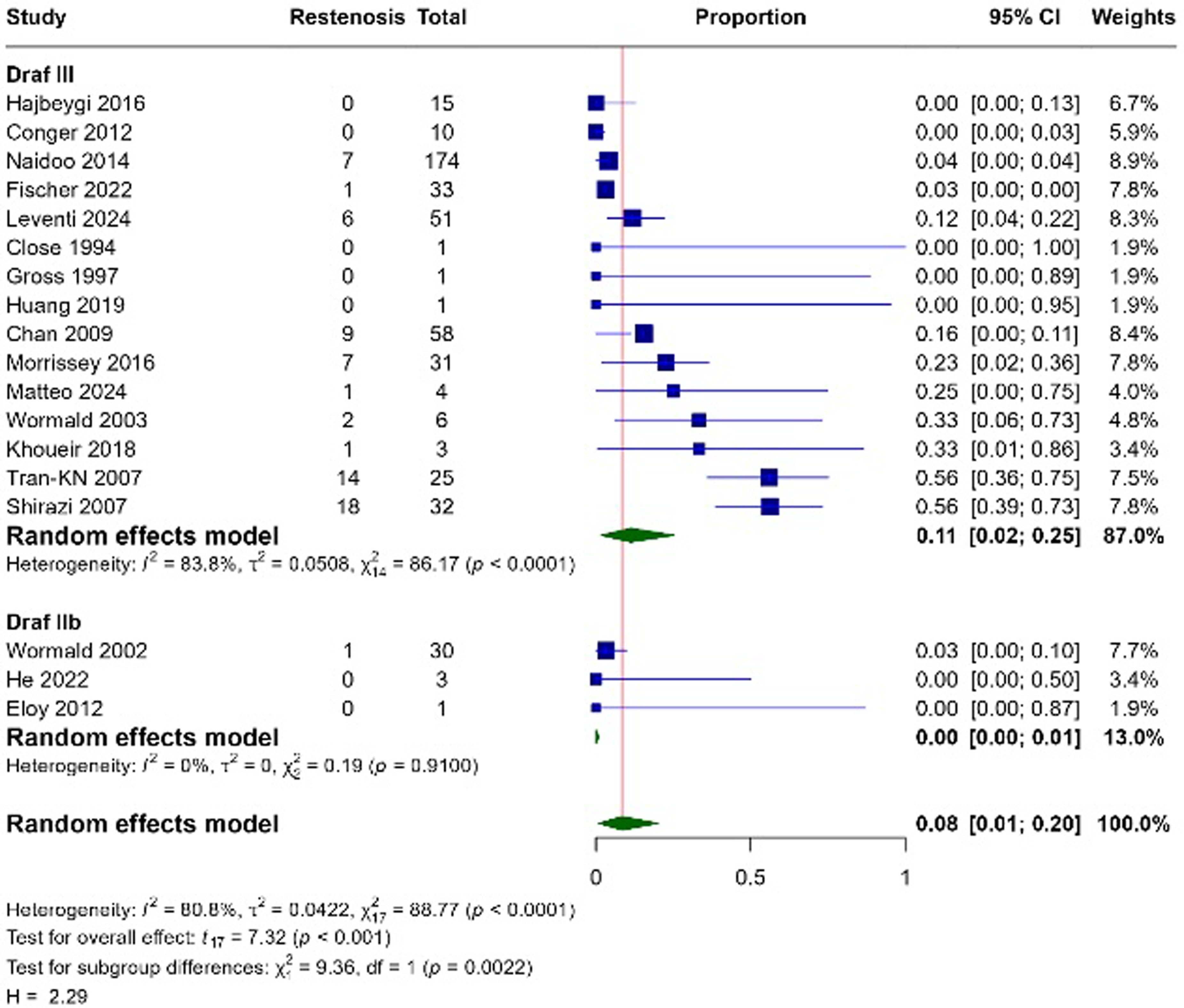
Proportional meta-analysis comparing restenosis outcomes between Draf IIb and Draf III in type 2 CRS.
Revision Surgery
Within the Type 2 CRS subgroup, only one study reported revision outcomes for Draf IIb, in which 1 of 3 patients required revision surgery, yielding a revision proportion of 0.33 (33%) (95% CI: 0.01-0.86). Five studies reported revision outcomes following Draf III, comprising 112 patients, 26 of whom underwent revision surgery. The pooled revision proportion for Draf III was 0.11 (11%) (95% CI: 0.00-0.30), with low-to-moderate heterogeneity (I2 = 16.6%). The test for subgroup differences demonstrated no statistically significant difference between Draf IIb and Draf III (p = .556) (Figure 7).
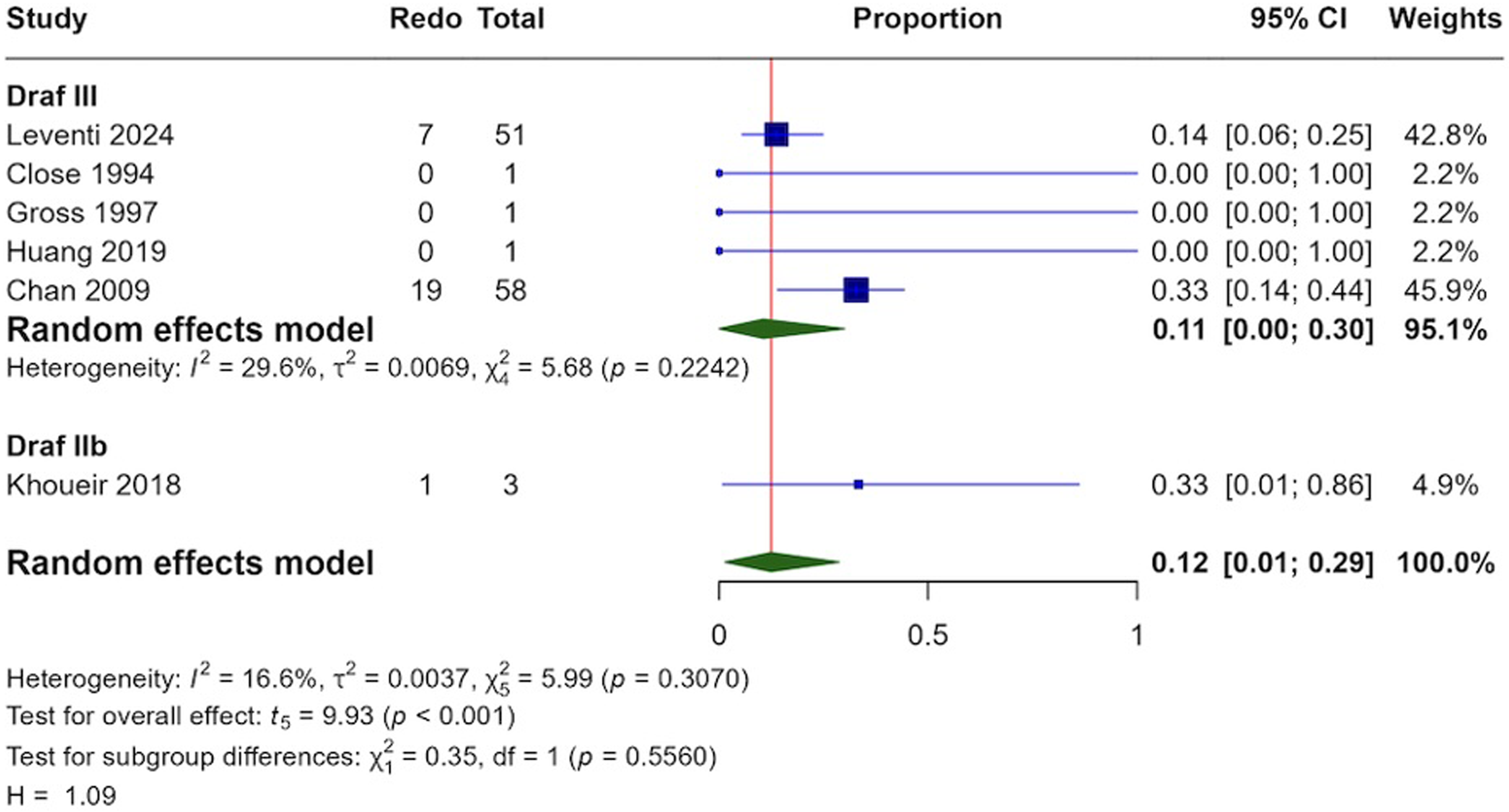
Proportional meta-analysis comparing revision outcomes between Draf IIb and Draf III in type 2 CRS.
Draf IIb Versus Draf III in Non-Type 2 CRS
Outcomes were also stratified by Draf procedure type within the non-Type 2 CRS subgroup.
Restenosis
Within the Non-Type 2 CRS subgroup, four studies reported restenosis outcomes following Draf IIb, comprising 67 patients, only one of whom developed restenosis. The pooled restenosis proportion was 0.00 (0%) (95% CI: 0.00-0.40), with moderate-to-high heterogeneity (I2 = 58.7%). In contrast, twelve studies reported restenosis outcomes following Draf III, encompassing 522 patients, of whom 38 developed restenosis. The pooled restenosis proportion for Draf III was 0.04 (4%) (95% CI: 0.01-0.07), with low heterogeneity (I2 = 17.3%). The test for subgroup differences did not reach statistical significance (p = .060) (Figure 8).
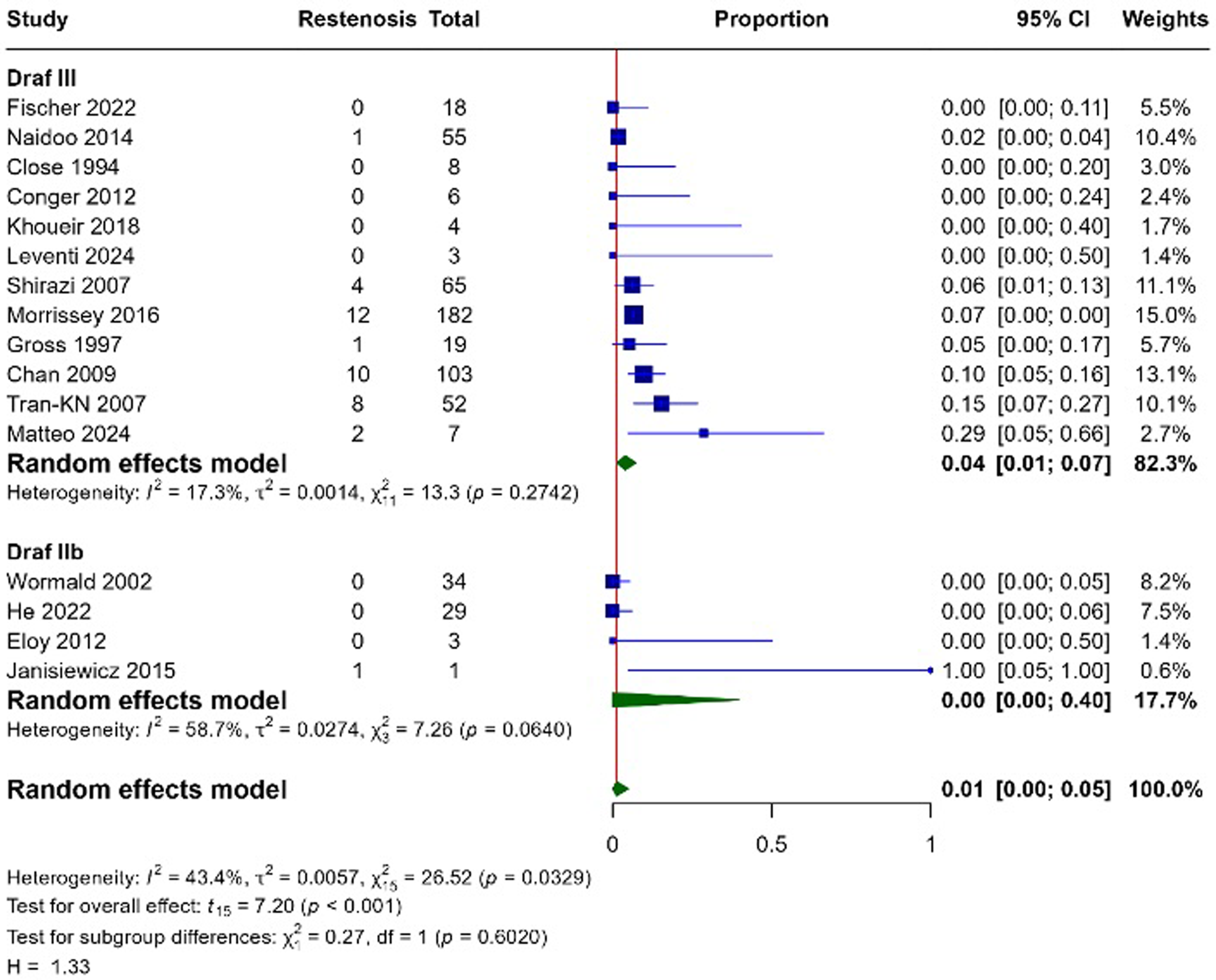
Proportional meta-analysis comparing restenosis outcomes between Draf IIb and Draf III in non-type 2 CRS.
Revision
Within the non-Type 2 CRS subgroup, only one study reported revision outcomes for Draf IIb, comprising four patients, none of whom required revision surgery. The resulting revision proportion was 0.00 (0%) (95% CI: 0.00-0.38). For Draf III, four studies reported revision outcomes, encompassing 133 patients, of whom 32 required revision surgery. The pooled revision proportion for Draf III was 0.04 (4%) (95% CI: 0.00-0.38), with high heterogeneity (I2 = 80.8%). The test for subgroup differences was not statistically significant (p = .79) (Figure 9).
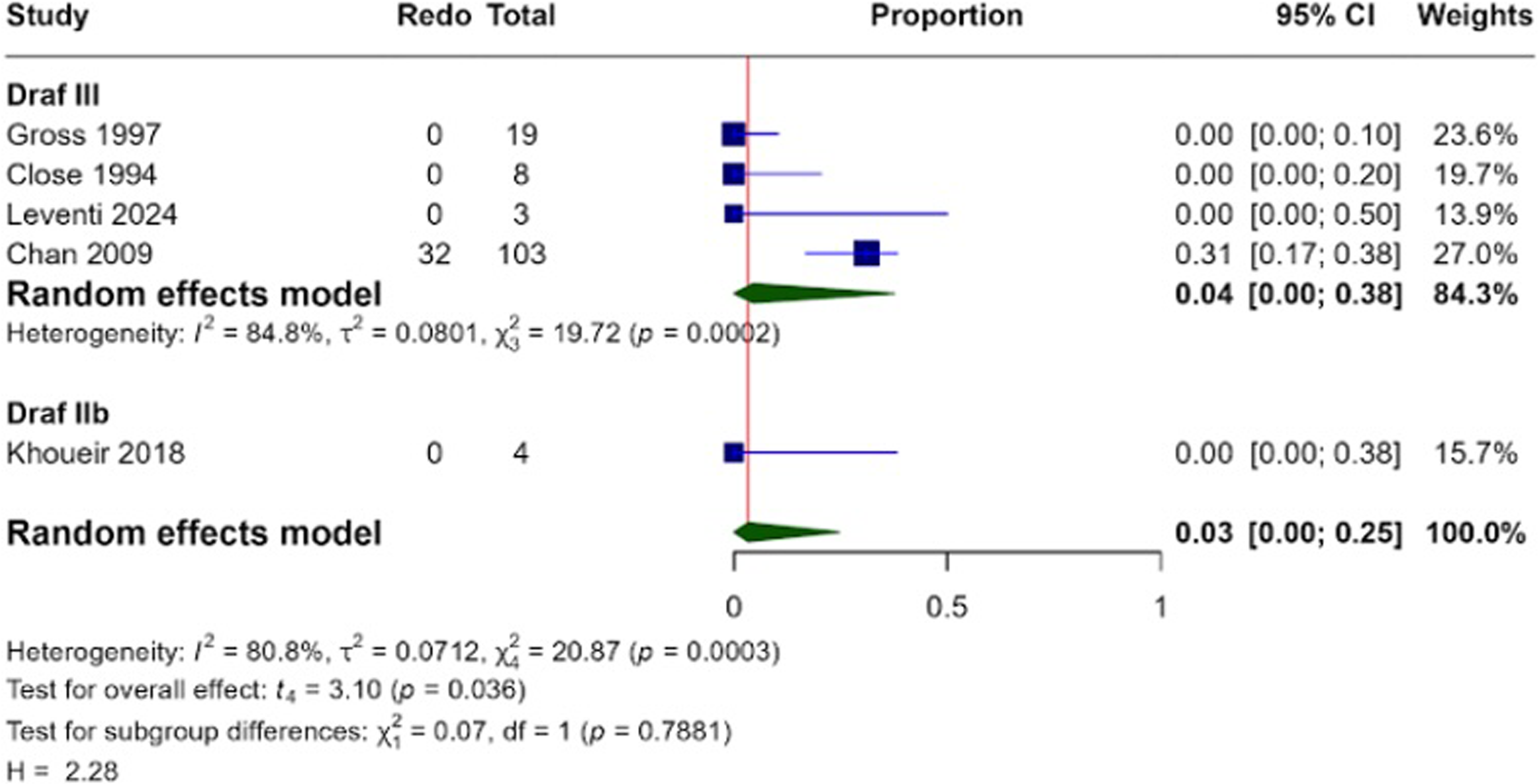
Proportional meta-analysis comparing revision outcomes between Draf IIb and Draf III in non-type 2 CRS.
Discussion
Long-term frontal sinus surgical success is largely determined by restenosis rates and the frequency of revision procedures. To date, no systematic review has comprehensively reported these outcomes for Draf IIb and Draf III in the context of CRS and its inflammatory endotypes. Our systematic review and meta-analysis, conducted without date restrictions, aimed to address this gap.
We found that overall restenosis rates were substantially lower for Draf IIb (0.8%) compared with Draf III (12%). When analyzed by endotype, a similar pattern was observed in Type 2 CRS, whereas in non-Type 2 CRS restenosis rates were lower for both procedures; 4% for Draf III and 0.00% for Draf IIb, indicating higher patency in non-Type 2 disease. Although CRS is traditionally categorized phenotypically (with or without nasal polyps), emerging literature highlights considerable overlap between phenotype and endotype, with endotype increasingly recognized as a more reliable predictor of revision surgery risk.
Patients with more aggressive Type 2 inflammatory disease require closer follow-up and strict adherence to postoperative topical steroid regimens. Type 2 CRS is consistently associated with a more severe disease course than non-Type 2 CRS, a trend reflected in our findings: revision rates were 9% for Draf III and 1% for Draf IIb, and when stratified by endotype, 13% in Type 2 CRS versus 7% in non-Type 2 CRS. Higher revision and restenosis rates likely stem from both intrinsic disease factors and iatrogenic contributors. Excessive drilling and heat generation may provoke osteitis and subsequent restenosis, while suboptimal postoperative compliance particularly in Type 2 CRS may further worsen outcomes.
The role of frontal sinus surgery in CRS has long been a subject of debate among otolaryngologists. Surgeons with a dedicated rhinology practice may be more inclined to address the frontal sinus comprehensively, whereas those with a broader general practice may opt for a more conservative approach to minimize the risk of intracranial injury. Recent international consensus guidelines, however, increasingly support comprehensive sinus surgery that addresses all diseased sinus compartments, reflecting a shift toward evidence-based management. 56 Additionally, a recent systematic review by Blauwblomme et al. identified Draf IIa as a conservative procedure that still reliably permits effective frontal sinus irrigation with topical corticosteroids. 57
Strengths and Limitations
A systematic review comparing Draf IIb and Draf III across all surgical indications 17 has previously been published. Although that work provided comparative insights, it did not focus specifically on CRS. To our knowledge, this is the first systematic review and meta-analysis to report restenosis and revision outcomes in CRS stratified by inflammatory endotype offering a more clinically nuanced understanding of factors influencing frontal sinus surgical success.
Most studies used standard diagnostic criteria and clearly described eligibility, demographics, clinical features, and surgical details. However, several methodological concerns warrant caution when interpreting our findings. Case selection was often insufficiently defined, as many studies failed to specify if patients were recruited consecutively, introducing potential selection bias. Follow-up reporting was also inconsistent, frequently lacking detailed durations or clear definitions for restenosis and revision surgery, limiting comparability; restenosis definitions varied across studies, Assessments primarily included direct endoscopic visualization, instrument passability thresholds (eg, inability to pass 3‒5 mm suction tips), and percentage-based reductions (eg, <50% original size). While these represent accepted functional assessments of patency, this variance in measurement thresholds represents a limitation when directly comparing individual study outcomes.
Insufficient reporting of postoperative care (eg, steroid dosage and duration) and undocumented patient compliance may further influence outcomes and introduce unmeasured bias. Post-op debridement practices were underreported across the literature, mentioned only in five of 38 included studies. Variation in surgical experience and surgeon preference may also have contributed to heterogeneity, particularly as Draf III is often reserved for refractory cases with refractory disease, neo-osteogenesis and prior surgical failures. The available studies did not report stratified baseline disease severity metrics (eg, Lund-Mackay scores or neo-osteogenesis grading) between Draf IIb and Draf III cohorts. Moreover, our review did not examine adjunctive techniques such as stents, mucosal flaps, or grafts, which may influence outcomes for both Draf procedures in CRS.
Overall, these limitations underscore the need for high-quality prospective studies with standardized definitions, consistent follow-up, and endotype-specific reporting to refine indications for Draf IIb and Draf III.
Conclusion
Draf IIb was associated with lower restenosis and revision surgery compared with Draf III in patients with CRS. Restenosis and revision rates were consistently higher in individuals with Type 2 inflammatory disease. Future research should prioritise prospective, endotype-stratified studies comparing Draf IIb and Draf III using standardized definitions of restenosis and revision, protocolized postoperative regimens, and extended follow-up periods. Further investigation is warranted into how adjunctive interventions such as biologics, mucosal flaps, and stents can be integrated into tailored surgical strategies for high-risk Type 2 CRS.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924261456359 - Supplemental material for Comparative Restenosis and Revision Rates of Draf IIB Versus Draf III Frontal Sinusotomy in Chronic Rhinosinusitis: A Meta-Analysis Stratified by Endotype
Supplemental material, sj-docx-1-ajr-10.1177_19458924261456359 for Comparative Restenosis and Revision Rates of Draf IIB Versus Draf III Frontal Sinusotomy in Chronic Rhinosinusitis: A Meta-Analysis Stratified by Endotype by Muhammad Sohaib Shahid, Naimal Naeem, Muhammad Danish Lone, Umer Adnan, Muhammad Mahad Khurram, Yuri Hirayama and Haissan Iftikhar in American Journal of Rhinology & Allergy
Footnotes
Ethical Considerations
As this study is a systematic review and meta-analysis of previously published literature, institutional review board (IRB) or ethics committee approval and patient informed consent were not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available within the published article and its supplementary information files. Additional data extracted for this meta-analysis are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.