
Abstract
Background
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a chronic inflammatory condition affecting the sinuses, resulting in the appearance of nasal polyps and is often associated with comorbidities. Many cases do not respond to corticosteroid treatment or surgery.
Objective
This study aimed to explore the role of tezepelumab in the treatment of CRSwNP.
Methods
Pubmed, Embase, Scopus, Web of Science, and Cochrane Library were searched. Three randomized controlled trials (RCTs) comparing tezepelumab and placebo in 655 patients with CRSwNP were included. The main outcomes were nasal polyp size (nasal polyp score, NPS), nasal congestion or obstruction (nasal congestion score, NCS), and quality of life using the sino-nasal outcome test (SNOT-22).
Results
Three RCTS were included, in which tezepelumab was used to treat CRSwNP. The mean age was 50.9 years, with 56.9% male patients and 75.6% of patients with coexisting asthma. The mean difference (MD) for NPS ranged from −0.9 to −2.0 compared to placebo. Consistent benefits were observed for NCS with MD between −0.8 and −1.0 compared to placebo and SNOT-22 with MD ranging from −10 to −28 points compared to placebo.
Conclusion
In conclusion, evidence suggests that tezepelumab may improve NPS and NCS, SNOT-22, loss of sense of smell, and clinically relevant endpoints (reduced need for surgery and corticosteroid use), as demonstrated in all included trials. However, the certainty and clinical applicability remain limited due to small trial size, industry sponsorship, and the lack of direct comparison with standard management and endoscopic sinus surgery. Large-scale, independent clinical trials are needed to confirm the position of tezepelumab in clinical practice for patients with moderate to severe CRSwNP.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is a chronic inflammatory disease of the nasal and paranasal sinuses that affects approximately 10%-15% of adults. It is classified into 2 subtypes: CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). 1 CRSwNP is a multifactorial condition that may arise from genetic or environmental influences and is frequently associated with asthma, as both conditions are driven by type 2 (T2) inflammation with eosinophilic tissue infiltration. 2 When the 2 disorders coexist, they are linked to more severe disease and poor asthma control, leading to marked reductions in quality of life, work productivity, and overall treatment burden. Patients frequently experience loss of smell, nasal obstruction, facial pressure, and sleep disturbance, symptoms that persist for years and often recur despite medical and surgical treatment. 3
Surgical treatment is often indicated when CRSwNP is not adequately controlled with corticosteroids; however, recurrence is frequent and surgery carries inherent risks. The introduction of biologic therapies has reshaped management, particularly in patients with refractory disease. 4 Most approved biologics for asthma have also shown effectiveness in CRSwNP by targeting downstream mediators of T2 inflammation. Among them, dupilumab is a monoclonal antibody that blocks the signaling of interleukin-4 (IL-4) and interleukin-13 (IL-13), 2 cytokines crucial for the initiation and amplification of the type 2 response. 5 Omalizumab, a recombinant humanized IgG1 anti-IgE antibody, acts by binding to the high-affinity IgE receptor present on mast cells, basophils, and eosinophils, thereby preventing IgE-mediated activation. 5 Mepolizumab, an anti-interlukin-5 monoclonal antibody, prevents interleukin-5 (IL-5) from binding to eosinophils, resulting in a significant decrease in its blood levels. 6 These agents act at earlier checkpoints within the inflammatory cascade but still operate downstream of tezepelumab, which neutralizes the upstream epithelial alarmin thymic stromal lymphopoietin (TSLP) and influences multiple effector pathways simultaneously. 7
Tezepelumab is a fully human monoclonal antibody that binds TSLP with high affinity, preventing its interaction with the receptor complex and thereby downregulating the activation of dendritic cells, ILC2 s, and Th2 lymphocytes. While tezepelumab is approved for asthma, its role in CRSwNP is still being investigated. 7 Recent randomized controlled trials (RCTs) have begun to address this question, but the available evidence remains limited. This emerging line of research suggests that targeting TSLP could represent a promising therapeutic strategy, particularly for patients with recurrent disease, yet further evaluation is needed to clarify its clinical impact and long-term benefits. Therefore, the aim of this systematic review is to evaluate the efficacy and safety of tezepelumab in adult patients with CRSwNP by synthesizing data from RCTs.
Materials and Methods
This systematic review was performed and reported in accordance with the Cochrane Collaboration Handbook for Systematic Review of Interventions 8 and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Statement Guidelines. 9 The protocol was prospectively registered in PROSPERO (CRD420251185626).
Eligibility Criteria
The included trials predominantly enrolled adults with moderate-to-severe bilateral CRSwNP inadequately controlled despite ongoing intranasal corticosteroid therapy. Most studies required elevated baseline nasal polyp scores (NPSs) and persistent symptom burden. A substantial proportion of participants had prior exposure to systemic corticosteroids and/or previous endoscopic sinus surgery, reflecting a population with difficult-to-treat disease. Definitions of disease severity and control status varied slightly across trials, particularly regarding prior systemic corticosteroid exposure and surgical history, which may contribute to clinical heterogeneity.
Inclusion in this systematic review was restricted to studies that met all of the following eligibility criteria: (1) RCT (2) comparing tezepelumab, irrespective of dose or administration schedule, to placebo (3) enrolling patients who have confirmed diagnosis of CRSwNP according to established clinical criteria (eg, EPOS) (4) with no time restriction on follow-up (5) reporting of at least one of the prespecified clinical outcomes of interest. We excluded studies with (1) no control group (2) studies focusing on non-polypoid CRS or asthma without confirmed CRSwNP (3) evaluation of biologics other than tezepelumab (4) tezepelumab investigated for conditions unrelated to CRSwNP (5) duplicate or overlapping data (6)non-randomized or uncontrolled designs (7) animal or in vitro studies.
Search Strategy
We systematically searched PubMed, Embase, Cochrane, Web of Science, and Scopus from inception to May 2025. The following Boolean search string was applied: (Tezepelumab OR “Thymic stromal lymphopoietin”) AND (“Chronic Rhinosinusitis” OR Rhinosinusitis OR “Chronic sinusitis” OR “Ethmoid Sinusitis” OR “paranasal sinusitis”) AND (“nasal polyps” OR “sinus polyps”). Reference lists of included trials were also screened manually to identify additional eligible studies. Two reviewers (H.E. and N.S.) independently performed study selection and data extraction using predefined forms, and discrepancies were resolved by consensus, with the involvement of a third reviewer (A.J) when necessary.
Endpoints
The primary outcomes of interest were reduction in nasal polyp size as measured by the NPS, improvement in nasal congestion or obstruction, and health-related quality of life assessed by the sino-nasal outcome test (SNOT-22). Secondary outcomes included the need for systemic corticosteroids or surgical intervention, changes in sense of smell, annualized asthma exacerbation rate, pre-bronchodilator forced expiratory volume in one second (FEV1), fractional exhaled nitric oxide, blood eosinophil counts (BEOs), scores from the asthma control questionnaire-6, and levels of inflammatory cytokines such as IL-5 and IL-13.
Risk of Bias Assessment (Figure 1)
We evaluated the risk of bias in randomized studies using the Cochrane Risk of Bias 2.0 tool (RoB-2). 10 Two reviewers (H.E. and R.P.) independently performed the assessment, and discrepancies were resolved through discussion until consensus was reached.
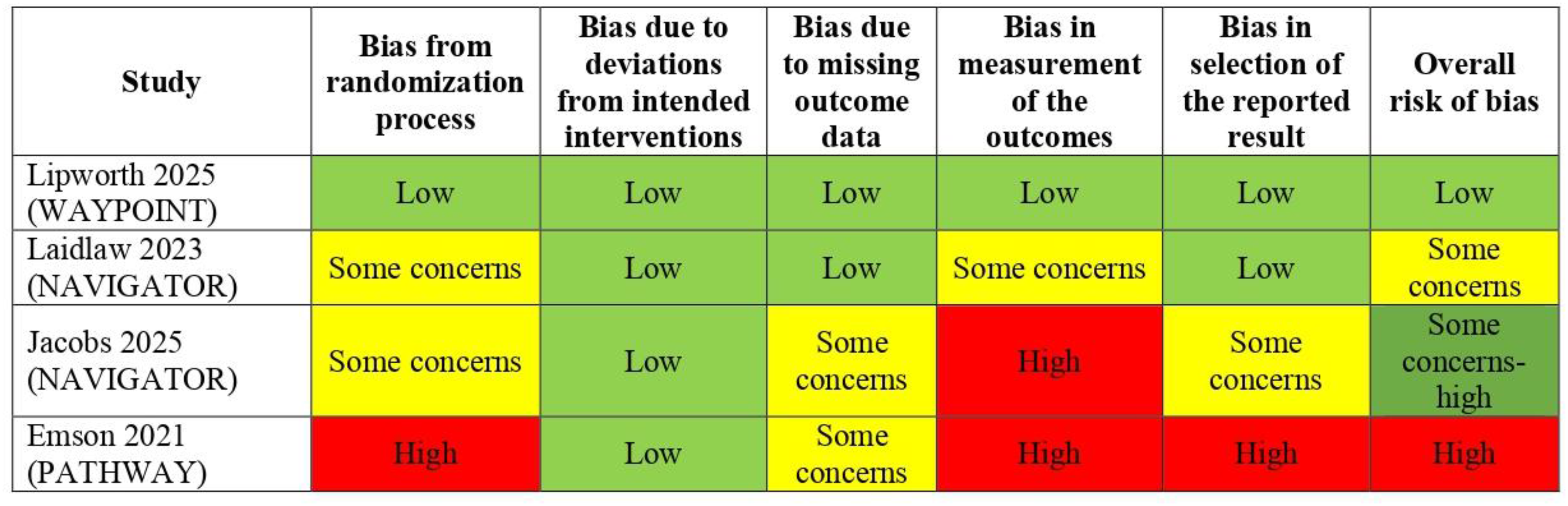
Risk-of-bias assessment across the included randomized controlled trials evaluating tezepelumab in patients with chronic rhinosinusitis with nasal polyps. Domains assessed included bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Judgments are displayed as text within each cell to allow interpretation independent of color. Included trials were WAYPOINT (Lipworth 2025), NAVIGATOR (Laidlaw 2023; Jacobs 2025), and PATHWAY (Emson 2021). 12 14 15
In addition, we extracted the funding sources and sponsorship for each included study (Table 1). Industry sponsorship was not considered as a separate domain of ROB-2; however, it was qualitatively assessed when interpreting the independence, applicability, and certainty of available evidence. 11
Funding Source and Sponsor Involvement of Included Tezepelumab Studies.
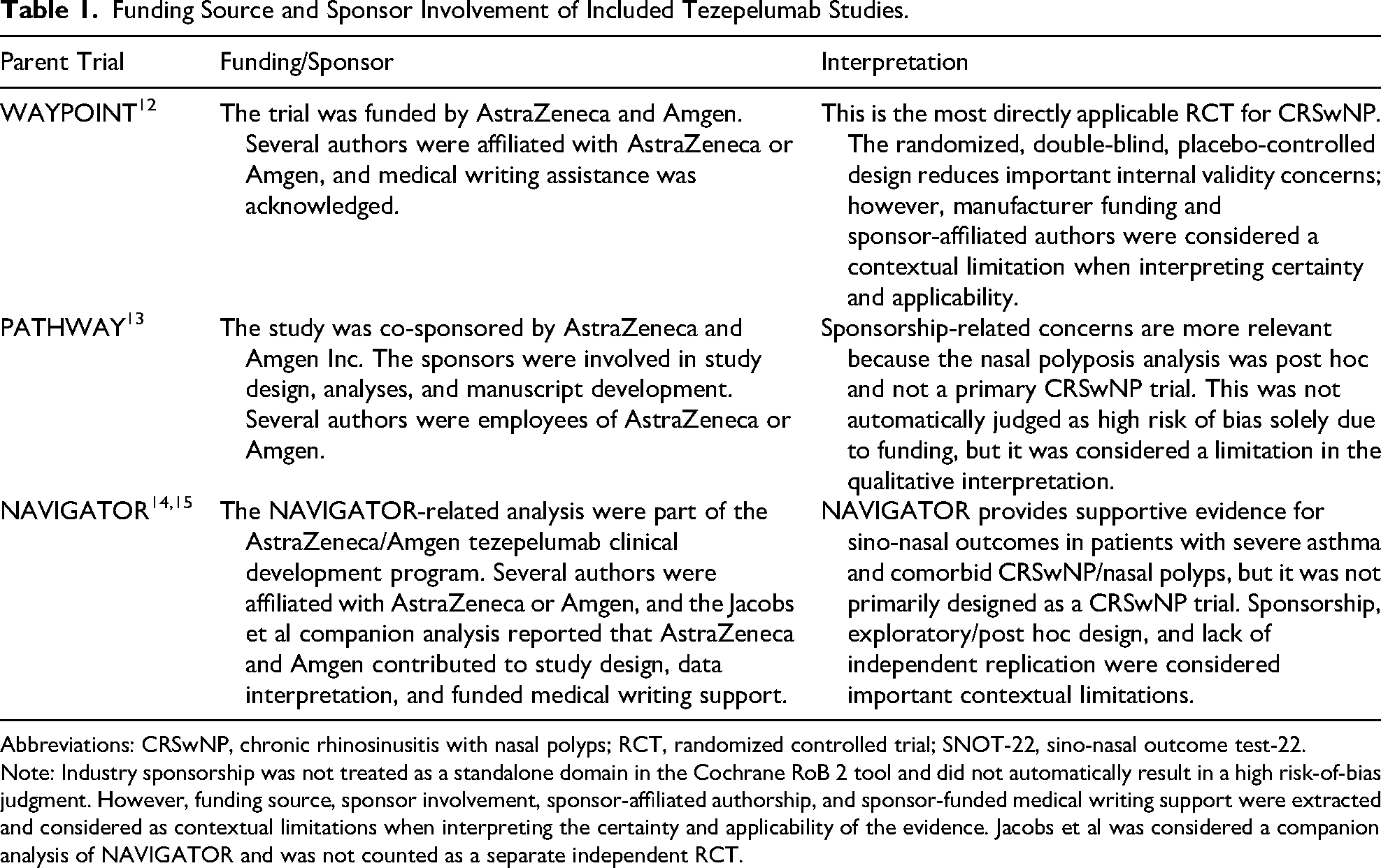
Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyps; RCT, randomized controlled trial; SNOT-22, sino-nasal outcome test-22.
Note: Industry sponsorship was not treated as a standalone domain in the Cochrane RoB 2 tool and did not automatically result in a high risk-of-bias judgment. However, funding source, sponsor involvement, sponsor-affiliated authorship, and sponsor-funded medical writing support were extracted and considered as contextual limitations when interpreting the certainty and applicability of the evidence. Jacobs et al was considered a companion analysis of NAVIGATOR and was not counted as a separate independent RCT.
Results
A total of 780 records were identified through the electronic database search. After removing 391 duplicates, 389 unique studies remained. Of these, 374 were excluded after title and abstract screening, leaving 15 articles for full-text assessment. Following a detailed review, 3 RCTs met the eligibility criteria and were included in the systematic review. Studies were excluded for the following reasons: protocol publication only (n = 4), single-arm trial (n = 1), no subgroup analysis of patients with CRSwNP (n = 1), ongoing trial without published results (n = 1), and unrelated outcomes (n = 1). The study selection process is summarized in Figure 2.
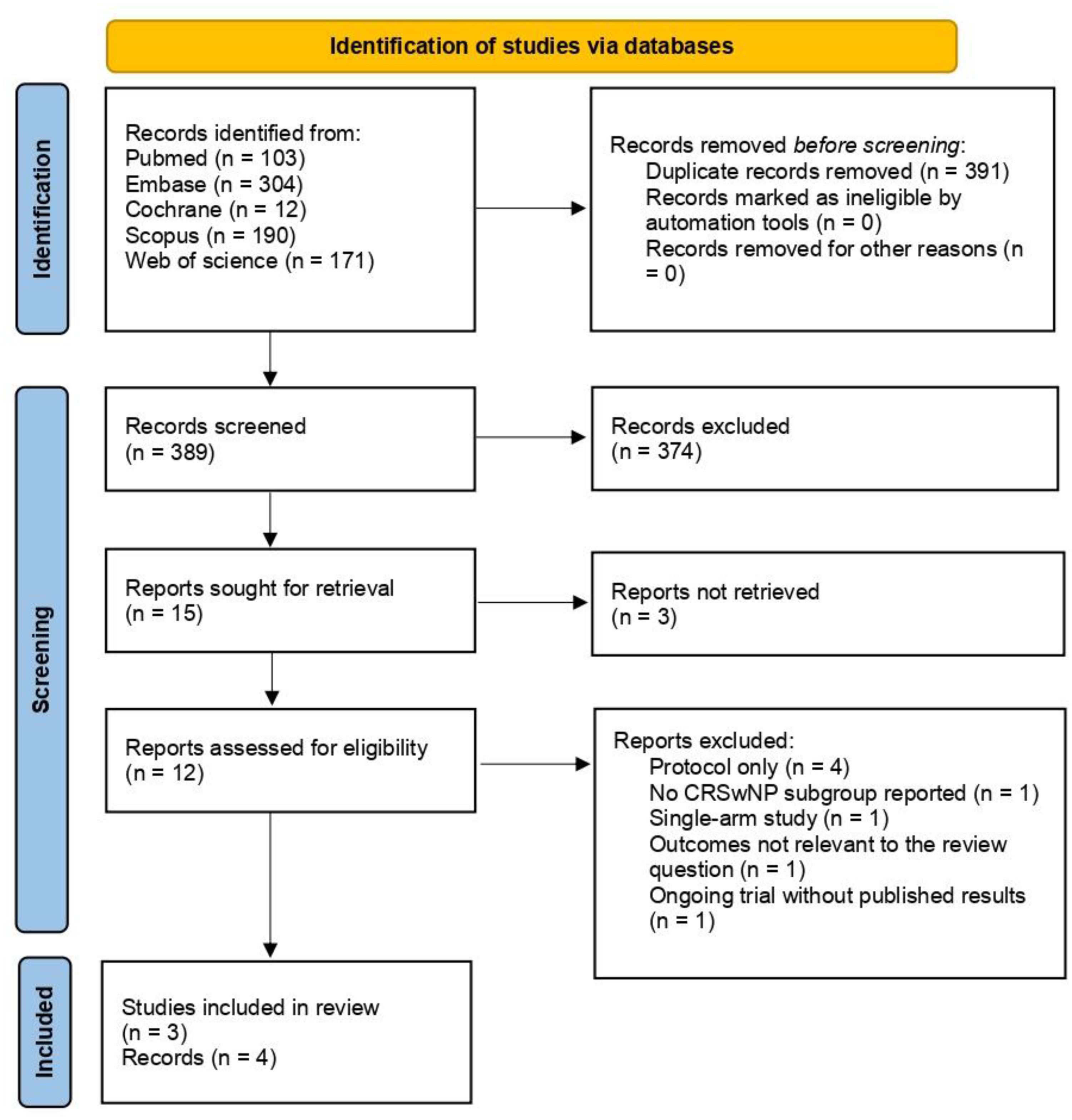
PRISMA 2020 flow diagram of study selection. Flowchart illustrating the identification, screening, eligibility assessment, and inclusion of studies evaluating tezepelumab for chronic rhinosinusitis with nasal polyps (CRSwNP).
Among the eligible studies, three RCTs fulfilled the inclusion criteria, enrolling a total of 655 patients with severe or uncontrolled CRSwNP. These comprised 2 large phase 3 trials (WAYPOINT,12,16), (NAVIGATOR,14,15), and one early-phase 2 trial (PATHWAY, 13 ). For the WAYPOINT and NAVIGATOR trials, both abstracts and full-texts were retrieved; importantly, the PATHWAY trial was the only study to include patients aged ≥12 years, whereas all other trials were restricted to adult populations.
All included trials were placebo-controlled, and the evidence primarily points to tezepelumab efficacy and safety rather than considering it as a direct alternative for endoscopic sinus surgery or optimal medical therapy and corticosteroids.
Baseline Characteristics of Included Studies
Study durations ranged from 16 to 52 weeks, and all compared 210 mg of subcutaneous tezepelumab with placebo, administered every 4 weeks in addition to standard care. Sample sizes varied between ∼80 (Emson C) and over 400 participants (WAYPOINT). Of these, 203 patients in a total of 408 in the first study (Lipworth BJ) received tezepelumab, 90 in a total of 165 in (Jacobs J) study, and 23 in a total of 82 in the last study (Emson C). The mean age of participants varied across the included trials with a weighted overall mean of 50.9 years. In terms of sex distribution, 56.9% (373) of the 655 participants were male. The detailed sex distribution and age are presented in Table 2. Prior glucocorticoid treatment was also reported in 78.5% of the study population (514 patients).
Baseline Clinical and Demographic Characteristics of Participants Across Included Trials.
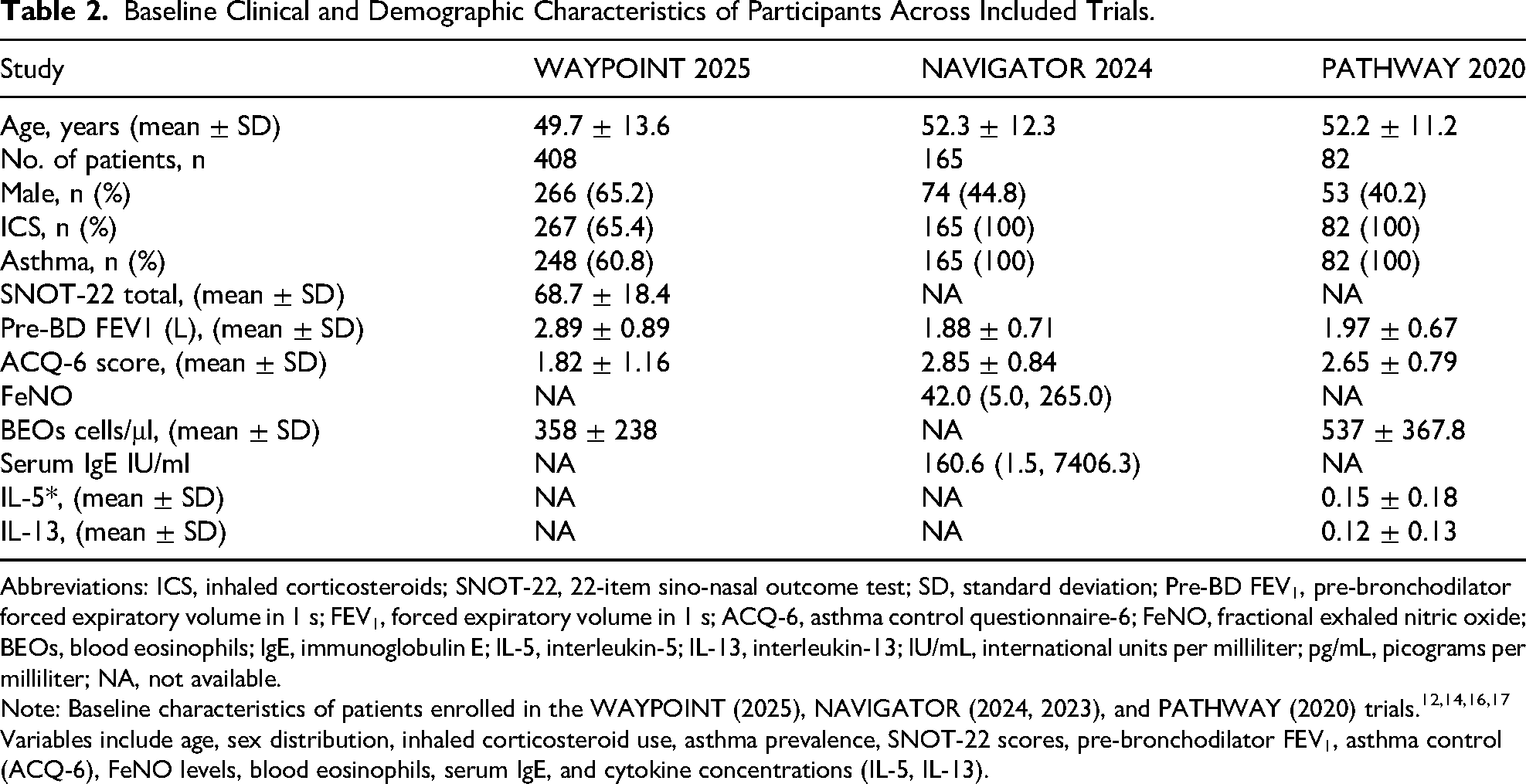
Abbreviations: ICS, inhaled corticosteroids; SNOT-22, 22-item sino-nasal outcome test; SD, standard deviation; Pre-BD FEV1, pre-bronchodilator forced expiratory volume in 1 s; FEV1, forced expiratory volume in 1 s; ACQ-6, asthma control questionnaire-6; FeNO, fractional exhaled nitric oxide; BEOs, blood eosinophils; IgE, immunoglobulin E; IL-5, interleukin-5; IL-13, interleukin-13; IU/mL, international units per milliliter; pg/mL, picograms per milliliter; NA, not available.
Note: Baseline characteristics of patients enrolled in the WAYPOINT (2025), NAVIGATOR (2024, 2023), and PATHWAY (2020) trials.12,14,16,17 Variables include age, sex distribution, inhaled corticosteroid use, asthma prevalence, SNOT-22 scores, pre-bronchodilator FEV1, asthma control (ACQ-6), FeNO levels, blood eosinophils, serum IgE, and cytokine concentrations (IL-5, IL-13).
Efficacy Outcomes
Across all 3 trials, tezepelumab consistently demonstrated superiority over placebo in across the included trials, tezepelumab consistently outperformed placebo in reducing objective disease measures. NPS was reported in Emson 2021 and Lipworth 2025, both showing modest but favorable reductions versus placebo (approximately −0.9 in Emson 2021 at week 16 and −2.0 in Brian 2025 at week 52). Nasal congestion score (NCS) was likewise assessed in Emson 2021 and Lipworth 2025, demonstrating consistent improvements (about −0.8 to −1.0). These findings indicate that tezepelumab provides measurable benefits across early-phase and later-phase trials for polyp size and nasal obstruction.
Patient-Reported Outcomes
Patient-reported outcomes (SNOT-22) were exclusively available from the 3 later trials—Tanya 2023, Jacobs 2025, and Lipworth 2025. All 3 showed clinically meaningful reductions, with mean differences (MDs) ranging from −10 to −28 compared with placebo. The largest improvement was observed in Lipworth 2025, while Tanya 2023 and Jacobs 2025 demonstrated moderate but consistent benefit (approximately −10 to −12). These findings support tezepelumab's impact on global symptom burden and quality of life in CRSwNP.
Radiological and Surgical Outcomes
Radiological results paralleled clinical improvements. Both phase 3 studies reported significant reductions in the Lund-Mackay CT score (MD −4.5 to −5.7; P < .001). Importantly, the phase 3 WAYPOINT trial showed a marked reduction in the need for rescue surgery (0.5% vs 22.1%; HR 0.02) and systemic corticosteroids (5.2% vs 18.3%; HR 0.12), highlighting a meaningful decrease in treatment burden for severe CRSwNP.
Safety Outcomes
Safety outcomes were favorable, with tezepelumab generally well-tolerated across all studies. Adverse events occurred at rates comparable to placebo, and no new safety signals were identified. The most frequent events—nasopharyngitis, injection-site reactions, and headache—were mild and occurred at similar frequencies in both groups.
Risk of Bias Assessment
Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool for RCTs. 10 Among the included studies, the WAYPOINT trial 12 demonstrated an overall low risk of bias across all assessed domains. The NAVIGATOR trials 15 (Tanya ML et al, 2023) showed some concerns, primarily related to the randomization process and outcome measurement, resulting in an overall judgment of some concerns. In contrast, the PATHWAY trial 13 was judged to be at high risk of bias, mainly due to issues in the randomization process, outcome measurement, and selective reporting. Overall, the risk of bias varied across trials, with higher methodological robustness observed in later-phase studies.
Overall Effect
Taken together, evidence from 3 RCTs consistently supports tezepelumab as an effective and well-tolerated treatment for CRSwNP. The drug demonstrated improvements across objective measures (polyp size, radiological scores), patient-reported outcomes (SNOT-22, loss of smell), and clinically relevant endpoints (reduced surgery and corticosteroid use). These findings underscore tezepelumab's potential as a promising therapeutic option for patients with severe or uncontrolled disease, combining robust efficacy with a favorable safety profile. Results are summarized in Figure 3.
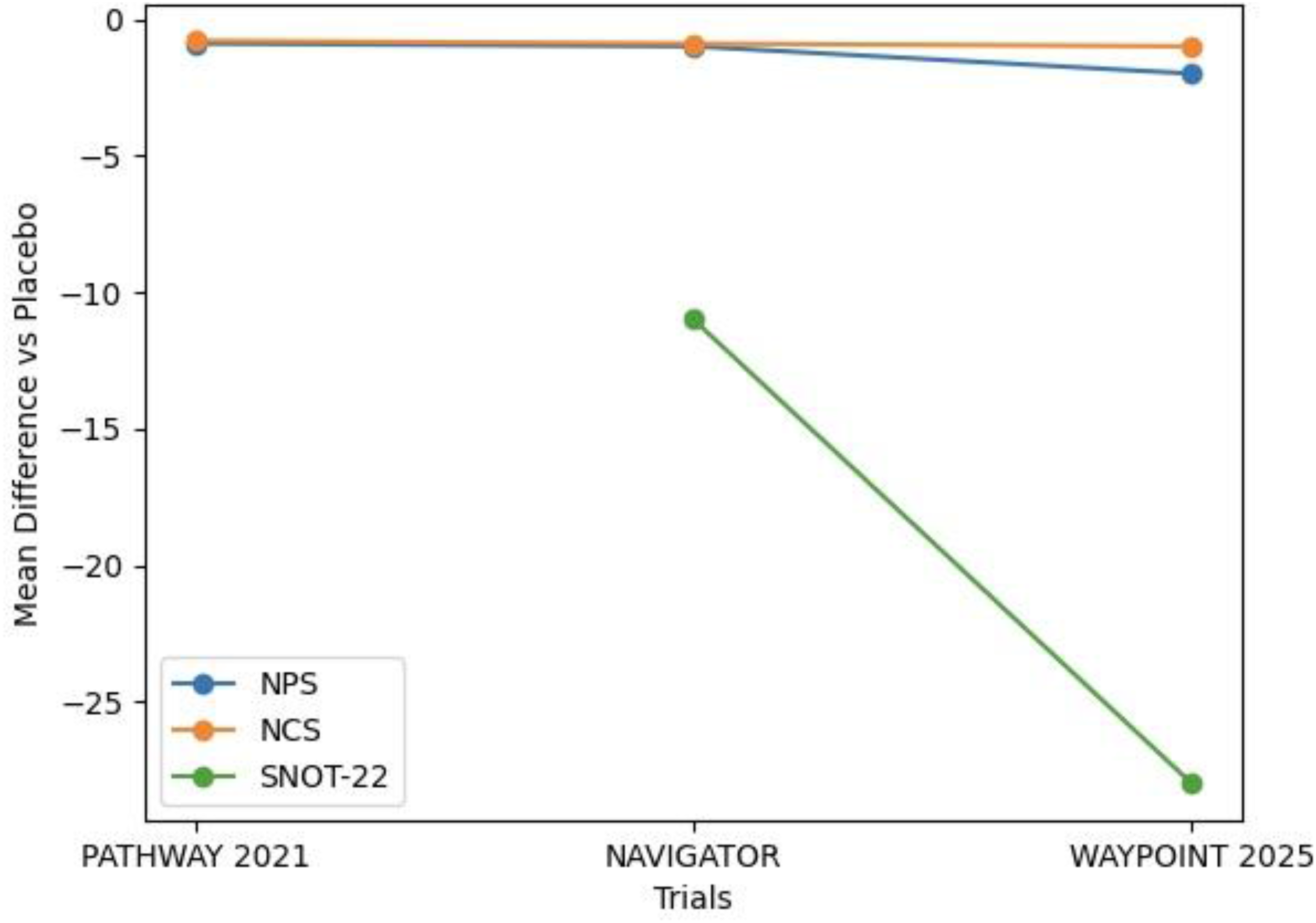
Efficacy outcomes of tezepelumab versus placebo in CRSwNP clinical trials. Mean differences versus placebo are shown for nasal polyp score (NPS), nasal congestion score (NCS), and sino-nasal outcome test-22 (SNOT-22) across included randomized controlled trials.
Discussion
CRS includes a wide range of phenotypes and inflammatory disorders of the nose and paranasal sinuses, affecting approximately 11% of the population in Europe and the USA. 18 According to the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS), CRS (with or without nasal polyps) in adults is defined by the presence of at least 2 symptoms, one of which must be nasal obstruction or nasal discharge (either anterior or posterior), with possible facial pain/pressure and/or olfactory dysfunction, persisting for 12 weeks or longer and confirmed through interview or telephone assessment. CRSwNP corresponds to CRS as defined above, combined with bilateral polyps visualized endoscopically in the middle meatus. 18
CRSwNP is frequently driven by type 2 inflammation and tends to evolve with exacerbations. Standard management includes intranasal corticosteroids, saline irrigation, short courses of systemic corticosteroids, and in many cases, lead to endoscopic sinus surgery. 19 The introduction of biologic therapies targeting type 2 pathways has significantly improved the management of difficult-to-treat CRSwNP. 20 Compared with other chronic inflammatory disorders, some of which are far less common, CRS remains under-investigated, particularly regarding the development of targeted treatments, reflecting a persistent underestimation of its clinical impact. 7 Managing CRSwNP can be particularly complex when maximal medical therapy, including intranasal corticosteroids, and even endoscopic sinus surgery fail to achieve adequate disease control. Many patients also present with comorbid type 2 conditions such as asthma. 19
TSLP plays a central role in asthma pathophysiology, as demonstrated by the efficacy of tezepelumab, the first anti-TSLP monoclonal antibody approved for both T2-high and T2-low severe asthma. Its involvement in CRSwNP is supported by genetic and mechanistic evidence showing that TSLP orchestrates type 2 inflammation and may influence non-type 2 pathways as well. 21 Approximately 1 patient out of 5 remains uncontrolled despite appropriate therapy, this reflects the heterogeneity of the underlying disease, the high disease severity at the start of the study, and the well-defined response criteria in the trial, rather than the inappropriate use of treatment. 7 Biologic agents have therefore emerged as a promising option for CRSwNP. To date, dupilumab is the only FDA-approved biologic specifically indicated for CRSwNP. 22
Several targeted monoclonal antibodies have become available for inflammatory diseases relevant to otolaryngology and allergy, but treatment selection should be individualized according to disease severity, prior treatment response, presence of other concomitant diseases, accessibility, and cost. 23 Anti-TSLP (tezepelumab) or anti-IL4Rα (dupilumab) provide the best improvements in coprimary end points of nasal polyp and congestion score compared with other biologics including anti-IL5/5Rα (mepolizumab, depemokimab, and benralizumab) and anti-IgE (omalizumab). 20 Corticosteroids and surgery have long been the mainstay of therapy for eosinophilic CRS, yet biologics such as mepolizumab, benralizumab, and tezepelumab have shown greater benefit in patients with asthma associated with nasal polyps than in those without polyps. 24 Initial guidance for biologic use relied on EPOS 2020 and EUFOREA recommendations, despite limited evidence regarding indications, response criteria, and treatment duration. Updated guidance issued in the EPOS/EUFOREA 2023 revision has since refined these elements.17,18
Most patients with CRSwNP exhibit type 2 inflammatory features, typically reflected by elevated eosinophil counts in blood and polyp tissue. Core treatment remains based on high-dose intranasal corticosteroids, with systemic corticosteroids and antibiotics used during acute exacerbations. 25 The latest recommendations define biologic eligibility according to specific markers of type 2 inflammation, lowering the blood eosinophil threshold from 250 to 150 cells/µL. 26
Clinical response to biologics is now categorized into 3 levels based on changes in polyp size, quality of life, and olfactory function. 22 Tezepelumab has demonstrated significant reductions in polyp size, nasal congestion, sino-nasal symptoms, and the need for systemic corticosteroids or surgical intervention in adults with severe, uncontrolled CRSwNP. 12 Treatment was associated with reductions in BEOs and other type 2 inflammatory biomarkers, and with improvements in NPSs and CT imaging findings.13,14 Administered subcutaneously, it is being developed by Amgen and AstraZeneca for the treatment of asthma, chronic obstructive pulmonary disease, CRSwNP, chronic spontaneous urticaria, and eosinophilic oesophagitis.
Reported adverse effects include pharyngitis (4.1%), arthralgia (3.8%), back pain (3.8%), and injection-site reactions (3.8%). 27 Moreover, data from WHO-VigiAccess pharmacovigilance analyses indicate distinct safety profiles among CRSwNP-targeted biologics, with tezepelumab showing a notable signal for cardiac adverse events. 19 Nevertheless, given the accumulating evidence, tezepelumab is anticipated to obtain approval for CRSwNP.12,28
The current findings from the included trials do not answer whether tezepelumab is superior to standard management. Therefore, the current evidence should not be interpreted as suggesting that tezepelumab is a first-line treatment option or an alternative to standard therapy. Rather, the trials support tezepelumab as a promising add-on biologic option for patients with refractory or uncontrolled CRSwNP.12,17
Regulatory updates now increasingly support the integration of biologics into CRSwNP management, and emerging molecules such as tezepelumab continue to show encouraging results.12,17 Treatment reassessment is recommended at 6 months, followed by yearly evaluation. Extended dosing intervals, such as every 4 weeks, have also proven effective in patients with well-controlled disease. 29
Compared to endoscopic surgery, which significantly improves symptoms, biologic therapies require long-term repeated administration and associated with high direct costs. Several studies reported that endoscopic surgery is more cost-effective than biologics for CRSwNP, and starting with biologics as first-line treatment without prior sinus surgery adds a direct cost burden.30–32
In summary, CRSwNP is characterized by nasal obstruction, rhinorrhea or postnasal drip, olfactory loss, and at times, facial pain. Its chronic course, frequent infectious exacerbations, and limited response to conventional medical and surgical treatment significantly impair patients’ quality of life, underscoring the need for innovative therapeutic strategies.
Conclusion
This systematic review indicates that tezepelumab is an emerging therapeutic option for patients with severe or uncontrolled CRSwNP who remain symptomatic despite guideline-directed therapy and frequent prior surgery. Across the available trials, it produced consistent reductions in polyp size, nasal obstruction, and overall symptom burden, along with improvements in radiologic findings and quality-of-life measures, independent of baseline eosinophil levels. Treatment was associated with a reduced need for systemic corticosteroids and surgical revision. Evidence remains limited by study heterogeneity, industry sponsorship, short follow-up durations, presence of comorbidities, and the small number of phase III trials. Even with these constraints, tezepelumab appears to be a useful addition to the biologic options for CRSwNP and supports a more individualized, mechanism-based approach to disease management rather than a replacement for current management strategies. Therefore, large-scale, independent, long follow-up trials are required to elucidate the role of tezepelumab in CRSwNP and compare it with standard therapy and endoscopic sinus surgery.
Footnotes
Acknowledgments
The authors thank all investigators and participants of the randomized controlled trials included in this systematic review. No specific funding was received for this work.
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.