
Abstract
Background
The aim of this study was to investigate the relationship between specific sinonasal anatomical parameters and primary acquired nasolacrimal duct obstruction (PANDO) using paranasal sinus computed tomography (PSCT).
Methods
This retrospective case-control study included 42 patients with PANDO and 42 controls. Axial and coronal PSCT images were analyzed to measure the anterior medial lacrimal crest–uncinate process angle (AMLC–UP), nasal bone–lacrimal crest angle (NB–LC), and orbital–maxillary wall distance (OMD). Independent samples t-tests and Mann–Whitney U tests were applied based on data distribution. Variables were entered into stepwise binary logistic regression to identify independent predictors of PANDO.
Results
AMLC–UP angle was significantly higher in the PANDO group compared with controls (mean difference 4.04°, 95% CI: 0.34-7.74, P = .033), while NB–LC angle and OMD did not differ significantly. Multivariate analysis identified both AMLC–UP (OR = 0.916, P = .007) and NB–LC (OR = 1.061, P = .030 (Control:1, PANDO:0)) angles as independent predictors of PANDO. An increasing AMLC–UP angle and a decreasing NB–LC angle were independently associated with higher odds of PANDO. OMD was not retained in the final model. The logistic regression explained 14.6% of variance (Nagelkerke R2) with an overall classification accuracy of 61.9%.
Conclusion
Subtle angular variations between the lacrimal crest, uncinate process, and nasal bone are independently associated with PANDO, suggesting that lateral nasal wall anatomy contributes to nasolacrimal duct patency. These findings may inform preoperative planning for endoscopic dacryocystorhinostomy.
Keywords
Introduction
PANDO is a common cause of epiphora in adults, predominantly affecting middle-aged women.1–3 PANDO is mostly idiopathic, with unclear etiology. Age, female sex, and infections are potential risk factors.3,4 The underlying mechanism of PANDO is thought to involve a chronic, progressive process characterized by obstruction of the nasolacrimal duct (NLD), followed by inflammation and subsequent fibrosis.5,6 Inflammation may originate from ocular or nasal sources.2,3
Anatomically, the nasolacrimal sac is located within the lacrimal fossa, a bony depression formed by the frontal process of the maxilla anteriorly and the lacrimal bone posteriorly, between the anterior and posterior lacrimal crests.7,8 The lacrimal sac is close to the ethmoid air cells and the inferior meatus.5,7 Sinonasal diseases and anatomical variations have therefore been proposed as potential predisposing factors for PANDO. Paranasal sinus computed tomography (PSCT) enables detailed multiplanar visualization of the bony NLD and its surrounding structures, allowing comprehensive assessment of anatomical relationships that may contribute to obstruction. 9 Previous studies have examined associations between PANDO and sinonasal pathologies, nasal septal deviation, and osteomeatal complex disease, with inconsistent results.5,10–12
Among the anatomical structures adjacent to the lacrimal sac, the uncinate process plays a particularly important role. As a thin, curved bony structure of the anterior ethmoid, the uncinate process forms part of the lateral nasal wall and lies in close proximity to the NLD and lacrimal sac. Its attachment pattern and spatial relationship to the lacrimal fossa have important implications not only for the pathogenesis of PANDO but also for surgical planning, particularly in endoscopic dacryocystorhinostomy (DCR).13,14 DCR creates a new drainage pathway by opening the lacrimal sac into the nasal cavity and can be performed endonasally or externally.15–17
Although several studies have focused on intranasal pathologies and sinonasal inflammation in relation to PANDO, quantitative radiological assessments evaluating specific angular and linear relationships between the lacrimal apparatus and adjacent bony structures remain limited. In particular, the spatial relationship between the lacrimal crest, uncinate process, nasal bone, and medial orbital wall has not been sufficiently explored. Therefore, the present study aimed to investigate specific anatomical parameters measured on PSCT (including AMLC–UP angle, NB–LC angle, and OMD) in patients with PANDO compared with a control group. These parameters were selected to characterize the spatial anatomy of the lateral nasal wall surrounding the lacrimal fossa. While AMLC–UP and NB–LC angles evaluate potential angular differences and spatial crowding between the lacrimal apparatus, uncinate process, and nasal bone, OMD was selected as a linear reference baseline to determine whether simple cross-sectional distance limits nasolacrimal patency. By elucidating these anatomical relationships, we sought to contribute to a better understanding of the potential role of lateral nasal wall anatomy in the pathogenesis of PANDO and to provide clinically relevant information for surgical planning in DCR.
Materials and Methods
This retrospective case-control study was approved by the ethics committee and conducted in accordance with the Helsinki Declaration (December 17, 2025, no: 2025/24-13).
Patient Selection
The study included patients diagnosed with PANDO in the ophthalmology department who were subsequently referred to the otolaryngology department for evaluation of nasal pathologies and PSCT. The PANDO group comprised 42 patients (2 men, 40 women; 42 affected eyes), aged 22 to 69 years (mean 41.38 ± 12.71 years). The control group consisted of 42 patients (2 men, 40 women) aged 20 to 57 years (mean 36.50 ± 12.26 years) who underwent PSCT for nasal septal deviation and had no history of NLD obstruction.
The exclusion criteria included a history of paranasal sinus or nasal surgery, the presence of tumors or destructive lesions in the sinuses, and congenital anomalies of the sinuses that might alter the anatomy of the septum or turbinates. Although control subjects underwent PSCT for septal deviation, none had epiphora, dacryocystitis, or radiologic findings involving the nasolacrimal drainage system, making them appropriate anatomical controls.
PSCT Evaluation
The anterior medial lacrimal crest–uncinate process angle (AMLC–UP angle) was defined on axial CT images as the angle formed by the anterior medial lacrimal crest, the lacrimomaxillary suture, and the most anterior insertion of the uncinate process.
The nasal bone–lacrimal crest angle (NB–LC angle) was the angle formed between the medial surface of the nasal bone and the anterior lacrimal crest on axial CT slices.
On the coronal CT slice immediately posterior border to the NLD, the orbital-maxillary wall distance (OMD) was measured. This was defined as the horizontal distance between two vertical lines dropped perpendicular to the nasal floor: one from the attachment of the inferior turbinate to the medial maxillary wall, and the other from the junction of the inferior and medial orbital walls (Figures 1-3). To minimize intersubject variability, all measurements were obtained on the same predefined axial and coronal plane using fixed anatomical landmarks. All PSCT scans were obtained with a uniform slice thickness of 1 mm.
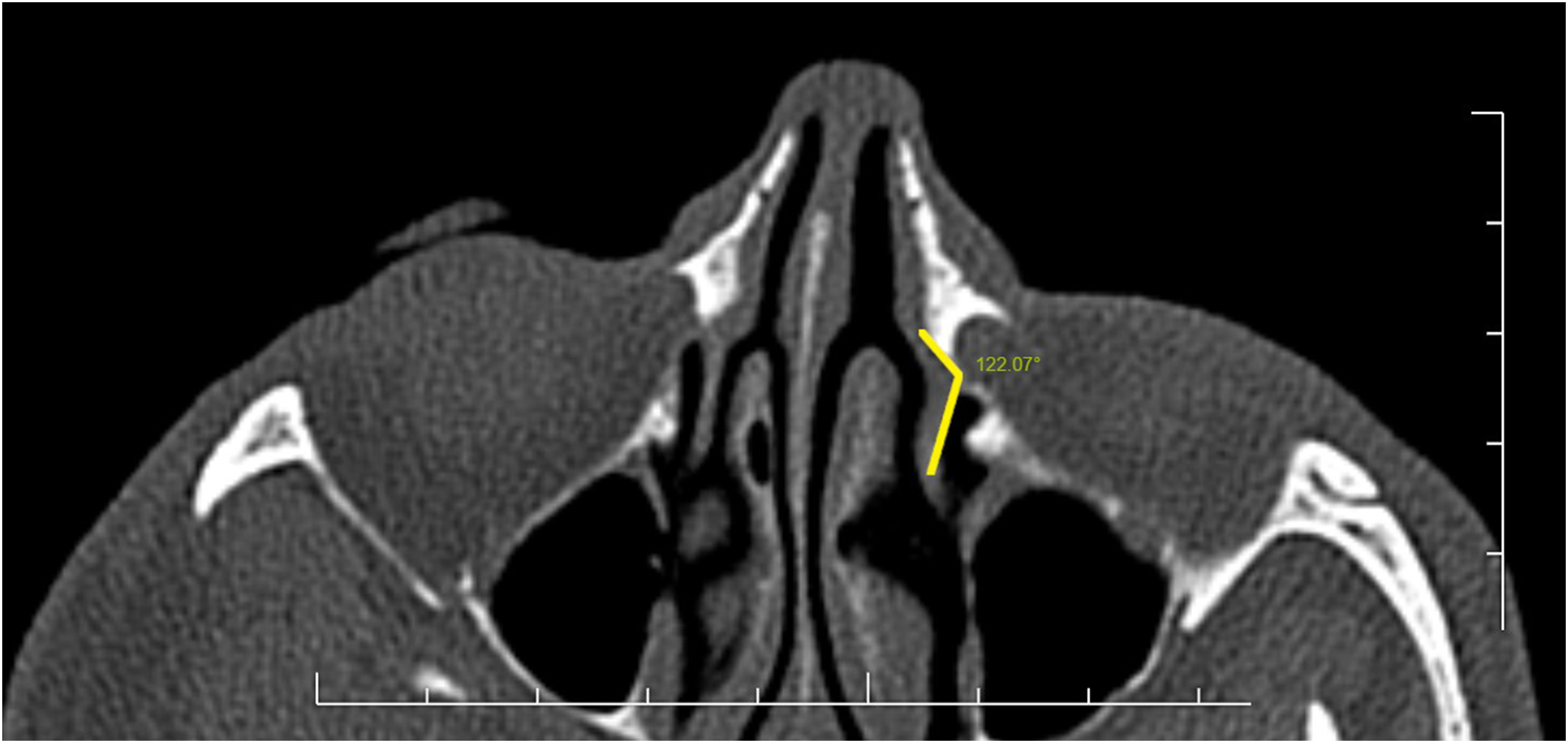
On axial CT images, the angle formed between the anterior medial lacrimal crest, the junction between the maxillary bone and the lacrimal bone and the most anterior insertion of the uncinate process (AMLC–UP angle).
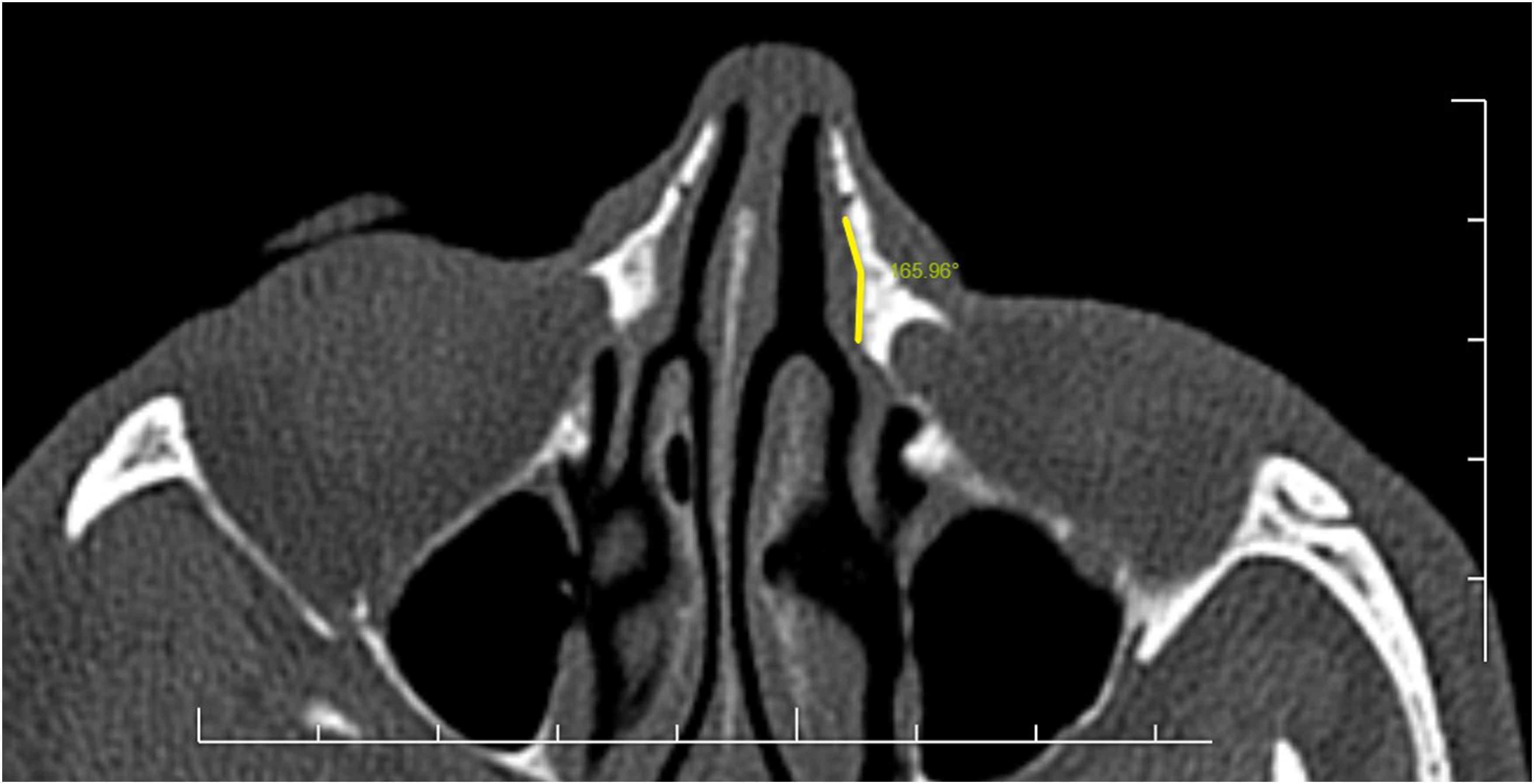
The angle formed between the medial surface of the nasal bone and the anterior medial lacrimal crest (NB–LC angle) were measured.
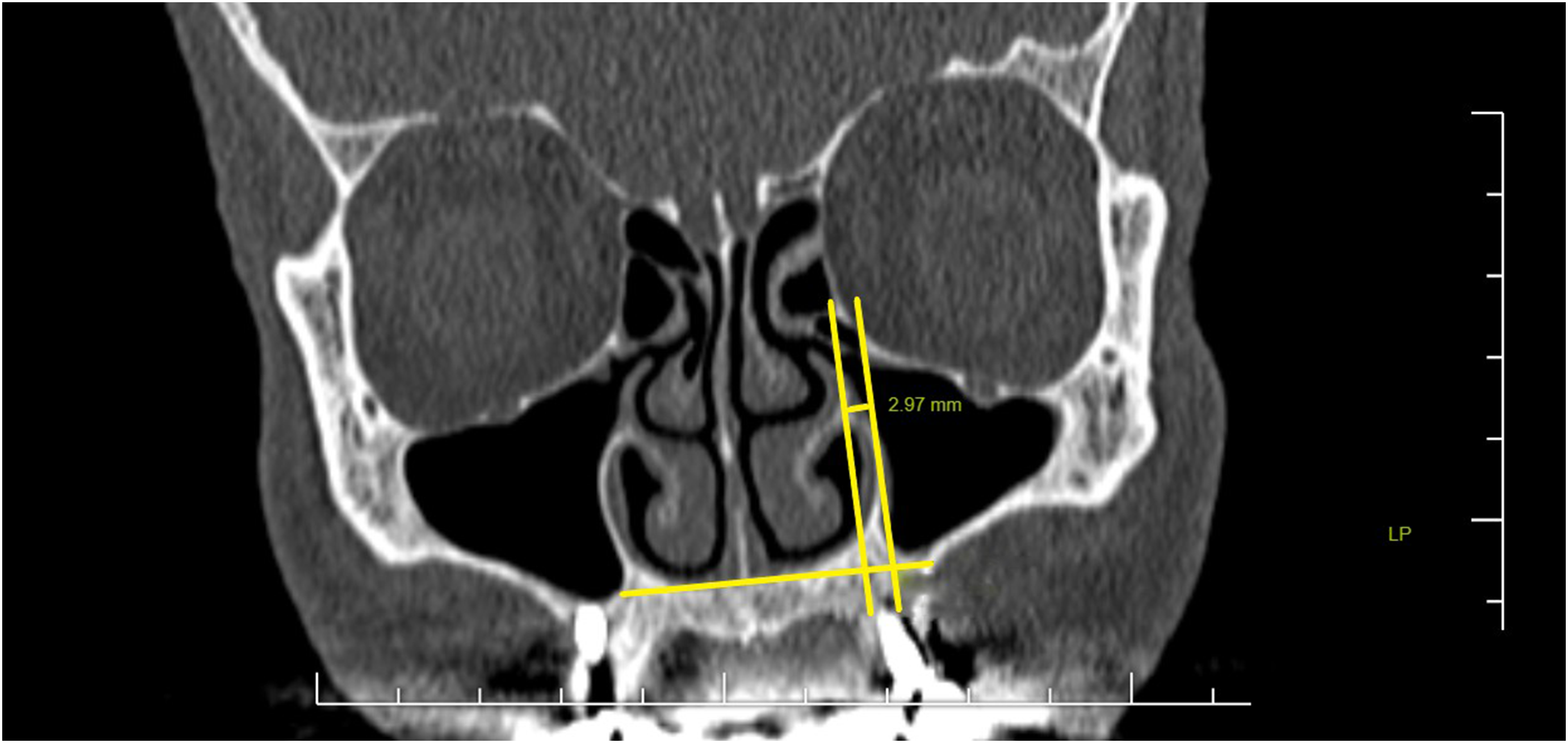
On the coronal CT slice immediately posterior border to the NLD, the orbital-maxillary wall distance (OMD) was measured. This was defined as the horizontal distance between two vertical lines dropped perpendicular to the nasal floor: one from the attachment of the inferior turbinate to the medial maxillary wall, and the other from the junction of the inferior and medial orbital walls.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR), as appropriate. Categorical variables were summarized as frequencies and percentages. Normality was assessed with Shapiro–Wilk, and appropriate parametric or nonparametric tests were applied. Accordingly, between-group comparisons were primarily performed using independent samples t-tests. Homogeneity of variances was evaluated using Levene's test; when the assumption of equal variances was violated, Welch's t-test was applied. To ensure robustness of the findings, nonparametric analyses (Mann–Whitney U test) were additionally performed for variables not meeting strict normality assumptions. The consistency between parametric and nonparametric results was examined to confirm the stability of the conclusions. Variables demonstrating statistical significance at the univariate level (P < .05) or considered clinically relevant were entered into a stepwise binary logistic regression model to determine independent predictors of PANDO. Model fit was assessed using the Omnibus test of model coefficients, Cox and Snell R2, Nagelkerke R2, and overall classification accuracy. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. A two-tailed P-value < .05 was considered statistically significant.
Results
Normality assumptions were assessed prior to group comparisons. Independent samples t-tests were performed to compare OMD, NB–LC angle, and AMLC–UP angle values between the study and control groups. According to the independent samples t-test results for OMD, no statistically significant difference was observed between the groups (t = 0.262, df = 66.41, P = .794). Similarly, for the NB–LC angle, no significant difference was observed between the study and control groups (t = −1.115, df = 82, P = .268). In contrast, the AMLC–UP angle demonstrated a statistically significant difference between the groups. Although Levene's test suggested homogeneous variances (P = .080), the t-test showed significantly higher values in the study group compared with the control group (t = 2.172, df = 82, P = .033). The mean difference was 4.04°, with a 95% confidence interval ranging from 0.34° to 7.74° (Table 1).
Independent Samples t-Test Results Comparing the PANDO and Control Groups.
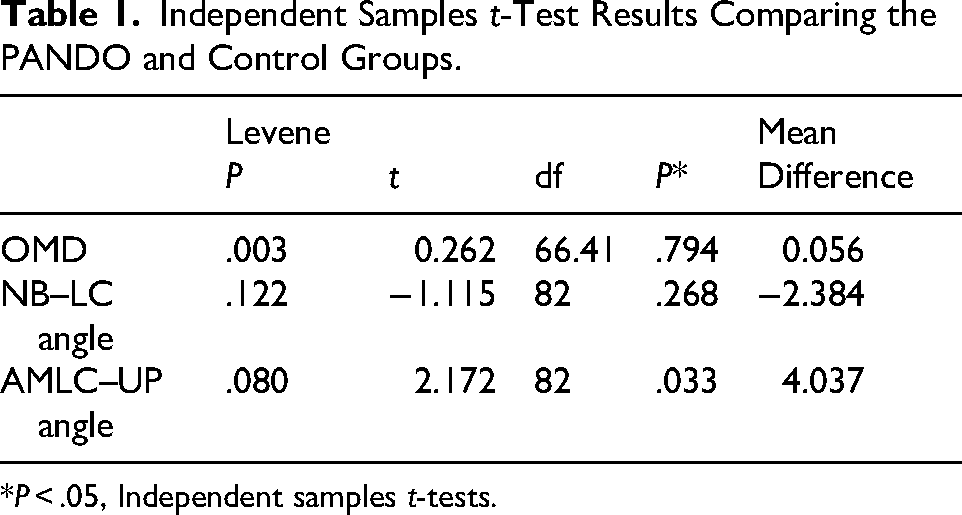
*P < .05, Independent samples t-tests.
Comparisons between the study and control groups were performed using the Mann–Whitney U test. There was no statistically significant difference between the groups in terms of OMD (U = 856.0, Z = −0.233, P = .816) or NB–LC angle (U = 759.0, Z = −1.100, P = .271). Although the AMLC–UP angle was higher in the study group compared with the control group, this difference did not reach statistical significance (U = 671.0, Z = −1.888, P = .059) (Table 2).
Mann–Whitney U Test Results Comparing the PANDO and Control Groups.
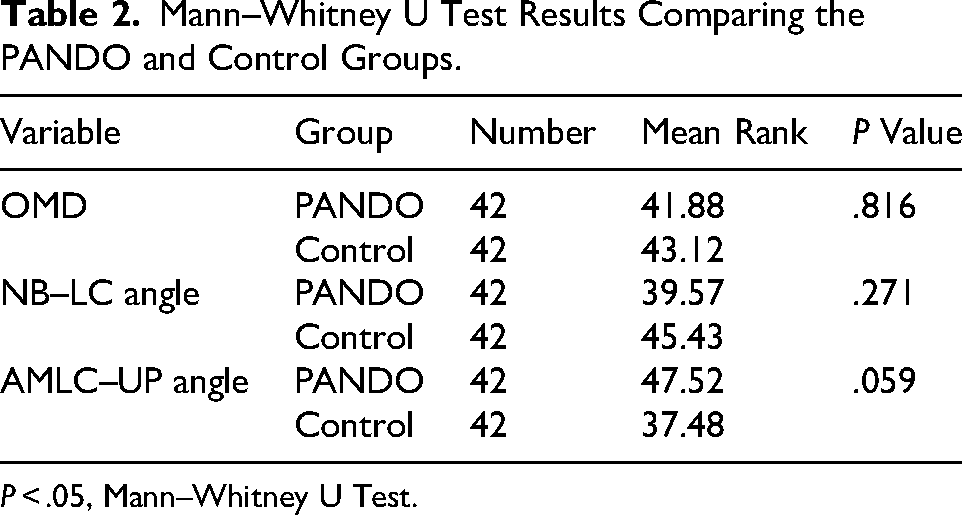
P < .05, Mann–Whitney U Test.
Since OMD and AMLC–UP angle were found to be normally distributed, the results of the t-test were used for these variables. As the NB–LC angle did not meet the normality assumption, the results of the Mann–Whitney U test were used for this variable.
In univariate analysis, only the AMLC–UP angle demonstrated a significant intergroup difference (P = .033), whereas the NB–LC angle (P = .271) and OMD (P = .794) did not. When these variables were entered into the stepwise binary logistic regression model (where control was encoded as 1 and PANDO as 0), a suppressor effect was observed. In multivariate binary logistic regression analysis, the overall model was statistically significant (χ2 = 9.765, P = .008). The model explained 11.0% of the variance according to Cox & Snell R2 and 14.6% according to Nagelkerke R2, with an overall classification accuracy of 61.9%.
Both the NB–LC angle (OR = 1.061, P = .030) and the AMLC–UP angle (OR = 0.916, P = .007) were identified as independent predictors of PANDO. An increasing AMLC–UP angle and a decreasing NB–LC angle were independently associated with higher odds of PANDO. OMD was not retained in the final regression model.
Discussion
PANDO is widely accepted as a chronic, progressive condition characterized by inflammation-induced fibrosis of the NLD, ultimately leading to impaired tear drainage and epiphora.5,6 Although the condition is traditionally considered idiopathic, increasing evidence suggests that local anatomical factors and their relationship with adjacent sinonasal structures may contribute to its pathogenesis.2,3,5 In the present study, we evaluated specific bony anatomical relationships surrounding the NLD using PSCT and compared these parameters between patients with PANDO and a matched control group. In the univariate analysis, only the AMLC–UP angle demonstrated a statistically significant difference between the groups, showing higher angular values in the PANDO group. In contrast, the NB–LC angle and OMD did not show significant baseline differences at the univariate level. However, when evaluated within a multivariate framework to adjust for confounding relationships, a distinct suppressor effect emerged; whereby both the AMLC–UP and NB–LC angles were retained as significant independent predictors of PANDO. Specifically, the multivariate model revealed that an increasing AMLC–UP angle paired with a decreasing NB–LC angle independently associated with higher odds of PANDO. This underscores that these anatomical parameters do not act in isolation; rather, their cumulative and interactive structural configuration along the lateral nasal wall shapes the predisposition to nasolacrimal obstruction.
The close anatomical proximity of the nasolacrimal sac and duct to the lateral nasal wall, inferior turbinate, uncinate process, and maxillary sinus has long been recognized.5,7,8 These relationships are particularly relevant because inflammatory or anatomical alterations in the sinonasal region may facilitate ascending inflammation toward the lacrimal drainage system, thereby contributing to chronic obstruction and fibrosis.2,3 Our findings support this concept by demonstrating a significant alteration in the spatial relationship between the lacrimal crest, nasal bone, and the uncinate process in patients with PANDO.
The uncinate process is a key structure of the anterior ethmoid and plays an important role in shaping the osteomeatal complex.13,14 Variations in its orientation and attachment have been shown to influence sinonasal ventilation and drainage, potentially promoting chronic inflammation. 18 Fayet et al 13 reported that the uncinate process is attached to the lacrimal bone at the level of the lacrimal recess in a substantial proportion of cases, emphasizing its close relationship with the lacrimal sac. In this context, an increased AMLC–UP angle, as observed in our PANDO study, may reflect an anatomical configuration predisposing to chronic regional inflammation.
Previous studies investigating the association between sinonasal pathology and PANDO have yielded conflicting results. Borges et al 10 reported no significant association between PANDO and chronic sinusitis (CRS) or osteomeatal complex disease, whereas Habesoglu et al 11 found a higher prevalence of osteomeatal pathology and maxillary sinusitis on the side affected by NLD obstruction. Similarly, Yu et al 19 demonstrated inflammatory changes in the anterior ethmoid, frontal, and maxillary sinuses on the affected side, suggesting a bidirectional interaction between sinonasal inflammation and the lacrimal drainage system. Our study differs from these investigations in that it focuses primarily on bony anatomical relationships rather than overt inflammatory findings, providing complementary insight into structural contributors to PANDO.
The lack of significant difference in OMD suggests that not all anatomical parameters adjacent to the NLD are equally relevant to disease development. Instead, our results indicate that the relationship between the lacrimal crest, nasal bone and the uncinate process may be of particular importance. This observation aligns with the hypothesis proposed by Gul et al, 5 who suggested that specific angular and spatial relationships between the inferior turbinate, maxillary sinus, and adjacent structures may promote chronic inflammation and fibrosis in the NLD.
DCR is an effective surgical treatment for acquired NLD obstruction; however, several factors have been associated with surgical failure. Previous studies have demonstrated that intranasal pathologies; including nasal septal deviation, concha bullosa, middle turbinate hypertrophy, nasal polyps, and hyperpneumatized agger nasi cells, may predispose to postoperative adhesions, thereby negatively affecting DCR outcomes.20–26 From a surgical perspective, these findings have important implications for DCR, particularly the endonasal approach. Successful endoscopic DCR relies on precise identification of intranasal landmarks and adequate exposure of the lacrimal sac.27,28 The uncinate process has been the subject of ongoing debate regarding its removal during endonasal DCR. Fayet et al 14 advocated planned uncinectomy as a key step to safely expose the lacrimal sac in most anatomical configurations, whereas others have suggested that uncinectomy may not always be necessary.29,30 The uncinate-lacrimal relationship should be carefully evaluated in endonasal DCR planning. Our multivariate findings provide a quantitative perspective on the surgical relevance of uncinate process and lacrimal crest relationships. The combination of a widened AMLC–UP angle and narrowed NB–LC angle may alter lacrimal sac projection and distort the posterior surgical corridor. As recently underscored by Beck et al, 31 the architectural variations of the frontal process of the maxilla dictate the projection and visibility of the lacrimal sac. These findings support the view of Fayet et al 14 that tailored uncinectomy or posterior mobilization may facilitate safer and more complete exposure of the lacrimal fossa during endoscopic DCR, potentially reducing postoperative failure.
The mean difference of 4.04° in the AMLC–UP angle between the groups highlights a subtle but statistically significant structural deviation. From a clinical perspective, such a minor angular discrepancy is admittedly below the threshold of qualitative visual detection by an interpreter during standard radiological reporting. However, its significance becomes apparent when integrated into quantitative preoperative surgical planning and digital mapping software for endoscopic DCR. In the highly confined space of the lateral nasal wall, a few degrees of regional rotation or osseous remodeling can profoundly alter the mechanical vectors of the lacrimal pump mechanism and increase localized mucosal tension. This subtle distortion promotes microbending at the junction of the lacrimal sac and the bony NLD, triggering a cascade of chronic microinflammation and progressive subepithelial fibrosis rather than gross mechanical blockage. Therefore, these subtle angular variations should be viewed as subvisual morphometric markers of a multifactorial disease process rather than signs for routine qualitative diagnosis.
From an anatomical perspective, the combined widening of the AMLC–UP angle and narrowing of the NB–LC angle may reflect three-dimensional remodeling of the lacrimal fossa boundaries. Rather than causing direct mechanical compression, this altered configuration may disturb lacrimal drainage biomechanics and promote chronic localized inflammation, ultimately contributing to fibrosis and PANDO development.
In univariate analyses, only the AMLC–UP angle differed significantly between groups in the independent samples t-test, whereas this difference showed borderline significance in the Mann–Whitney U test. This discrepancy likely reflects the moderate sample size and the sensitivity of distribution-dependent statistical testing. Given the balanced group sizes, parametric analyses were considered statistically robust; moreover, the consistency of directionality across both tests suggests that the observed difference is not spurious but of moderate magnitude. Notably, NB–LC angle did not show a significant intergroup difference in univariate testing but emerged as an independent predictor in multivariate logistic regression. This apparent inconsistency is methodologically plausible. Univariate analyses assess crude mean differences without accounting for interrelationships among anatomical variables. In contrast, logistic regression evaluates the independent contribution of each parameter while adjusting for others. The significance of NB–LC angle in the multivariate model therefore suggests that its effect may be subtle and context-dependent, becoming evident only when analyzed within a combined anatomical framework.
Although the logistic regression model was statistically significant, its explanatory capacity was limited (Nagelkerke R2 = 0.146), indicating that anatomical variation likely represents only one component of a multifactorial disease process. Mucosal inflammation, hormonal influences, environmental exposure, age-related remodeling, and other yet unidentified factors may interact with structural predisposition in the development of PANDO.
This study has certain limitations. The sample size was relatively modest, which reduces the statistical power to detect smaller effect sizes and limits immediate generalizability. Larger prospective cohorts are necessary to validate these angular parameters as screening markers. Second, our cohort featured a high female predominance (95.2%), likely driven by referral patterns and strict exclusion criteria that eliminated secondary or post-traumatic obstructions. Third, subclinical or low-grade CRS was not controlled for in our multivariate model. Extensive CRS can trigger ascending mucosal inflammation, representing a confounding pathway. Additionally, due to the retrospective design, objective endoscopic staging of localized mucosal inflammation along the NLD was unavailable. Future large-scale, prospective multicenter trials combining high-resolution CT morphometry with standardized endoscopic mucosal staging are warranted to fully clarify the interplay between osseous anatomy and soft-tissue inflammation in PANDO.
Conclusion
AMLC–UP and NB–LC angles may influence PANDO risk. Subtle lateral nasal wall variations can affect NLD patency; larger prospective studies are needed. These findings may inform preoperative planning for endoscopic DSR.
Footnotes
Abbreviations
Ethics
The study was approved by the Ethics Committee of Bursa City Hospital on December 17, 2025, No: 2025/24-13.
Informed Consent
This is a retrospective study, there is no need to take informed consent.
Author Contributions
Oğuzhan Dikici: literature survey, design, planning, data collection, intellectual review of the results, writing, and approving the final manuscript. İsmail Alkan: data collection, intellectual review of the results, and approving the final manuscript. Osman Durgut: data collection, intellectual review of the results, and approving the final manuscript. Fevzi Solmaz: data collection, intellectual review of the results, and approving the final manuscript. Malik Afifoğlu: data collection, intellectual review of the results, and approving the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.