
Abstract
Background
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant disorder with multiorgan manifestations, necessitating a multidisciplinary approach. Epistaxis is a common manifestation leading to significant morbidity. Current treatments are variable in efficacy, and adequate control of epistaxis remains a significant challenge.
Objective
To describe the cohort of patients treated at a dedicated multidisciplinary HHT clinic and to evaluate the efficacy of an HHT-related epistaxis treatment protocol at a multidisciplinary HHT clinic.
Methods
This study included both retrospective and prospective cohorts of adult patients (≥ 18 years) with confirmed HHT attending a tertiary multidisciplinary clinic. The retrospective cohort comprised patients managed prior to the establishment of the treatment protocol and contributed to baseline demographic and disease characteristics only. The prospective cohort of patients, recruited from September 2022 to September 2024, was managed using a tiered protocol progressing from topical treatment to surgical intervention to systemic therapy. Epistaxis severity score (ESS) was recorded longitudinally. Treatment efficacy was assessed by comparing ESS at baseline, pre-intervention, and post-intervention time points.
Results
A total of 62 patients, including 31 retrospective and 31 prospective patients, were identified with a mean age of 52.5 ± 17.4 years and female predominance of 62.9%. Baseline ESS scores were highest in patients in the “Bevacizumab” group, followed by those in the “Surgical treatment” group, and lowest in patients in the “Topical treatment only” cohort (P = .001). Within the prospective cohort, significant improvements in ESS were observed following surgery (ΔESS = 4.31, P = .006) and bevacizumab (ΔESS = 4.74, P = .005). Nearly half (48.4%) of patients in this clinic achieved satisfactory control with conservative measures alone.
Conclusion
A structured, multidisciplinary protocol enables effective management of HHT-related epistaxis, matching treatment intensity to disease severity to achieve satisfactory symptom control for patients.
Keywords
Introduction
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant, multisystem disorder caused by mutations within the TGFB/BMP signaling pathway, resulting in defective vascular remodeling and maintenance. 1 Diagnosis is established using the clinical Curaçao criteria or through genetic testing for known pathogenic variants (ENG, ACVRL1, and SMAD4). 2 Genotype correlates with phenotypic differences, particularly in the distribution of visceral AVMs. 3
Epistaxis is the most frequently reported symptom, affecting over 90% of individuals with HHT. Its severity is highly variable, ranging from infrequent nosebleeds to life-threatening hemorrhage requiring emergency care and ongoing transfusion support. 4 While several treatment options exist for recurrent epistaxis, most will require repeated interventions for recurrent symptoms.
The second iteration of the International Guidelines for the Diagnosis and Management of HHT guidelines presents a range of treatment modalities and the strength of their evidence. 5 The expert panel strongly recommends the use of nasal humidifying / moisturizing therapies in all patients and, beyond this, consideration of oral tranexamic acid, systemic anti-angiogenic agents, ablative therapies and, if refractory to all treatments, septodermoplasty, or nasal closure. However, the guideline does not provide the practitioner with a stepwise escalation pathway. As a result, clinicians are left to interpret how best to integrate these therapies into real-world practice.
In this study, we describe the management of patients with HHT at a dedicated multidisciplinary HHT clinic within a tertiary referral center in Australia. We present our structured, and replicable, protocol for managing HHT-related epistaxis that integrates guideline-recommended therapies with institutional clinical experience. Of note, this protocol utilizes topical beta-blocker (timolol), due to a growing body of evidence of its anti-angiogenic effects, despite its absence from the latest HHT guidelines. This protocol also incorporates clinical experience with bevacizumab in cases of treatment-refractory epistaxis. We hypothesize that the implementation of this protocol would result in effective symptom control while reserving surgical and systemic therapies for patients with more severe disease.
Methodology
Patient Pathway
The multidisciplinary HHT clinic was established in September 2022 and accepts referrals for patients with suspected or confirmed HHT. The multidisciplinary team is composed of an otolaryngologist overseeing epistaxis management and a respiratory physician (with an HHT interest) overseeing systemic screening. Genetic counseling and genetic testing through a clinical geneticist are offered in the same setting. Additional specialist input is sought as required.
Treatment for epistaxis is initiated as per a standardized protocol (see Figure 1). The validated epistaxis severity scoring (ESS) tool is used longitudinally to monitor response to epistaxis treatment. Routine hematological monitoring is performed in collaboration with the patient's general practitioner. Patients are reviewed at 3, 6, or 12 monthly intervals depending on severity of epistaxis and the need for close follow-up.
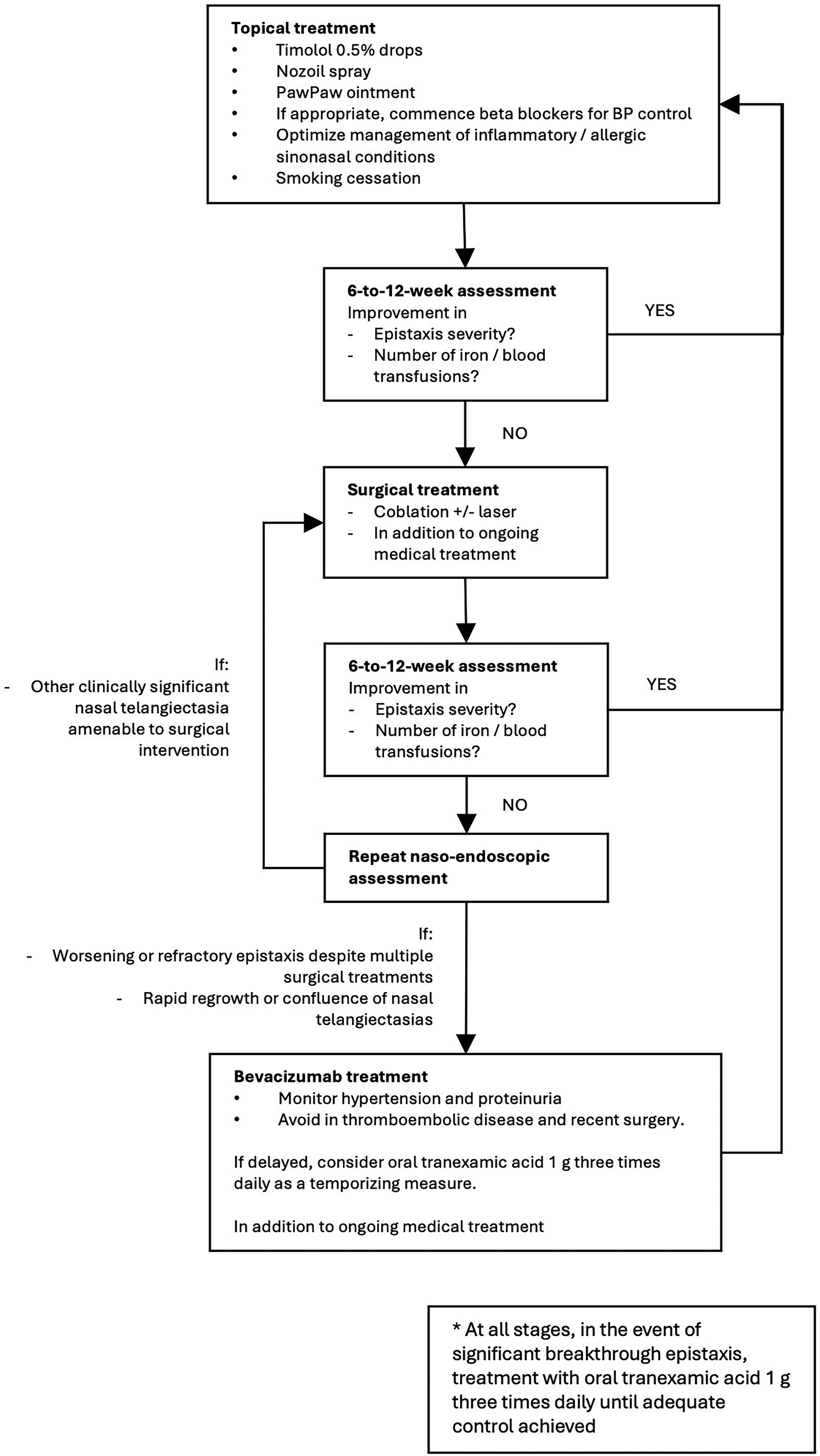
HHT-related epistaxis tiered treatment protocol. HHT, hereditary hemorrhagic telangiectasia.
Standardized Hereditary Hemorrhagic Telangiectasia-Related Epistaxis Treatment Protocol
All patients with epistaxis were treated as per the standardized protocol (Figure 1). Treatment-naïve patients commence at the initial step, while those previously managed elsewhere may enter the protocol further downstream. Treatment decisions, including escalation between various tiers, are made in consultation with the patient following a discussion of risks, benefits, and available alternatives.
Symptom control was defined using a combination of patient-reported improvement in epistaxis severity and quality of life, alongside clinical indicators including ESS, endoscopic findings, and transfusion (both iron and blood products) requirements. Treatment failure was defined as inadequate control despite an appropriate trial of therapy (6-12 weeks) with confirmed adherence. Escalation was guided by shared decision-making in the setting of persistent symptoms with significant impact on their quality of life or requiring increasing iron or blood supplementation.
Topical Treatment
First-line therapy included as follows:
topical emollients (Pawpaw or Vaseline ointment, and Nozoil® nasal spray) to maintain mucosal hydration, intranasal 0.5% timolol ophthalmic solution, medical optimization, including blood pressure control, smoking cessation, and management of coexisting sinonasal disease.
For treatment-naïve patients, a trial of topical therapy for at least 6 to 12 weeks is recommended before treatment escalation. Oral tranexamic acid (1 g 3 times daily) was used as interim salvage therapy when excessive epistaxis was experienced.
Surgical Treatment
Where topical management proves insufficient, surgical intervention is recommended, which includes:
Topical treatment is continued in conjunction. Mucosal preservation is critical; for patients who require bilateral septal treatments, the procedures are staged 6 to 8 weeks apart to minimize septal perforation.
Bevacizumab Treatment
Patients with rapid symptomatic regrowth following Coblation or laser ablation were offered off-label intravenous bevacizumab every 4 weeks for 6 months. It was also considered for severe or recurrent gastrointestinal bleeding (outside this protocol). Contraindications included recent surgery and thromboembolic disease, with monitoring of blood pressure and proteinuria required. Oral tranexamic acid (1 g 3 times daily) was used as interim therapy when treatment initiation was delayed.
Study Population
This study comprised both a prospective cohort and a retrospective cohort of consenting, non-pregnant adult patients over the age of 18 years with a confirmed diagnosis of HHT, based on 3 or more Curaçao criteria being fulfilled or a genetic diagnosis of known causative variants. The prospective cohort was recruited from September 2022 onward after the establishment of this clinic and its standardized epistaxis treatment protocol. The retrospective cohort, comprised patients who received care prior to the establishment of this clinic, was included to provide a comprehensive description of the complete HHT population. Because these patients received care preceding the standardized protocol, they were not included in any treatment efficacy analyses and, instead, only contributed to baseline demographic and genotype-phenotype analyses.
For all patients, the following variables were collected: demographic information, genetic information, systemic AVM screening data, details of topical, surgical and systemic interventions and ESSs. For analytic purposes, mutations were grouped into 3 categories: ACVRL1, ENG, and “other” which consisted of patients whose results were either of uncertain significance, missing, not performed or positive for SMAD4.
A CONSORT-style diagram detailing cohort selection, exclusions, and the final analytic sample is provided in Figure 2.
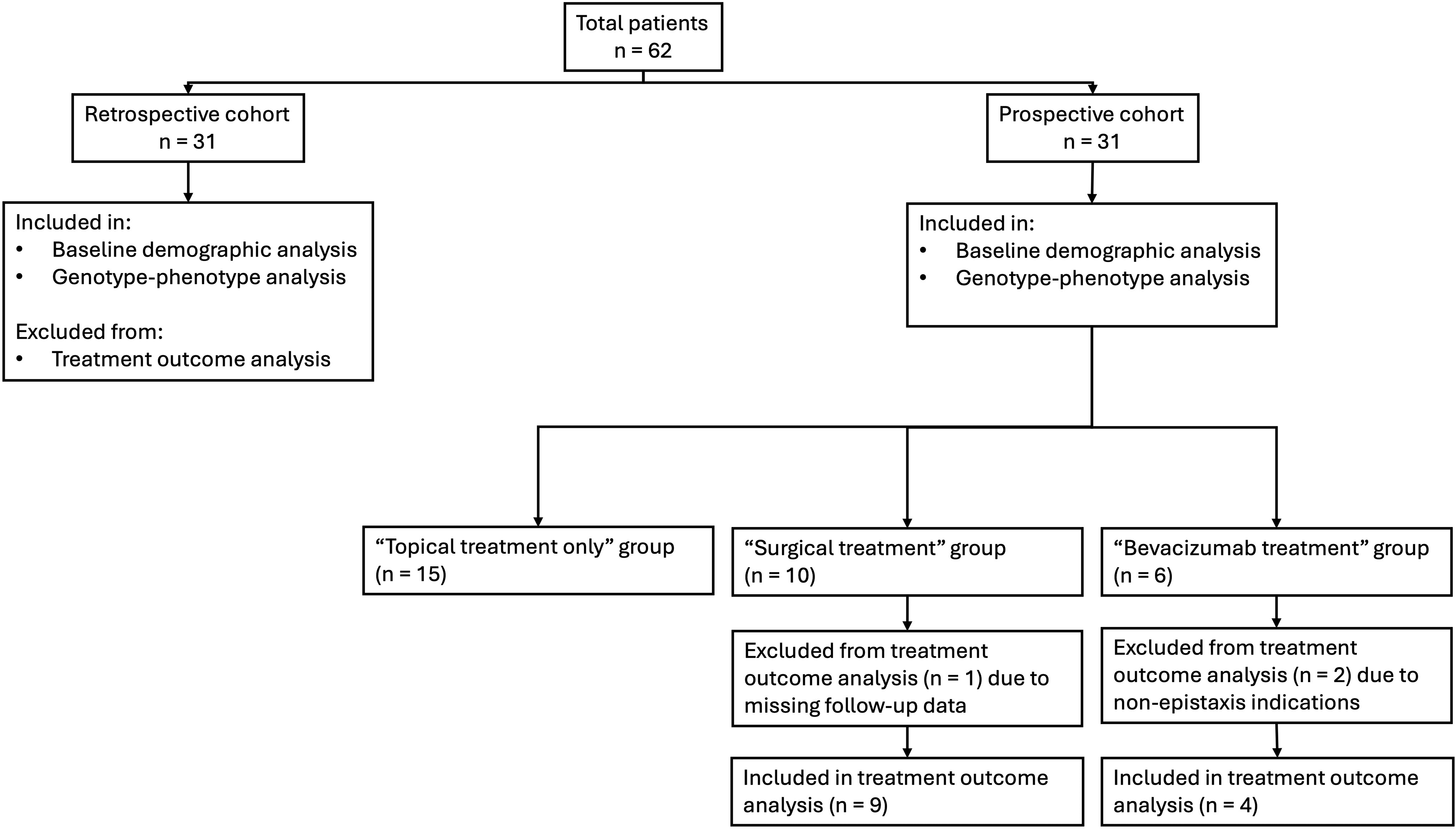
CONSORT-style participant flow diagram demonstrating cohort selection, exclusions, and final analytic sample for treatment and efficacy analyses.
Statistical Analysis
Statistical analyses were performed using Jamovi (Version 2.6.2). Descriptive statistics summarized baseline characteristics for the combined and prospective cohorts. Gene group comparisons were conducted using Chi-square tests for categorical variables and one-way ANOVA or Kruskal-Wallis tests for continuous variables, depending on normality and variance assumptions.
For evaluation of treatment efficacy in the prospective cohort, ESS scores were compared across 3 predefined time points: (1) baseline (first visit), (2) pre-intervention defined as most recent ESS prior to intervention (for patients receiving staged coblation, this corresponds to ESS prior to first coblation), (3) post-intervention, defined as most recent ESS within 3 months after completion of treatment(s) for surgical intervention and 6 months after bevacizumab initiation. Patients with missing follow-up data or those who received bevacizumab for non-epistaxis indications were excluded from comparative analysis. Repeated-measures ANOVA was used to evaluate changes in ESS over time. Assumptions of normality and sphericity were assessed, and Greenhouse-Geisser corrections were applied where violations occurred. Statistical significance was defined as P < .05.
Results
Baseline Characteristics
Baseline Demographic Data for Overall and Treatment Cohorts of Patients from the HHT Clinic.
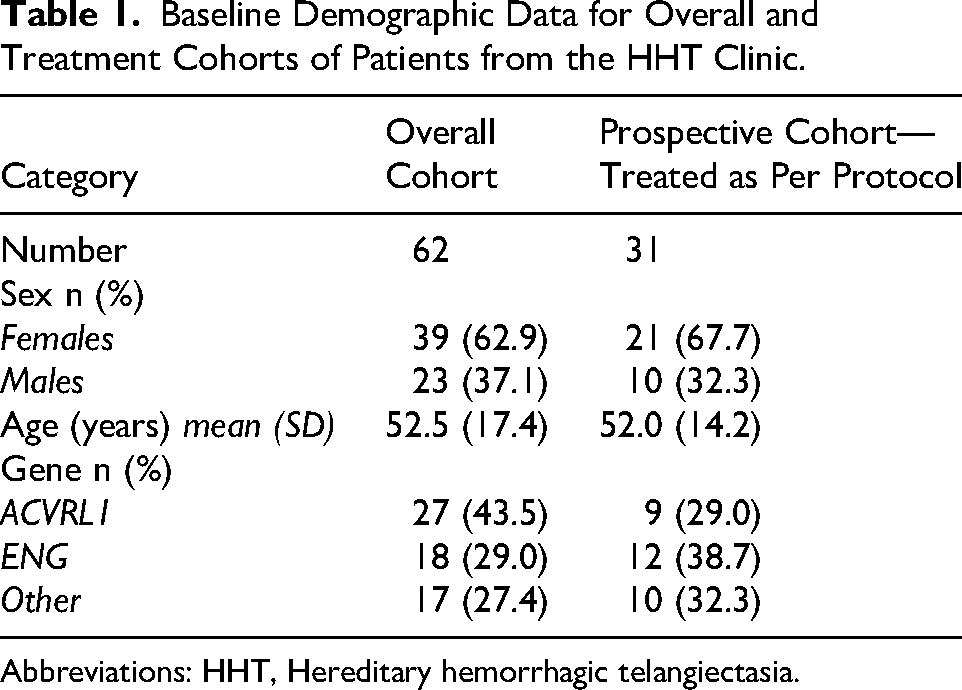
Abbreviations: HHT, Hereditary hemorrhagic telangiectasia.
Among the prospective cohort, there was a female predominance (21 patients, 67.7%) and a mean age of 52.0 ± 14.2 years. The most commonly identified gene was ENG (12 patients, 38.7%), followed by ACVRL1 (9 patients, 29.0%). The remaining 10 patients (32.3%) were categorized as “Other.”
Genotype-Phenotype Relationships
Comparison of Frequency of Arteriovenous Malformations by Genotype.

Abbreviations: AVM, arteriovenous malformation.
Comparison of Age, Baseline ESS Scores by Genotype.

Abbreviations: ESS, epistaxis severity score.
Treatment Pathways and Outcomes
At time of analysis, the epistaxis symptoms for 15 patients (48.4%) were well controlled with topical treatment alone. 10 patients (32.3%) required surgical interventions, and 6 (19.4%) received systemic bevacizumab. Of the 6 patients who received bevacizumab, 3 also received surgical intervention prior to this as part of the treatment protocol with little to no improvement. Of the remaining 3, one was not suitable for surgical intervention prior to bevacizumab initiation and 2 received bevacizumab treatment for primarily non-epistaxis indications (severe and refractory gastrointestinal bleeding).
Comparison of Baseline ESS and Genotype by Treatment Modality Subsequently Received.
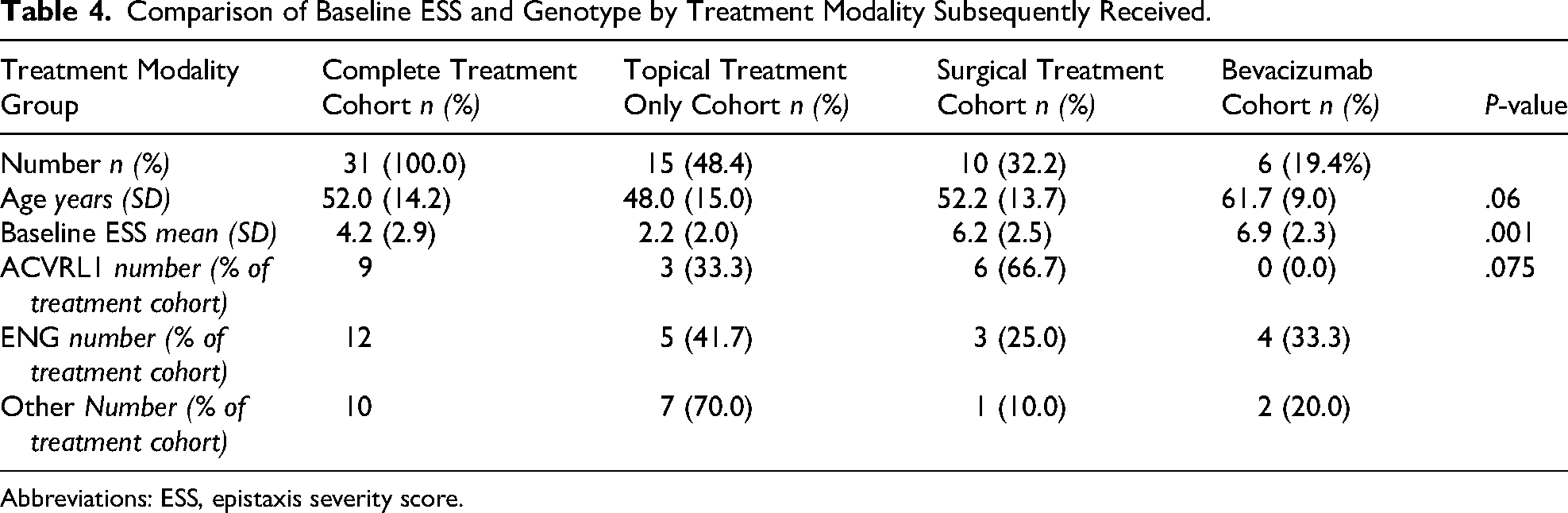
Abbreviations: ESS, epistaxis severity score.
Complete follow-up data were available for 9 (of 10) patients who underwent surgical treatment and for 4 patients who received bevacizumab for recalcitrant epistaxis. The 2 patients who received bevacizumab for non-epistaxis indications were excluded from this analysis.
In the “Surgical treatment” cohort, ESS scores showed non-significant change from baseline to the pre-intervention visit, despite maximal topical treatment (P = .185). However, postoperatively, patients demonstrated statistically significant improvements of 4.3 points (P = .006) in ESS scores within the 3-month period. Patients in the “Bevacizumab” cohort also showed non-significant change prior to treatments, both topically and surgically, (P = .626) but received marked improvement of ESS 4.7 points (P = .038) in ESS scores post-intervention within the 6-month period (Figure 3).
Heterogeneous Clinical Trajectories and Treatment Response
Longitudinal clinical trajectories for all patients with complete follow-up data are presented in Figures 3 and 4, including 9 patients undergoing surgical treatment and 4 patients receiving bevacizumab therapy.
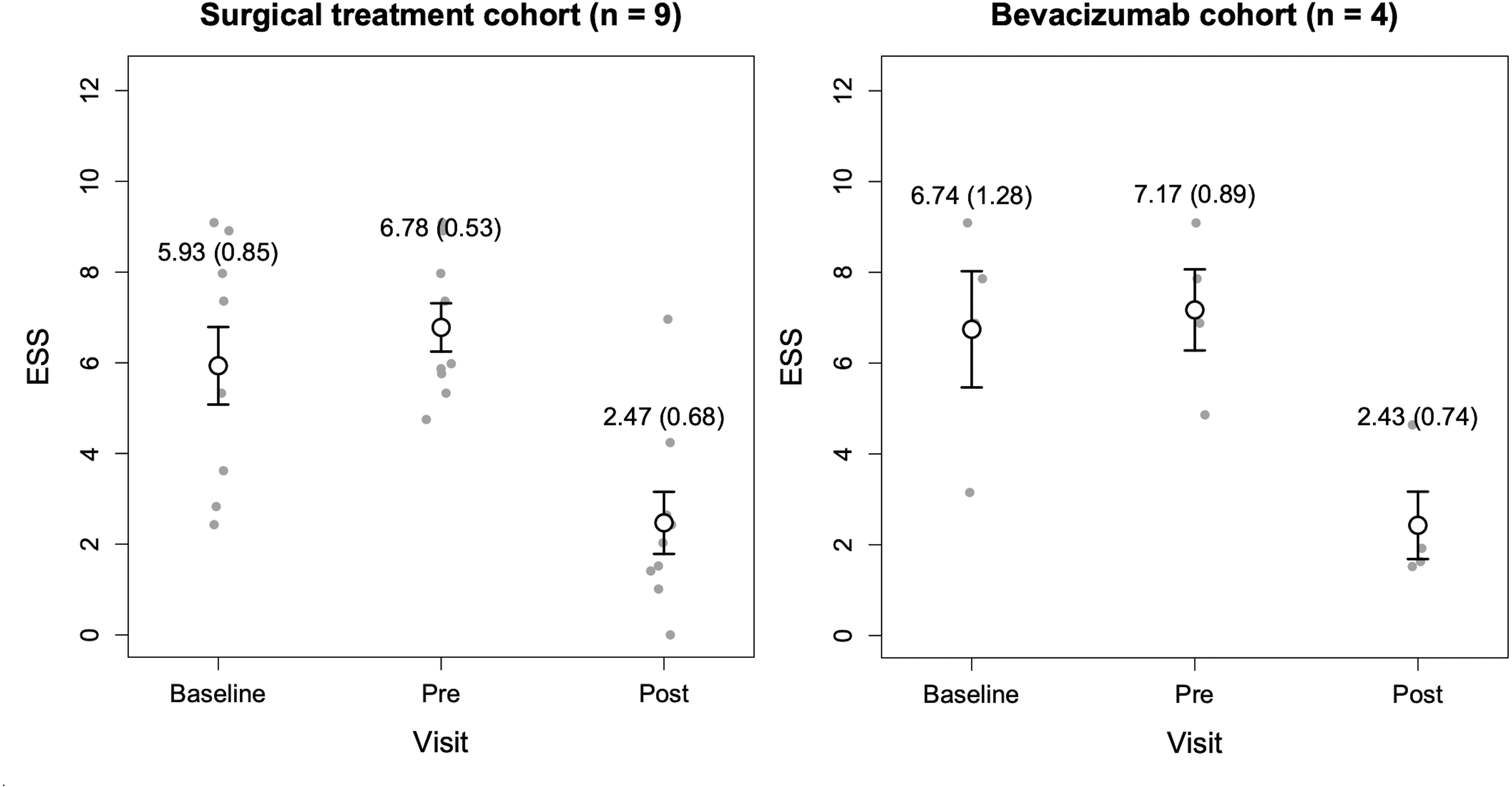
Comparative analysis of mean epistaxis severity scores at baseline, pre-intervention, and post-intervention for the surgical treatment and bevacizumab groups. Error bars represent standard error.
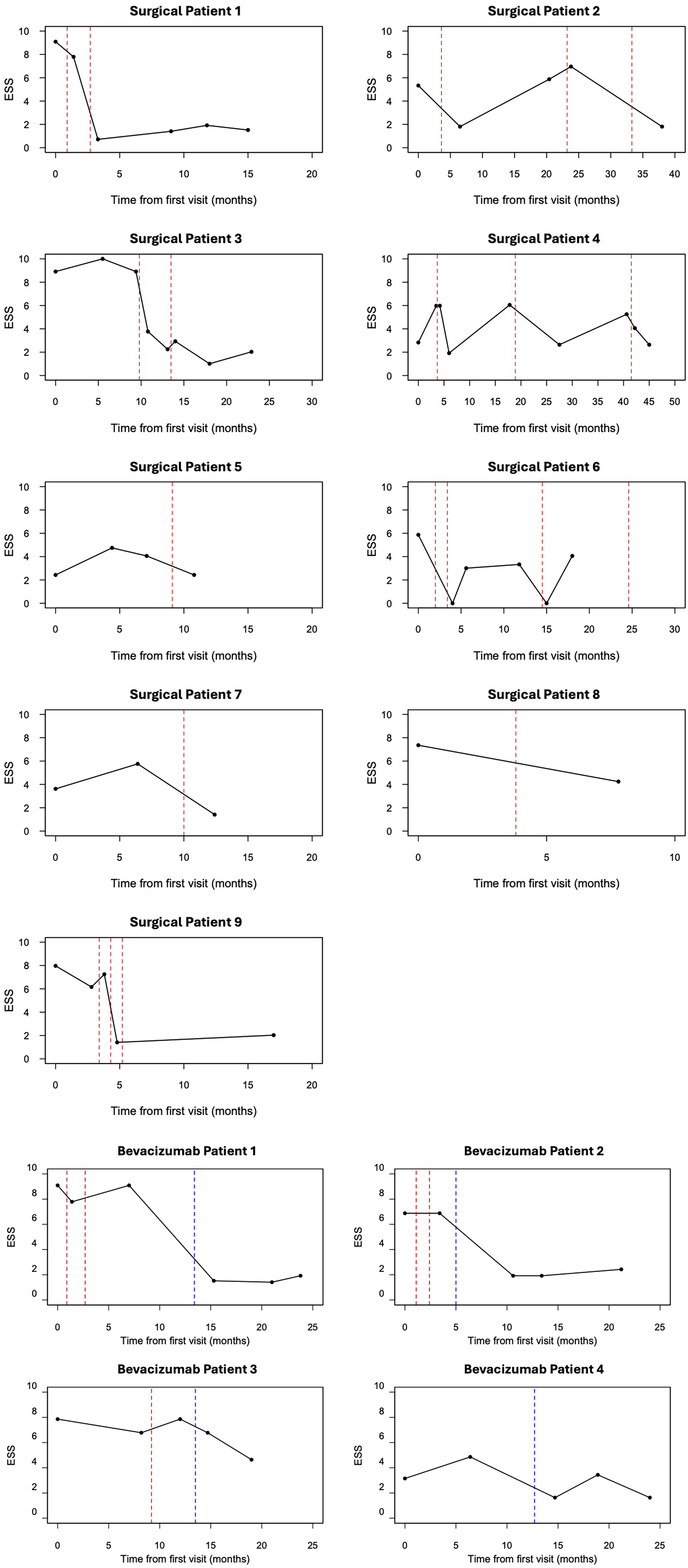
Longitudinal ESS trajectories for patients undergoing surgical and bevacizumab treatment. Red dashed lines indicate timing of surgical interventions and blue dashed lines indicate bevacizumab treatment. ESS, epistaxis severity score.
Considerable heterogeneity in both baseline severity and treatment response was observed. In the surgical cohort, many patients demonstrated improvement in ESS following intervention; however, the magnitude and durability of response varied. Some patients (Figure 3—surgical patients 1, 3, and 7) showed marked and sustained improvement following a single set of surgical treatments, whereas others (Figure 3—surgical patients 2, 4, 6) demonstrated recurrence of symptoms after an initial response, necessitating repeated interventions over time. All patients are maintained on topical treatments, which commenced the following day post-surgical ablation.
Among patients receiving bevacizumab, treatment was typically initiated in the context of refractory disease or rapid recurrence of epistaxis following prior interventions. We observed that improvement in epistaxis control generally occurs after 3 weeks of commencing the bevacizumab treatment. Patient 4 had significant co-morbidities (notably body mass index of 55), precluding safe administration of a general anesthetic. The patient was offered an escalation with bevacizumab infusion after a period of topical treatment.
Discussion
To our knowledge, this is among the first studies, both in an Australian and international context, to present a standardized protocol for the management of HHT-related epistaxis. It incorporates both existing guideline-recommended therapies and emerging therapies in a stepwise escalation pathway, with the intent of matching level of treatment escalation to the patient's symptom burden, with the aim of reducing overtreatment and treatment-related complications.
Notably, nearly half of the patients were successfully managed with protocolized topical therapy alone. In a country such as Australia, Canada and America, characterized by large geographic distances and substantial rural populations, this model enables local practitioners to initiate evidence-based management while maintaining referral pathways to specialist multidisciplinary services. Patients who fail topical therapy can then be appropriately escalated to surgical intervention or systemic bevacizumab treatment within specialized centers.
Heterogeneous Cohort Seen at Multidisciplinary Clinic
The average age at presentation was approximately 50 years, despite epistaxis typically beginning in adolescence. 8 This likely reflects delayed specialist referral due to mild early symptoms, limited awareness of HHT, and geographic barriers.9–12
The genetic distribution mirrored international data, with ACVRL1 and ENG mutations comprising the majority of cases. Although ENG mutations have been associated with earlier epistaxis onset, we observed no significant differences in age at presentation or baseline ESS between genotypes, likely reflecting referral once a threshold symptom burden was reached. 13
As expected, AVM distribution varied significantly by genotype. AVM distribution varied by genotype, with ENG mutations associated with a higher prevalence of pulmonary AVMs, consistent with established genotype-phenotype associations (66.6% vs 7.4%, P < .001). 3 Differences in cerebral and hepatic AVM patterns reported elsewhere were not observed, potentially reflecting incomplete screening data.
Rationale and Efficacy of Tiered Protocol
The most salient finding was that nearly half of the patient cohort was managed on topical treatment alone. For those requiring escalation, significant improvements in ESS were observed following both surgical intervention (ΔESS: 4.31, P = .006) and bevacizumab treatment (ΔESS: 4.74, P = .005). Noting that the minimum clinically important difference for this scoring tool was 0.71, these changes represent significant improvements. 14 It is important to appreciate that the nasal telangiectasia typically progresses over time, leading to recurrent symptoms and the need for repeated interventions. Accordingly, this protocol emphasizes ongoing topical therapy as a maintenance strategy.
Based on emerging evidence, topical timolol was incorporated into the protocol, selected for its accessibility as a 0.5% ophthalmic formulation. Randomized controlled trials have shown mixed results, with modest benefit reported in some studies.15,16 Given its favorable safety profile and ease of application, timolol was maintained across all tiers of the protocol. Tolerability was generally good, with only one patient discontinuing timolol due to asthma exacerbation and a small number discontinuing adjunctive moisturizing therapies because of unpleasant taste or stickiness.
The second international HHT guidelines recommend consideration of oral tranexamic acid for epistaxis not controlled by topical therapies. 5 While supported by high-quality evidence, its clinical benefit is modest, and caution is advised in patients with thromboembolic risk. In our practice, we adopt a more cautious approach. Tranexamic acid is used selectively as an interim therapy rather than a routine step in the escalation pathway. This reflects thromboembolic events observed locally, including a young patient who developed a saddle pulmonary embolism after 2 years of continuous oral use, despite a lack of thrombophilia or related risk factors being identified on extensive work-up.
For patients requiring treatment escalation, the choice of surgical modality was guided by telangiectasia morphology. Coblation (EVAC 70 or Precise EZ View) was preferentially used for larger or more confluent telangiectasias. 6 In contrast, KTP or TruBlue laser therapy was employed for smaller, punctate lesions, given their vascular selectivity and ability to ablate telangiectasias while minimizing collateral mucosal injury. 17
Sclerotherapy was not included in the current protocol due to limited local expertise; however, we acknowledge emerging evidence and recent consensus recommendations supporting its use and are exploring its incorporation into future iterations of the protocol.18,19
Septodermoplasty and nasal closure are recognized salvage options for severe, refractory disease; however, in our cohort, symptom control was achieved using less invasive measures, and these procedures were not required. Given their associated morbidity, including crusting, altered nasal physiology, and potential impact on quality of life, we did not incorporate them into the routine protocol.20,21
Bevacizumab was utilized in a small subset of patients with refractory disease following either failure of topical and surgical therapies or, in one case, because they were not suitable for surgical intervention. Those who failed surgical treatment often demonstrated a rapid regrowth and confluence of telangiectasias soon after intervention. While there is emerging evidence supporting its use in HHT-related epistaxis, it is not currently an approved or routinely funded therapy for this indication, and its role remains investigational. In our protocol, bevacizumab is reserved as a later-line option, reflecting both its systemic effects and the need for careful patient selection. Given the small number of patients and heterogeneity of clinical presentations in this cohort, conclusions regarding its efficacy or optimal positioning within the treatment pathway should be interpreted with caution.
Factors Involving Treatment Response
Variability in responsiveness to treatment can be influenced by patient factors. Lack of adherence to topical therapy can be an issue and needs to be addressed prior to any escalation. Environmental factors, such as smoking or level of air humidity, can increase the friability of the nasal mucosa. All patients who are current smokers in the clinic were counseled regarding smoking cessation. Comorbidities can also influence treatment selection; for example, asthma may limit the use of topical beta-blockers, while significant medical comorbidities may preclude general anesthesia and necessitate alternative treatment pathways. Patients who engaged in strenuous physical activity could potentially trigger more frequent epistaxis episodes, thereby escalating the need for surgical ablation.
Disease-related factors can also play a major role. Prior studies note that location, density, and morphology of telangiectasias can significantly impact the severity of epistaxis, with diffuse vasculature, anterior septal involvement, and larger telangiectasias linked to more severe epistaxis.22–24 Furthermore, it is possible that some lesions, depending on their location, may be less amenable to topical treatment, compared to others, thus resulting in a variable response.
Limitations and Future Directions
The main limitation of this study is the small sample size, reflecting the rarity of HHT and limiting detailed subgroup analysis. As this study was conducted in a real-world clinic setting, follow-up intervals varied and were not strictly standardized, which introduces some inconsistency but, on the other hand, provides a practical view of how the protocol works in routine care. Its monocentric, observational design precludes strong causal inferences.
Nearly half of the patients were successfully managed with topical therapy alone; however, this finding should be interpreted cautiously. ESS outcomes for this group were not analyzed due to limited early follow-up data, as these patients are typically reviewed at longer intervals (∼12 months) precluding meaningful short-term comparisons, though prior work from our group has demonstrated modest improvements in ESS with topical therapy25. In the absence of a comparator group, definitive conclusions regarding protocol efficacy or its ability to prevent overtreatment cannot be drawn. Instead, these findings represent indirect, non-comparative support for a stepwise approach. Future comparative studies incorporating treatment utilization metrics (eg, operative frequency, infusion burden, and emergency presentations) are warranted to more definitively evaluate protocol efficacy.
Preliminary data suggest that higher ESS scores and specific endoscopic features could help stratify patients for earlier escalation. 22 It is also possible that different telangiectasia phenotypes respond differently to various treatment modalities. Continued work to systematically phenotype patients at presentation will help optimize progression through the treatment protocol and outcomes within the clinic.
Supplemental Material
sj-docx-1-ajr-10.1177_19458924261459226 - Supplemental material for Implementation and Outcomes of a Structured Epistaxis Protocol in Hereditary Hemorrhagic Telangiectasia: An Observational Cohort Study from a Multidisciplinary Clinic
Supplemental material, sj-docx-1-ajr-10.1177_19458924261459226 for Implementation and Outcomes of a Structured Epistaxis Protocol in Hereditary Hemorrhagic Telangiectasia: An Observational Cohort Study from a Multidisciplinary Clinic by Niridu Peiris, Raymond Hayler, Kathleen Le Marquand, Pak Leng Cheong, Lisa Worgan, Edmund Lau and Tsu-Hui (Hubert) Low in American Journal of Rhinology & Allergy
Footnotes
Ethics Approval Statement
The study was approved by the Sydney Local Health District Human Research Ethics Committee (2023/ETH00644). All participants provided written informed consent prior to participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated analyzed during the current study are not publicly available due to participant confidentiality but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.