
Abstract
Background
Epithelial-myoepithelial carcinoma of the sinonasal tract is rare, and optimal postoperative management remains unclear, particularly regarding the role of adjuvant radiotherapy.
Objective
To evaluate associations between surgical margin status, adjuvant radiotherapy, insurance status, and overall survival (OS) in patients with epithelial-myoepithelial carcinoma of the sinonasal tract.
Methods
The National Cancer Database (2004–2020) was queried for patients with epithelial-myoepithelial carcinoma arising in sinonasal subsites (ICD-O 8562). Demographic, tumor, and treatment variables were analyzed for 81 patients. OS was estimated using the Kaplan–Meier analysis with log-rank testing. Cox proportional hazards models were used to evaluate associations between treatment modality, margin status, insurance status, and OS.
Results
Mean age was 64.2 years; 56.8% were female. Surgery was performed in 69/81 patients (85.2%); 51 had documented margin status (37 negative, 14 positive). Overall 1-, 5-, and 10-year OS were 95.0%, 76.3%, and 44.9%, respectively. Negative-margin resection was associated with superior OS compared with positive margins (log-rank p = .002). Among patients with negative margins, adjuvant radiotherapy was not associated with improved OS (log-rank p = .82). Insurance-related differences in OS were observed (p = .002).
Conclusion
In epithelial-myoepithelial carcinoma of the sinonasal tract, achievement of negative surgical margins is the principal determinant of overall survival. Adjuvant radiotherapy following negative-margin resection was not associated with improved overall survival in this cohort.
Keywords
Introduction
Epithelial-myoepithelial carcinoma (EMC) is an extremely rare carcinoma that accounts for approximately 1% to 2% of all salivary gland neoplasms.1,2 It most commonly arises in the major salivary glands but has been reported in minor salivary sites, including the sinonasal tract. 3 Diagnosis is confirmed histologically by its characteristic biphasic ductal architecture.4–8 Therefore, EMC can present anywhere there is a double ductal layer pattern, including the minor salivary tissue of the sinonasal region (EMCSN) in rare cases. 7 When EMC arises in the sinonasal tract, primary surgical resection and the delivery of postoperative radiotherapy may be technically challenging given the anatomic constraints and proximity to critical structures. The role of adjuvant postoperative radiotherapy in this setting remains poorly defined.1,4,7,9
Patients with EMCSN typically present with nonspecific unilateral nasal obstruction with or without epistaxis. Tumors most commonly arise in the nasal cavity or maxillary sinus and may cause facial swelling, epiphora, hyposmia, or visual symptoms depending on the extent of invasion.1–4,9 Published literature suggests 5- and 10- year overall survival (OS) of 72.7% and 59.5%. 2 Prognosis varies based on tumor size, presence of nodal or distant metastases, patient age at presentation, and treatment modality. 1
As with most salivary gland malignancies, the first-line treatment is complete surgical resection with negative margins, but the role of adjuvant treatment remains controversial.1,3,4,9 Rates of local recurrence and distant failure vary in literature, from 26.7% to 50% and from 4.5% to 35%, respectively, with positive surgical margins being the greatest predictor for increased risk of local recurrence.3,9 Adjuvant radiation therapy may play a role in improving locoregional control in cases of positive or close margins, especially in sinonasal subsites where disease may be difficult to clear.
There have been few reports of large cohorts evaluating the relationship between treatment modalities and overall survival of patients diagnosed with EMC at any site. Most reports of EMCSN are small case series, and none have investigated the role of adjuvant radiation on survival. Current practice at most centers is centered on approaches for other salivary gland malignancies: surgical resection followed by adjuvant radiotherapy in cases with positive surgical margins or high-grade histology. The survival impact of adjuvant radiotherapy, however, remains unclear, especially in rare sinonasal cases.9,10 Understanding this relationship may inform discussion and recommendations regarding treatment of this rare malignancy. This study assesses the association between treatment modality, patient and tumor characteristics, and survival outcomes using data from the National Cancer Database (NCDB).
Materials and Methods
Data Source
Data were obtained from the NCDB, a hospital-based registry of de-identified cancer cases from Commission on Cancer-accredited institutions. This study was deemed exempt by the University of Chicago Institutional Review Board.
Patient Population
Patients diagnosed with EMCSN between 2004 and 2020 according to the ICD-O histology code 8562 and ICD-9 site codes covering the nasal cavity, paranasal sinuses, and nasopharynx (C300-301, C110-C113, C118-119, C310-313, and C318-319) were included in this study. The NCDB includes data from 1989 to 2020. The Fall 2023 release used in this analysis compiled data from 2004 to 2020. Patients without clinical staging data, survival or follow-up data, or treatment details were excluded. The final analytic cohort included 81 patients.
Independent and Dependent Variables
Treatment modality was the primary exposure variable. Treatment modalities included surgery alone, surgery with adjuvant radiotherapy, primary radiotherapy, chemotherapy, and chemoradiotherapy (with or without surgery). For patients who underwent surgery, the presence of positive or negative margins was noted. The primary outcome was overall survival (OS), defined as time from diagnosis to death from any cause; patients alive at last contact were censored at last contact. Patients without documented treatment plans were excluded.
Covariates
Patient demographic included age, sex, race, degree of urbanization, insurance status, and Charlson–Deyo medical comorbidity score. 11 Age was coded as <50, 50 to 60, 60 to 70, and >70 years. Race was coded as White, Black, Asian, and Other. The degree of urbanization was based on population count and geographical location of the county where the patient resided. It was categorized as “Metro,” “Urban,” and “Rural.” Insurance status was defined by payor into private insurance, Medicaid, Medicare, other government sponsored, and unknown or not insured. Comorbidity was dichotomized as 0 versus ≥1.
Clinical characteristics included primary site, tumor staging, tumor grade, presence of nodal disease or distant metastases, treatment modalities, and timing of treatments. Primary sites included in this study were nasal cavity, nasopharynx, maxillary sinus, and ethmoid sinus. Tumor grade/differentiation was categorized from Grades I to IV from well-differentiated to undifferentiated, respectively. Treatment modalities evaluated included surgery, radiotherapy, and chemotherapy. If surgery was performed, margin status was assessed and coded as positive, negative, or unknown margin status.
Statistical Analysis
Data were extracted from the NCDB database and analyzed in R software version 4.3.0. Descriptive statistics are presented as n (%) for categorical variables and mean (SD) for continuous variables. P-values for between-group comparisons are reported in Tables 1–3. Univariate analysis was performed for associations between overall survival and treatment modality. Survival was estimated using the Kaplan–Meier method and compared with the log-rank test; 1-, 5-, and 10-year overall survival estimates are reported. Multivariable Cox proportional hazard models were fit to assess associations between overall survival and selected covariates; hazard ratios (HRs) with 95% confidence intervals (CIs) are reported in Supplementary Tables S1–S3.
Results
Patient Characteristics
A total of 81 patients were identified as having primary EMCSN and were included in this study. The mean age was 64.19 years, with 42% of patients being greater than 70 years old. The majority (56.79%) of patients were female. The cohort was 85.19% white, and 59.26% had government-sponsored insurance. The majority (55.56%) of patients presented with a primary tumor in the nasal cavity, followed by the maxillary sinus (18.52%). Most patients were staged as T1 (55.56%) and N0 (97.53%) with no metastasis at diagnosis. Sixty-nine (85.19%) underwent resection of the primary tumor, 25 received radiation (30.86%), and 10 received chemotherapy (12.35%). All patient and tumor characteristics are summarized in Table 1.
Demographics and Clinical Characteristics of the EMC-SN Cohort (n = 81).
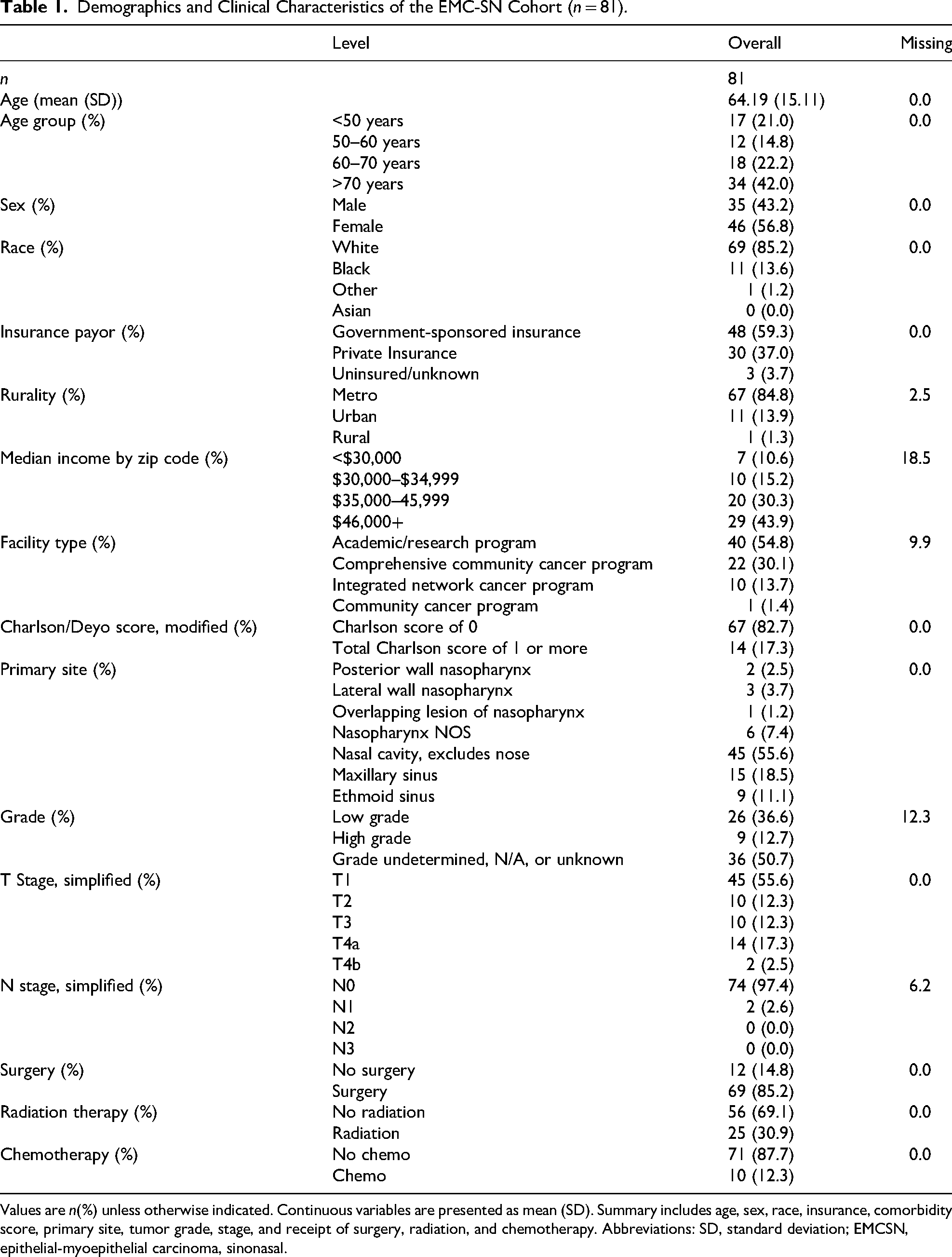
Values are n(%) unless otherwise indicated. Continuous variables are presented as mean (SD). Summary includes age, sex, race, insurance, comorbidity score, primary site, tumor grade, stage, and receipt of surgery, radiation, and chemotherapy. Abbreviations: SD, standard deviation; EMCSN, epithelial-myoepithelial carcinoma, sinonasal.
Treatment Modalities
In total, 69 (85.2%) patients received surgery, 16 of whom received adjuvant radiotherapy. Of the 12 patients who did not receive surgery, 9 underwent radiation. Ten patients in total underwent chemotherapy. On average, treatment was started 29.75 (±48.99) days after diagnosis.
Surgery
Of the 69 patients that underwent surgery, 37 had negative margins, 14 had positive margins, and the margin status of 18 patients were unknown. Ninety percent of patients with private insurance underwent surgical resection, while 18.8% of patients with government-sponsored insurance did not. Differences in primary site were significantly associated with surgical intervention, but no clear pattern was identified (p = .021). There was no difference in rates of surgery when stratified by grade (p = .893), though a significant proportion of patients were missing grade data. Treatment modalities for tumors classified as grade undetermined/unknown grade tumors included surgery (72.2%), surgery with radiation (11.1%), and chemoradiation therapy (11.1%). Of the patients who received surgery monotherapy, the majority (84.9%) had low tumor stage (T1/T2).
Adjuvant Radiation Therapy
Thirteen patients underwent surgical resection of the primary tumor followed by adjuvant radiation. When stratified by grade, surgery with radiation was the second most common treatment modality for low-grade (15.4%) and high-grade (33.3%) tumors. Comparatively, for grade undetermined/unknown grade tumors, surgery with radiation (11.1%) was the second most common treatment plan. Patients with high-grade tumors were significantly more likely (p = .012) to receive radiation than those with low-grade or unknown/undetermined-grade tumors (Table 2). Tumor grade did not have a statistically significant association with adjuvant radiotherapy treatment (Table 2). There was no statistically significant association between the presence of positive, negative or indeterminate margins with adjuvant radiotherapy treatment (Table 3).
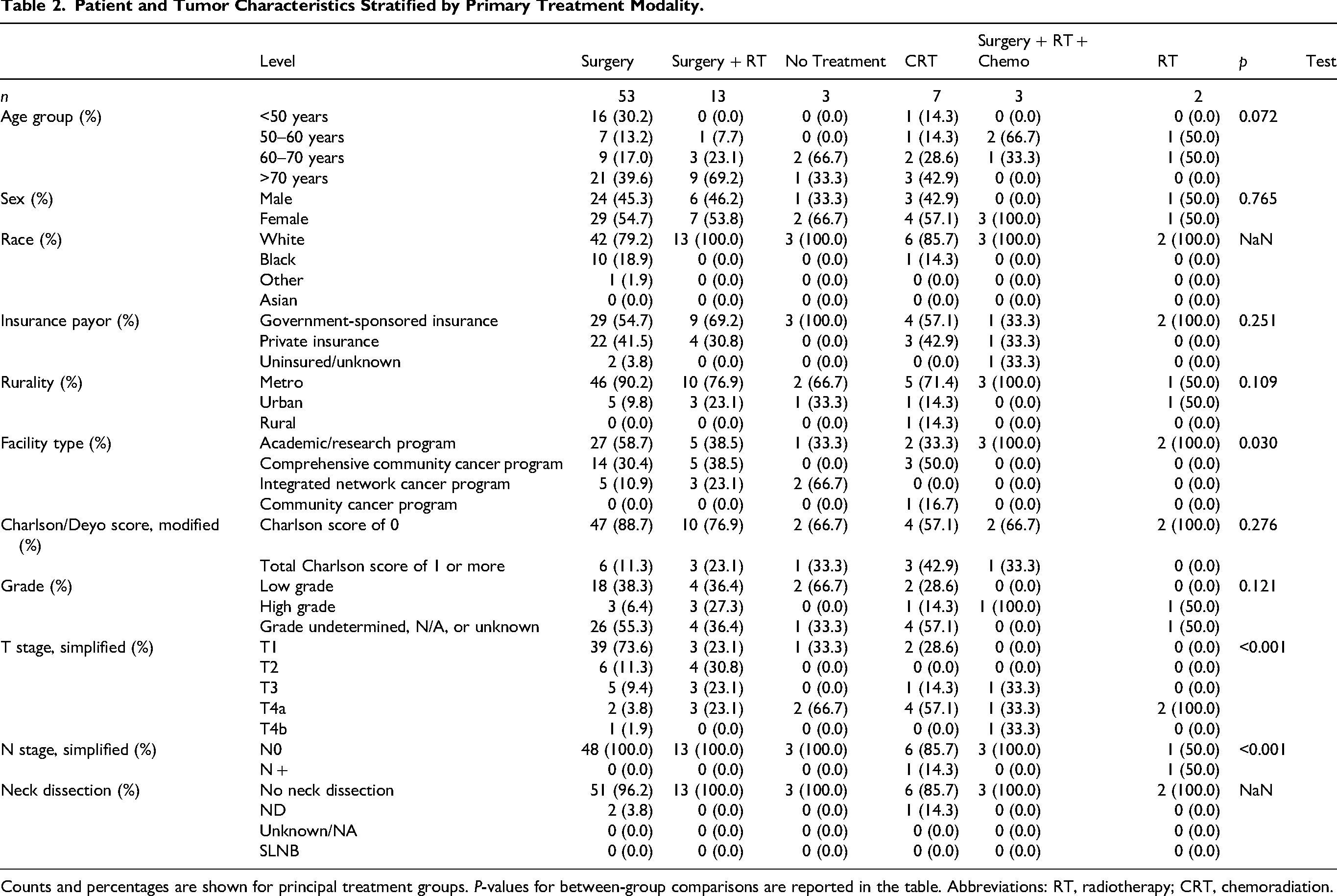
Counts and percentages are shown for principal treatment groups. P-values for between-group comparisons are reported in the table. Abbreviations: RT, radiotherapy; CRT, chemoradiation.
Treatment Characteristics by Insurance Category.
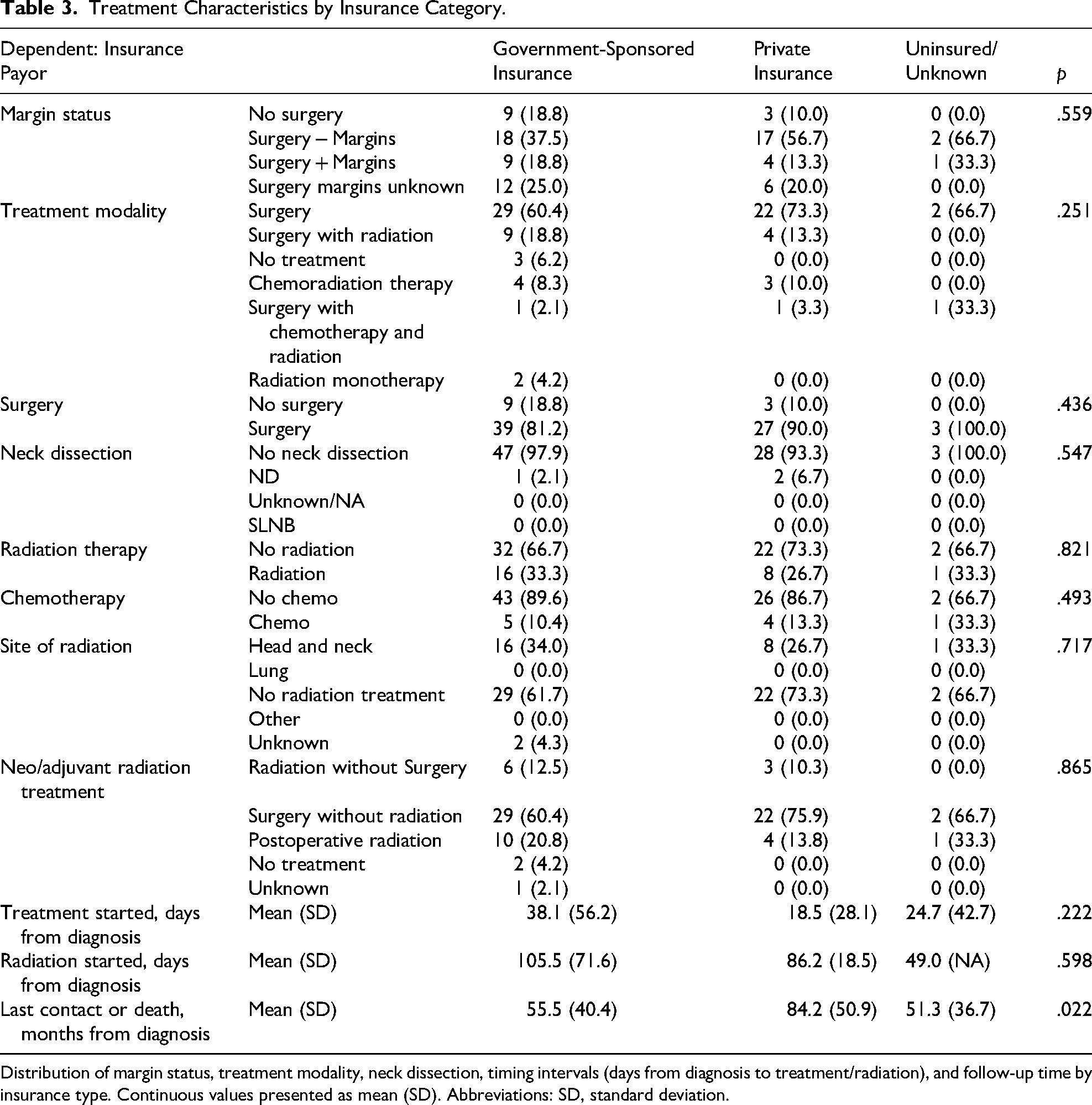
Distribution of margin status, treatment modality, neck dissection, timing intervals (days from diagnosis to treatment/radiation), and follow-up time by insurance type. Continuous values presented as mean (SD). Abbreviations: SD, standard deviation.
Chemotherapy
A total of 10 patients underwent chemotherapy. The use of chemotherapy was not significantly associated with age (p = .372) or comorbidity score (p = .114). Among patients who underwent chemotherapy, 30.0% received it as part of a multimodal treatment approach, including surgery and radiation therapy. Margin status was known for patients who had surgery in addition to chemotherapy, with 20.0% having positive margins and 30.0% having negative margins.
Insurance Status
A larger proportion of patients with government-sponsored insurance did not undergo surgical treatment when compared to privately insured patients (18.8% and 10%, respectively, p = .436). Patients with private insurance had the shortest time to treatment initiation following diagnosis, whereas those with government-sponsored insurance had the longest time (18.5 days and 38.1 days, respectively, p = .222). Similarly, radiation therapy was initiated sooner in privately-insured patients and later in patients with government-sponsored insurance (86.2 days and 105.5 days, respectively, p = .598).
Overall Survival
Full univariable and multivariable Cox model outputs (HRs and 95% CIs) are presented in Supplementary Tables S1–S3; the main text reports the Kaplan–Meier estimates and long-rank group comparisons (Tables 1–3, Figures 1–8).
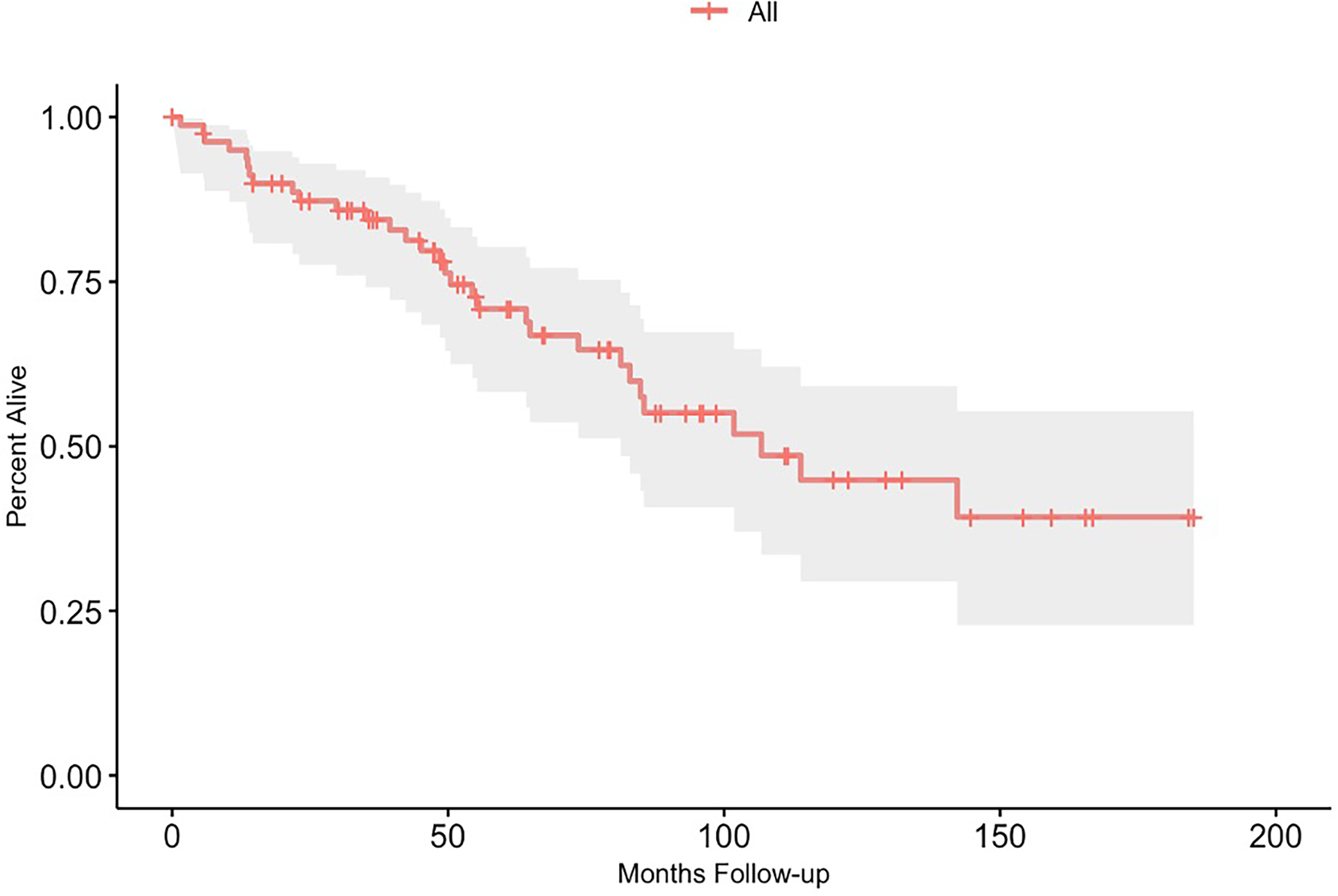
Overall survival (Kaplan–Meier) for the EMC-SN cohort (n = 81). One-, five-, and ten-year overall survival were 94.97%, 76.3%, and 44.87%, respectively. Median follow-up = 106.74 months.
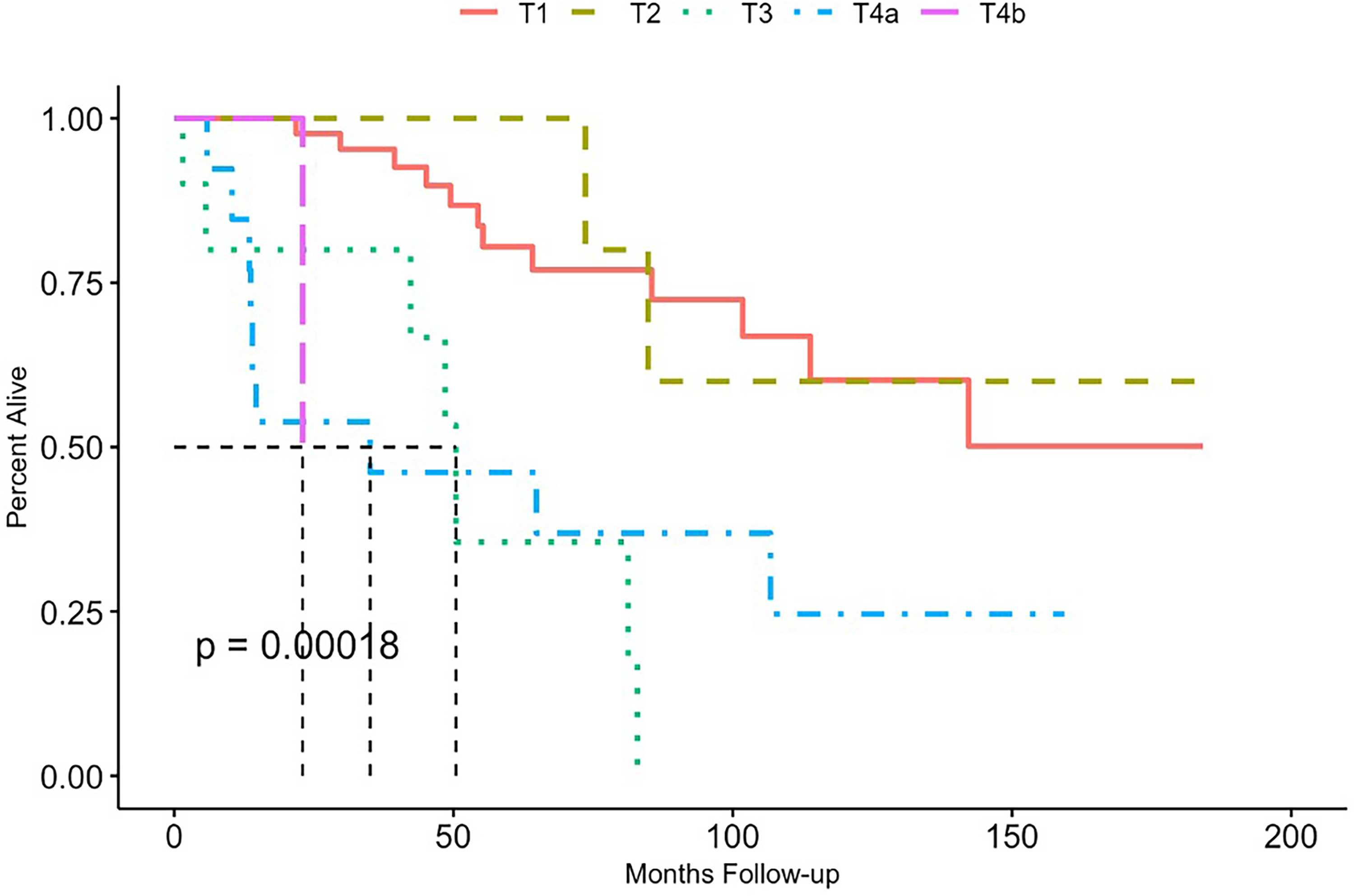
Kaplan–Meier overall survival by T stage (T1/T2 vs T3/T4). Survival estimates for each group are shown in the plot; group comparison by log-rank test is reported in the main text and figure.
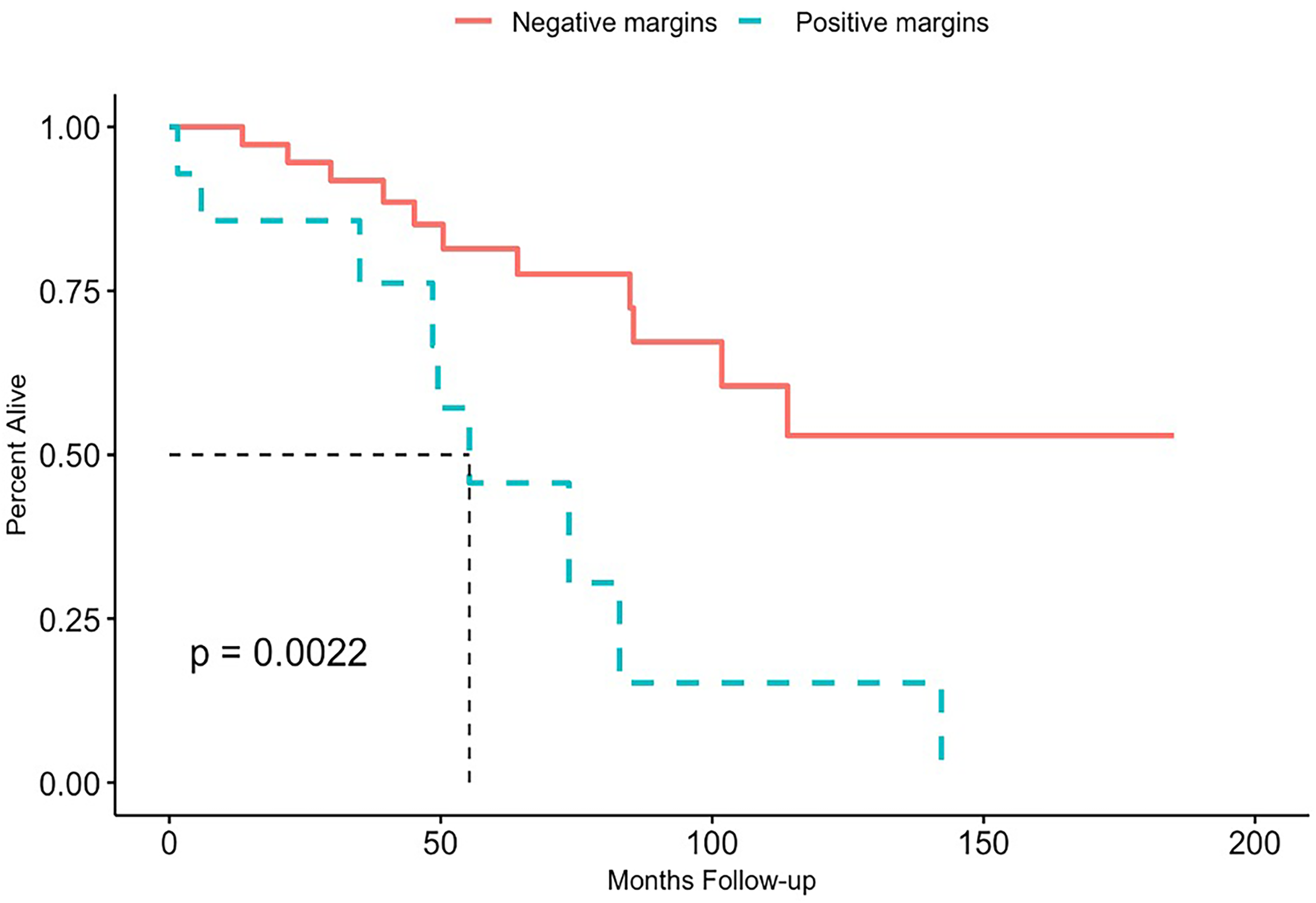
Kaplan–Meier overall survival stratified by surgical margin status (negative vs positive) among patients with documented margins (n = 51). Negative-margin patients (n = 37) had 1-, 5-, 10-year OS of 100%, 81.43%, and 52.93%; positive-margin patients (n = 14) had 85.71%, 45.71%, and 15.24% (log-rank p reported in the main text).
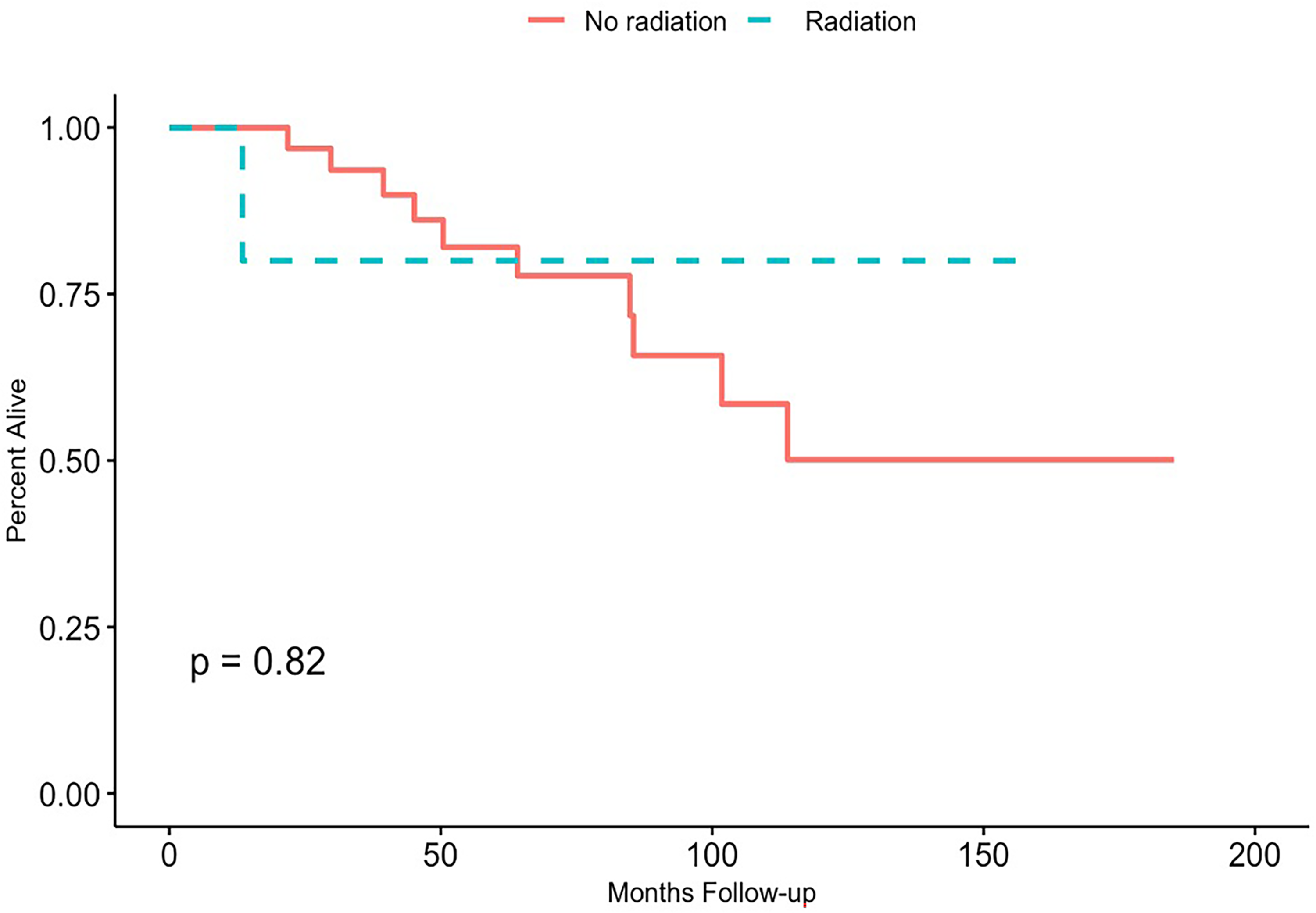
Overall survival among patients with negative margins: no postoperative radiotherapy versus postoperative radiotherapy (n = 37). No significant difference in OS was observed (log-rank p reported in the main text). Dose information (where available) is presented in the figure/table.
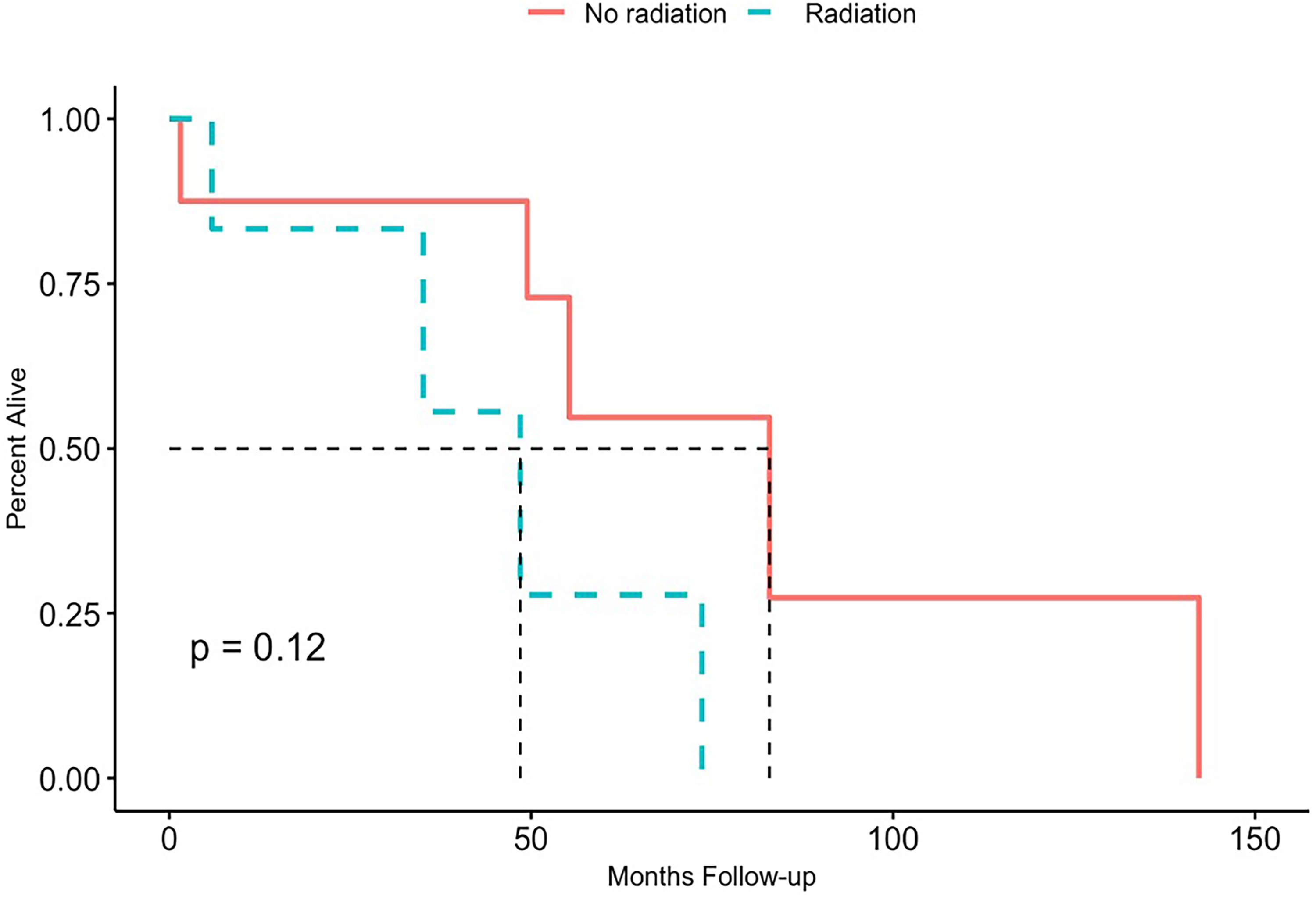
Overall survival among patients with positive margins: no postoperative radiotherapy versus postoperative radiotherapy (n = 14). No significant difference in OS was observed (log-rank p reported in main text).
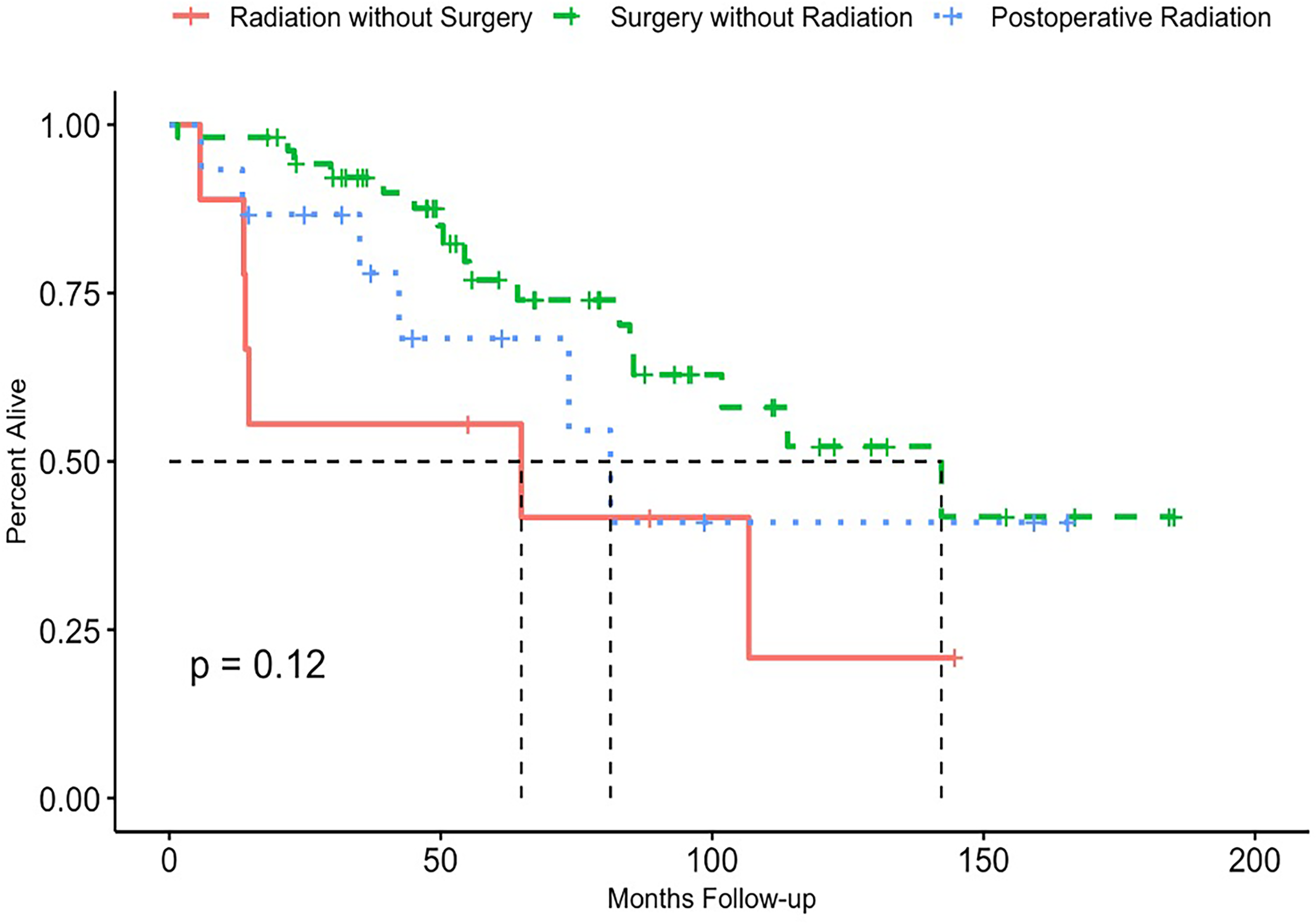
Overall survival by treatment category: surgery without RT, postoperative RT, and radiation monotherapy. Group sizes and log-rank comparison are shown in the figure and described in the main text.
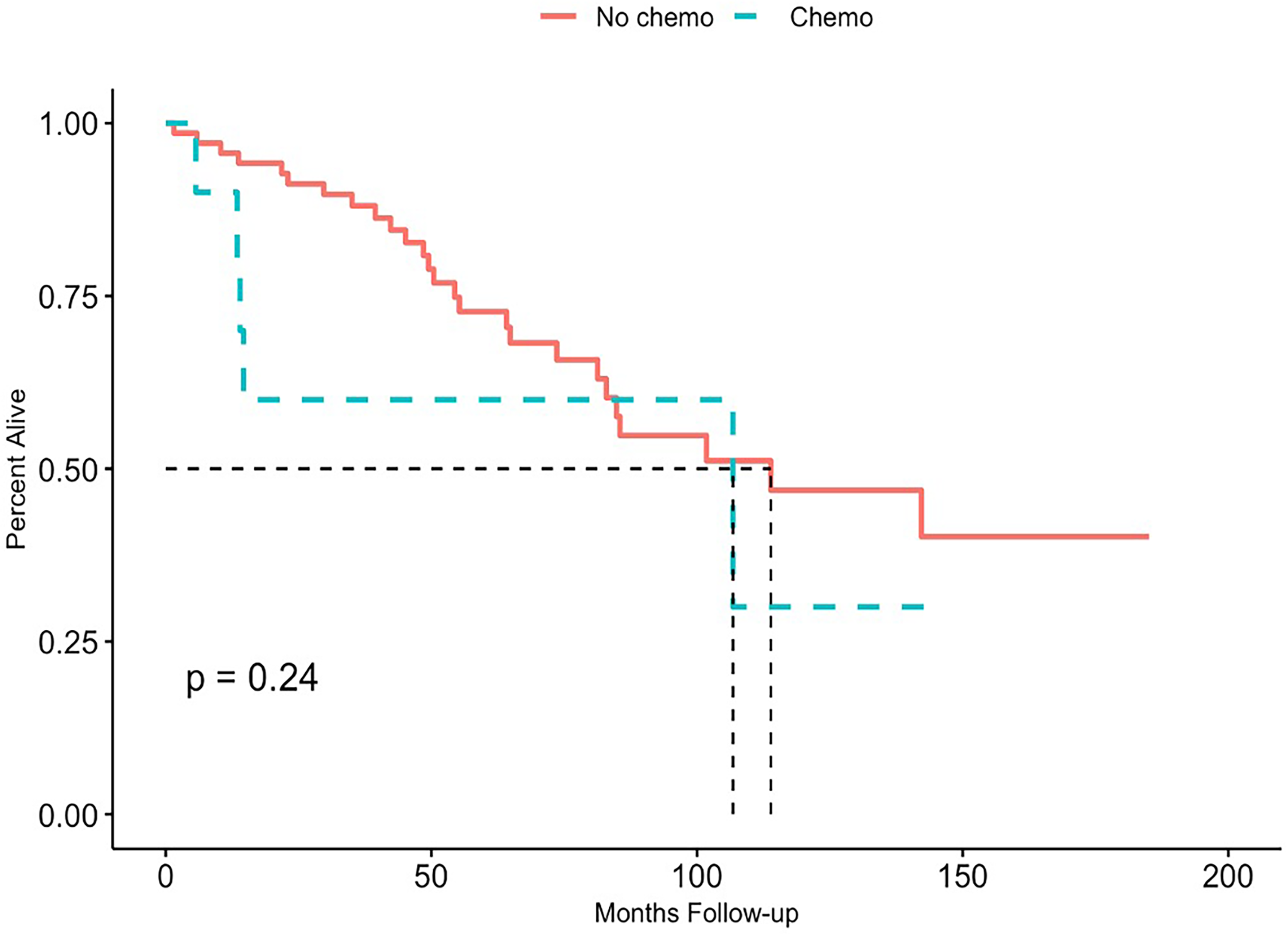
Overall survival by receipt of chemotherapy. Comparison between patients who did and did not receive chemotherapy is shown (n values in the figure); see main text for p-value.
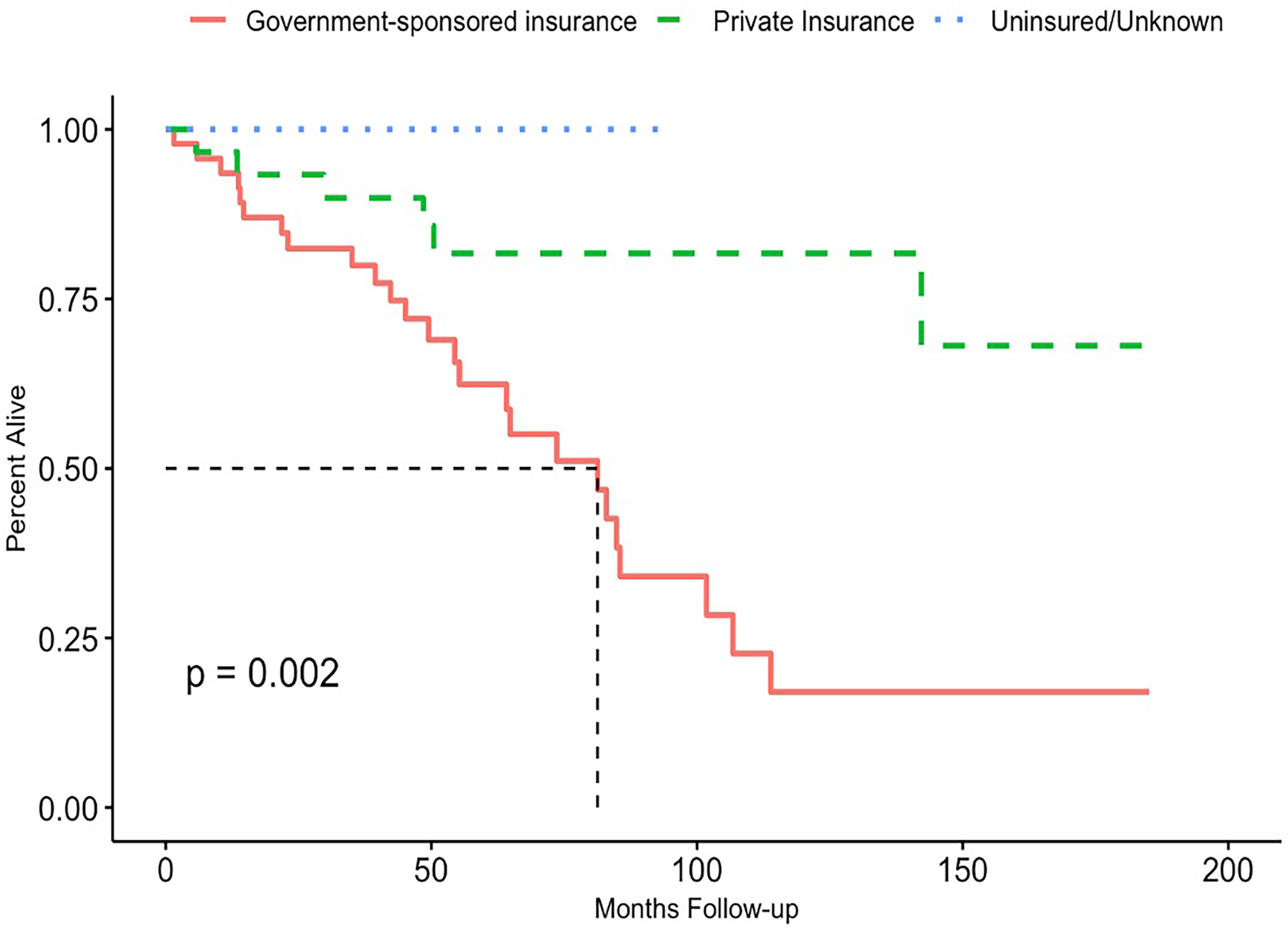
Overall survival by insurance status (private, government-sponsored, uninsured/unknown). Group sizes are shown in the figure; log-rank p is reported in the main text.
The Kaplan–Meier survival curve of all EMCSN patients showed survival rates of 94.97%, 76.3%, and 44.87% at 1-, 5-, and 10-years, respectively (Figure 1). Full multivariable Cox model outputs (univariable and multivariable) are provided in Supplementary Tables S1–S3. Advanced T stage at the time of presentation was associated with worse OS. For T1/T2 stages, 1-, 5-, and 10-year survival rates were 100%, 83.38%, and 58.5%. For advanced stages (T3/T4), survival rates were significantly decreased at 1-, 5-, and 10-years at 85.91%, 42%, and 25.2% (p < 0.01) (Figure 2). Patients with private insurance were significantly more likely (p = .008) to have better survival, at 6.98 ± 4.01 years compared to patients with government-sponsored (4.18 ± 3.02) and unknown/no insurance (4.23 ± 3.06). Univariate analysis showed that patients who received surgery had a significantly (p = .007) greater length of survival post diagnosis, at 5.54 (±3.52) years, compared to patients who did not receive surgery (1.75 ± 2.53). Radiation therapy was not associated with any significant changes in OS.
Treatment modality was also associated with differences in OS. Of the 51 patients who underwent surgery with documented margins, 72.55% had negative margins, with survival rates of 100%, 81.43%, and 52.93% at 1-, 5-, and 10-years, respectively. Furthermore, 27.45% of the patients with positive margins had statistically significantly (p < 0.01) decreased OS for 1-, 5-, and 10-years at 85.71%, 45.71%, and 15.24%, respectively (Figure 3). Of the 37 patients that underwent surgery and had oncologic clearance, 5 underwent adjuvant radiation therapy, with no statistically significant difference in OS (p = .82) (Figure 4). Similarly, of the 14 patients who underwent surgery with positive margins, 6 underwent adjuvant radiation therapy with no statistically significant difference in OS (p = .12) (Figure 5). Adjuvant radiation did not have a statistically significant impact on OS for patients who underwent surgery. There was no statistically significant difference in OS between patients who received radiation monotherapy and patients who received surgery (p = .12) (Figure 6). Chemotherapy was not found to have any association with OS (p = .24) (Figure 7). Uninsured patients had statistically significantly (p = .002) worse OS, relative to both private and government-sponsored insurance patients (Figure 8).
Discussion
This analysis of a large, nationally based cohort of patients undergoing treatment for EMCSN showed that patients undergoing negative-margin surgical resection had significantly better OS. There was no additional OS benefit with adjuvant radiotherapy regardless of margin status. These findings suggest that the most important predictor of OS in EMCSN is negative margin surgical resection.
Notably, our analysis identified significant OS disparities by insurance status: privately insured patients had a mean post-diagnosis survival of 6.98 ± 4.01 years versus 4.18 ± 3.02 years (government-sponsored) and 4.23 ± 3.06 years (uninsured/unknown). Privately insured patients also began treatment sooner (mean 18.5 vs 38.1 days) and were more likely to undergo surgery with negative margins. Our prior work in nasopharyngeal carcinoma and olfactory neuroblastoma likewise found private insurance to be associated with earlier presentation and improved survival, and other head-and-neck studies report similar patterns.12–16 This suggests that differences in access and timeliness of care mediate worse outcomes in underinsured patients. These observations are consistent with the higher proportion of advanced (T3/T4) presentation and lower rates of definitive resection among uninsured/underinsured patients in our cohort, which likely contribute to the observed survival gap.
Current research suggests that surgery has been the most common treatment for EMC patients.17,18 This trend continues in EMCSN patients, with most case studies reporting EMCSN patients undergoing surgery as the primary treatment.3,4 A study using the Surveillance, Epidemiology, and End Results (SEER) database found excision of the tumor with clear margins to be the most common treatment modality in EMC patients; it led to the highest 2- and 5- year overall survival rates at 97% and 85%, respectively. 2 Our study data concurred with this finding and was able to also look at longer term data with 1-, 5-, and 10- year survival rates at 100%, 81.43%, and 52.93%, respectively, for EMCSN patients receiving surgery. Lower rates of distant metastasis in most EMC patients, 19 with the current study finding all patients at N0 stage, may be a factor for why surgical resection of the tumor is an appropriate treatment.
Previous studies have concluded that the presence of negative margins is the most important factor in the surgical resection of EMC patients.9,19,20 This study confirms this outcome in EMCSN in a large nationally representative sample, with negative margins in surgical patients being associated with a significantly greater increase in OS. This may be due to positive margins being associated with increased risk of local recurrence. 9 To mitigate the risks of recurrence in patients who are unable to achieve oncologic clearance during surgery, previous studies have recommended adjuvant radiotherapy. 21
However, although previous studies have suggested a benefit of adjuvant radiotherapy,9,21 our analysis found that adjuvant radiotherapy lacked a significant association with improved OS. This corroborates the finding of a previous literature review of 13 EMCSN case reports that found no survival benefit with the addition of postoperative radiation. 4 The conflicting views in the literature regarding radiotherapy as a mechanism for improving OS may be due to the indolent and rare nature of EMCSN.
There are several limitations to this study. This retrospective database study could not establish causality between predictors and OS. Furthermore, the rarity of EMCSN limits sample size despite the use of a national registry. Additionally, the NCDB does not report disease-specific survival measures or recurrence, limiting outcome assessment. The NCDB does not provide detailed information regarding re-resection for margin clearance or the intent of subsequent surgical procedures. Therefore, we were unable to distinguish patients who underwent revision surgery for positive margins from those managed with adjuvant radiotherapy alone. As a result, conclusions regarding optimal management of positive or close margins should be interpreted with caution. The small number of patients with positive margins also limits statistical power for subgroup analysis.
Future studies should expand upon the role of adjuvant therapy, specifically in patients with positive margins, to improve mortality rates and reduce recurrence and metastases. It would also be informative to study disease-specific survival outcomes and recurrence rates in relation to each primary treatment modality to further understand the long-term effects of the various therapies. Lastly, further research into EMCSN, via multi-institutional studies, could provide insight into factors that are associated with survival benefit.
Conclusion
Negative margin resection is the most important prognostic factor for patients presenting with EMCSN. Adjuvant radiotherapy was not associated with improved overall survival. Disparities in access to appropriate surgical therapy were observed, with patients on government-sponsored insurance less likely to receive optimal surgical care, potentially leading to poorer outcomes. These findings highlight the need for further research to optimize EMCSN treatment strategies and address healthcare disparities to ensure equitable access to appropriate surgical interventions.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924261456834 - Supplemental material for Adjuvant Radiotherapy Does Not Improve Overall Survival After Negative Margin Resection of Sinonasal Epithelial-Myoepithelial Carcinoma
Supplemental material, sj-docx-1-ajr-10.1177_19458924261456834 for Adjuvant Radiotherapy Does Not Improve Overall Survival After Negative Margin Resection of Sinonasal Epithelial-Myoepithelial Carcinoma by Medha Venigalla, Vanshika Narala, Sharanya Thodupunoori, Samuel Auger and Christopher Roxbury in American Journal of Rhinology & Allergy
Footnotes
Ethical Approval
This study was deemed exempt by the University of Chicago Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the National Cancer Database (NCDB). Restrictions apply to the availability of these data, which were used under license for this study and are not publicly available. Data may be obtained from the NCDB through application and approval by the American College of Surgeons and the Commission on Cancer.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.