
Abstract
Objective
To evaluate the long-term anatomical and functional efficacy of a hybrid surgical technique combining endoscopic dacryocystorhinostomy (En-DCR), endoscopic common canaliculotomy, and temporary bicanalicular silicone intubation in patients with severe common canalicular obstruction (CCO).
Methods
This retrospective case series analyzed 43 eyes of 43 patients (mean age: 55.4 ± 8.0 years) with severe CCO treated between February 2018 and July 2022. Severe CCO was confirmed intraoperatively by soft resistance to probing ≥10 mm from the punctum. The surgical technique included wide bony ostium creation, lacrimal sac marsupialization, direct endoscopic incision of the fibrotic common canaliculus, and bicanalicular silicone tube intubation (stent removed at 3 months). Outcomes were assessed at ≥12 months postoperatively using epiphora symptom resolution, lacrimal irrigation, nasal endoscopy, and fluorescein dye disappearance test. Anatomical success was defined as a patent ostium with unobstructed irrigation; functional success required anatomical patency plus complete epiphora resolution.
Results
At a mean follow-up of 18.8 ± 6.9 months, anatomical success was achieved in 37 eyes (86.0%), and functional success in 35 eyes (81.4%). Failures included 5 cases of ostial fibrosis and 1 recurrent CCO; 2 patients reported persistent epiphora despite anatomical patency. No major complications (eg, orbital hemorrhage, sinusitis) occurred.
Conclusions
In carefully selected patients with isolated severe CCO, the hybrid technique of En-DCR with canaliculotomy and temporary intubation demonstrates promising success rates and a favorable safety profile while preserving physiological drainage. These findings suggest it may serve as a physiologically favorable alternative to conjunctivodacryocystorhinostomy, mitigating the long-term complications associated with permanent bypass tubes.
Keywords
Introduction
Common canalicular obstruction (CCO) is a clinically significant cause of debilitating epiphora, representing a substantial proportion of lacrimal drainage disorders. 1 While mild stenoses often respond to probing and intubation, severe CCO—characterized by dense fibrotic obliteration at the common canaliculus–lacrimal sac junction—poses considerable therapeutic challenges. 2 Blind probing in these cases is not only ineffective but also risks iatrogenic false passage formation and secondary stenosis. 3
Conjunctivodacryocystorhinostomy (CDCR) with Jones tube placement remains the historical gold standard for severe CCO.4,5 Although effective for drainage restoration, this nonphysiological bypass sacrifices the native lacrimal anatomy and carries substantial long-term risks, including tube migration, extrusion, obstruction, and granuloma formation, often requiring lifelong maintenance and revision surgeries.5–8 These limitations highlight the need for surgical alternatives that preserve physiological drainage while avoiding permanent prostheses.
Endoscopic dacryocystorhinostomy (En-DCR) has advanced the management of nasolacrimal obstructions through superior visualization, minimal invasiveness, and preservation of lacrimal pump function.9,10 Its key advantage lies in the complete exposure of the medial lacrimal sac wall and common canalicular entrance following marsupialization. 11 This systematic exposure enables precise identification and targeted management of proximal obstructions under direct vision, forming the anatomical basis for successful reconstruction.2,11
Building upon this foundation, we developed a hybrid technique integrating En-DCR, endoscopic common canaliculotomy, and temporary bicanalicular intubation. This approach permits direct visual incision of fibrotic membranes with temporary stenting to restore natural drainage pathways. This study evaluates the long-term outcomes of this technique in severe CCO, testing its viability as a first-line CDCR alternative that maintains physiological function while eliminating permanent tube-related complications.
Subjects and Methods
This single-center, retrospective consecutive case series analyzed all consecutive patients patients with severe CCO who underwent combined En-DCR, endoscopic common canaliculotomy and temporary bicanalicular silicone intubation between February 2018 and July 2022. The Institutional Review Board approved the protocol, and written informed consent was obtained from all participants.
We collected data regarding each patient's demographic and clinical profile, Computed Tomography Dacryocystography (CT-DCG) findings, surgical findings, outcomes, and complications. Inclusion criteria required clinical diagnosis of CCO confirmed by the following constellation: (1) Immediate reflux from the superior punctum upon lacrimal irrigation through the inferior punctum without mucopurulence; (2) A Bowman probe arrested ≥10 mm from the punctum by soft resistance, without bony contact; (3) Delayed clearance on fluorescein dye disappearance test (FDDT) (Figure 1A); (4) CT-DCG demonstrating obstruction at the common canaliculus and absence of contrast in the lacrimal sac (Figure 1B).
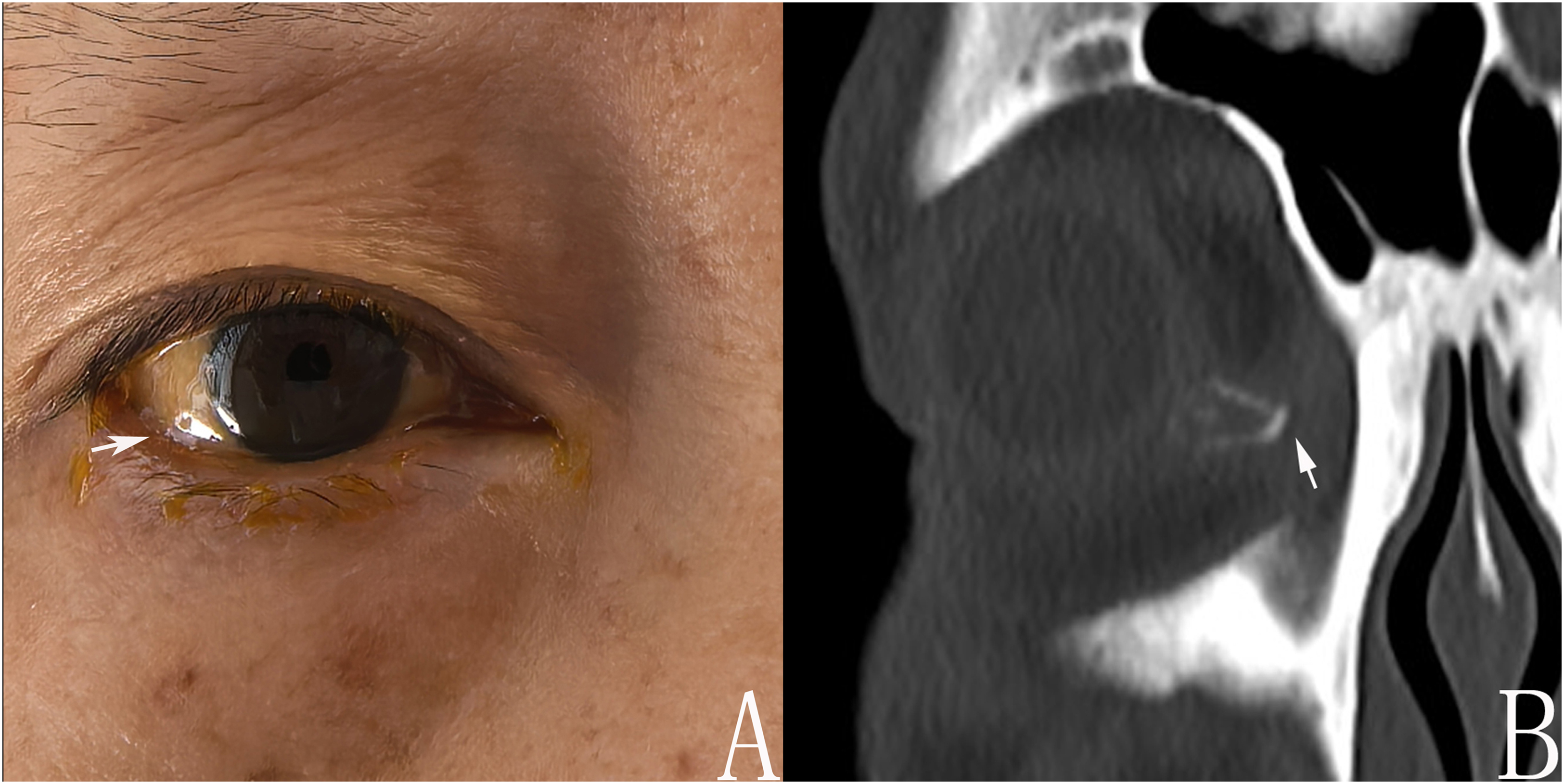
Preoperative diagnostic evaluation of severe common canalicular obstruction. (A) Fluorescein dye disappearance test at 5 min shows delayed clearance (arrow), indicating impaired lacrimal drainage. (B) Coronal computed tomography-dacryocystography demonstrates obstruction at the common canaliculus (arrow). Note the contrast retention proximal to the obstruction and the absence of contrast within the lacrimal sac.
Slit-lamp examination ruled out eyelid malposition and punctal stenosis, while nasal endoscopy and sinus CT excluded neoplasia and significant sinonasal pathology. Exclusion criteria comprised age <18 years, severe sinusitis, previous nasal/orbital trauma, primary lacrimal sac tumors, bleeding diathesis, and follow-up under 12 months. When significant septal deviation compromised endoscopic access, septoplasty was performed prior to En-DCR.
Surgical Technique
All procedures were performed by a single experienced lacrimal surgeon (B Y) under general anesthesia with the patient supine and the head elevated 15°. A 4 mm, 0° rigid endoscope provided continuous visualization via the ipsilateral nasal cavity.
Step 1—Intraoperative grading of CCO: After punctal dilation, a Bowman probe was advanced through the inferior canaliculus. Gentle pressure was applied until either (1) the probe met bone and saline irrigated freely into the inferior meatus (mild obstruction; excluded), or (2) persistent soft resistance was encountered ≥10 mm from the punctum, preventing lacrimal-sac entry (severe CCO; included). Step 2–Combined En-DCR, canaliculotomy and intubation: (1) Nasal preparation: Cottonoids soaked in 1:1000 epinephrine were applied for 2 min to achieve mucosal decongestion and haemostasis. (2) Osteotomy: A 1 cm mucosal incision was made anterior to the middle turbinate. Submucosal dissection exposed the lacrimal-maxillary suture; the frontal process of the maxilla was thinned with a 4 mm diamond burr and removed with sphenoid punches to create a 1 × 1.5 cm bony ostium. (3) Sac exposure: A vertical incision through the medial lacrimal-sac wall, extending to the fundus, opened the sac and created a broad posterior mucosal flap. (4) Canalicular recanalisation: A probe introduced via the inferior punctum tented the obstructed common canaliculus (Figure 2A and B). Under direct endoscopic view, the fibrotic membrane was sharply incised with a 15° micro-knife until the probe emerged into the nasal cavity (Figure 2C and D); patency was confirmed by unobstructed saline egress through the superior punctum. (5) Intubation and closure: A bicanalicular silicone tube was passed through both canaliculi and the newly created common canalicular opening, with both ends were tied and positioned in the nasal cavity. The posterior lacrimal-sac flap was anastomosed to the corresponding nasal mucosal flap (Figure 2E). The osteotomy margins were covered with self-linked sodium hyaluronate to inhibit fibrosis (Figure 2F).
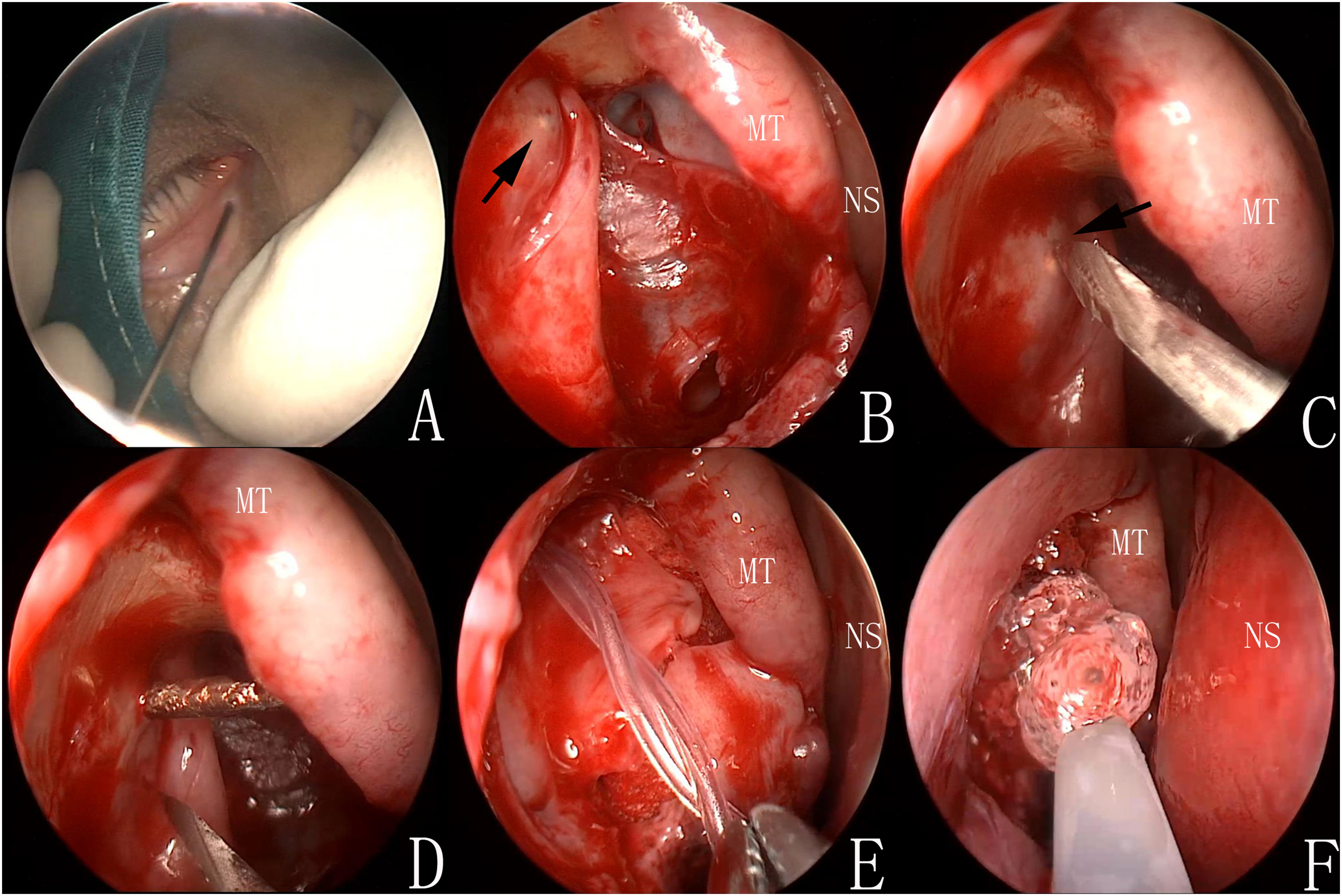
Intraoperative endoscopic views during hybrid endoscopic dacryocystorhinostomy with canaliculotomy and intubation (right nasal cavity, 0° endoscope). (A, B) A Bowman probe introduced via the inferior canaliculus tents the obstructed common canaliculus at the lacrimal sac junction (arrow). MT, middle turbinate; NS, nasal septum. (C, D) Under direct vision, the fibrotic membrane at the common canalicular opening is sharply incised with a 15° micro-knife (arrow), allowing the probe tip to emerge into the nasal cavity. (E) Bicanalicular silicone tube in situ, traversing both canaliculi and the newly created opening. (F) The bony osteotomy margins are coated with self-linked sodium hyaluronate to inhibit fibrosis.
Postoperatively, patients received intravenous ceftriaxone for 2 days, topical levofloxacin for 2 months, a stepped antiinflammatory regimen (fluorometholone then pranoprofen), and intranasal budesonide for 2 months. Follow-up examinations were conducted at 1 week, 2 weeks, and 1, 3, 6, and 12 months. At each visit, symptoms, irrigation findings, FDDT, and endoscopic ostium assessment were documented. The severity of epiphora was graded using the standardized Munk scale (0-4) by an independent, masked assessor who was unaware of the patient's surgical history and intraoperative findings. 12 The Munk scale categorizes epiphora as: Grade 0 (none), Grade 1 (occasional, requiring dabbing ≤ twice daily), Grade 2 (requiring dabbing 2-4 times daily), Grade 3 (requiring dabbing 5-10 times daily), and Grade 4 (constant or requiring dabbing >10 times daily). Silicone tubes were removed endoscopically at 3 months. Anatomical success was defined as a patent ostium on endoscopy with unobstructed irrigation; functional success required anatomical patency plus complete resolution of epiphora, defined as a postoperative Munk score of 0 or 1.
Statistical Analysis
Descriptive statistics were used for demographic and clinical characteristics. Continuous variables were expressed as mean ± standard deviation, categorical variables as frequencies and percentages. All analyses were performed using SPSS version 26.0.
Results
A total of 49 eyes underwent initial screening for eligibility. Six were excluded for the following reasons: 3 had intraoperatively confirmed mild obstruction (as defined in our Methods), 1 had a history of naso-orbital trauma, and 2 were lost to follow-up before reaching the 12-month endpoint. The remaining 43 eyes (43 patients) formed the final analytical cohort. Demographic and clinical characteristics of the 43 included patients are summarized in Table 1. The study group consisted of 26 females and 17 males, with a mean age of 55.4 ± 8.0 years. Surgery was performed on 20 right eyes and 23 left eyes. Two patients underwent concomitant endoscopic septoplasty. The median interval from epiphora onset to surgery was 23.5 ± 12.2 months.
Baseline Characteristics of the Study Cohort (n = 43).
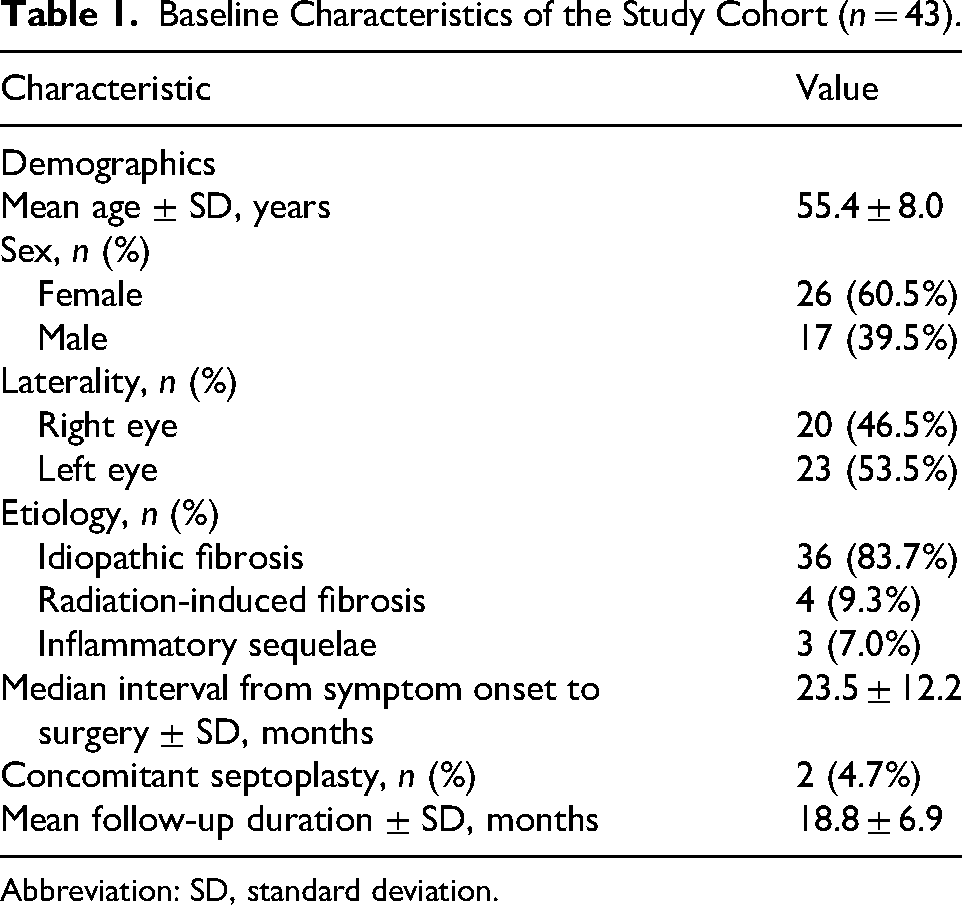
Abbreviation: SD, standard deviation.
Etiology analysis revealed idiopathic fibrosis in 83.7% of cases, radiation-induced fibrosis in 9.3%, and inflammatory sequelae in 7.0%. All procedures were completed without major complications. Transient bleeding occurred in 2 eyes (4.7%), controlled with bone wax and cautery. No conversions to external approach were needed. Mild nasal foreign-body sensation related to the stent (27.9%) resolved after removal.
At a mean follow-up of 18.8 ± 6.9 months, anatomical success was achieved in 37 eyes (86.0%) and functional success in 35 eyes (81.4%) (Figure 3A and C). Among the 6 cases of anatomical failure (5 with ostial fibrosis and 1 with recurrent CCO), the etiologies of the original CCO were distributed as follows: idiopathic in 4 cases, radiation-induced in one, and inflammatory in one. Three patients underwent revision surgery with success in 2 cases. Two patients (4.7%) reported persistent epiphora despite anatomical patency. No sight-threatening or sinonasal complications occurred.
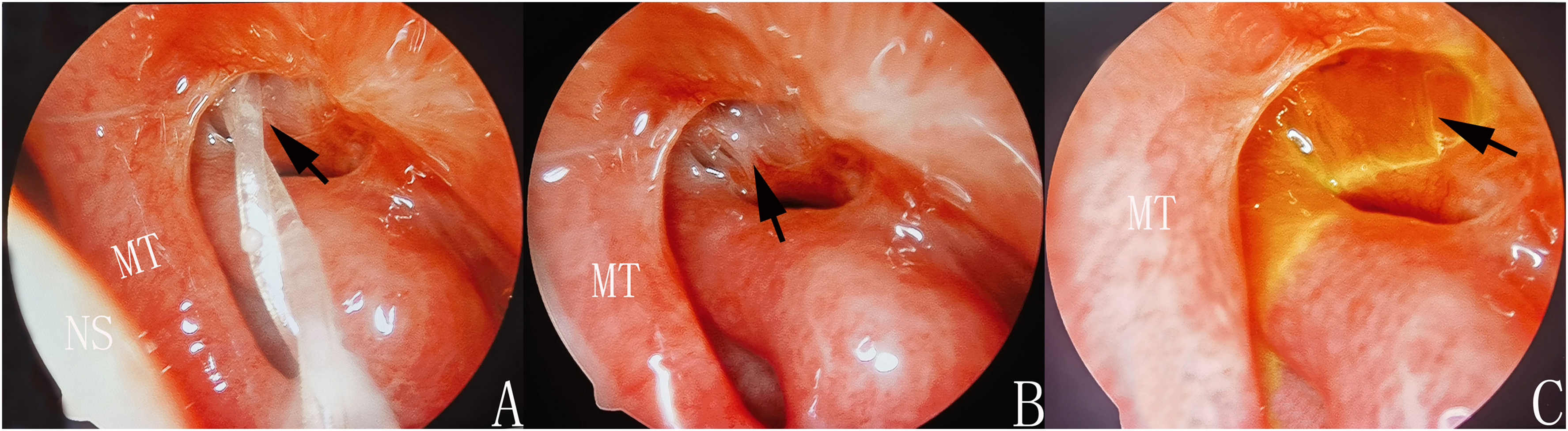
Postoperative endoscopic and clinical outcomes in a representative case (right side). (A) Endoscopic view at 2 months postoperatively shows the silicone tube in situ within a well-healed osteotomy (arrow). (B) Endoscopic view at the final follow-up (18 months) shows a widely patent, fully epithelialized osteotomy (arrow). (C) Fluorescein dye disappearance test at 5 min under cobalt-blue light shows complete clearance, confirming functional success (arrow).
Discussion
Acquired lacrimal canalicular obstruction represents a clinically significant entity, accounting for approximately 16% to 25% of patients presenting with epiphora.13,14 CCO constitutes a challenging subset of this condition, although its precise prevalence remains unreported. The management of CCO is particularly difficult due to the intricate anatomy of the canalicular system and its propensity for fibrotic occlusion. Severe CCO is characterized by dense fibrous obliteration at the common canaliculus–lacrimal sac junction, frequently leading to refractory epiphora that significantly impairs quality of life. 15 Etiological analysis in our cohort revealed a multifactorial pattern: idiopathic fibrosis formed the predominant subgroup (83.7%), likely originating from chronic subclinical inflammation and dysregulated fibroblast activation mechanisms, predominantly affecting middle-aged and elderly patients without identifiable predisposing factors. Secondary etiologies included radiation-induced fibrosis (9.3%), typically manifesting 8 to 36 months after radiotherapy for head or nasal malignancies, and inflammatory sequelae (7.0%) following severe mucopurulent conjunctivitis. This etiological heterogeneity underscores the complex pathophysiology underlying CCO and emphasizes the need for individualized surgical management strategies.
Accurate diagnosis and precise stratification of obstruction severity are paramount for formulating appropriate management strategies. Our institutional protocol employs a comprehensive multimodal diagnostic approach incorporating detailed clinical history, physiological assessment including FDDT, lacrimal irrigation demonstrating immediate reflux through the opposite punctum without lacrimal sac distension, and high-resolution CT-DCG to definitively localize the obstruction level and exclude secondary pathologies such as neoplasms or dacryoliths. In the present study, the findings from CT-DCG were concordant with intraoperative probing in all included cases, underscoring the reliability of our preoperative diagnostic workflow. Probing revealing characteristic soft resistance ≥10 mm from the punctum, absent bony contact, provides additional diagnostic confirmation.15–17 Crucially, intraoperative assessment under anesthesia remains the definitive diagnostic step, enabling reliable differentiation between mild and severe obstruction through tactile feedback and direct visualization, thereby guiding optimal surgical strategy selection.
Mild or partial CCO can often be managed effectively with simple probing and temporary silicone intubation. In contrast, severe CCO—characterized by dense fibrotic occlusion at the common canaliculus–lacrimal sac junction—poses a substantially greater therapeutic challenge. Conventional blind probing in these cases is not only often ineffective but also carries substantial risks of iatrogenic injury, including false passage formation and aggravated fibrosis. Similarly, standalone trephination with silicone intubation yields unsatisfactory outcomes, with reported failure rates exceeding 40%, underscoring the limitations of conventional techniques.18,19 In our study, surgical management was individualized according to intraoperative obstruction severity. Patients with gentle probing reaching the bony lacrimal crest and free saline irrigation were classified as mild CCO and received standard intubation, whereas those with persistent soft resistance preventing lacrimal sac entry were categorized as severe CCO and underwent hybrid endoscopic reconstruction.
Dacryoendoscopy has advanced lacrimal disorder management by enabling direct intraluminal visualization. This technology facilitates precise endoscopic exploration and supports targeted interventions including laser-assisted recanalization and sheath-guided bicanalicular intubation.20,21 As the sole minimally invasive modality providing real-time, high-resolution luminal imaging, it is essential for locating obstructions, detecting foreign bodies, and evaluating mucosal pathologies.22,23 Although applied therapeutically in laser recanalization and stent placement, its adoption remains limited. While short-term outcomes appear promising with improved patency and reduced invasiveness, robust long-term evidence is scarce and large-scale randomized trials are lacking. Furthermore, substantial equipment costs and technical demands have confined its use mainly to high-volume tertiary centers. 24 These constraints continue to impede routine clinical integration, despite its significant potential for managing complex obstructions.
CDCR with Jones tube placement has historically been regarded as the gold standard for managing severe CCO and other proximal canalicular pathologies where anatomical reconstruction is not feasible. Indications include complete canalicular obstruction, traumatic canalicular loss, previous failed lacrimal surgery, and extensive fibrosis involving the common canaliculus.4,5 The procedure involves creating a new drainage pathway from the medial canthus directly into the nasal cavity, completely bypassing the natural lacrimal system. A Pyrex glass tube is then permanently installed to maintain patency.4,8 Although CDCR effectively alleviates epiphora in over 70% of cases, it is plagued by a high rate of long-term tube-related complications, including displacement, extrusion, mucus obstruction, biofilm formation, granulomatous inflammation, and chronic medial canthal irritation. Additionally, the Jones tube necessitates lifelong maintenance and frequent clinical adjustments, with up to 40% of patients requiring revision surgery.4–6,8,25 These significant drawbacks highlight the urgent need for more physiological and sustainable surgical alternatives.
In response to these clinical challenges, we developed a hybrid surgical technique integrating En-DCR, direct endoscopic common canaliculotomy, and temporary bicanalicular silicone intubation. This approach leverages the superior visualization afforded by modern endoscopic systems to achieve precise anatomical reconstruction while preserving physiological drainage mechanisms. A critical component of this procedure is the systematic exposure of the common canalicular plane, which begins with the creation of a generously sized bony ostium and complete marsupialization of the lacrimal sac. It has been well documented that exposure of the common canalicular inlet is essential in cases involving a small lacrimal sac (≤5 mm in diameter) and significantly contributes to surgical success even in normal-sized sacs by facilitating accurate identification of the obstruction site and ensuring adequate mucosal apposition during healing.11,26 In our technique, strategic incision superior to the common canaliculus–lacrimal sac junction ensures consistent visualization of this critical landmark. Under endoscopic guidance, meticulous microsurgical incision of the fibrotic tissue is performed, significantly minimizing iatrogenic trauma and false passage formation. Subsequent temporary bicanalicular stenting serves as a scaffold during the healing phase, promoting mucosal regeneration while avoiding long-term complications associated with permanent prostheses. By preserving the native lacrimal drainage pathway and maintaining physiological pump function, this technique fundamentally differs from CDCR, thereby eliminating the need for permanent hardware and its associated complications.5,6,8,25
Our results demonstrate that this integrated approach achieves high anatomical and functional success rates over a mean 18.8-month follow-up, surpassing outcomes reported with conventional techniques. These outcomes reflect several key factors: strict selection of isolated CCO cases; enhanced visualization enabling precise obstruction identification and incision; complete lacrimal sac marsupialization promoting mucosal regeneration; and perioperative antifibrotic strategies using self-linked sodium hyaluronate and corticosteroid sprays to modulate healing and minimize scarring.27–29 It is noteworthy that the prolonged use of topical corticosteroids and antiinflammatory agents postoperatively, as employed in our protocol, may have contributed to the favorable outcomes by suppressing inflammation and fibrosis. Future studies are needed to determine the extent of this contribution and whether comparable results can be achieved with different or minimized adjunctive medical regimens. The technique demonstrated exceptional safety, with minimal morbidity: only 4.7% experienced transient bleeding, easily controlled with conventional measures. No serious complications such as orbital fat prolapse, hematoma, diplopia, visual impairment, or sinusitis occurred. Stent-related foreign body sensation resolved completely after removal at 3 months, contrasting with CDCR's permanent tube-related complications.
Several limitations of our study warrant consideration. The retrospective, single-center design and modest sample size may affect the generalizability of our findings. The subjective nature of our CCO severity classification, based primarily on tactile feedback during probing, introduces potential interobserver variability that could influence patient selection. Future studies incorporating objective metrics such as intraoperative dacryoendoscopy or pressure measurements could refine severity assessment and enhance reproducibility. Additionally, by focusing exclusively on isolated CCO, our study does not evaluate this technique's efficacy in cases with concurrent distal obstruction or significant lacrimal sac pathology, representing an important area for future investigation. The absence of a control group precludes direct comparison with other surgical modalities, necessitating cautious interpretation of our outcomes relative to existing literature.
Conclusion
In conclusion, our study suggests that the hybrid technique of En-DCR with common canaliculotomy and temporary bicanalicular intubation may offer an effective and safe intervention for carefully selected patients with isolated severe CCO. This approach aims to reconstruct the physiological drainage pathway, achieving favorable anatomical and functional outcomes while mitigating the long-term risks associated with permanent prostheses. Supported by a satisfactory safety profile and reproducible results in our cohort, this technique emerges as a physiologically favorable alternative to CDCR in this specific patient population. Its adoption could be considered in clinical settings with appropriate endoscopic expertise. Further validation through prospective, comparative studies will be essential to more definitively establish its role in the management of severe CCO.
Footnotes
Acknowledgments
The authors thank the medical and nursing staff of the Orbital and Oculoplastic Minimally Invasive Center for their support in patient care and data collection.
Ethical Approval
This study was approved by the Institutional Review Board of the Eye Hospital of Wenzhou Medical University (Approval No. 2023-065-K-53). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.