
Abstract
Background
The frontal sinus drainage pathway (FSDP) includes the frontal recess as its most anatomically complex segment, where surrounding cell pneumatization can influence drainage patterns. Despite this variability, large-scale 3-dimensional characterization of the drainage pathway in both opacified and nonopacified sinuses remains limited, particularly with operative validation.
Objective
To perform 3-dimensional mapping of the FSDP and evaluate its relationship to adjacent cells, focusing on drainage patterns associated with frontal sinus opacification.
Methods
This single-center cross-sectional study analyzed 1008 frontal sinuses using 3-dimensional computed tomography reconstruction software. Frontal recess cells were classified according to the International Frontal Sinus Anatomy Classification. The course of the FSDP relative to adjacent cells was mapped and compared between opacified and nonopacified sinuses. A subset of 112 opacified sinuses that underwent endoscopic frontal sinus surgery was included for surgical validation, with preoperative mapping correlated with intraoperative findings.
Results
The FSDP most frequently coursed posterior to the agger nasi cell (63.9%). In the presence of supra-agger cell and supra-agger frontal cell, it predominantly followed a medial course (55.3% and 68.7%, respectively). It consistently ran anterior to supra-bulla cell (100%), lateral to frontal septal cell (100%), and most commonly anterior to supra-bulla frontal cell and supraorbital ethmoid cell (79.7% and 97.3%, respectively). Pathway–cell relationships did not differ between opacified and nonopacified groups. Preoperative 3-dimensional mapping showed high intraoperative concordance.
Conclusion
This study demonstrates that the anatomical configuration of the FSDP is largely consistent across both opacified and nonopacified sinuses. These findings provide a structured 3-dimensional anatomical framework that may assist preoperative assessment and surgical orientation in endoscopic frontal sinus surgery.
Keywords
Introduction
The frontal sinus drainage pathway (FSDP) comprises the frontal infundibulum, frontal ostium, and frontal recess, through which mucus drains from the frontal sinus. Its most complex segment lies within the frontal recess, where configuration depends on the presence and pneumatization patterns of surrounding cells. Even when individuals share the same frontal cell pattern, the FSDP may vary depending on the extent and direction of cell pneumatization, resulting in anatomical variability.
Previous studies have focused on identifying frontal recess cells and reporting their prevalence using 2-dimensional computed tomography (CT), and the International Frontal Sinus Anatomy Classification (IFAC) provides a standardized framework for categorization. Most investigations have evaluated the distribution of these cells and compared their occurrence between inflamed and noninflamed sinuses rather than directly characterizing the course of the FSDP.1–4 Studies systematically describing the FSDP in relation to adjacent cells remain scarce.
Furthermore, the 3-dimensional spatial configuration of the FSDP and its relationship with surrounding cells have not been comprehensively characterized, particularly with respect to their stability under inflammatory conditions. A thorough understanding of these spatial anatomical relationships is essential for accurate preoperative planning, as it enables surgeons to anticipate the drainage pathway, navigate complex frontal recess anatomy with greater confidence and tailor surgical strategies to individual patients.
In this study, we employed the IFAC system to categorize frontal cells and used 3-dimensional CT reconstruction to evaluate frontal cells and the FSDP in a large cohort. We determined cell prevalence, mapped the FSDP 3-dimensional course, and analyzed associations between cell configurations, FSDP anatomy, and sinus opacification. A subset of surgically treated cases was included to assess intraoperative concordance with preoperative mapping and provide anatomical validation.
Methods
Study Design and Ethics
This single-center cross-sectional study analyzed DICOM data from 1008 frontal sinuses in 2024. Institutional ethics approval was obtained (No: 03/GCN-BVTMH), and informed consent was secured from all participants.
This study was designed as a CT-based anatomical analysis. Clinical data, including patient symptoms, inflammatory endotypes, and comorbidities, were not collected as part of the study protocol. The focus was limited to structural evaluation of the FSDP.
Patient Selection and Imaging Acquisition
CT scans from 504 adult patients with clinical and endoscopic features of chronic rhinosinusitis were analyzed. Among 1008 frontal sinuses, 375 demonstrated opacification. All scans were acquired using a Siemens CT scanner with 0.8-mm axial slice thickness. Data were analyzed separately for each side. Exclusion criteria included massive unilateral or bilateral nasal polyposis, frontal sinus aplasia, head trauma, nasal or paranasal sinus tumors, and prior frontoethmoidal surgery.
Three-Dimensional Reconstruction and Anatomical Assessment
Stryker Building Blocks software (version 3.6.0; Stryker Leibinger GmbH & Co. KG, Germany), validated as a preoperative planning tool for frontal sinus surgery,5–7 was used for data analysis. The software generated 3-dimensional reconstructions enabling continuous tracing of the FSDP in multiplanar views. Two independent rhinologists drew blocks representing frontal cells and traced the frontal sinus outflow tract. Disagreements were resolved by joint image review until consensus was reached.
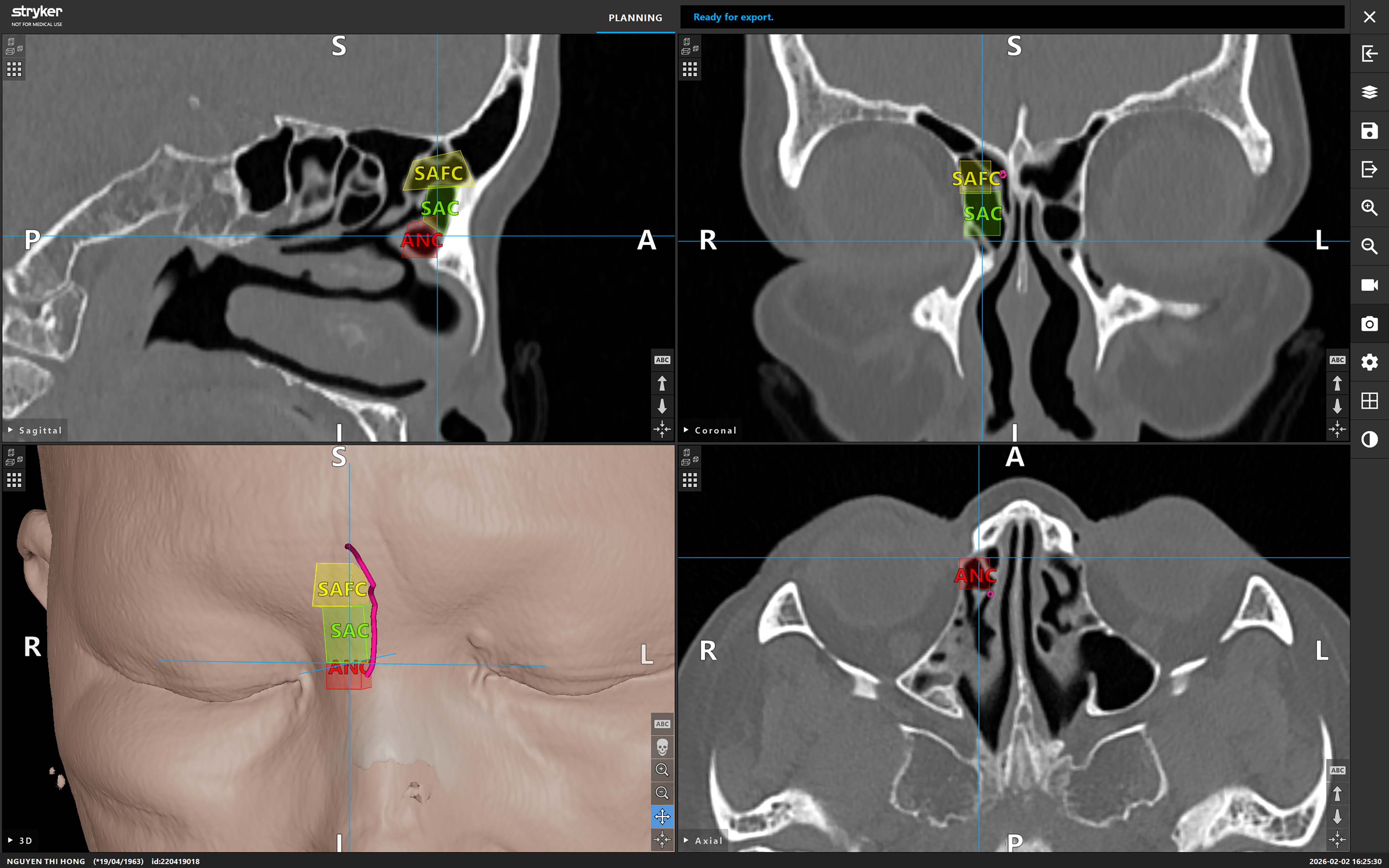
Frontal sinuses were categorized into 2 groups: opacified and nonopacified. The following cells were identified, labeled, and color-coded: ethmoid bulla cell (BE), agger nasi cell (ANC), supra-agger cell (SAC), supra-agger frontal cell (SAFC), supra-bulla cell (SBC), supra-bulla frontal cell (SBFC), supraorbital ethmoid cell (SOEC), frontal septal cell (FSC). A curved pink line representing the FSDP was drawn through the identified cells and adjusted in triplanar CT views. The course of the drainage pathway relative to the frontal cells and its relationship with each individual cell were analyzed (Figure 1).
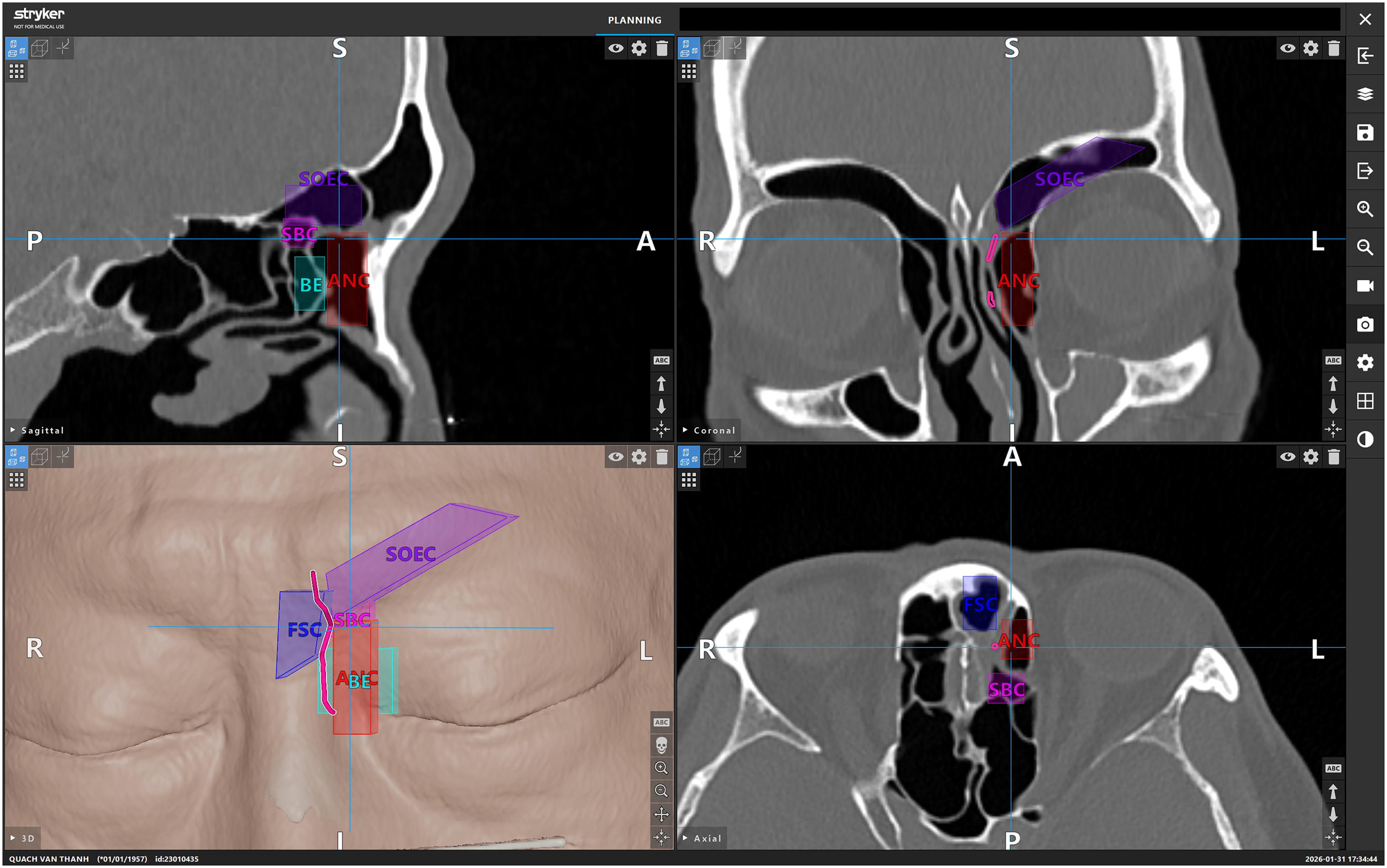
Stryker building blocks interface demonstrating labeled frontal recess cells and the drainage pathway (curved line) of the left frontal sinus in sagittal (upper left), coronal (upper right), axial (lower right), and 3-dimensional views (lower left).
Surgical Validation
A subset of 112 opacified frontal sinuses undergoing endoscopic frontal sinus surgery was included for surgical validation. Preoperative 3-dimensional mapping delineated frontal recess anatomy and the anticipated drainage pathway. Reconstructions were reviewed preoperatively to guide individualized planning and dissection. In anatomically complex or technically challenging cases, image-guided surgery was used to enhance localization of frontal cells and confirm the mapped FSDP course. During surgery, frontal cells and the FSDP were identified according to the preoperative 3-dimensional plan, and findings were documented. Concordance was defined as agreement between preoperative 3-dimensional mapping and intraoperative findings regarding accurate identification of frontal cells and correct delineation of the FSDP relative to these cells.
Statistical Analysis
Continuous variables are presented as means ± standard deviations, and categorical variables as frequencies and percentages. A P-value < .05 was considered statistically significant.
Results
Study Population and Demographics
We reviewed 1008 frontal sinuses from 504 patients, including 375 opacified sides (37.2%). Patient age ranged from 16 to 94 years (mean 45.8 ± 14.8), with a female-to-male ratio of approximately 1:1.
Frontal Recess Cells
The prevalence of each frontal cell is listed in Table 1. Apart from ANC (95.4%), SAC was the most common anteriorly based cell, accounting for 26% of sides. Among posteriorly based cells, SBC was the most prevalent (65.1%), whereas SBFC was the least common (6.4%).
Association Between Frontal Recess Cells and Frontal Sinus Opacification.
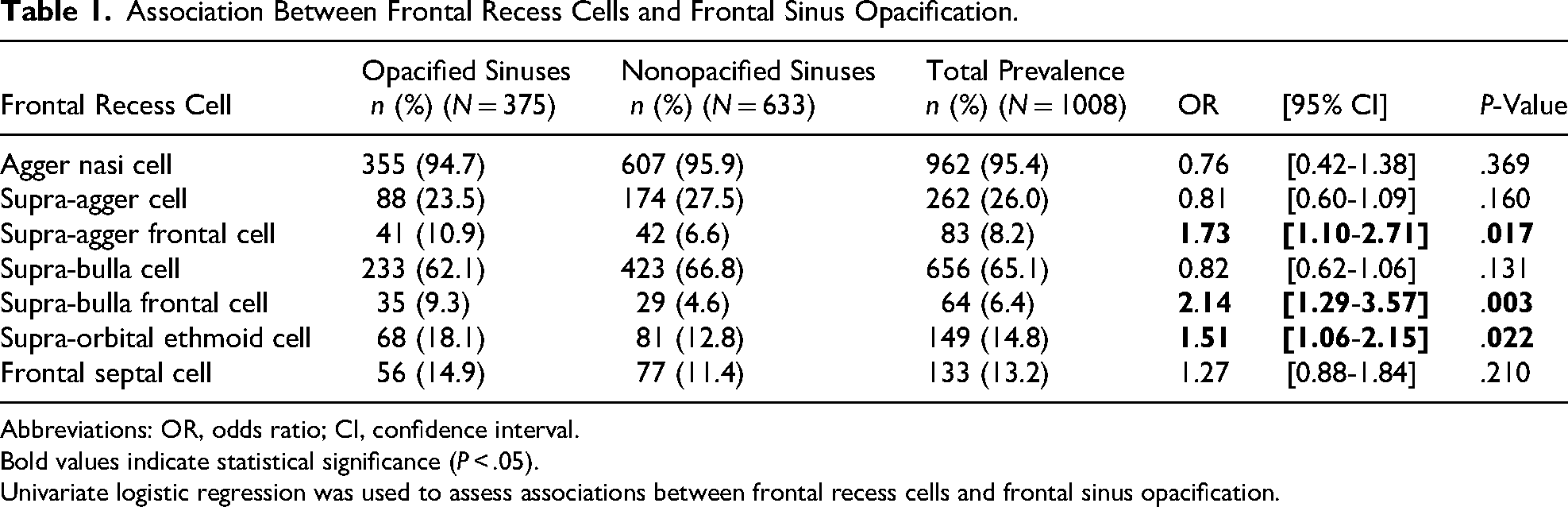
Abbreviations: OR, odds ratio; CI, confidence interval.
Bold values indicate statistical significance (P < .05).
Univariate logistic regression was used to assess associations between frontal recess cells and frontal sinus opacification.
The prevalence of SAFC, SBFC, SOEC differed significantly between opacified and nonopacified groups (Table 1). No significant differences were observed for ANC, SAC, SBC, or FSC.
Concurrent Frontal Recess Cell Groups
When frontal cells were analyzed according to the number of concurrently present IFAC groups, no significant association was observed between frontal sinus opacification and the presence of 0, 1, or 2 cell groups (P > .05). However, the simultaneous presence of all 3 cell groups was significantly associated with frontal sinus opacification (P = .011) (Table 2).
Association Between the Number of Concurrent Frontal Recess Cell Groups and Frontal Sinus Opacification.
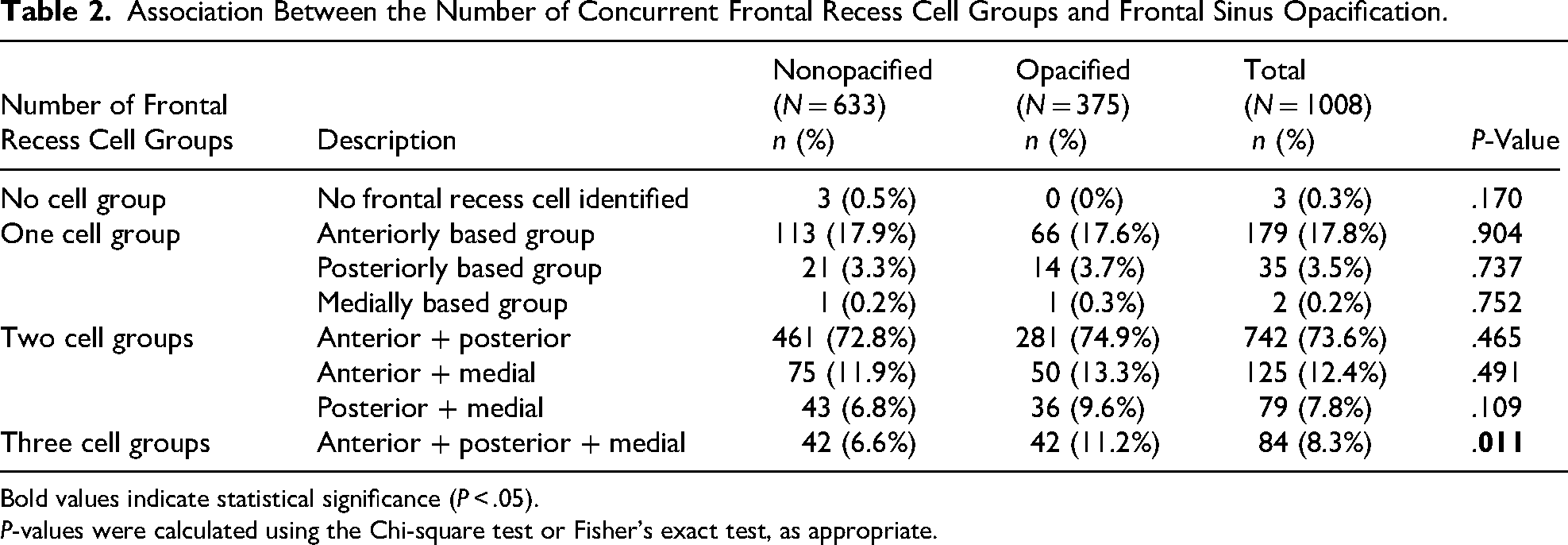
Bold values indicate statistical significance (P < .05).
P-values were calculated using the Chi-square test or Fisher's exact test, as appropriate.
FSDP in Relation to Adjacent Cells
Anteriorly Based Cells
In relation to ANC, the FSDP most commonly ran posterior to the cell (63.9%), followed by a medial course (35.6%). When SAC was present, the FSDP most frequently ran medial to the cell (55.3%), followed by a posterior course (41.2%). In cases with SAFC, the FSDP predominantly ran medial to the cell (68.7%), followed by a posterior course (28.9%). An anterior or lateral course relative to SAFC was observed in only one case each (1.2%).
No significant differences in FSDP configuration relative to ANC, SAC, or SAFC were identified between opacified and nonopacified frontal sinuses (Table 3).
Distribution of FSDP Positions Relative to Anteriorly Based Frontal Cells.
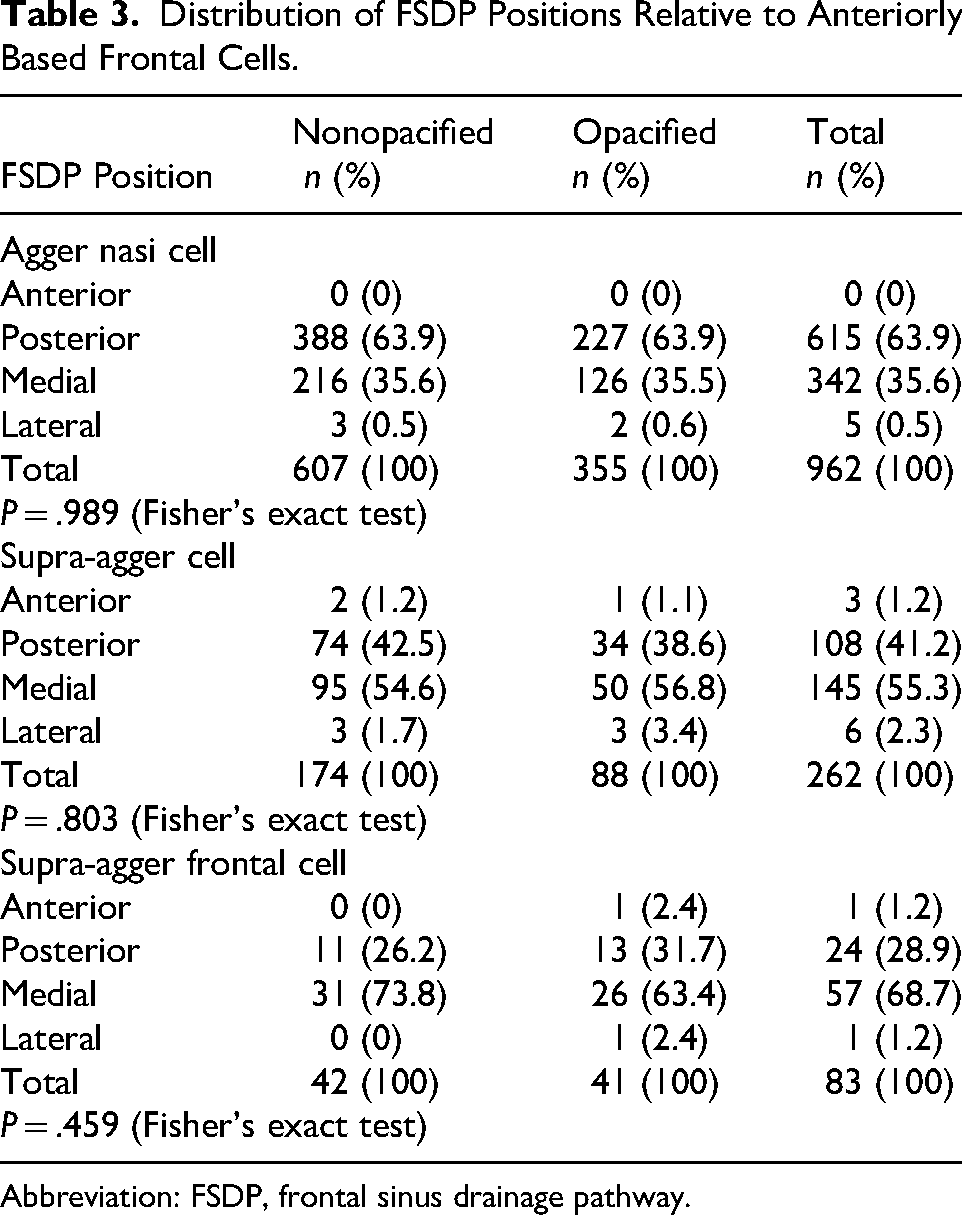
Abbreviation: FSDP, frontal sinus drainage pathway.
Posteriorly- and Medially-Based Cells
For SBC, the FSDP ran anterior to the cell in 100% of cases, with no variation in course relative to the SBC in either group. In the presence of SBFC, the FSDP most commonly coursed anterior to the cell (79.7%), followed by a medial course (18.8%) and a lateral course (1.6%). Similarly, when SOEC was present, the FSDP passed anterior to the cell in 97.3% of cases and medial to the cell in 2.7%. No significant differences in FSDP configuration relative to SBC, SBFC, or SOEC were observed between opacified and nonopacified frontal sinuses (all P > .05) (Table 4).
Distribution of FSDP Positions Relative to Posteriorly- and Medially Based Frontal Cells.
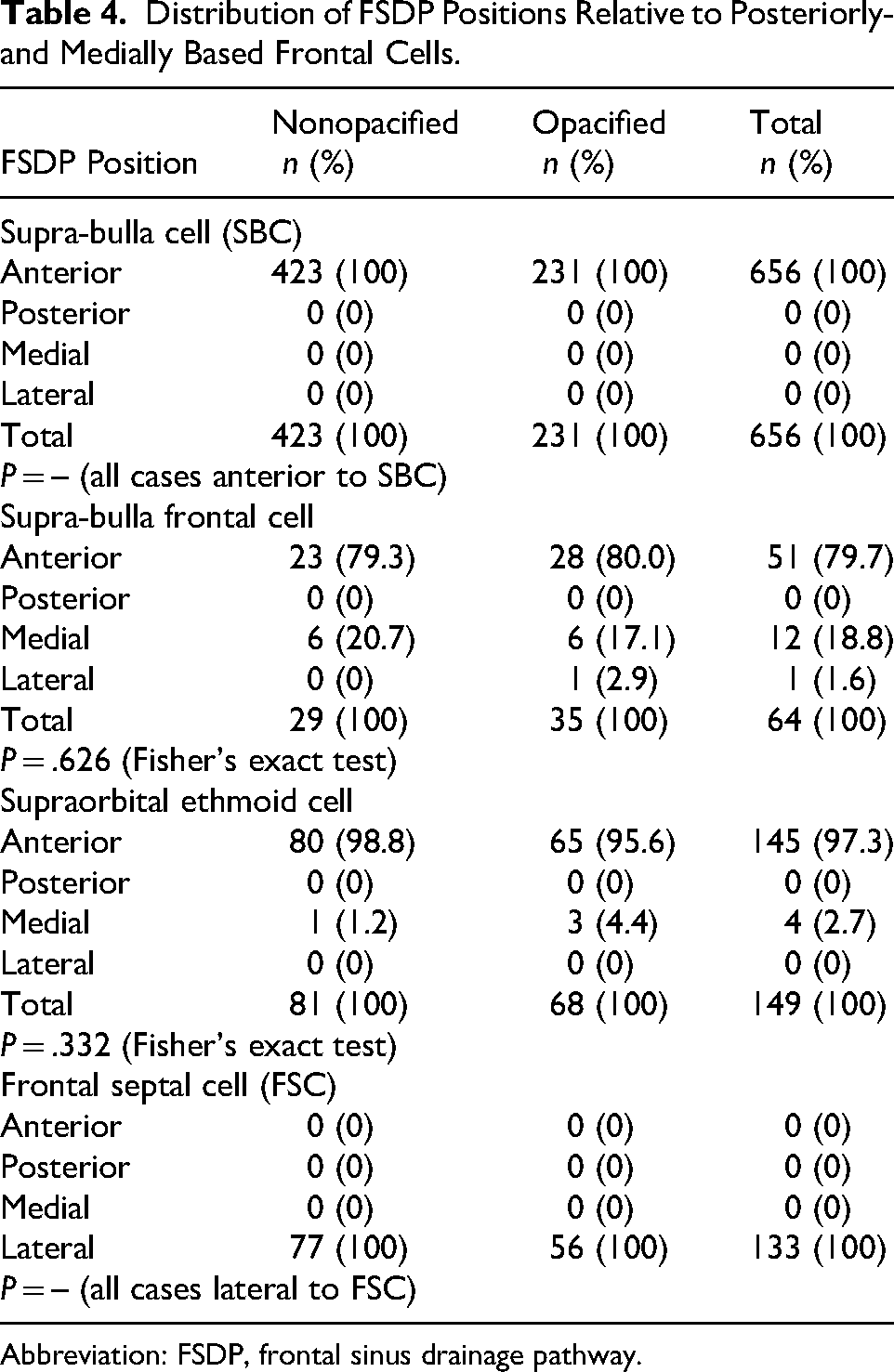
Abbreviation: FSDP, frontal sinus drainage pathway.
In all cases with FSC, the FSDP ran lateral to the cell (100%), with no variation between groups (Table 4).
Rare Posterior-to-Bulla Drainage
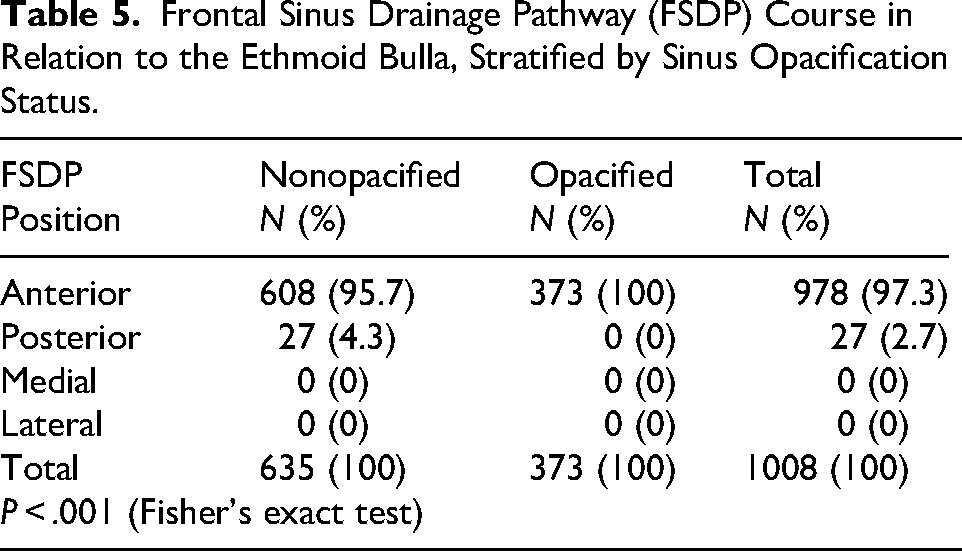
A posterior-to-bulla drainage configuration was identified in 27 frontal sinuses (2.7%). Notably, this pattern occurred exclusively in nonopacified frontal sinuses and was not observed in any opacified case (P < .001) (Table 5).
Frontal Sinus Drainage Pathway (FSDP) Course in Relation to the Ethmoid Bulla, Stratified by Sinus Opacification Status.
Surgical Validation
A total of 112 opacified frontal sinuses underwent endoscopic frontal sinus surgery and were included for surgical validation. Preoperative 3-dimensional mapping using the Stryker Building Blocks software was reviewed to guide individualized surgical planning.
Overall, preoperative 3-dimensional mapping demonstrated high concordance with intraoperative findings. Complete agreement between preoperative mapping and intraoperative identification of frontal cells was achieved in 101 of 112 cases (90.1%) (Figure 2). In the 11 remaining cases, small SAC (6/11, 54.5%) or SBC (5/11, 45.5%) were not clearly identified intraoperatively, mainly due to their small size, thin bony septations, or inadvertent removal during dissection of adjacent cells. In 7 of these cases, marked mucosal edema and bleeding further hindered precise intraoperative identification.

Preoperative planning, intraoperative validation, and postoperative outcomes following endoscopic frontal sinus surgery in a representative case with coexisting anteriorly-, posteriorly-, and medially based frontal recess cells, representing a relatively complex anatomical configuration. (A) Preoperative CT-based planning using Stryker Building Blocks software demonstrating the frontal sinus drainage pathway (FSDP, curved line). The FSDP courses medial to the agger nasi cell (ANC), lateral to the frontal septal cell (FSC), and anterior to the supra-bulla cell (SBC) and supraorbital ethmoid cell (SOEC). (B) Intraoperative endoscopic view confirming concordance with the preoperative plan; the FSDP is indicated by an arrow. (C) Postoperative CT scan demonstrating a widely patent frontal recess with an unobstructed drainage pathway. (D) Endoscopic view at 6-month follow-up demonstrating a well-drained frontal recess with preservation of the anterior ethmoidal artery (star).
Using the preoperatively mapped FSDP as a guide, the drainage pathway was successfully identified intraoperatively in all cases. Surgical instruments were consistently advanced along the mapped route to safely expose and remove obstructing frontal cells, and no case resulted in misidentification of the true FSDP. Complete removal of frontal cells was achieved in 71.7% of operated sinuses, while partial preservation of bony septations occurred in 28.3%, without residual obstructing cells causing persistent blockage of the drainage pathway.
No intraoperative complications were observed, including anterior ethmoidal artery injury, orbital hematoma, lamina papyracea violation, or cerebrospinal fluid leak.
Postoperative CT at 6 months demonstrated a complete dissection of frontal cells in 82.1% of cases. In the remaining 17.9%, a small superior bony remnant of the SAFC or SBFC could not be completely removed endoscopically because it extended too far superiorly within the frontal sinus. However, the cell had been adequately opened and widely incorporated into the FSDP without evidence of obstruction. A patent FSDP was observed in 86.8% of operated sinuses, partial opacification in 10.6%, and complete opacification in 2.6%, attributed mainly to postoperative mucosal edema. The frontal sinus Lund–Mackay score decreased significantly from 1.4 ± 0.5 preoperatively to 0.2 ± 0.4 postoperatively (P < .001).
Discussion
This study presents a large-scale, CT-based 3-dimensional characterization of the FSDP, with additional intraoperative correlation in a subset of cases. The findings demonstrate a high degree of consistency with established anatomical descriptions and suggest that these structural relationships are largely preserved across both opacified and nonopacified sinuses. While the size of the dataset and the use of 3-dimensional reconstruction strengthen the reliability of these observations, the results should be interpreted within the context of a descriptive anatomical study.
These findings build upon a previously published radiological study that was limited to a smaller cohort of nonopacified frontal sinuses and lacked surgical validation. 8 While that earlier work described drainage patterns in relation to frontal cells, it did not evaluate opacified sinuses nor verify anatomical predictions intraoperatively. The present study extends this foundation by incorporating a larger and more heterogeneous cohort, including diseased sinuses, with surgical validation. To our knowledge, few studies have combined large-scale 3-dimensional mapping with comparative analysis across inflammatory states and operative validation.
Frontal Recess Cells and Frontal Sinus Opacification
Anatomical variations in frontal cells may influence the FSDP by narrowing the frontal sinus ostium and impairing drainage. In our study, univariate logistic regression showed that SAFC, SBFC, and SOEC were significantly associated with frontal sinus opacification, whereas other frontal cells were not. These findings suggest that specific pneumatization patterns may affect frontal sinus ventilation and drainage.
In our research, the prevalence of SAFC was significantly higher in patients with frontal opacification than in those without (P < .05) (Table 1). This finding aligns with the study of Aksakal et al 1 and contrasts with the results of recent studies by Fawzi et al 2 and Seth et al. 3 Among the posteriorly based frontal cells, SBFC and SOEC were significantly associated with frontal sinus opacification (P < .05) (Table 1). The prevalence of these cells was markedly higher in opacified frontal sinuses than in nonopacified ones. Similar associations have been reported in previous studies, in which Fawzi et al 2 documented a higher prevalence of SOEC in opacified frontal sinuses, and Nair et al 4 reported a comparable correlation for SBFC. These associations should be interpreted as descriptive observations rather than evidence of causality, as the cross-sectional design does not allow determination of whether anatomical complexity contributes to disease or is influenced by inflammatory processes.
Beyond individual cell types, we evaluated the cumulative effect of concurrent frontal recess cell groups. The presence of 0, 1, or 2 groups was not associated with frontal sinus opacification, whereas coexistence of all 3 groups was significant (Table 2). This may reflect a threshold effect of anatomical complexity rather than a simple linear relationship. The simultaneous presence of anteriorly-, posteriorly-, and medially based cells may produce multidirectional narrowing of the frontal recess. However, our study design does not allow determination of whether increased anatomical complexity predisposes to impaired drainage or arises as a secondary consequence of chronic inflammatory processes. Therefore, these associations should be interpreted cautiously and not as evidence of pathogenic mechanisms.
FSDP Types and Frontal Opacification
Previous anatomical studies have mainly reported the prevalence of frontal cells, while data describing the FSDP in relation to these cells remain limited. By employing validated 3-dimensional reconstruction software in a large cohort, the present study enabled continuous tracing of the FSDP and detailed evaluation of its spatial relationships with adjacent cells.
Anteriorly based frontal cells are often considered more relevant during frontal recess dissection than posteriorly based cells, particularly for surgeons who approach the frontal sinus with intact bulla technique. In addition, the drainage pathway in relation to anteriorly based cells demonstrates greater anatomical variability than that observed with posteriorly based cells. In our study, the FSDP most commonly ran posterior or medial to anteriorly-based cells (Table 3) (Figure 3). More than 99% of FSDPs were located posterior or medial to the ANC, and over 96% were located posterior or medial to SAC. These dominant configurations may help improve anatomical orientation during frontal recess dissection.
Representative 3-dimensional and multiplanar CT views demonstrating the relationship between the frontal sinus drainage pathway ( curved line) and anteriorly based cells. The drainage pathway ran posterior to the agger nasi cell (ANC), medial to the supra-agger cell (SAC) and supra-agger frontal cell (SAFC).
We identified a posterior-to-ethmoid-bulla drainage configuration in 2.7% of sinuses, occurring exclusively in nonopacified cases (Figure 4). Similar findings have been infrequently reported in the literature, including by Kikawada et al. 9 This rare variant was typically associated with a large ANC displacing the FSDP posteriorly to the BE. However, given its low prevalence, the clinical significance of this anatomical configuration remains uncertain.
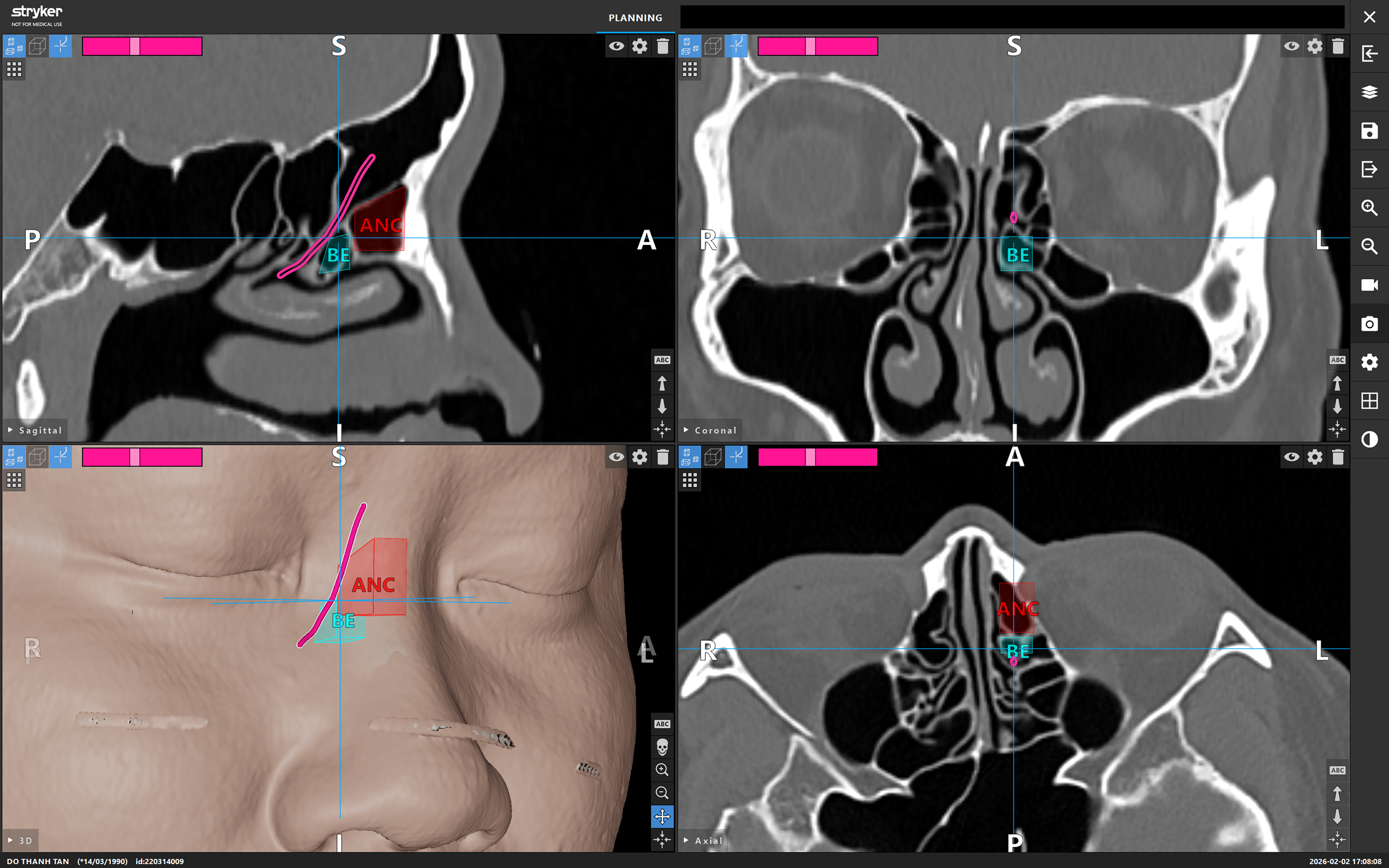
Representative 3-dimensional and multiplanar CT views demonstrating a frontal sinus drainage pathway (curved line) coursing posterior to the ethmoid bulla (BE). A large agger nasi cell (ANC) extends posteriorly and abuts the anterior wall of the BE, displacing the frontal sinus drainage pathway posteriorly.
The high concordance between preoperative mapping and intraoperative findings supports the anatomical accuracy of the 3-dimensional reconstruction. However, the present study was not designed to determine whether this approach improves surgical outcomes or clinical decision-making. Postoperative CT imaging in this study was included for illustrative anatomical purposes only, demonstrating complete frontal recess cell dissection and widening of the FSDP following surgery guided by preoperative 3-dimensional anatomical analysis, rather than to assess surgical outcomes or disease control.
Several limitations should be acknowledged. This was a single-center, cross-sectional imaging study, and anatomical distributions may vary across populations. Statistical analysis was limited to univariate regression, and interactions among frontal cells were not evaluated. In addition, the study relied exclusively on CT imaging without integration of clinical or inflammatory variables such as eosinophilic inflammation, aspirin-exacerbated respiratory disease, tobacco exposure, or treatment adherence. Consequently, the anatomical findings should be interpreted as descriptive observations rather than predictors of disease behavior, prognosis, or surgical outcomes.
Future studies integrating imaging analysis with clinical phenotyping and outcome assessment are required to determine the clinical relevance of these anatomical findings.
Conclusion
This large-scale 3-dimensional mapping study demonstrates that the FSDP maintains consistent and predictable spatial relationships with frontal recess cells. Anteriorly based cells show greater directional variability, with the FSDP most commonly located posterior or medial and progressively medializing with superior extension. In contrast, posteriorly- and medially based cells exhibit highly stable configurations, with the FSDP consistently positioned anterior or lateral to these structures. These anatomical patterns provide a structured framework that may assist preoperative planning and surgical orientation for individualized frontal sinus surgery.
Footnotes
Acknowledgments
The authors used artificial intelligence–based language editing assistance (ChatGPT) to improve grammar and clarity. The authors take full responsibility for the scientific content of this manuscript.
Ethical Considerations
Ethical approval for this study was obtained from the research ethics board of Ear Nose Throat Hospital of Ho Chi Minh City (No: 03/GCN-BVTMH).
Consent to Participate
Informed consent was secured from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data are available from the corresponding author upon reasonable request.