
Abstract
Objectives
Sinonasal metastases are far rarer than primary sinonasal malignancies, hence seldom reported or analyzed in existing literature. To address these gaps, we have retrospectively analyzed 35 patients with sinonasal metastasis in a single university hospital in South Korea, over a 24-year period.
Methods
From 1998 to 2022, among 11,814 pathology reports of sinonasal tissues, 35 (0.3%) were identified with sinonasal metastasis from solid organ cancers. Patients' clinical characteristics, presentation, primary tumor profiles, treatment modalities for the sinonasal metastasis, and overall survival (OS) were retrospectively reviewed and analyzed, in addition to the literature review.
Results
Hepatocellular carcinoma (HCC) was the most common primary cancer (37.1%), followed by lung (14.3%), breast (11.4%), and thyroid (8.6%). The most common presentation was epistaxis (20%), however, 20% were identified incidentally. The nasal cavity (37.1%), sphenoid and maxillary sinus (31.4%), and skull base (34.3%) were the most prevalent metastatic locations. Although the median OS following a sinonasal metastatic diagnosis was 7.0 months, patients with isolated sinonasal metastasis, thyroid cancer- metastases, or definitive therapy for sinonasal metastasis had significant longer OS (p=0.037, 0.035, and p-trend=0.003, respectively).
Conclusion
In our study, HCC was the most common primary cancer for sinonasal metastasis, contrasting with renal cell carcinoma prevalence in Western literature, suggesting that regional cancer incidence variations may influence sinonasal metastasis epidemiology. Despite the poor prognosis in general, in selected patients with thyroid cancer or solitary sinonasal metastases, the definitive treatment for the sinonasal metastasis may aid in an increased duration of survival.
Introduction
Cancer metastasis to the sinonasal cavity is extremely rare; they are far less common than original sinonasal malignancies, which themselves account for only a small percentage of head and neck cancers.1–4 Due to its exceptional rarity, the clinical characteristics, demographic profiles, etiological factors, treatment approaches, and outcomes of sinonasal metastasis remain poorly defined, in contrast to primary sinonasal malignancies, for which therapeutic strategies and prognostic outcomes are well-established. 1 The existing literature on sinonasal metastasis primarily consists of isolated case reports and small series, highlighting a significant gap in comprehensive studies or systematic analyses.5–11 In the practice of otorhinolaryngology, although rare, clinicians may occasionally encounter patients suspected of having cancer metastasize to the sinonasal cavity, particularly during consultations with individuals who have a history of cancer.1–3 Nonetheless, the limited evidence in the existing literature challenges physicians, particularly in establishing management strategies and understanding clinical outcomes that remain largely unexplored, underscoring a critical need for further research in this area.
Historically, the understanding of sinonasal metastases was initially reported in the publications by Bernstein et al in 1966 and Friedmann et al in 1965, who were the first to document instances of these rare occurrences in the USA and UK, respectively.12,13 However, their reports were based on the presentation of a small case series of sinonasal metastatic cancers, not including any analysis of clinical or oncologic features, treatment strategies, or clinical outcomes.12,13 Furthermore, these reports predominantly focused on Western populations and were published several decades ago, which limits their applicability to the global population in the 2020s. More recently, two publications from Asia, specifically case series analyses of 17 sinonasal metastases in Taiwan by Huang et al (2008) and Chang et al (2019), have provided more detailed insights into the nature and outcomes of these conditions.2,3 Documenting 17 cases each, these studies offered valuable clinical presentations and perspectives but were limited by their relatively short study durations, absence of survival outcomes and associated factors, and small sample sizes.2,3 These limitations underscore the need for more extensive research that incorporates significant survival-related factors and longer study periods to provide a more comprehensive analysis of the epidemiological and clinical features of sinonasal metastasis.
To address this scholarly gap, the authors conducted a comprehensive investigation of sinonasal metastasis at a single academic university hospital over a 24-year period. Utilizing a retrospective cohort of 35 patients, our study analyzed the oncological profiles and metastasis patterns of sinonasal metastasis, along with previously unexplored aspects such as cancer surveillance, survival outcomes, and prognostic factors that will enhance the understanding of various cancer metastasis to the sinonasal region, in addition to the literature review.
Materials and Methods
Study Subjects Inclusion and Exclusion Criteria
Patients who received a histological diagnosis of metastatic cancer to the sinonasal cavity originating from solid organ cancers at the authors’ Medical Center from January 1998 through February 2022 were retrospectively reviewed and included in the study. During this 24-year period, a total of 11,814 biopsy tissue pathology reports from the sinonasal cavity, including the nasal cavity, nasal septum, paranasal sinuses, nasopharynx, skull base including the anterior cranial fossa (ACF), and nasal vestibule, were obtained. Patients with sinonasal metastases originating from hematolymphoid malignancies and mucosal malignant melanoma were excluded. 14
Data Curation: Clinical Manifestations and Oncological Profiles
For the 35 patients included in the final analysis for the retrospective cohort analysis, a confirmed diagnosis of sinonasal metastasis was made based on the pathologist's report from the obtained specimens. Demographic, clinical, radiological, and oncological data were collected, which included information on the primary cancer and its staging at the time of recurrence. Following the diagnosis, therapeutic interventions administered to the metastatic lesions were reviewed and categorized as definitive, palliative, or supportive care. Additionally, a literature review of the past studies on sinonasal metastasis was conducted, especially focusing on the primary cancer sites of sinonasal metastasis with providing the cancer incidence of each cancer incidence obtained from the national cancer database for the mean year of each study's inclusion period.15–18
Statistical Analysis
For all 35 sinonasal metastasis patients, descriptive statistics were analyzed to describe the demographic, clinical, and oncological characteristics of sinonasal metastasis. To analyze survival depending on several oncological characteristics, a Kaplan-Meier curve was depicted to analyze the median duration of survival following sinonasal metastasis diagnosis, and the significance of the survival outcomes was analyzed using a log-rank test, providing the hazard ratio (HR) with 95% confidence interval (CI). A P-value of less than 0.05 was considered significant, and all analysis was bi-directional.
Results
Patient Demographics, Clinical Presentations, and Primary Cancer Profiles
From January 1998 to February 2022, metastatic cancer of the sinonasal cavity, including the ACF skull base, was diagnosed in 35 (0.3%) of 11,814 patients undergoing biopsies of the sinonasal area. The median age at diagnosis was 54 years, with a predominance of male (65.7%) compared with female (34.3%) patients (Table 1). A significant majority (80%) presented with symptoms warranting otorhinolaryngology consultations or radiographic evaluations, with the most common being epistaxis (20.0%), nasal obstruction (11.4%), and headaches (17.9%), followed by facial pain and numbness (8.6% each). Notably, 20% of the cases were asymptomatic, identified incidentally during initial staging work-ups (5.7%), or routine cancer surveillance (14.3%). Most metastatic lesions were unilateral (85.7%).
The Demographical, Clinical, and Oncological Outcomes of Patients with Sinonasal Metastasis.
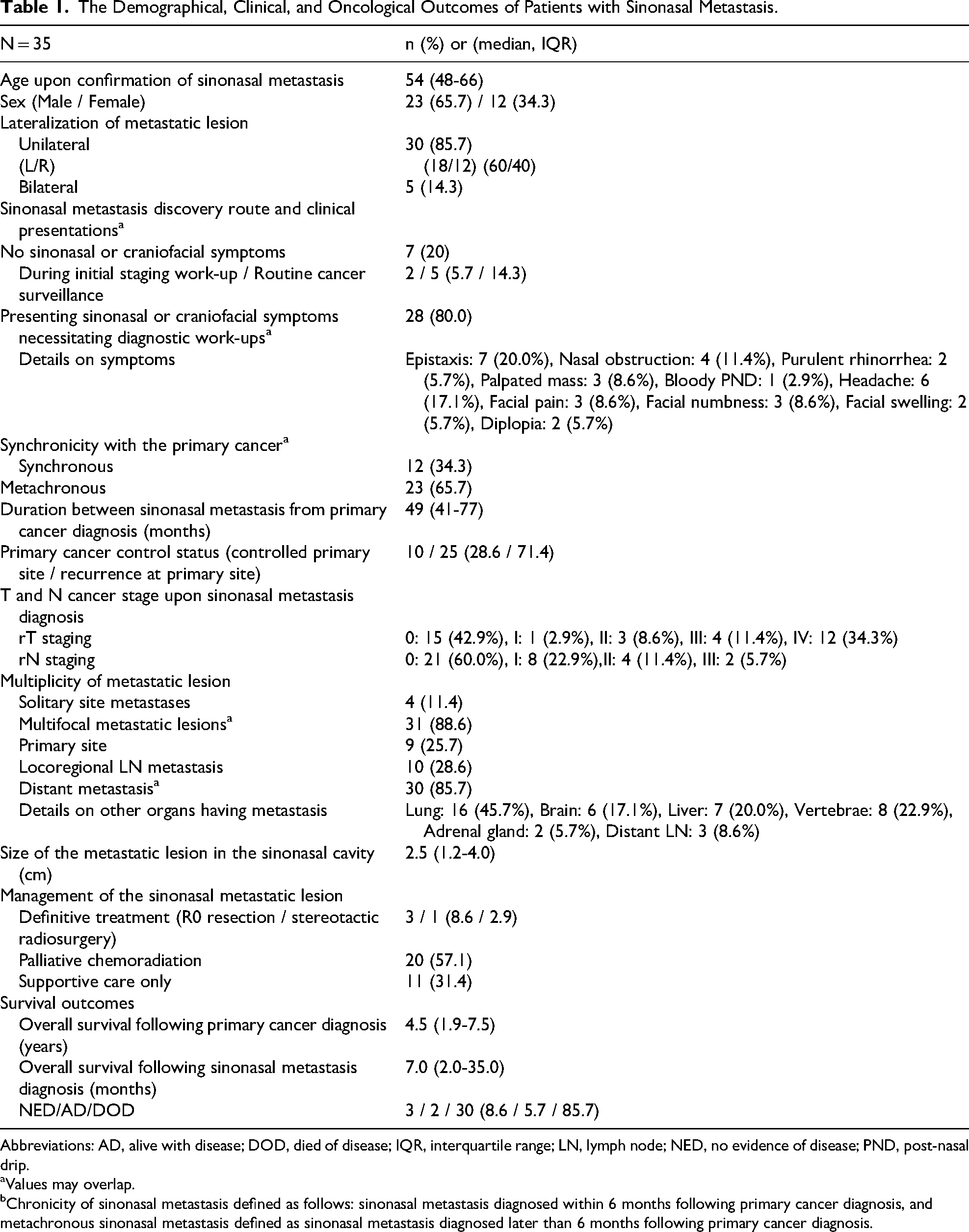
Abbreviations: AD, alive with disease; DOD, died of disease; IQR, interquartile range; LN, lymph node; NED, no evidence of disease; PND, post-nasal drip.
Values may overlap.
Chronicity of sinonasal metastasis defined as follows: sinonasal metastasis diagnosed within 6 months following primary cancer diagnosis, and metachronous sinonasal metastasis defined as sinonasal metastasis diagnosed later than 6 months following primary cancer diagnosis.
The liver was the most common primary site for sinonasal metastases, accounting for 37.1% of cases, as shown in Figure 1A. Lung cancer, breast cancers, and gastrointestinal (GI) cancers followed, contributing to 14.2%, 11.4%, 11.4%, respectively. Of lesser frequency, kidney and thyroid gland cancers accounted for both 8.6%. Hepatocellular carcinoma (HCC) emerged as the predominant histological type, representing 37.1% of these cases, followed by adenocarcinoma and invasive ductal cell carcinoma at 22.8% and 11.4%, respectively (Figure 1B). All the cancers that originated from the kidney was renal cell carcinoma (RCC), and among 3 (8.6%) patients with thyroid cancer sinonasal metastasis, 2 patients (5.7%) were diagnosed with papillary thyroid carcinoma (PTC) and 1 patient (2.9%) with follicular thyroid carcinoma. The nasal cavity and the ACF skull base were the most frequently affected sites in 37.1% and 34.3% of patients, respectively (Figure 2). The sphenoid and maxillary sinuses each showed metastatic involvement in 31.4% of cases, with the nostril and anterior ethmoid sinus affected in 17.1% of cases each.
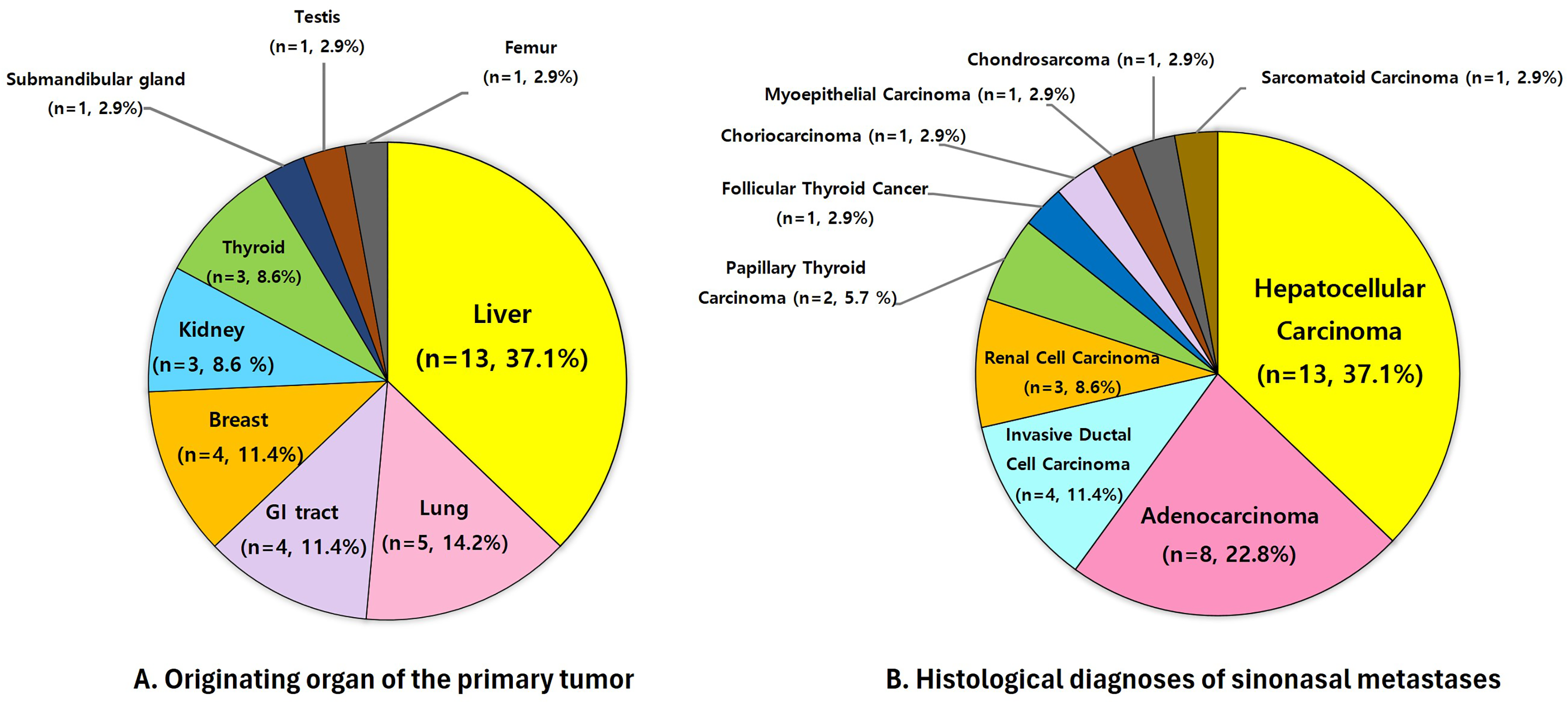
Distribution of primary tumor origins and histological types in sinonasal metastases (n = 35). (A) Originating organ of the primary tumor: pie chart illustrating the distribution of primary tumor origins in patients with sinonasal metastases, highlighting the liver as the most common source. (B) Histological diagnoses of sinonasal metastases: pie chart showing the histological subtypes of the tumors metastasizing to the sinonasal region, with hepatocellular carcinoma (HCC) being predominant.
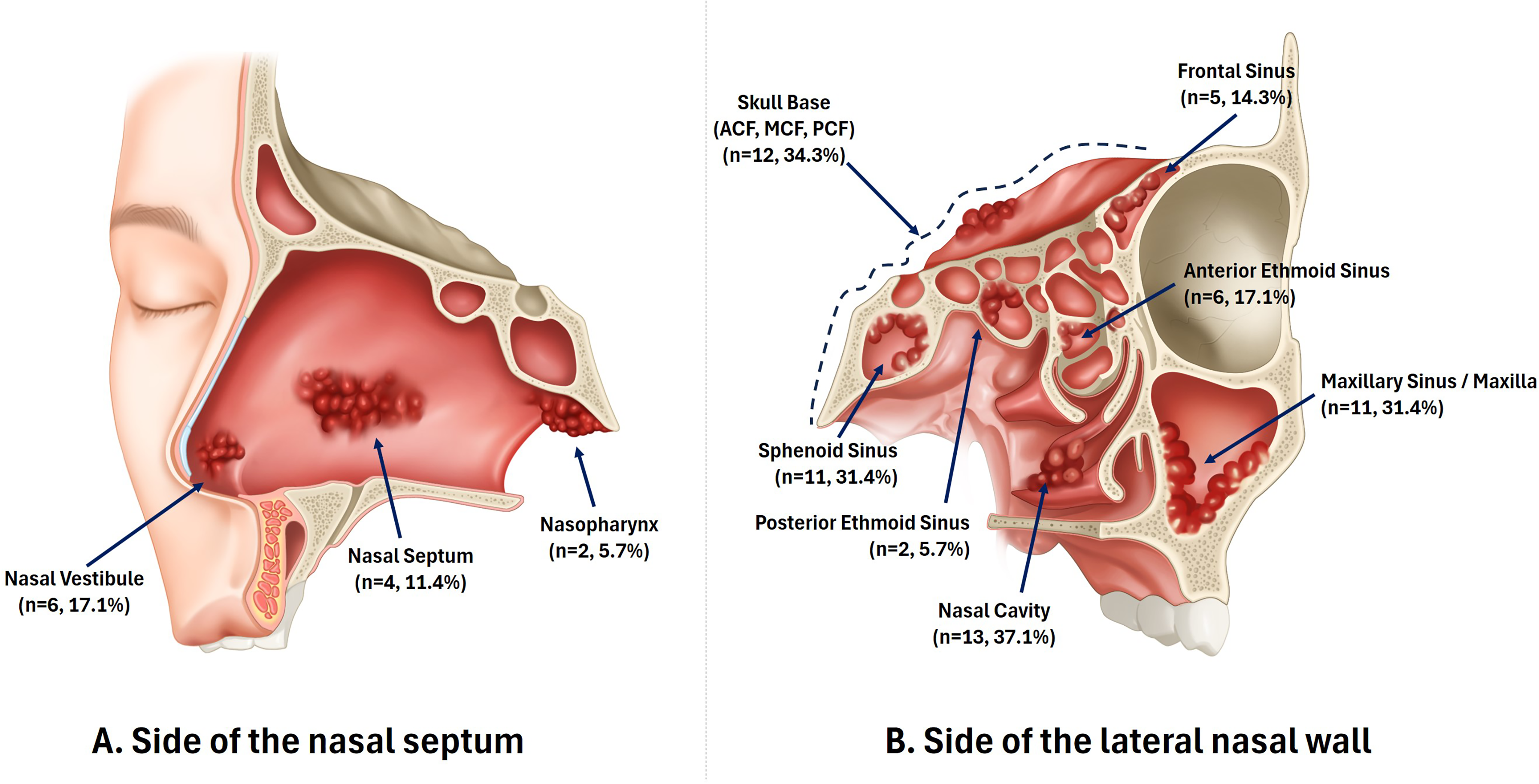
Anatomical localization of sinonasal metastases (n = 35). Detailed anatomical illustrations depicting common sites of sinonasal metastases, showing the distribution of metastases within the nasal cavity, nasal septum, nasal vestibule, nasopharynx, anterior cranial fossa (ACF), skull base, and the paranasal sinuses, including the sphenoid, posterior ethmoid, anterior ethmoid, maxillary, and frontal sinuses.
Regarding the timing of sinonasal metastasis lesion detection, 34.3% were classified as synchronous, being diagnosed within 6 months following the initial primary cancer diagnosis, whereas 65.7% were identified as metachronous, detected more than 6 months after primary cancer detection (Table 1). The median interval between the primary cancer diagnosis and the identification of sinonasal metastasis was 49 months, approximately 4 years. At the time of diagnosis, 71.4% of patients had a recurrence of their primary cancer. In contrast, 28.6% showed no recurrence at the primary site but had distant metastases, including in the sinonasal region. Most metastatic lesions were multifocal, accounting for 88.6% of cases. Conversely, a small number of patients (11.4%) presented with solitary site metastases confined to the sinonasal area.
Radiographic review of CT and/or MR images demonstrated frequent osseous involvement or bony change in sinonasal metastases, observed in 24 patients (68.6%) (Table 2). The most common findings were bony destruction in 13 (37.1%), followed by cortical bony erosion in 5 (14.3%), expansile or remodeling-type bony change in 2 (5.7%), and an osteoblastic lesion in 1 (2.9%); according to primary cancer type, osseous involvement was observed in all breast cancer metastases, 9 of 13 HCC, 3 of 5 lung cancer, 2 of 3 RCC, and 2 of 3 thyroid cancer cases. The most frequent internal imaging finding was an enhancing soft-tissue mass or mucosal thickening in 27 patients (77.1%), followed by heterogeneous, mixed, rim, or well-enhancing patterns in 9 (25.7%), necrotic, cystic, or low-attenuation components in 8 (22.9%), and calcification in 2 (5.7%). Extension beyond the primary sinonasal compartment was also common, including adjacent soft-tissue extension in 15 patients (42.9%), orbital or periorbital extension in 6 (17.1%), and intracranial or dural extension in 6 (17.1%).
Radiographic Characteristics of Sinonasal Metastases Shown on CT and/or MR Images.
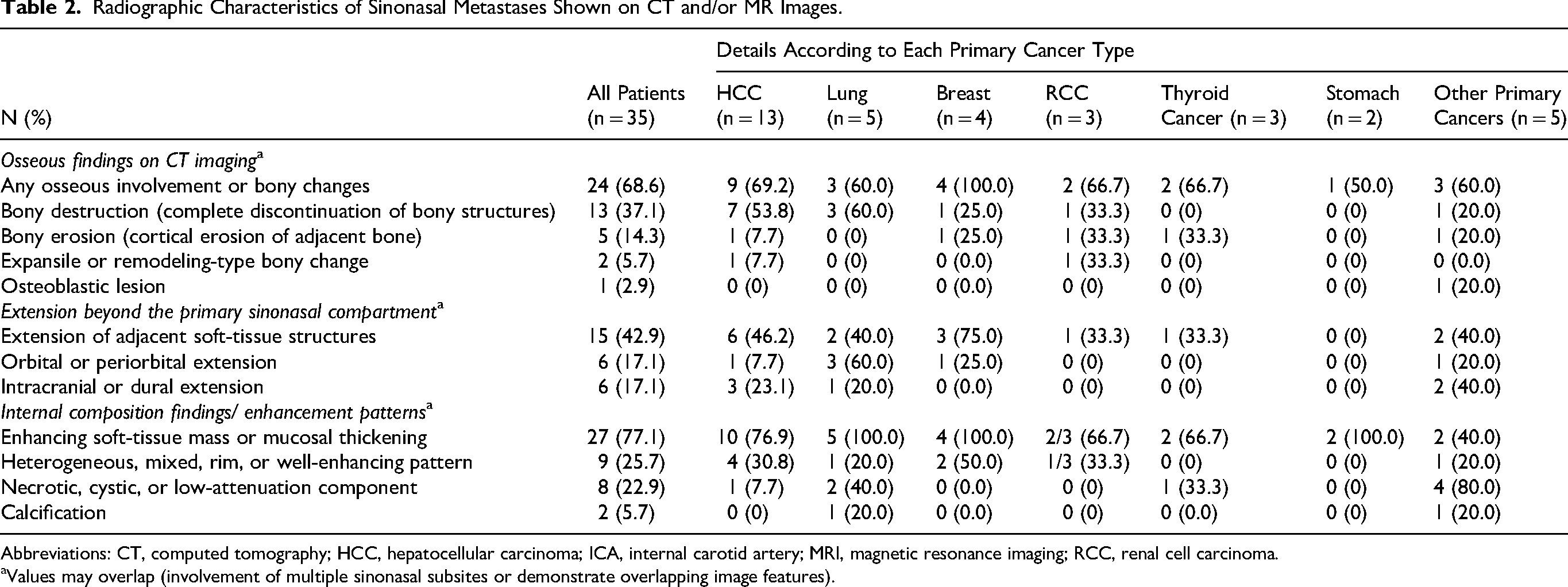
Abbreviations: CT, computed tomography; HCC, hepatocellular carcinoma; ICA, internal carotid artery; MRI, magnetic resonance imaging; RCC, renal cell carcinoma.
Values may overlap (involvement of multiple sinonasal subsites or demonstrate overlapping image features).
Treatment and Survival Outcomes
Following sinonasal metastasis diagnosis, 11.4% of patients in good general condition received definitive treatments, including surgical resection with negative margins (8.6%) and gamma-knife radiosurgery (2.9%) (Table 1). The majority, however, could not fully eradicate their metastatic tumors and received either palliative chemoradiation (57.1%) or supportive care only (31.4%), often owing to heavy tumor burden or poor general health.
The treatment modality of 4 patients who underwent local ablative treatment of sinonasal metastatic lesions is further outlined in Supplementary Table 1. Case #1 was a 67-year-old female with a history of advanced-stage PTC previously treated with total thyroidectomy, modified radical neck dissection, retropharyngeal lymph node resection, radioactive iodine (RAI) therapy at 150 mCi, and external-beam radiotherapy at 66 Gy. 15 years after primary cancer treatment, a solitary right posterior sphenoid sinus metastasis with bony erosion and cavernous sinus involvement was detected incidentally. The patient's sinonasal metastasis was treated with CyberKnife stereotactic radiosurgery at 20 Gy in 2 fractions, in consideration of prior irradiation history and proximity to critical skull base structures. No additional RAI was given because of absent I131 uptake on radioiodine whole-body scanning. However, 5 years later, recurrence later developed in the sphenoid sinus and retropharyngeal/cervical nodes, and the patient eventually died of the disease.
Case #2 was a 46-year-old male with synchronously diagnosed PTC, and an incidentally detected 1.2-cm protruding right posterior septal/choanal metastasis without bony invasion, for which endoscopic R0 resection was performed with concurrent total thyroidectomy and central lymph node dissection followed by RAI therapy at 30 mCi, and the patient remained without evidence of disease.
Case #3 was a 68-year-old male who underwent total hepatectomy with concurrent liver transplantation for HCC, later developed pulmonary and hard-palate metastases treated with pulmonary resection and R0 hard-palate resection, and subsequently developed a 2.7-cm expansile heterogeneously enhancing left maxillary sinus metastasis with adjacent bony destruction that was treated with medial maxillectomy with R0 resection, followed 1 year later by infrastructure maxillectomy for local recurrence at the inferior margin of the previous maxillectomy site, after which the sinonasal cavity remained controlled but pulmonary metastasis recurred and the patient died of disease despite sorafenib treatment.
Case #4 was a 44-year-old female with clear-cell RCC previously treated with nephrectomy who later developed multiple brain and pulmonary metastases treated with pazopanib and stereotactic radiotherapy to the brain lesion at 35 Gy in 5 fractions, and then presented 6 months later with complete unilateral nasal obstruction and intractable epistaxis caused by metastatic RCC filling the right nostril and nasal cavity. Although multiple metastatic lesions were present in other organs, endoscopic endonasal ablation was performed as a palliative local-control measure to control epistaxis and restore nasal breathing, followed shortly thereafter by R0 excision via a lateral rhinotomy approach because of progression with invasion of the nostril skin and nasal vestibule, but ipsilateral cheek recurrence and progressive pulmonary metastases later developed despite adjuvant cabozantinib and palliative systemic therapy, and the patient died of disease soon thereafter.
Overall survival (OS) outcomes were generally poor, with most patients (85.7%) dying from the disease. The median OS following a sinonasal metastasis diagnosis was 7 months, in contrast to 4.5 years from the primary cancer diagnosis. Of note, patients with a single metastatic site experienced significantly better outcomes than those with multiple metastases, showing a median survival of 27 months versus 5 months (HR of 2.43, 95% CI of 1.05-5.60), (P = 0.037) (Figure 3). Furthermore, patients receiving definitive treatments (HR of 7.28, 95% CI of 1.97-26.9), (P = 0.003) and palliative treatment (HR of 3.46, 95% CI of 1.29-9.21), (P = 0.013) showed significantly longer OS than in patients only receiving supportive care, showing median OS of 45 months, compared with 12 months and 2 months for those receiving palliative and supportive care, respectively (p-trend = 0.003). Additionally, the type of primary cancer had a significant effect on survival rates; patients with thyroid cancer demonstrated an increase in the OS, with a median OS of 65 months versus 7 months for those with other types of cancers (HR of 2.83, 95% CI of 1.08-7.43), (P = 0.035).
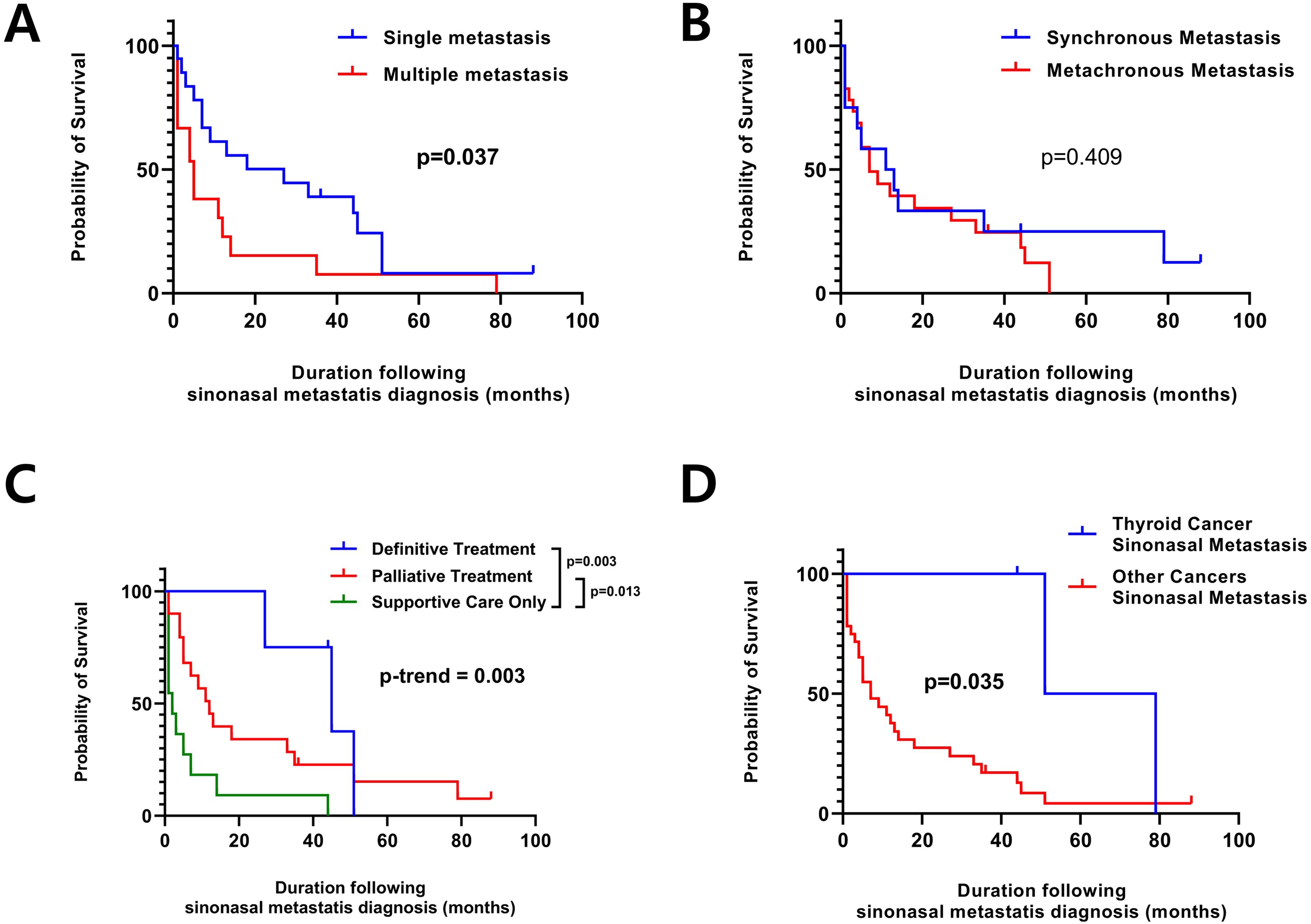
Overall survival outcomes and Kaplan-Meier curves comparing survival probabilities based on various oncologic profiles and treatment modalities in patients with sinonasal metastases. (A) Single sinonasal metastasis showing significant improved survival compared with multiple metastases upon presentation (P = 0.037). (B) Synchronous versus metachronous metastasis, showing no significance in survival difference. (C) Survival based on treatment modalities, demonstrating a significant survival gain among patients receiving definitive treatment for the sinonasal metastasis, compared with palliative treatment, and supportive measurement only (P = 0.004). (D) Survival comparison by primary cancer type: compares survival outcomes for patients with thyroid cancer-related sinonasal metastases shows better survival outcome, compared with other cancer types (P = 0.035).
Primary Organ Sinonasal Metastasis
In Supplementary Table 2, sinonasal metastasis arising from various solid organ primary cancers are presented, along with the number of each primary cancer reported in the previously published literatures with more than 15 case series globally, as well as each study's national cancer database. HCC and thyroid cancer sinonasal metastasis were more prevalent in the East Asian regions, specifically in Korea and Taiwan, but not in the USA or UK. By contrast, RCC, lungs, breast, and testicular cancer sinonasal metastasis are relatively more frequently reported in Western countries.
Discussion
In our study, the liver was the most common primary site of origin for sinonasal metastasis, as HCC accounted for 35% of cases, followed by lung, GI tract, and breast cancers. Of interest, this predominance of liver cancer and the relatively rare identification of RCC sinonasal metastasis (9%) contrast with findings from Western countries, such as the USA, UK, and France.1,4,12,13,19 In Western countries, RCC and breast cancer are more commonly identified as major primary sites for sinonasal metastasis, with no reported cases of HCC sinonasal metastasis.1,4,12,13,18 This discrepancy likely reflects demographic, epidemiological, and genetic predisposition differences between Western and Asian populations, which exhibit distinct cancer incidence patterns. One contributing factor to the higher proportion of HCC sinonasal metastasis in our study may be the endemic presence of the hepatitis B virus in South Korea over many decades, a known cause of chronic hepatitis, liver cirrhosis, and HCC. 19 In addition, the notably high incidence of thyroid and stomach cancers in South Korea may explain the increased proportion of sinonasal metastasis from these cancers observed in our data, compared with studies from regions with lower incidences of these cancers.20,21
Previous research has identified the maxillary sinus as the most commonly affected site for sinonasal metastasis, followed by the sphenoid, ethmoid, frontal sinuses, and nasal cavity.2–4,12,13,19 Consistent with these findings, our study found that the maxillary and sphenoid sinuses were the most frequently affected paranasal sinuses, each accounting for 31.4% of cases. Metastases in the head and neck regions are known to follow pathways along the meningeal venous plexus situated along the skull base and the roof of the paranasal sinuses, which could account for our finding that 34.3% of metastases occurred at the ACF skull base and sphenoid sinus (31.4%), making it one of the most common locations in our study. 22 The high rate of metastasis to the maxillary sinus (31.4%) in our study is likely owing to its extensive vascularization from branches of the external carotid artery that communicate with the pterygoid plexus, particularly in cancers such as RCC or HCC, which are known for their high propensity for hematogenous spread. 23
In our cohort, sinonasal metastasis was associated with poor prognosis, with a median survival of 7 months after diagnosis. Most patients received palliative chemoradiation (57.1%) or supportive care (31.4%) due to poor general condition. Although limited by small numbers, our findings suggest that definitive local therapy may prolong survival in selected patients, aligning with the ICAR: sinonasal tumors consensus recommending surgery or stereotactic radiosurgery for highly selected cases. 1 As shown in Figure 3, markedly longer survival occurred in patients with isolated sinonasal metastasis, particularly from thyroid carcinoma. Four (11.4%) patients underwent definitive local treatment; three surgical resections and one radiosurgery, all with solitary lesions (two PTC, one RCC, one HCC). Among them, three died of disease and one survived, with a mean post-diagnosis survival of 45 months, suggesting potential benefit of aggressive local therapy in carefully chosen cases.
Although these findings may not be universally applicable to all patients with sinonasal metastasis, definitive resection of the sinonasal metastasis may be particularly accepted and applied in some selected cases. Therefore, in consultations regarding solitary sinonasal metastasis, especially in thyroid cancer sinonasal metastasis, a broader indication for definitive surgical interventions may be warranted. Evaluating oncological factors alongside the patient's overall condition could potentially enhance survival outcomes and even offer a chance for a definitive cure, as evidenced by 8.6% of our patients achieving no evidence of disease status and 5.7% alive with disease with definitive measures. Consequently, a multidisciplinary approach involving oncologists, otorhinolaryngologists, neurosurgeons, radiation oncologists, and radiologists is advisable. This approach facilitates the careful selection of patients who may benefit from a definitive resection of the sinonasal metastatic lesion and underscores the need for further research in this area.
To elucidate global variations in sinonasal metastasis epidemiology, Supplementary Table 1 summarizes previous literature comprising studies or case series with more than 15 cases.15–18 Cross-regional comparison of data from Taiwan, the USA, and the UK revealed distinct metastatic tendencies among primary cancers, independent of regional incidence.3,13,24,25 Despite their low prevalence, RCC and testicular cancers appeared repeatedly among sinonasal metastases, indicating a high metastatic propensity.3,13,24,25 HCC sinonasal metastasis occurred almost exclusively in East Asian populations, paralleling the regional predominance of HCC and its near absence in Western cohorts. Previous reports also corroborate these findings, showing hematogenous spread of HCC via the portal vein and of RCC through the renal veins and inferior vena cava, explaining their predisposition to sinonasal dissemination.26–30 Although rare, testicular cancer demonstrated disproportionately frequent sinonasal involvement, with seminoma spreading lymphatically to the neck and brain, and choriocarcinoma and yolk-sac tumors metastasizing hematogenous to brain and bone, respectively.31–34 The sinonasal region's dense vasculature and complex bony labyrinth likely contribute to its exceptional susceptibility to metastasis.
Our study offers novel insights but has inherent limitations. Inclusion was confined to pathologist-confirmed sinonasal metastases, possibly excluding undiagnosed cases and reducing the sample size. The retrospective nature spanning 1998 to 2022 introduces temporal bias due to evolving diagnostic imaging, surgical methods, and chemotherapy, may have influenced the detection and outcomes of these patients. 35 Although national incidence data were considered, institutional differences in patient volume, settings, and multidisciplinary protocols may have introduced selection bias. Given the rarity of sinonasal metastasis, future multicenter collaborations are needed to refine understanding and optimize management.
Conclusion
Although sinonasal metastasis is rare and often asymptomatic, it may develop from various primary cancers, most commonly from HCC in our data. Despite the extremely low incidence of primary RCC and testicular cancers, their consistent association with sinonasal metastasis across studies suggests a distinct metastatic propensity to the sinonasal cavity. Although generally having poor prognosis, it may be favorably altered in selected patients, particularly those with isolated or thyroid cancer sinonasal metastases, through definitive treatment of the metastatic lesion.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924261457745 - Supplemental material for Cancer Metastasis to the Sinonasal Cavity: Clinical Characteristics and Survival Analysis in 35 Patients
Supplemental material, sj-docx-1-ajr-10.1177_19458924261457745 for Cancer Metastasis to the Sinonasal Cavity: Clinical Characteristics and Survival Analysis in 35 Patients by Marn Joon Park, Yeong Ju Lee, Ji Heui Kim, Yoo-Sam Chung and Myeong Sang Yu in American Journal of Rhinology & Allergy
Footnotes
Ethics Statement
This study was approved by the institutional review board (IRB) of Asan Medical Center (Investigation No. 2021-1838).
Patient Consent Statement
The IRB approved the waiver of informed consent, owing to the retrospective design of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.