
Abstract
Background
Endoscopic sinus surgery (ESS) remains the gold standard for chronic rhinosinusitis, but complications such as adhesions, ostial stenosis, and poor mucosal healing occur. Chitosan-based nasal packs and gels have been proposed as adjuncts for their hemostatic and anti-adhesive properties.
Objective
To assess chitosan-based therapies after ESS.
Methods
Randomized trials comparing chitosan-based products with no treatment, standard care, or active comparators were included; active comparators included standard dressings or biomaterials, whereas no-treatment comparisons reflected split-nose designs. Outcomes were ostial area preservation and wound-healing parameters at final follow-up. Random-effects models pooled weighted mean differences (WMDs) for ostial outcomes and risk ratios (RRs) for binary outcomes.
Results
Ten randomized controlled trials were included (5 reporting ostial outcomes, up to 9 reporting binary outcomes). Six studies compared chitosan-based products with no treatment and 4 with active comparators. At final follow-up, chitosan-based products improved ostial area preservation versus no treatment (WMD = 18.3%, 95% confidence interval: 11.6-25.1%; P < .0001), with greater effects in the frontal (WMD = 23.9%) and sphenoid (WMD = 23.4%) than maxillary sinus (WMD = 9.1%; subgroup P = .027). Pooled analyses showed chitosan-based products reduced adhesions (RR = 0.36, P = .006) and crusting (RR = 0.67, P = .009). However, after stratification by comparator type, neither adhesions nor crusting remained significant in the no-treatment subgroup, whereas crusting remained significant only versus active comparators (RR = 0.64, P = .007). Chitosan-based products reduced infection versus no treatment (RR = 0.39, P = .002), but not versus active comparators.
Conclusions
Chitosan-based preparations may preserve frontal and sphenoidal but not maxillary ostial size and reduce infection when compared with no treatment. Reduced crusting was observed only with active comparators. Small subgroup sizes and limited head-to-head evidence do not support claims of superiority; given the cost of chitosan-based dressings, more RCTs are needed.
Keywords
Introduction
Endoscopic sinus surgery (ESS) has been the standard approach for sinus disease since the late 1980s. 1 Sinonasal debridement is recommended early to enhance symptom relief. 2 Residual air cells, adhesions, and the postoperative narrowing of the sinus openings are the most probable causes to hinder ESS success. Many perioperative strategies have been developed to expedite and enhance re-epithelialization and the restoration of ciliary function, while minimizing the risk of stenosis and adhesions. Regular endoscopic debridement, topical nasal steroids, and consistent nasal irrigation are advised by a number of clinicians. 3
Chitosan is a polysaccharide obtained by de-acetylating chitin, which is found in the exoskeletons of crustaceans. 4 Chitosan-based dressings use chitosan derivatives and have shown promising results as postoperative nasal dressings, including reducing adhesions and sinus ostial stenosis while acting as hemostatic agents. 5
Chronic rhinosinusitis (CRS) represents a substantial global health burden and remains prone to recurrence despite technically successful ESS, due to postoperative complications such as adhesions, stenosis, and delayed mucosal healing. These challenges have increased interest in the use of advanced biomaterials to improve surgical outcomes.
Given these limitations, chitosan-based gels and dressings have shown promise as postoperative nasal dressings because of their hemostatic, anti-adhesive, and anti-stenotic properties. This systematic review and meta-analysis aim to evaluate the efficacy of chitosan-based dressings in improving postoperative outcomes in patients undergoing ESS.
Materials and Methods
Protocol Registration
The present systematic review was registered in PROSPERO (CRD420251082092) on June 29, 2025. It adhered to PRISMA-P for protocol formulation and PRISMA 2020 reporting standards.
Search Strategy and Eligibility Criteria
A comprehensive search of Web of Science, PubMed (MEDLINE), Google Scholar, and CENTRAL was conducted up to July 2025. The detailed search strategy and study selection process are outlined in Figure 1.
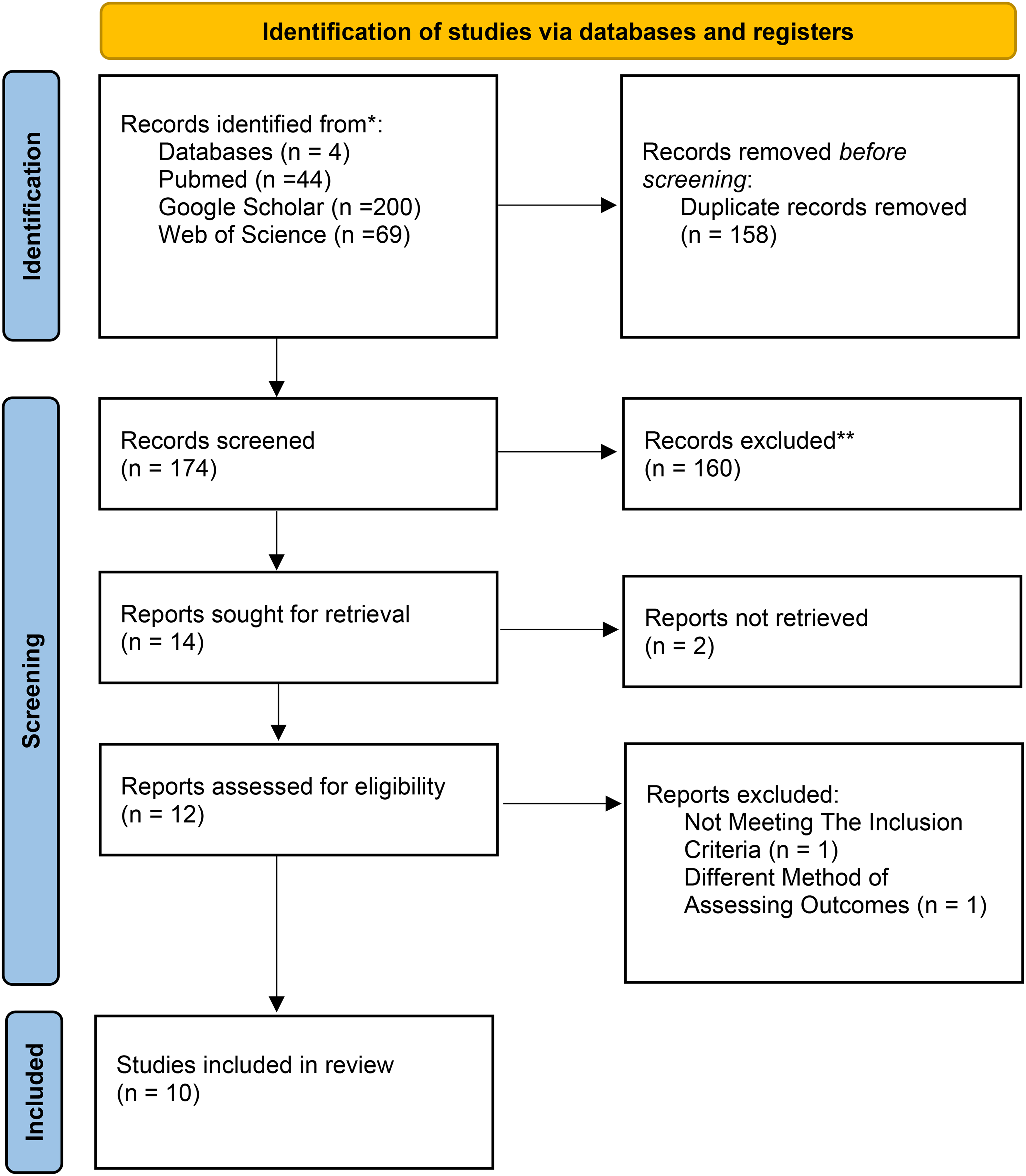
PRISMA flowchart.
Eligible studies included RCTs enrolling adults (≥18 years) with CRS undergoing ESS who received chitosan-based nasal packs and gels. Comparators included no intervention, placebo, or standard care, such as saline irrigation or nasal packing. Studies were required to report at least one postoperative outcome, including wound infection, adhesions, hemostasis, or adverse events. Non-randomized studies, pediatric populations, non-English publications, and non-original studies were excluded.
Data Extraction and Standardization
Wound-healing outcomes were extracted as binary events. Ostial measurements were standardized as a percentage of baseline area maintained. [Additional details can be found in Supplementary Methods S1].
Study Selection and Data Preparation
Recruitment periods, interventions, and study populations were examined to minimize the risk of overlapping patient cohorts among trials. For the primary meta-analysis, only the final reported follow-up time point per study was included for each outcome to ensure independence of observations and avoid repeated inclusion of the same study population across multiple postoperative time points.
Effect Size Calculation
Risk ratios (RRs) were calculated for binary outcomes using the Mantel-Haenszel method, with a continuity correction of 0.5 applied to studies with zero events in either arm. Weighted mean differences (WMDs), expressed in percentage points, were calculated for ostial area preservation at the final follow-up endpoint. Additional details are provided in Supplementary Methods S1.
Subgroup Analyses and Meta-Regression Analysis
Subgroup analyses were performed for ostial area preservation by anatomical site (frontal, sphenoid, and maxillary) using only the final reported postoperative endpoint from each study. For binary outcomes, pooled effects of chitosan-based dressings were estimated using data from the final follow-up endpoint, stratified by comparator type (no treatment vs active comparator). Comparator type was classified as either no treatment or an active comparator. “No treatment” generally referred to split-nose designs in which the contralateral side received no postoperative dressing or biomaterial. “Active comparator” referred to standard postoperative dressings or biomaterials with an intended therapeutic effect, such as nasal packing, peptide hydrogel, PureRegen gel, or other topical biomaterials. Subgroup interaction tests were used to evaluate whether treatment effects differed between strata. Additional model details are provided in Supplementary Methods S1.
Statistical Analysis
Random-effects meta-analyses were performed using restricted maximum likelihood. For continuous ostial outcomes, effect estimates were reported as WMDs, expressed in percentage points of ostial area preservation. For binary outcomes, effect estimates were reported as RRs with 95% confidence intervals (CIs). Statistical heterogeneity was evaluated using Cochran's Q statistic, I2, and τ2. Leave-one-out sensitivity analyses were undertaken to assess the robustness of pooled estimates derived from the final follow-up endpoint of each study. Potential publication bias or small-study effects were assessed using visual inspection of funnel plots and Egger's regression test. All analyses were conducted in R Version 4.3.0. Supplementary analyses based on standardized mean differences and all reported postoperative time points are presented in the Supplemental Material.
Results
A total of 332 records were identified through database and registry searches, of which 10 RCTs were included in the systematic review (Figure 1). Characteristics of the included studies are shown in Table 1.5–14 This systematic review included 10 RCTs (2010-2024) from Australia (n = 6), USA (n = 2), South Korea (n = 1), and Qatar (n = 1). Nine studies employed split-nose designs while one used parallel groups. Participants were adults with CRS refractory to medical therapy. The combined population had a mean age ranging from 39 to 55 years with slight male predominance (54%).
Characteristics of Included Studies.
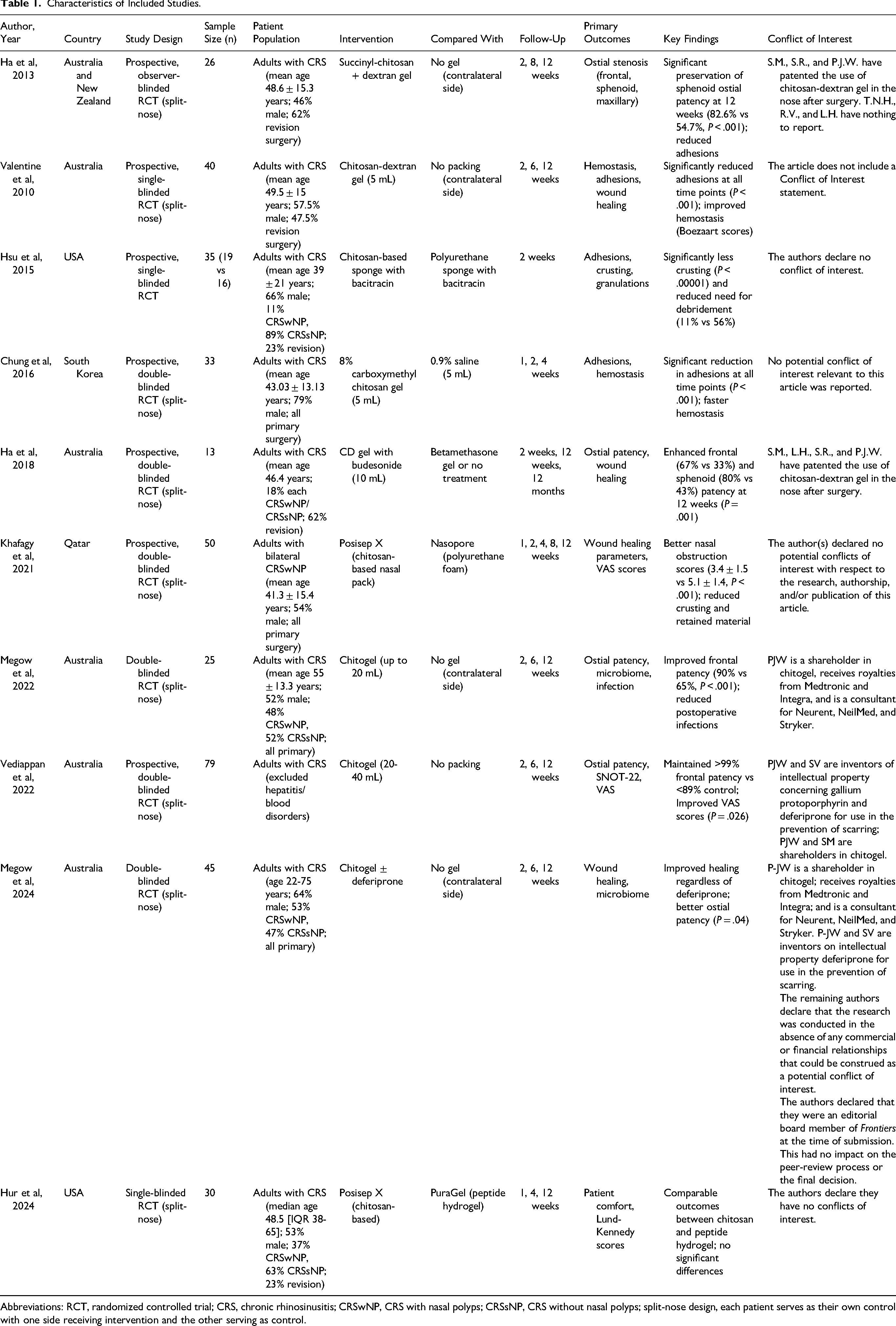
Abbreviations: RCT, randomized controlled trial; CRS, chronic rhinosinusitis; CRSwNP, CRS with nasal polyps; CRSsNP, CRS without nasal polyps; split-nose design, each patient serves as their own control with one side receiving intervention and the other serving as control.
Chitosan-based interventions varied across studies, including chitosan-dextran gels, chitosan-based nasal packs such as Posisep X and chitosan sponge, and carboxymethyl chitosan gel. Chitogel was the most frequently evaluated named product among the included studies. Ha et al (2018) uniquely combined chitosan with budesonide, while Megow et al (2024) added deferiprone. In no-treatment comparisons, the control side received no postoperative dressing or biomaterial in split-nose designs, whereas active-comparator studies used alternative packing materials or biomaterials.
Ostial Measurements
The pooled analysis demonstrated a statistically significant benefit of chitosan-based dressings for ostial area preservation (Figure 2), with arm-level pooled preservation of 84.4% in the chitosan group compared with 65.3% in the no-treatment group (WMD = 18.3 percentage points, 95% CI: 11.6-25.1, P < .0001; I2 = 65.2%), indicating a clinically meaningful advantage in favor of chitosan-based dressings. Heterogeneity was moderate (I2 = 65.2%, τ2 = 95.07, Q = 40.28, df = 14, P = .0002).
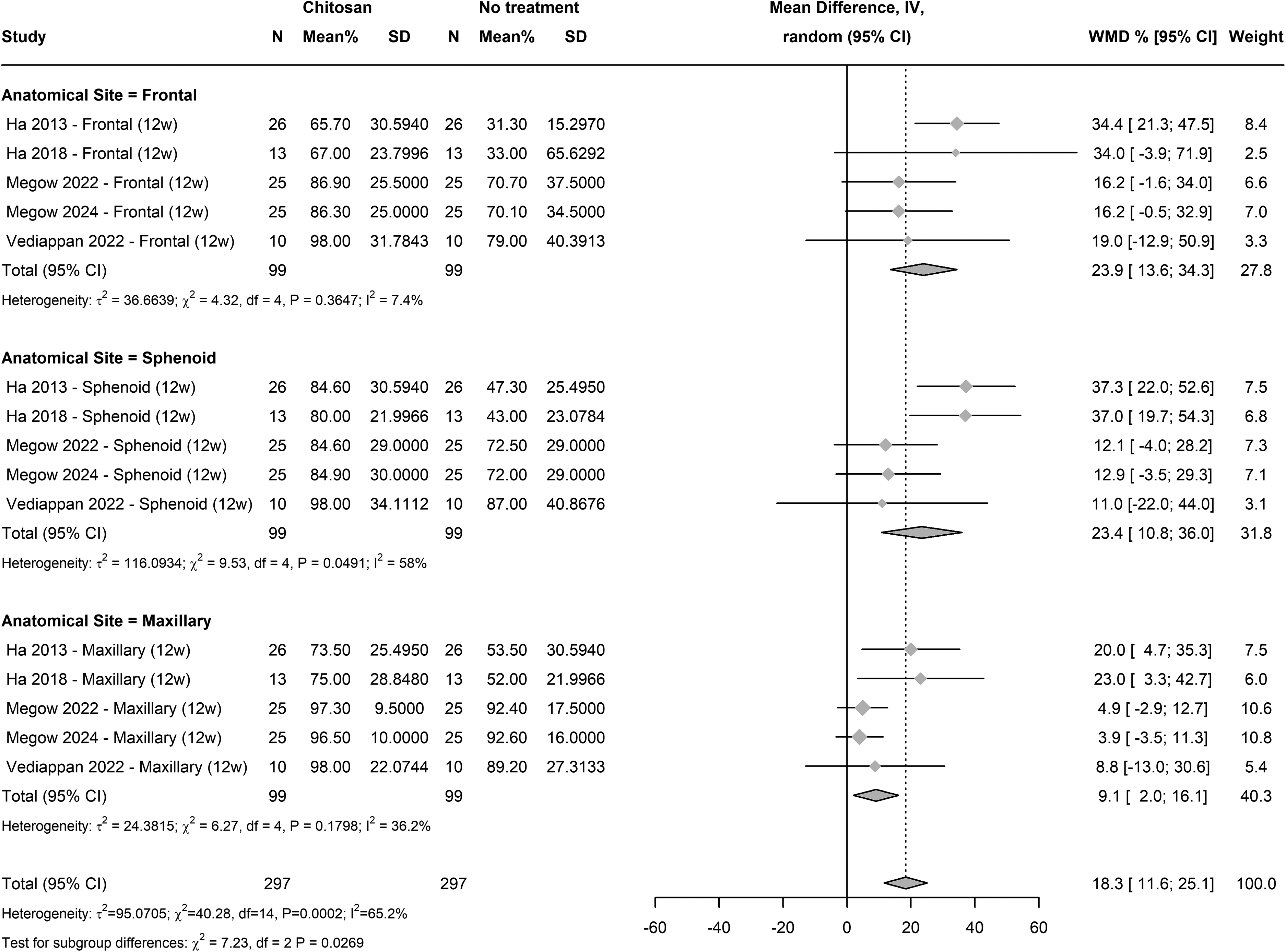
Weighted mean difference (%) in ostial area preservation at final follow-up for chitosan-based dressings versus no treatment, stratified by sinus site.
Egger's regression test indicated potential small-study effects (t = 2.34, df = 13, P = .036, bias estimate = 2.08, SE = 0.89), although this finding should be interpreted cautiously given the small number of contributing studies (k = 5). Visual inspection of the funnel plot for ostial outcomes (Supplementary Figure S2) suggested mild asymmetry, which should be interpreted cautiously given the small number of contributing studies. Funnel plots for binary outcomes are shown in Supplementary Figure S3.
The leave-one-out analysis demonstrated that the overall pooled effect of chitosan on ostial area preservation was stable. Exclusion of any single study did not materially change the effect size, with WMD consistently ranging between 16.6% and 20.0%, all of which remained statistically significant (P < .0001). The overall pooled estimate after leave-one-out was WMD = 18.3% (95% CI: 11.6-25.1%, P < .0001), identical to the main analysis. Supplementary sensitivity analyses including all reported postoperative time points yielded findings consistent with the primary final-endpoint analysis (Supplementary Figures S4-S6).
At final follow-up, chitosan-based dressings significantly improved ostial area preservation versus no treatment (WMD = 18.3%, 95% CI: 11.6-25.1%, P < .0001, I2 = 65.2%). Subgroup analysis demonstrated the greatest effect in the frontal sinus (WMD = 23.9%, 95% CI: 13.6-34.3%, I2 = 7.4%), followed by the sphenoid sinus (WMD = 23.4%, 95% CI: 10.8-36.0%, I2 = 58.0%). The maxillary sinus showed a smaller but statistically significant benefit (WMD = 9.1%, 95% CI: 2.0-16.1%, I2 = 36.2%). The test for subgroup differences was significant (P = .027), suggesting statistically reliable variation in treatment effect between anatomical sites, with larger effects in the frontal and sphenoid sinuses compared to the maxillary sinus.
Binary Outcomes
Subgroup Analysis by Comparator Type
When all 10 studies were pooled regardless of comparator type, chitosan-based dressings significantly reduced adhesions (RR = 0.36, 95% CI 0.17-0.75, P = .006) and crusting (RR = 0.67, 95% CI 0.49-0.91, P = .009) at the final follow-up endpoint. However, stratification by comparator type (Table 2) revealed that these pooled effects were driven primarily by comparisons with active dressings rather than no treatment alone. In the no-treatment subgroup, chitosan did not significantly reduce adhesions (RR = 0.39, 95% CI 0.14-1.07, P = .069) or crusting (RR = 0.88, 95% CI 0.40-1.95, P = .754), but did significantly reduce infection/pus formation (RR = 0.39, 95% CI 0.21-0.70, P = .002). In the active-comparator subgroup, chitosan significantly reduced crusting (RR = 0.64, 95% CI 0.46-0.89, P = .007) but not adhesions (RR = 0.36, 95% CI 0.08-1.50, P = .160) or infection (RR = 0.79, 95% CI 0.14-4.36, P = .784). Subgroup interaction tests were non-significant for all outcomes (all P > .05), indicating that the apparent differences between strata should be interpreted cautiously. No significant effects were observed for bleeding, granulation tissue, mucosal edema, postoperative debridement, or retained material in either stratum.
Pooled Effects of Chitosan-Based Dressings on Binary Postoperative Outcomes at the Final Follow-up Endpoint, Stratified by Comparator Type.
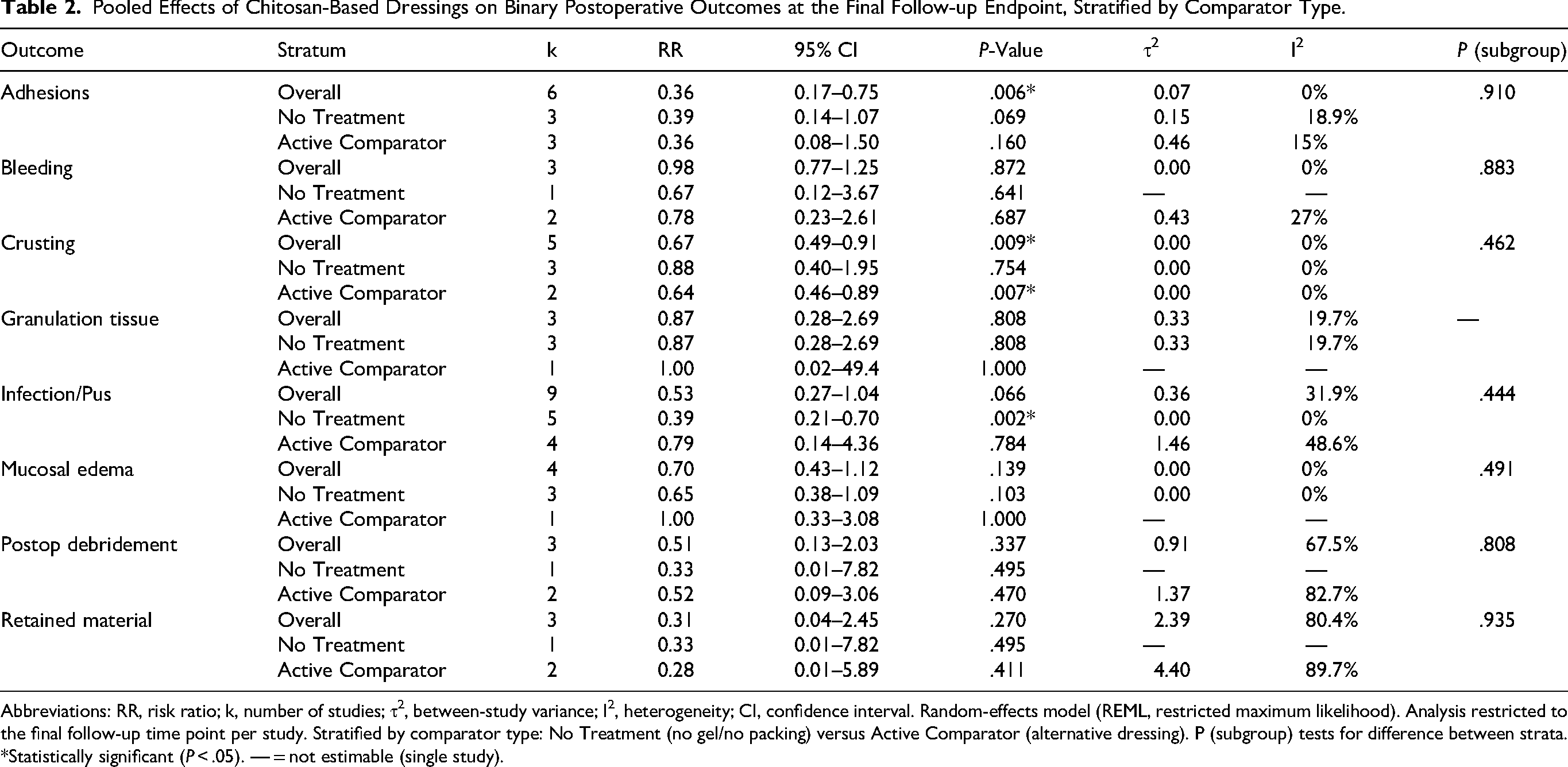
Abbreviations: RR, risk ratio; k, number of studies; τ2, between-study variance; I2, heterogeneity; CI, confidence interval. Random-effects model (REML, restricted maximum likelihood). Analysis restricted to the final follow-up time point per study. Stratified by comparator type: No Treatment (no gel/no packing) versus Active Comparator (alternative dressing). P (subgroup) tests for difference between strata.
*Statistically significant (P < .05). — = not estimable (single study).
Forest Plot for Adhesions, Bleeding, Crusting, and Granulation Tissue
Forest plots present pooled RR with 95% CIs for the effect of chitosan-based dressings on (a) adhesions, (b) bleeding, (c) crusting, and (d) granulation tissue at the final follow-up endpoint, stratified by comparator type (no treatment vs active comparator) (Figure 3). In the no-treatment subgroup, chitosan showed a non-significant trend toward reduced adhesions (RR = 0.39, 95% CI 0.14-1.07, P = .069) and no effect on crusting (RR = 0.88, 95% CI 0.40-1.95, P = .754) or bleeding (RR = 0.67, 95% CI 0.12-3.67, P = .641). In the active-comparator subgroup, chitosan significantly reduced crusting (RR = 0.64, 95% CI 0.46-0.89, P = .007) but not adhesions (RR = 0.36, 95% CI 0.08-1.50, P = .160) or bleeding (RR = 0.78, 95% CI 0.23-2.61, P = .687).
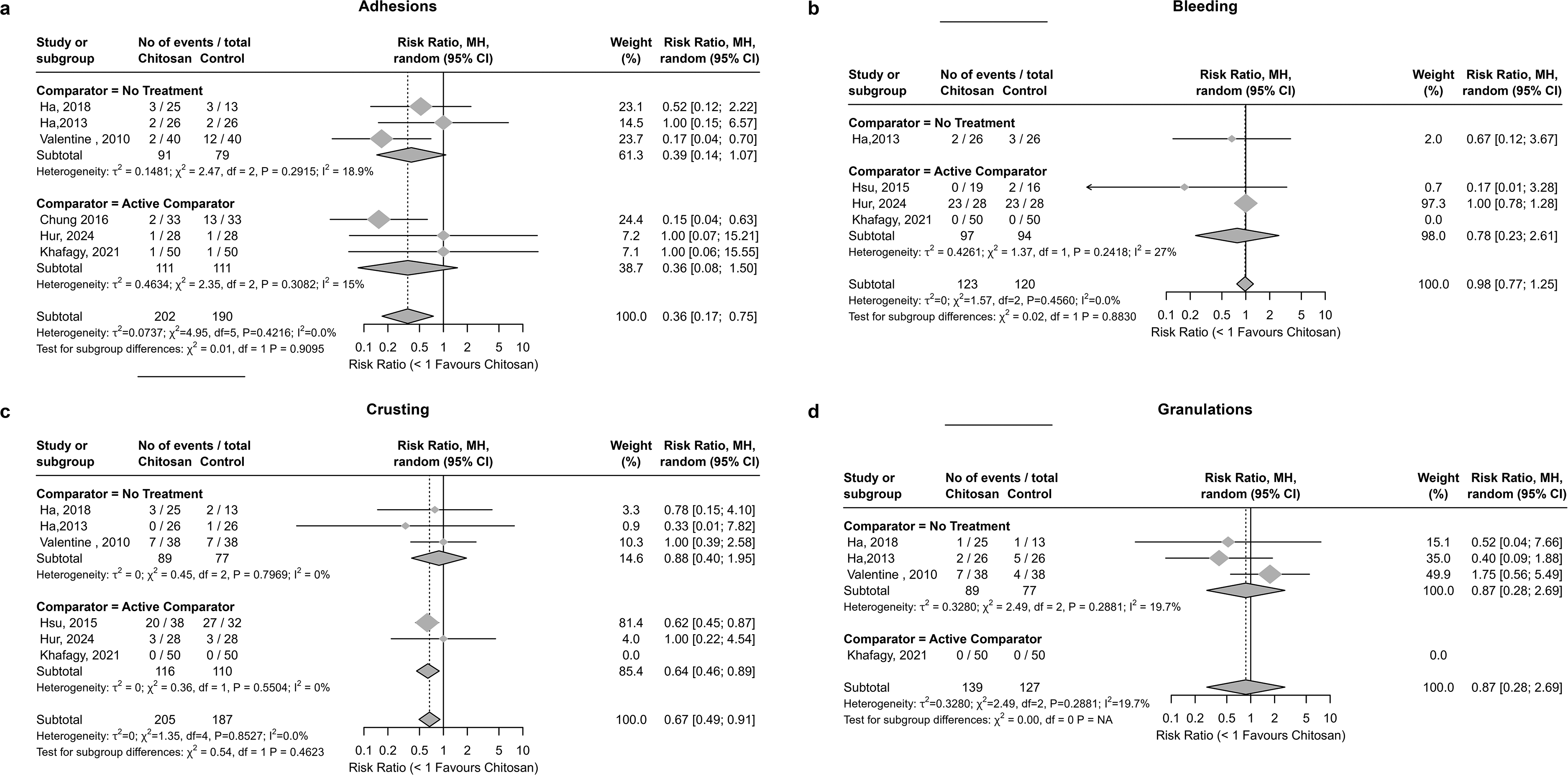
Forest plots of the effect of chitosan-based dressings on postoperative wound-healing outcomes (adhesions, bleeding, crusting, and granulation tissue) at the final follow-up endpoint, stratified by comparator type (no treatment vs active comparator).
Granulation tissue was not significantly affected by chitosan in either subgroup (no treatment: RR = 0.87, 95% CI 0.28-2.69, P = .808; active comparator: single study, RR = 1.00). Subgroup interaction tests were not significant for any of these 4 outcomes.
Forest Plot for Infection/Pus Formation, Mucosal Edema, Need for Debridement, and Retained Material
Forest plots present pooled RR with 95% CIs comparing chitosan-based dressings with controls for (a) infection/pus formation, (b) mucosal edema, (c) need for debridement, and (d) retained material at the final follow-up endpoint, stratified by comparator type (no treatment vs active comparator) (Figure 4). For infection/pus formation, chitosan significantly reduced risk in the no-treatment subgroup (RR = 0.39, 95% CI 0.21-0.70, p = .002; I2 = 0%), but not in the active-comparator subgroup (RR = 0.79, 95% CI 0.14-4.36, P = .784; I2 = 48.6%). For mucosal edema, chitosan showed a non-significant trend toward reduction in the no-treatment subgroup (RR = 0.65, 95% CI 0.38-1.09, P = .103) with only a single active-comparator study available (RR = 1.00).
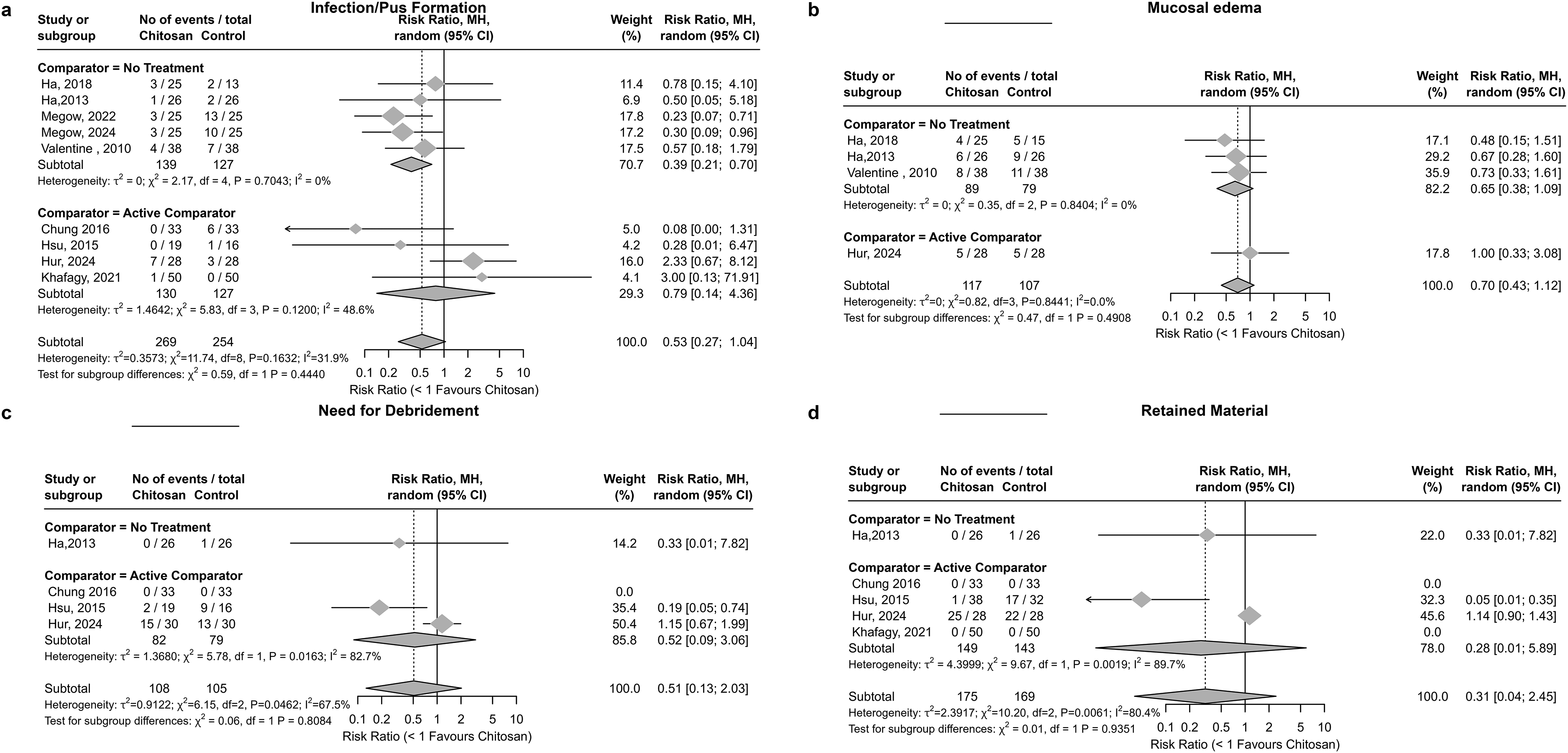
Forest plots of the effect of chitosan-based dressings on postoperative infection/pus formation, mucosal edema, need for debridement, and retained material at the final follow-up endpoint, stratified by comparator type (no treatment vs active comparator).
For postoperative debridement, neither subgroup showed a significant effect (no treatment: RR = 0.33, P = 0.495; active comparator: RR = 0.52, P = .470), with substantial heterogeneity in the active-comparator stratum (I2 = 82.7%). Retained material was also non-significant in both strata (no treatment: RR = 0.33, P = .495; active comparator: RR = 0.28, P = .411), with high heterogeneity (I2 = 89.7% in the active-comparator subgroup). Subgroup interaction was non-significant for all 4 outcomes.
Discussion
This systematic review and meta-analysis suggest that chitosan-based dressings may offer postoperative benefits, particularly in preserving ostial patency when compared with no treatment. However, the evidence base remains limited: all 5 ostial studies compared chitosan-based products with no treatment alone (none with an active comparator), and 6 of 10 included trials originated from a single research group.6–10,15 An important distinction emerged when binary outcomes were stratified by comparator type: the pooled benefits for adhesions and crusting were driven primarily by studies using active-comparator dressings, not by studies comparing chitosan-based products with no treatment alone.
Ha et al demonstrated chitosan-dextran gel preserved larger ostial areas at 12 weeks compared with no treatment, 6 with further enhancement of ostial area preservation at 12 months. 11 Megow et al reported that Chitogel was associated with improved wound-healing, reduced infection rates, and postoperative microbiome changes. 7 Chitosan-based dressings have been associated with reduced revision surgery rates and significant cost savings, suggesting potential health-economic advantages. 15 Our findings build on earlier trials, though most evidence derives from a single center. The absolute improvement of 18.3% in ostial area preservation (WMD = 18.3%, 95% CI: 11.6-25.1%; P < .0001) is clinically important, considering that restenosis is a leading cause of surgical failure. Site-specific analyses demonstrated the strongest effect in the sphenoid sinus, which concurs with the results provided by Ha et al6,11 The analysis aligns with the hypothesis that chitosan-based dressings may be most beneficial in regions where postoperative stenosis poses the greatest risk of surgical failure. Ostial area preservation should also be interpreted with consideration of differences in outcome assessment across studies. Although measurements were standardized as percentage area preserved from baseline, differences in measurement techniques, follow-up timing, and anatomical sites assessed may limit direct comparability. Importantly, all studies contributing to ostial area preservation compared chitosan-based products with no treatment, most often in split-nose designs; therefore, these findings cannot be interpreted as evidence of superiority over active postoperative dressings or biomaterials.
While chitosan-based dressings appear most notable in preventing adhesion formation and ostial stenosis, benefits on other postoperative outcomes were not consistently demonstrated. Importantly, when studies were stratified by comparator type, the significant pooled effect on adhesions did not persist in either the no-treatment (P = .069) or active-comparator (P = .160) subgroup. For crusting, the effect remained significant in the active-comparator subgroup (RR = 0.64, P = .007) but not in the no-treatment subgroup (P = .754), suggesting that this benefit may reflect a relative advantage over other dressings rather than over no intervention. The only outcome that was statistically significant in the no-treatment subgroup was infection/pus formation (RR = 0.39, P = .002), suggesting that chitosan's antimicrobial properties may represent its most robust benefit when compared with no postoperative intervention.7,11
However, it is noteworthy that the majority of the comparisons have been made with no treatment, not with standard of care dressings. In addition, there have been limited head-to-head trials with other dressings (eg, PureRegen). These have not shown any clear evidence of superiority. For example, in the most recent study by Cavada et al, published in 2025, the authors conducted a double-blind randomized controlled trial of Chitogel with topical corticosteroid versus PureRegen gel in terms of wound-healing and postoperative outcomes. The need for more head-to-head trials with existing alternatives is clear. The high cost of chitosan dressings warrants further prospective randomized controlled trials to establish the superiority and cost-effectiveness of these dressings. 16
The strengths of this review include a comprehensive search and standardized data extraction. Our results expand on earlier reviews of chitosan-based dressings in ESS, such as Khafagy et al, 11 by incorporating recent high-quality RCTs and exploring anatomical and temporal moderators.
It is important to note that the pooled analysis showed significant reductions in adhesions and crusting. The findings related to adhesions were inconsistent in leave-one-out sensitivity analysis and lost significance in both strata upon stratification by comparator type. Crusting remained significant in the active-comparator subgroup but not in the no-treatment subgroup, suggesting that this benefit may reflect an advantage over alternative dressings rather than a consistent advantage over no treatment.
Clinically, chitosan-based dressings may serve as an adjunct in ESS, particularly for patients at high risk of restenosis. However, the ostial patency data derive exclusively from comparisons with no treatment (k = 5, all from one research group), and no active-comparator data exist for this outcome. For binary outcomes, benefits appear contingent on the choice of comparator: the strongest evidence for a direct clinical benefit over no treatment was limited to infection reduction (k = 5, RR = 0.39, P = .002), while many subgroup estimates relied on very few studies (k = 1-3), limiting the reliability of stratum-specific conclusions.
A potential limitation of our review is that 6 of 10 included studies originated from a single research group (Australian/Wormald group) with declared industry affiliations, raising the possibility of patient overlap. However, no duplicated cohorts across trials were identified. Notably, all 5 studies contributing to ostial area preservation originated from this group, used the same product (Chitogel), and compared against no treatment. Sensitivity analyses excluding industry-affiliated studies did not materially alter pooled estimates for binary outcomes. Therefore, the risk of bias from overlap is considered minimal. Future studies should include large, multicenter, RCTs with standardized outcome, longer follow-up periods, and direct comparisons with alternative adjuncts, such as steroid-eluting stents. Mechanistic studies evaluating its interaction with the sinonasal microbiome and wound-healing pathways could help clarify which patient subgroups are most likely to benefit. Additionally, product type (chitosan gel vs nasal pack) was nearly completely confounded with comparator type: all gel studies (Ha 2020, Valentine 2010, Athanasiadis 2008, Vediappan 2022, Megow 2022, Cavada 2025) used no-treatment comparators, whereas all nasal pack studies (Hsu 2015, Khafagy 2021, Chung 2016, Hur 2024) used active-comparator dressings. As a consequence, the effects of product formulation and comparator type cannot be disentangled.
Conclusion
In conclusion, this systematic review suggests that chitosan-based dressings may improve ostial area preservation compared with no treatment, particularly in the sphenoid and frontal sinuses, although this finding is based on a small number of studies (k = 5) that all compared chitosan-based products with no treatment and originated predominantly from a single research group. Overall, the current evidence for chitosan-based dressings is constrained by small-study numbers, predominant reliance on no-treatment comparators, and concentration within a single research group. Large, multicenter, independently funded head-to-head trials comparing chitosan-based products with established postoperative dressings or biomaterials are essential before firm clinical recommendations can be made.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924261457275 - Supplemental material for The Effect of Chitosan-Based Dressings on Postoperative Outcomes in Patients Undergoing Endoscopic Sinus Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ajr-10.1177_19458924261457275 for The Effect of Chitosan-Based Dressings on Postoperative Outcomes in Patients Undergoing Endoscopic Sinus Surgery: A Systematic Review and Meta-Analysis by Ahmed K. Almukhlifi, Abdullah O. Almutairi, Lara S. Alansari, Osama B. Alharbi, Reema A. Almutairi, Ahmed H. Alkhaldi, Sarah K. Alkhorayef and Nayef S. Alkhazi in American Journal of Rhinology & Allergy
Footnotes
Ethical Considerations
Ethical approval and informed consent were not required because this study is a secondary analysis of previously published data.
Authorship Contribution
AA contributed to conceptualization, data extraction, data organization, proofreader, and project administration. AA contributed to methodology, writing the original draft (Introduction, Discussion, Conclusion), and reference arrangement. OA contributed to study screening, data extraction, and cover letter preparation. LA contributed to data extraction, data organization, and resource management. AA contributed to data extraction. RA contributed to data extraction and risk of bias assessment. SA contributed to abstract writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No new data were created or analyzed in this study. All data used in this systematic review and meta-analysis were extracted from previously published studies, which are cited within the article. Data sharing is therefore not applicable to this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.