
Abstract
We analyzed 30 pandemic films and developed a processual model to explain the social-level coping mechanisms to confront pandemics as portrayed in films. The model describes the underlying collective understanding of disease outbreaks. The model suggests that pandemic films divide the disease outbreak into three phases: emergence, transmission, and termination. Concurrently, three social processes tend to be activated to cope with the pandemic: healthcare, political, and public awareness. This model is used to compare the social imaginary reflected in films with the current COVID-19 outbreak. The resemblance of the model and the current outbreak suggests that fictional pandemic films may still follow our collective understanding of the pandemic dynamics. Four scenarios are suggested as road maps for futures and foresight practice concerned with future pandemic outbreaks.
Introduction
Since its inception in December 2019, the COVID-19 (Novel Coronavirus Disease 2019) outbreak quickly became a global pandemic. By February 9, 2022, according to the World Health Organization, confirmed cases had reached 397 million and the death toll was 5.75 million worldwide. Almost no country on earth has been spared from this outbreak. Although this particular disease is novel and we are just encountering its first outbreak, different infectious diseases have stricken human societies many times in history. From about seven thousand years ago, the emergence of complex human civilization has enabled people on earth to live in large and densely populated communities, which have provided ideal places for microbes that cause infectious diseases to flourish (Mager 2009). Indeed, due to their huge impact, pandemics are a significant theme across cultures and times, recorded in different forms of literature and art. Among them, films are a relatively new but very impactful art form. Pandemic films vividly show the outbreak of infectious disease, its impact on individuals and human society, as well as the fight to control it. These films have heightened public awareness of the risk of pandemics, demystified their causes by expelling superstitious beliefs; and served as roadmaps to understand and cope with them. Indeed, the outbreak of COVID-19 has unsurprisingly led to a surge of interest in pandemic films (Lindahl 2020).
However, there is a seemingly significant gap between the public interest in pandemic films and the scholarly attention to them. Conventionally, artworks such as films are seldom the subject of research for behavioral and social science scholars, with exceptions in history, literature, and communication studies (Han and Curtis 2020a, 2020b; Pappas et al. 2003; Pernick 2002; Tomes 2000, 2002). Fictional films are considered unrealistic and bear little significance to reveal true courses of events or guide best practices. Nevertheless, films reflect and shape the social imaginary of important issues in society. Films provide us with vivid representations of people’s understanding and course of actions facing certain critical situations. The COVID-19 outbreak provides us with a rare opportunity to examine whether pandemic films represent people’s interpretation of and course of action that they may take during outbreaks.
We consider how pandemic films reflect collective social imaginaries of human society under the crisis of a disease outbreak. In the current study, we identified and content analyzed 30 pandemic films. We used a qualitative grounded theory approach to generate a processual model 1 representing and explaining the way societies may respond to pandemic crises. We further compare how countries and societies have been responding to COVID-19 with what is portrayed in films. Our analyses reveal that fictional films on pandemics have great resemblances with what has happened, while some key differences deserve a systematic examination. These similarities and differences suggest that films are a fruitful repository to guide the foresight practice on future pandemic outbreaks. Indeed, similarities speak of the plausibility of the scenarios portrayed in the films, and differences speak of the discontinuities featured in such scenarios. These are two crucial elements for futures and foresight practice. Therefore, we conclude by discussing how themes portrayed in multiple films can serve as guidelines for scenarios of future pandemic outbreaks. The article is organized as follows. In the first section, we review the theoretical background that has informed our analysis. In the second and third sections, we report our research questions and the research method we used. In the fourth section, we report our findings. Our findings include (a) a brief descriptive account of the portrayal of pandemics in films, (b) the processual model explaining the coping mechanisms of human societies to confront pandemics portrayed in films, and (c) the similarities and differences between such model and what has happened in reality as a consequence of COVID-19 until the time this article is written. We further presented a 2x2 matrix of pandemic movies to inform futures and foresight practice.
Theoretical Background: Collective Social Imaginaries and Films
A social imaginary is a manifestation of beliefs and norms that guide people in a society to think and act (Gaonkar 2002), which can originate from religions, private enterprises, politicians, experts, media, and the art world (Beckert 2016; Gaonkar 2002). Due to its global reach and to the influence of the film industry today, cinema is an impactful art form that can reflect and shape collective social imaginary. Firstly, films are collectively construed and produced, differently from other art forms such as painting. They represent what the audience expects to see in them. Thus, films reflect the cultural norms and worldviews of the current era (Birdsell and Groarke 1996). Secondly, although fictional, films represent as-if reality, with concrete and immersive audiovisual cues on what might happen (Fergnani and Song 2020a). As such, films can shape up expectations and orient the current actions of the audience.
Futures scholars have paid attention to films, particularly sci-fi films, for their implications for Futures studies (Lombardo and Ramos 2015; Rumpala 2012). Fergnani and Song (2020b) studied the social imaginaries of the future through 140 films set in the future. They identified six major images portrayed in films, Growth & Decay, Threats & New Hopes, Wasteworlds, The Powers that Be, Disarray, and Inversion, which represent six macroscopic scenarios of destiny of humankind, that is, scenario archetypes. In Growth & Decay, collapse and decay of social order and living conditions are accompanied by the excessive power of monopolistic corporations. In the Powers that Be, after a catastrophic event, a totalitarian or dictatorial regime gains tight control over its citizens. In Wasteworlds, a global-scale catastrophe brings the world back to a premedieval or tribal state. In Threats & New Hopes, an apocalypse threatens the very existence of humanity. Humankind is saved through heroic and collective efforts. In Disarray, human society degenerates into a chaotic situation due to problems such as crime, social unrest, poverty, war, famines, or pandemics. In Inversion, a new agent such as an alien species replaces human beings to dominate the earth. Most pandemic films belong to the disaster-thriller genre. They resemble the image of Threats & New Hopes 2 . This corroborates that pandemic films are representative of common social imaginaries.
As collective imaginaries, pandemic films reflect people’s fear of infectious disease outbreaks, and envision where and how they may occur, including their dire consequences, the complexity to identify causes, and difficulties to find treatments. Such depiction may be based on the social context at the time and place when and where the films are made. According to the medical historian Nancy Tomes (2000), there have been two periods of germ “panic” in American popular culture. The first one occurred between 1900 and 1940, and the other has started in 1985, lasting until the current era. The public awareness and concerns on disease outbreaks are shaped by news and entertainment, including films; and by collaborations among social groups including scientific researchers, politicians, activists, journalists, and advertisers for different social, political, as well as economic interests (Tomes 2002).
In the first germ panic, between 1900 and 1940, infectious diseases which had troubled human societies for millennia, such as Plague, Smallpox, Yellow fever, and Tuberculosis, still occasionally led to outbreaks. However, pioneering works done by scientists such as Louis Pasteur and Robert Koch in the late 19th Century had made the medical community and the public aware of the microorganic cause of these diseases, the importance of hygiene, and the effectiveness of medical treatments and vaccines. Additionally, the development of mass media, particularly the birth and quick advancement of the art of motion picture, made public health campaigns more effective in reaching families and individuals.
In the second germ panic, AIDS, Ebola, and drug-resistant strains of older bacterial diseases have been generating viral panic. New knowledge (or fantasies) of genetics, the human immune system, and human-nature interaction have been shaping popular perceptions of fearsome emerging disease agents with no effective “magic bullets” against them. During this period, major changes in communication technologies including cable television, satellite technologies, and the internet have made 24-hour, on-the-spot coverage of and access to information possible, creating the so-called “tabloid sensationalism” (Tomes 2000, p. 194). The current germ panic is similar to the earlier one, in terms of high immigration rates, fears of economic interdependence, and apprehensions about the global movement of people and disease (Tomes 2000, 2002). However, a salient difference of the current germ panic in comparison to the former one is that the legitimacy of states’ power has been on its downswing. The US government has been on a prolonged retreat from an active role in building up public health infrastructures (Tomes 2000).
In between these two periods, World War II and the Cold War occurred. In the 1940s, people’s attention was caught by the war among humans, rather than by the war between humans and infectious diseases. After that, the rivalry between two superpowers, the United States and the Soviet Union, dominated international politics. Furthermore, antibiotics and vaccines became widely available in the 1960s and 1970s and lessened the threat of infectious diseases (Tomes 2000). However, during this period, the threat of an outbreak from a manmade biological agent becomes a more salient concern for the public. Although countries such as the UK and France started to study biological warfare in the 1920s, it was the Japanese military who first developed and used biological weapons during World War II in Northern China, whereas many as 200,000 civilians were killed. After the war, US officials guaranteed Japanese scientists of such biological weapons immunity from war-crimes prosecution in exchange for their information on their experiments and wartime attack maneuvers (Guillemin 2006). The atrocities of Japanese germ warfare were only exposed much later, such as in the Hong Kong film Men Behind the Sun. Both the USA and the former Soviet Union secretly developed their biological weapons during the Cold War period. In the 1960s and 1970s, the civil rights movement, protests against the Vietnam war, the assassinations of John Kennedy and Martin Luther King Jr., the oil price shock and following inflation, as well as the Watergate scandal added to the enduring shock and controversy in American society (Lev 2000), as well as to a deep distrust toward the government, particularly among youths. During and after the Vietnam War, the scientific community and the public were more aware of biological weapon programs (Guillemin 2006). The above historical contexts may explain the theme of deceitful leaders/governments secretly developing bioweapon programs portrayed in several films, primarily in the United States beginning with the 1965 film Satan Bug (Dehority 2020).
Whereas the above account summarizes how social and historical contexts shape pandemic films’ themes. Conversely, films, as collective social imaginaries, also influence human actions. Behavioral studies have shown that films can influence audiences’ transient mood and social judgments (Forgas and Moylan 1987). Furthermore, watching violent films can promote aggression (Black and Bevan 1992) while watching films vividly portraying personal responsibility can enhance this trait (Smithikrai, Longthong, and Peijsel 2015). Finally, Denvir (2004) analyzed George W. Bush’s claims of war against terrorism after al Qaeda attacked the World Trade Center and drew parallels between his military decisions and the “savage war myth” demonstrated in films portraying lawlessness, including The Man Who Shot Liberty Valance, The Godfather Parts I and II, and Dirty Harry. He demonstrated that certain locutions of the language used by the Bush administration, such as “Wanted Dead or Alive,” were indeed taken from films; thus, providing evidence of the possible influence of such films on political decisions. Pandemic films may also influence people’s perceptions of infection diseases and their further actions. For example, the former health secretary of U.K. Matt Hancock claimed that he had watched the film Contagion and the film had influenced his decision to insist to order more vaccine doses and set out early the order of priority for the jabs in the U.K. (BBC News, 3rd February 2021). However, films may also have negative influences and mislead the public. Dr. Stephen Morse, an epidemiologist from Columbia University who had consulted for the film Outbreak, claimed that some unscientific plots in it had attributed to the public confusion about the Ebola disease (Kendal 2021). All in all, films seem to play a role in, at least in part, shaping society and at the same be shaped by it.
Research Questions
We have formulated the following research questions abductively during the data collection and analysis to uncover the relationship between the construal of pandemic outbreaks in cinema and the actual response of current societies with COVID-19: RQ1: How are the emergence of and response to pandemic outbreaks constructed in films? RQ2: What are the major similarities and differences between the construal of pandemic outbreaks in films and the actual response of major countries with COVID-19?
In our findings section, after a summary of the content portrayed in the films analyzed, we present a processual model to explain the coping mechanisms to confront pandemic outbreaks as portrayed in the films, thereby answering the first research question. We then discuss the similarities and differences between this model and the current responses to COVID-19, thereby answering the second research question.
Methods
Sample
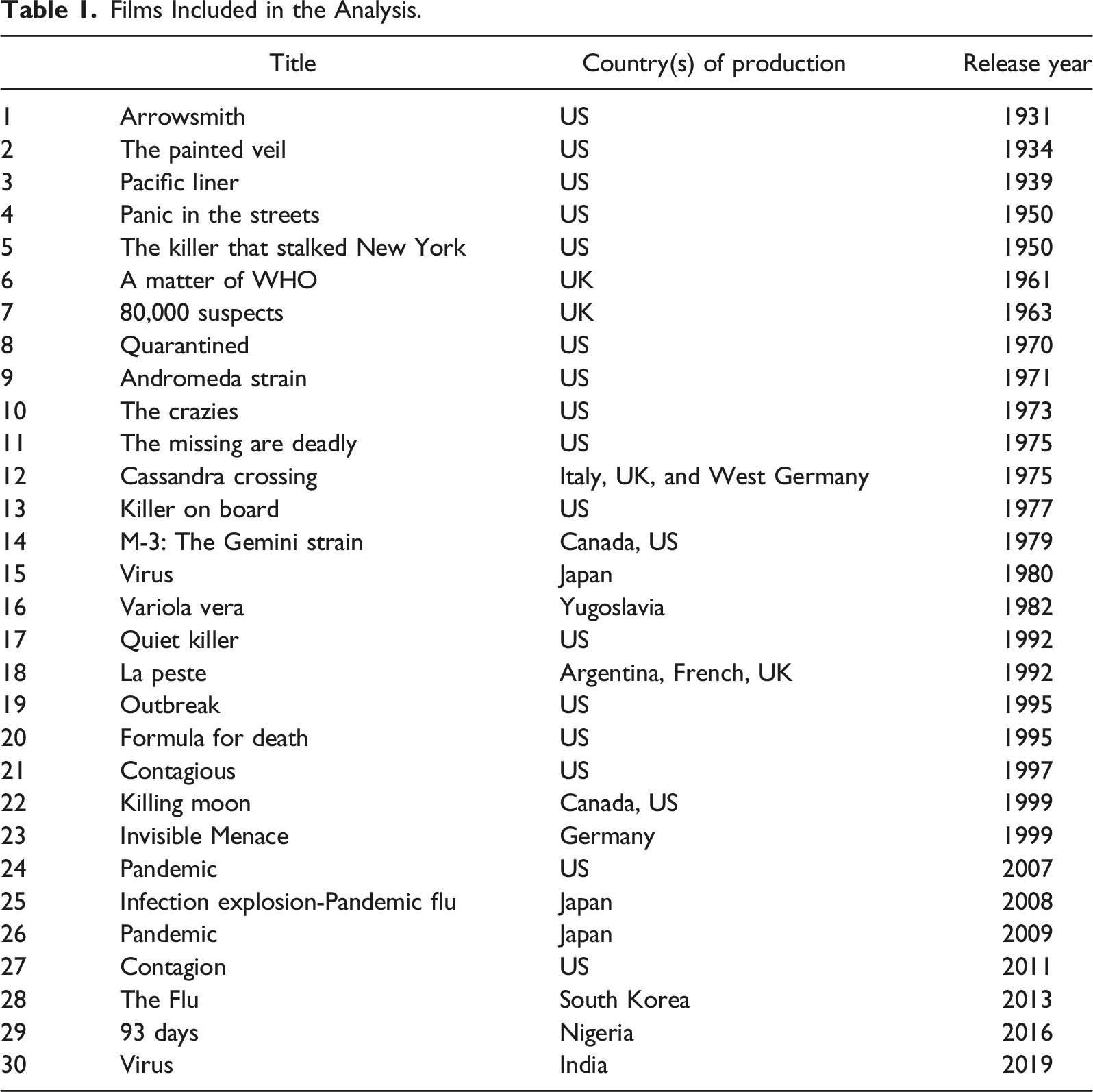
Films Included in the Analysis.
Coding and Analyses
We followed grounded theory guidelines (Charmaz 2014; Strauss and Corbin 1998) and adapted the procedures of Fergnani and Song (2020a) with three steps of data coding and analysis: films transcriptions, coding, and emergent theory construction. This approach fits well with our goal of extracting theory from films, which is a novel methodological development in grounded theory (Fergnani and Song 2020a, 2020b).
Specifically, we first watched those films and converted relevant information from them into transcripts. We recorded information relevant to nine abductively generated dimensions: disease, the outbreak, the protagonists, the medical organizations, professional organizations, political institutions involved, public reactions, containment measures, and treatments. In the second step, we assigned conceptual labels to events, situations, organizations, and individuals in each film. We considered each film as a subject and coded film-by-film. This was an iterative process of comparison between codes to ensure the distinction between them, going back and forth between data collection and analysis, consolidating, recurring or overlapping codes to a fewer number of overarching codes. The last step involved the identification of higher-order categories as well as the relation among categories until a clear and parsimonious explanatory pattern emerged. We also referred to published professional articles and guidelines for pandemic management to come up with categories and explanations (e.g., World Health Organization 2018).
A Note on Epistemology
It is worth noting that our research embraces an objective, critical realist epistemological stance, maintaining that reality is existent independent of the observer while our interpretations of it may be fallible (Bhaskar 1975). This differs from a social constructionist stance, the more often embraced epistemology in inductive qualitative research, which maintains that reality is socially constructed. Consequently, we regard our interpretations of the portrayal of pandemics in films as provisional and only instrumental to further triangulation by future research to discover the full properties of the phenomenon under investigation. This being said, inductive grounded theory is still a suitable research methodology for this objective analysis in absence of alternative sources of data on films. Indeed, grounded theory is not only amenable to different epistemological stances and often used for objective research purposes (Charmaz 2014), but critical realism can also conciliate the social constructivist claim that reality is fully shaped by our constructions of it by asserting that such social constructivist claim commits the epistemic fallacy of conflating ontology (reality) with epistemology (our interpretations of it via, e.g., research). From a critical realist perspective, these two claims have to be considered at different levels of analysis (Healey and Hodginkson 2014).
Findings
Portraying Outbreaks in Films
There are variabilities in the 30 films in terms of pathogens, locations, and scale of outbreaks that they demonstrated. Eighteen films are on real diseases. Of these, four films show a plague from bacterium Yesinia pestis (Arrowsmith, Panic in the Streets, Quiet Killer, and La Peste), four are on Smallpox from variola virus (The Killer that Stalked New York, A Matter of WHO, 80,000 Suspects, and Variola Vera), four are on Cholera from Vibrio cholera bacterium (The Painted Veil, Pacific Liner, Quarantined, and Contagious), two are on Ebola from Ebola virus (Formula for Death and 93 Days), two are on H5N1 Influenza virus (Infection Explosion-Pandemic Flu and The Flu), one on N1H1 Influenza virus or the Spanish flu (Invisible Menace), and one on Nipah outbreak (Virus 2019 4 ). The frequency of these diseases shown in films reflects some extent the prevalence and their impact on human history. Twelve films are on fictional diseases or pathogens, including Trixie virus (The Crazies), Mombasa fever virus (The Missing are Deadly), M-3 fertilizing bacterium (M-3: The Gemini Strain), MM88 virus (Virus 1980), Motaba virus (Outbreak), MEV-1 virus (Contagion), Menzies C5 (Killing Moon), Influenza H3N7 or Riptide virus (Pandemic 2007), and the alien microorganism Andromeda (the Andromeda Strain). For influenza H3N7, there does exist such a name but with no report of an outbreak; thus, the described disease is still considered fictional. These twelve also include three films on unnamed fictional pathogens (Cassandra Crossing, Killer on Board, and Pandemic 2009). While the majority of outbreaks in these films originate naturally, eight films portray manmade outbreaks or pathogens, for example, leaked from a laboratory or related to military bioweapon programs (the Andromeda Strain, The Crazies, The missing are Deadly, M-3: The Gemini Strain, Virus 1980, Formula for Death, Invisible Menace, and Killing Moon). Films with such a theme only started to be shown on screens after World War II. One film describes an outbreak with natural origin but is examined by a secret bioweapon program (Outbreak). At different periods, there are different trends in pandemic films. All films before 1971 are on pathogens of old and well-known diseases, such as Plague, Smallpox, and Cholera. Films made in the 1970s are mainly on lab or manmade pathogens, and films made after the 1990s are mainly on emerging infectious diseases, such as Ebola, Nipah, Influenza, or fictitious new diseases. These cinematic trends reflect the social and historical contexts as described in the theoretical background section.
In terms of locations and scale, six of these films show outbreaks in very confined spaces (e.g., on a train in Cassandra Crossing, on the airplane in Killing Moon, on a cruise ship in Pacific Liner and Killer on Board, and in a clinic/hospital in Quarantined and Variola Vera). Twenty are on outbreaks restricted in a town, a city, several cities, or several islands (e.g., Panic in the Streets in New Orleans, 93 days in Lagos, Nigeria). One is at the national level in Japan (Infection Explosion-Pandemic Flu). Three films are on global pandemics (Virus 1980, Pandemic 2009, and Contagion).
Processual Model: Coping with Pandemics
Despite such differences, we found that pandemic films share some common underlying elements of pandemics’ development and control. Across the films, the outbreak can be differentiated into three epidemic phases: emergence, transmission, and termination. These phases, together, make up the processual model to explain the social-level coping mechanisms to confront pandemics as portrayed in films, and thus describe the underlying collective understanding of disease outbreaks. During the emergence phase, the pathogen is transmitted to humans from its original carrier or transmitted from outside into a local community through a human host. The first infected human is the index patient, sometimes called patient O. In the second phase, transmission, the disease is spread in communities through human-to-human contacts. In the last phase, termination, the disease is expelled from the community through immunity and cure.
In the processual model, over the three phases as above, we present three concurrent social processes that tend to be activated in pandemic situations: healthcare, political, and public awareness. Coming up with a disease treatment requires healthcare and it is a highly specialized activity and profession in modern societies. Only trained medical doctors and professional healthcare organizations are permitted to engage in such activities by following standard protocols. In all films examined, medical doctors, either civilian or military, are at the forefront to fight the outbreak. Their roles are as described in explaining the three phases of pandemic control. Disease control requires the allocation of public resources and powers. It is no wonder that in all pandemic films, in one way or another, different political entities are involved in all phases of pandemic control. The outbreak of a contagious disease is a disastrous event that can have a profound impact on each individual and society as a whole. The public needs to be properly informed to avoid the spread of rumors and panic. Furthermore, to prevent the spread of a contagious disease, citizens’ compliance with the healthcare system’s guidelines is necessary. Therefore, public awareness of the cause of a disease, the risk to contract a disease as well as available treatments is vital in controlling the pandemic.
Pandemic by its nature is firstly a healthcare problem. Thus, the healthcare system needs to be activated to respond to the outbreak. The emergence phase is paired with the response interventions that are early detection and anticipation of the outbreak (World Health Organization 2018). Healthcare professionals engage in retrospective identification efforts to identify the index patient, the pathogen, the carrier, and the infection mechanisms. It is crucial to identify the index patient of an outbreak for two reasons. First, the index patient is the beginning of a chain reaction of human-to-human transmissions. Painstaking efforts are shown in films to identify those who have been in close contact with the index patient to prevent the further spread of the disease. Second, through the index patient, it is possible to identify the carrier of the pathogen (e.g., from the index patient James “Jimbo” Scott to the monkey carrier, Betsy, in Outbreak), which may lead to a possible cure of the disease. It is important to identify the pathogen, the cause of the infectious disease, as well as the infection mechanisms to control the transmission, cure the disease, and develop a vaccine. Identifying the carrier is also important. Animals are often carriers of infectious diseases. Rats in a ship are carriers of the Plague in Panic in the Streets. Bats are carriers in both Contagion and Virus 2019. A monkey from Africa is the carrier in Outbreak. Sea birds are carriers in Contagious. In Andromeda Strain, a meteorite in outer space is the carrier.
Additionally, besides the above retrospective efforts, anticipatory preparations are also necessary. In Outbreak, labs with different biosafety levels in USAMRIID are vividly portrayed at the beginning of the film. Virologist Lieutenant Colonel Sam Daniels (Dustin Hoffman) alerts his superior as well as the CDC of a possible outbreak of the Motaba virus in the USA after he investigates an outbreak in Zaire. Both dismiss his fears. When the virus outbreak indeed occurs, his early investigations on the Motaba virus appear to be of help. Early pandemic films, such as Panic in the Street, The Killer that Stalked New York, and 80,000 Suspects, demonstrate that facilities, personnel, and procedures are in place when outbreaks occur. Such anticipatory preparations are crucial for the successful containment of diseases.
In the second phase, transmission, the pathogen is passed to people through direct human contact, contaminated food, water, or fomites. Without proper control, the disease can be transmitted at an exponential speed. Associated with this transmission phase, containment strategies need to be implemented. Contact tracing, quarantine, and hospitalization are major strategies to contain the transmission of the disease in almost all films. Social distancing and hand washing are sometimes mentioned (e.g., Contagion). For professionals who handle patients or related materials, it is standard procedure to wear protective masks, gloves, gowns, and goggles. Arrowsmith, Panic in the Streets, and Cassandra Crossing are exceptions because lead doctors in the films have minimal self-protection gears when treating patients or those at high risk of infection. The importance of protection measures in treating infectious diseases is very well demonstrated in the films 93 days and Virus 2019. In 93 days, the index patient is treated in a normal clinic that is not specialized in infectious diseases. Most doctors and nurses in direct contact with the patient are infected by Ebola. In Virus 2019, the index patient is brought into a public hospital for emergency treatment. There is no isolation and protection during his treatment; therefore, a lot of nurses, patients, and bystanders are infected by the Nipah virus.
The last phase, termination, involves using an effective medication, developing and distributing a vaccine to the public, or reaching immunity; thus, the outbreak is terminated. In Panic in the streets, the pathogen is a bacterium. Those in close contact with the patients or fomites are inoculated with serum and streptomycin. In Contagious, Cholera can be treated by hydration and a vaccine is also made available. In the Killer that Stalked New York and 80,000 Suspects, smallpox outbreaks are terminated by mass vaccination. It is worth mentioning that the Smallpox vaccine was the earliest successful vaccine introduced in 1796, and Smallpox is the only human disease eradicated by vaccination thus far. Such deadly diseases of the past are not deadly anymore in modern times thanks to proper treatments. In several films, antibodies in serum are found to be the vaccine or cure of fictional viruses. In Outbreak, an antiserum created by mixing a monkey’s antibodies with experimental serum from a secret military program becomes the cure. In Contagion, the MEV-1 vaccine is developed from experiments with monkeys. In Pandemic 2007, tubercular antibodies in serum happen to be the vaccine for the Riptide virus. In M-3: Gemini Strain, the antitoxin for acetylcholine developed by the CDC and an M4 virus developed by Dr. Bill Fuller are the cures. In Pandemic 2009, the antiserum from recovered patients is the cure. In the Flu, an antibody from the serum of the immune person is the cure.
Compared to bacteria-caused infections, it is harder to develop the cure and vaccine for diseases due to viruses. In two films based on true stories, 93 days and Virus 2019, there is no proper treatment or vaccine. Rigorous containment efforts to identify and quarantine all infected individuals in the community are essential. Without effective medication, patients are either left to die or to recover by their immune response. The disease is eliminated and no one in the community is sick anymore.
In Andromeda Strain, it is the PH level outside of the human body that makes the pathogen harmless. In Cassandra Crossing, it is the high concentration of oxygen that cures those who are sick. In Virus 1980, the first vaccine development fails. Later, a doctor successfully develops the vaccine through nuclear radiation. Such scenarios are fictional and not scientifically supported.
Besides, healthcare activation, different governmental or international agencies are involved in the disease control process. During the emergence phase, government agencies such as the U.S. Center for Diseases Control (CDC) and U.S. Public Health Service (PHS) are tasked to fulfill such preventive missions. A strong information network and authority to obtain needed information are critical. In most American films, the CDC or PHS is engaged in early detection. In films made in other countries, national or local public health agencies are engaged in the pandemic response. In two Japanese films (Infection Explosion-Pandemic Flu and Pandemic 2009), the cabinet secretariat set up a special coordination committee to oversee the national outbreak response from the very beginning of the pandemic. In Virus 1980, the U.S. president is involved in the failed effort to control the global pandemic. It is worth mentioning that, in two Canada–US co-produced films (M-3: The Gemini Strain and Killing Moon) and two Japanese films (Infection Explosion-Pandemic Flu and Pandemic 2009), U.S. CDC is also involved, reflecting the political and professional influence of the U.S. on its allied nations. In The Matter of WHO and Contagion, since the pandemic is transnational or global, the World Health Organization (WHO) is involved in the identification process. In Variola Vera, Pandemic 2007, and 93 days, the WHO is also involved in the control of the pandemic in each country. The above organizations lead the effort to identify the index patient, trace the carrier, and uncover the pathogen. Law enforcement agencies are often asked to help trace the index patient and those who have been in close contact with her/him (e.g., police in Panic in the Streets and Contagious, FBI in Pandemic 2007).
Furthermore, consistent with conspiracy theories, the introduction and emergence of the disease can be directly or indirectly related to government agencies. For example, in Andromeda Strain, the military satellite to catch extraterritorial organisms for bioweapon development brings a strain of deadly pathogens to earth and kills almost all people in a town. In Cassandra Crossing, the US military keeps a strain of pneumonic plague in its mission to International Health Organization in Geneva, possibly relevant to a secret bioweapon program. In Outbreak, the military is aware of the virus since the 1960s and has developed the antibodies for possible biological warfare. Government agencies also tend to be concerned about the outbreak as a biological attack. In Contagion, the CIA and HNS consider the possibility of a terrorist attack. In Virus 2019, the Indian central government official worries about a possible weaponized attack and threatens to have the Ministry of Defense take over the investigation if local medical professionals are not able to uncover the origin of the disease in time.
In films portraying manmade pathogens, in the emergence phase, goals and activities may be different from those of naturally occurring diseases. When pathogens are leaked, the primary intention of those who own them is the coverup. For example, In Andromeda Strain, the pathogen and survivors are brought to a highly protected military lab to be studied. In the Crazies, soldiers wearing protection gears occupy the infected town like a war zone.
During the disease transmission phase, placing under quarantine those who are already sick and monitoring those who have been in close contact with patients are critical actions to contain the pandemic. Besides healthcare professionals such as public health workers, doctors, and nurses, other agencies with enforcement power tend to be mobilized. When the disease is very dangerous and the pandemic is hard to contain, military forces tend to be used to enforce quarantine, curfew, or lockdown. In Cassandra Crossing, armed soldiers with full-body protection get onboard the train of the outbreak and enforce the order. In Outbreak, a military troop is deployed to round up the town Bonneville, Oregon, when the virus spreads widely within, but not outside. In the Flu, the South Korean Army quarantines those who are sick and blocks the whole city of Budang by force. In Pandemic 2007, the California National Guard is ordered by the governor to lock down the whole city of LA. In Contagion, federal troops are deployed to closedown Chicago. When the pandemic becomes more serious and the death toll reaches 2.5 million in the U.S.A., riots in major cities are reported, and the implantation of mandatory curfews in major metropolitan areas ensues.
Other types of political struggles are also demonstrated in the films. In Panic in the Streets, the Mayor of New Orleans is persuaded to help control the disease, while the police head is not convinced of the necessity. In A Matter of WHO, the UK minister of foreign affairs phones the health minister to prevent the autopsy of a foreign minister who is suspected to die from Smallpox. In Pandemic 2007, the mayor of Los Angeles and the governor of California engage in a power struggle on who to give orders and take responsibilities. In Contagion, there is a lack of coordination at the federal level and fifty states act differently in responding to the crisis. In 93 Days, red tape in the city and state governments prevent swift allocation of resources to fight the pandemic. In Cassandra Crossing, it is indicated that most Western governments do not want the train with infected patients to stop in their territory to provide a place to quarantine all passengers. In summary, during the disease transmission phase, political struggle tends to be heightened in implementing containment measures.
In the termination phase, political involvement is less salient than the first two phases. The most significant political involvement is portrayed in Contagion, in which the lottery to allocate vaccines by birth date is supervised by a general in the CDC, and the vaccination centers are heavily guarded by federal troops. In Outbreak, the vicious General McClintock, who insists to bomb the town with an outbreak, is arrested. In Cassandra Crossing, the two officials who have orchestrated the military and medical measures for the infected train are under surveillance, suggesting a higher-level coverup. In Pandemic 2007, the political conflict between the city mayor and the state governor is resolved. In 93 Days and Virus 2019, a ceremony after the victory to end the outbreak is held to pay tribute to those who sacrificed their lives and show unity among all parties involved. To summarize, at the termination phase, there is some sort of actual or symbolic activity to indicate the closure of the political activation.
Media coverage is the most important means to activate public awareness. All films except for three involving military coverup missions (the Crazies, Andromeda Strain, and Cassandra Crossing), four where the outbreak is in a confined space (Pacific Liner, Quarantined, Killer on Board, and Killing Moon), or in a backward island in Southern China in the 1930s in The Painted Veil, have media coverage of the outbreak. In Contagion, Virus 2019, and 93 Days, healthcare agencies are proactive to publicly brief the situation on TV. In Panic in the Streets and Contagious, health care professionals in the early phase of the outbreak avoid reporters when they do not have concrete information of the cause and index patients to prevent spreading inaccurate information to the public and stirring unnecessary panic. In Panic in the Streets, the reporter is detained by the police for one night to prevent him to release the pandemic news in the morning newspaper. In the Flu, the media coverage of the pandemic is only sporadic and the disease spreads very fast, which may partially explain chaotic reactions from the public. In Contagion, conspiracy theorist Alan Krumwiede uses his blog to spread alternative explanations such as a Minamata disease outbreak coverup by the fishing industry or a biological weapon attack, as well as a false medication from forsythia. Such disinformation is equally contagious as it creates public chaos.
Another important aspect of the activation of the public is the people’s emotional reactions to the outbreaks. People tend to have panic and paranoia reactions particularly during the early stages of pandemics, which have been vividly demonstrated in films. In Pandemic 2009, many fearful people with symptoms rush into the hospital and make it overwhelmed. The chicken farm owner is wrongly accused by others to cause the pandemic and committing suicide. In Invisible Menace, the window of the house of the researcher who is suspected to cause the pandemic is broken by a brick throw from the street. In Contagion, many engage in panic buying in a supermarket. Such irrational reactions are common in real pandemics including the current COVID-19. During the transmission phase of the pandemic, we can see people comply with quarantine, curfew, or lockdown measures. However, there are occasions when people develop distrust over those measures and choose to disobey (e.g., the private security contractor Gibby Smolak breaks the curfew in Pandemic 2007) or turn into a riot (e.g., The Flu). At the final phase of the pandemic, we can see people seeking treatment or vaccine (e.g., Contagion and Pandemic 2007), and show appreciation of those who helped terminate the outbreak. People’s lives return to normal.
We provide a visual summary of the processual model in coping with pandemics in Figure 1. Processual model in coping with the pandemic.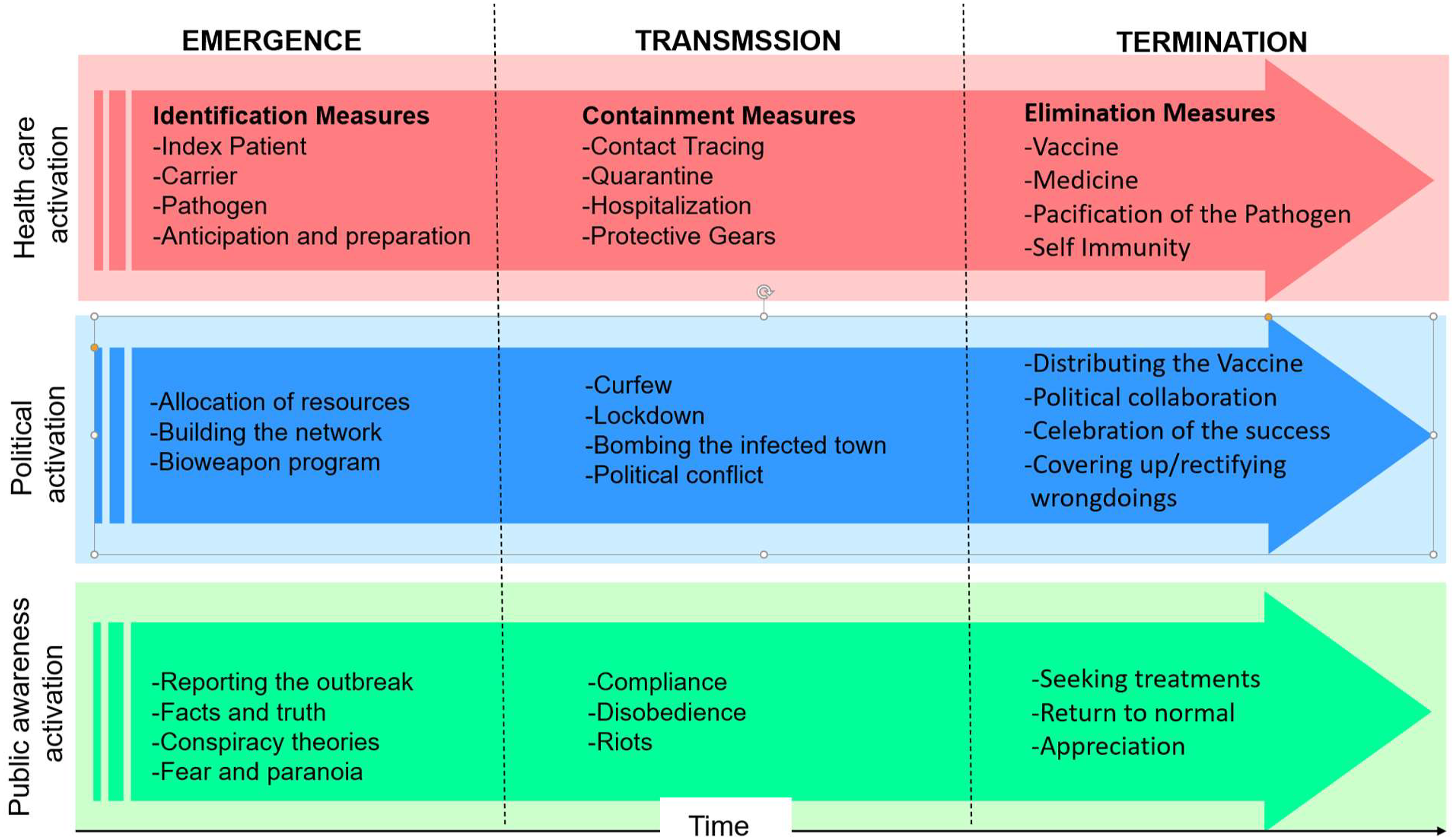
Similarities and Differences between Films and the COVID-19 Outbreak
We have summarized pandemic films and revealed their underlying model in describing mechanisms in coping with pandemics. Then, the next question is to what extent these fictional films share a resemblance with the current COVID-19 outbreak.
There is consensus on certain issues related to the COVID-19 outbreak: the pathogen is a coronavirus which is a respiratory virus spreading primarily through coughs, sneezes, droplets of saliva, or discharge from the nose of an infected person. The virus can also spread when an infected person speaks, sings, or breathes. The original animal host of the virus is likely the bat. However, the host animal has not been confirmed and the index patient has not been identified. Considering the more recent experience of SARS and MERS pandemics, we probably will never be able to trace the index patient for this pandemic. The disease started in Wuhan, China. It has become a global pandemic. The impact of this pandemic on the world is unparalleled in modern times after the 1918 Spanish flu pandemic. Most nations were not well prepared when the outbreak started to strike. Overwhelmed with patients in critical conditions, healthcare systems almost collapsed in some countries. How similar are these situations to those described in pandemic films?
Among 30 films reviewed, Contagion is probably the film sharing most similarities with the current outbreak. Contagion tells a story of the fictitious MEV-1 virus, which is more based on the Nipah virus that infects cells in the respiratory and nervous systems. The disease spreads through respiratory droplets and fomites. People become contagious even before the symptom onset or during the incubation period. All of these are very similar to what happened in the current COVID-19 outbreak. Both outbreaks in the film and reality started in China. The COVID-19 outbreak has caught most nations off guard, similar to what was described in the film. The global scale of the COVID-19 is also similar to the film. Furthermore, the vaccine is the best chance to control the outbreak in both the film and reality.
However, there are some notable differences between the film and the current outbreak. In Contagion, the mortality rate of the disease is very high (20–30%). The incubation period of the disease is short, less than a couple of days. In the real world, high mortality and short incubation diseases are difficult to spread quickly and globally without being noticed and blocked through preventive measures. On the contrary, the combination of relatively low mortality rate (around 2% globally), long incubation period (up to 14 days), and a high rate of asymptotic makes COVID-19 harder to detect and stop. In the film, CDC experts develop the vaccine within several weeks. Unfortunately, this is not possible in reality. Typically, years are needed to develop an effective vaccine. For COVID-19, more than 100 vaccine candidates are under development. The acceleration of the development process led to the approval of the first vaccine in December of 2020. According to the WHO, at least 13 different vaccines have been administrated. In the film, curfews and martial laws are implemented, but people are still free to move within cities, while in reality, we see more lockdowns of cities with stay-at-home orders.
As for other films, although few depict an outbreak like the current scale, there are some scenes bearing similarities with realities. For example, large scale infections among doctors and nurses in contact with patients in hospitals (e.g., 93 Days and Virus 2019), infections due to medical procedural errors (e.g., Outbreak), the transmission of disease among family members and friends (e.g., Panic in the Streets, Cassandra Crossing, and Virus 2019), and political battles among politicians (e.g., Pandemic 2007).
These similarities and differences are interesting. However, a more insightful exploration is to use the processual model that we developed from pandemic films to analyze the current COVID-19 outbreak. After the emergence of the current outbreak, medical communities in China and the world rushed to engage in the identification process: tracing the early patients, summarizing the common symptoms, analyzing the genome of the pathogen, identifying possible hosts, and exploring possible pathophysiological mechanisms. These remarkably fast identification efforts have greatly enhanced our scientific understanding of the disease and guided further treatment and prevention strategies. It is worth noting that several countries or regions that were hit hard by the SARS outbreak in 2011, such as Hong Kong, Taiwan, and Singapore, were more alert and quickly adopted preventive measures, such as travel restriction and widespread testing, at the very beginning of the COVID-19 outbreak. Their anticipatory preparations might have contributed to their better performance in controlling the outbreak within their borders.
However, on the political and public awareness levels, we have witnessed the spread of all sorts of explanations including conspiracy theories and political conflicts between nations (e.g., finger-pointing between the U.S. and China). For example, whilst the causes of the outbreak have been attributed to nature, most probably wild animals such as bats, which is widely accepted in the scientific community, Astrobiologist Chandra Wickramasinghe and his associates suggest it was a meteorite to carry the pathogen from the outer space to earth (Steele et al. 2020). China’s Foreign Ministry has claimed that although the epidemic was first reported in China, it does not necessarily mean that the virus has originated there. Indeed, there have been some scientific reports indicating or suggesting that the virus has appeared in Europe as early as March of 2019 (Chavarria-Miró et al. 2020; Deslandes et al. 2020; La Rosa et al. 2020). There are also occasional claims that the virus is from a lab-leak accident or a secrete bioweapon program in either China or the US (Nie 2020). The identification of the source of the outbreak and even the naming of the virus (e.g., China Virus vs. Coronavirus) have become very political matters with heightened debates and quarrels in media outlets.
In most countries, the outbreak is still at the transmission phase or early termination phase. Several containment measures have been implemented, such as lockdowns (started from Wuhan lockdown on 23rd of January 2020), curfews, travel restrictions, quarantine and hospitalization, social distancing, and hand cleaning. Healthcare workers wear full-body protection gear and people wear face masks. However, it is widely debated whether wearing face masks is necessary for the public, and different countries have drastically different policies. One striking fact in the current pandemic is that many healthcare workers who are attending infected patients have very limited protection due to insufficient storage and supplies of protection equipment, particularly in the first several months of the pandemic. Therefore, thousands of healthcare workers have been infected in China, Italy, U.S., among other countries. We have witnessed what happen in poor countries in 93 Days and Virus, but the same has happened in developed countries as well.
Political parties in each country have engaged in fights on suitable responses but compromised to pass urgent bills. In the United States, former President Donald Trump exchanged accusations with New York Mayor Bill de Blasio and the former New York State Governor Andrew Cuomo on who should be responsible for the lack of medical supplies in New York. The poor handling of the COVID-19 outbreak in the US is considered one of the major reasons for Donald Trump to lose the presidential election in 2020 to Joe Biden. The COVID-19 dominates TV channels and other media outlets which try to provide the most updated information to fit everyone’s needs. Medical organizations have been rushing to develop and test possible medicines and vaccines to cure or prevent the disease. Medical trials’ findings have become headlines in major TV channels and newspapers. Political leaders such as Donald Trump announced the effectiveness of hydroxychloroquine and recommended its usage in treating patients, contradicting professional recommendations (Samuels and Kelly 2020). Such interference from political forces over medical practices is unprecedented. In most pandemic movies, vaccines and medications developed by medical professionals tend to be trusted and accepted by the public. On the contrary, for the COVID-19 outbreak, we have witnessed a huge disparity within the public in responding to vaccination drives, although they have been strongly endorsed by the medical and scientific communities, government agencies, and the WHO. Such vaccine hesitancy in societies is rarely depicted in pandemic films. Partly as a consequence of such social conflicts, misinformation, and distrust that are related to the COVID-19, we are yet to claim the victory over the pandemic, different from the straightforward success in controlling the pandemic after vaccines or medicines are developed, which is often depicted in pandemic films. This situation is unfortunate when the disease containment and control require the strong collaboration of all nations and all citizens.
The above analyses and comparisons show past pandemic films do include plots that resemble the current COVID-19 pandemic. However, given the limited running time of films and their entertaining nature, no film can represent the real pandemic with all involved aspects and details. Next, using the futures and foresight method to analyze 30 pandemic films, we derive a simple 2x2 matrix with different scenarios that can guide future disease prevention and control.
Implications for Futures and Foresight Practice
Common themes across films can be viewed as a possible representation of what might happen when outbreaks strike. They can inform scenario generation on which possible different dimensions are important to consider in scenarios of future pandemic outbreaks. For this purpose, we try to categorize pandemic films in a 2x2 matrix, with one dimension of natural versus manmade origin, and the other dimension of known versus novel disease. These are the two most important distinguishing dimensions among films that we analyzed.
Pandemics of natural known diseases are portrayed in twelve films: Arrowsmith, The Painted Veil, Pacific Liner, Panic in the Streets, The Killer that Stalked New York, A Matter of WHO, 80,000 Suspects, Quarantined, Variola Vera, Quiet Killer, La peste, and Contagious. Those common infectious diseases such as Plague, Smallpox, and Cholera have caused a huge fatality in history and are still considered dangerous in modern times. Those older films before the 1970s are all in this category and this theme reappeared in cinema occasionally in later decades. In the early decades of the last century when effective treatments were not well established or available, those older films show the panic, fatality, and the limitation of the medical professionals when facing such diseases. Pandemics of natural novel diseases are shown in eight films, including Killer on Board, Outbreak, Pandemic, Infection Explosion-Pandemic Flu, Contagion, the Flu, 93 Days, and Virus 2019. This category includes real emerging infectious diseases such as Ebola and Nipah, as well as fictitious diseases such as Motaba and N5H1 influenza. Films in this category show painstaking efforts by medical professionals to identify the causes of diseases, their transmission mechanisms, and treatments.
Manmade outbreak from common infectious disease is rarely featured in films. Only Invisible Menace from Germany belongs to this category. In this film, the virus that caused the Spanish flu is leaked from a laboratory, leading to an endemic in Cologne. Eight films feature manmade novel diseases, including Andromeda Strain, The Crazies, The Missing are Deadly, Cassandra Crossing, M-3: The Gemini Strain, Virus 1980, Formula for Death, and Killing Moon. Among them, The Missing are Deadly, M-3: The Gemini Strain, and Formula for Death involve leaking of deadly viruses from the civilian labs, while the other five films in this category tend to be linked with military labs or operations. Those films featuring leaking of pathogens from secrete bioweapon programs tend to also show violent coverup operations.
Futures and foresight practice concerned with future outbreaks may take into account these four different configurations while referring to our processual model of coping with the pandemic, to build different while informative scenarios and allow more comprehensive response plans. The disease-prevention systems in the world now are more built around the first scenario to prevent natural pandemics from known diseases for which there tend to be mature containment procedures and treatments. However, current systems are much less effective in facing novel diseases or manmade outbreaks. The first case of COVID-19 emerged in Wuhan, China no later than December 1st of 2019. However, China’s CDC was only aware of the outbreak almost 1 month later partially because China’s infectious monitoring system at that time made reporting emerging diseases outside of the list of standard infectious diseases very difficult (New York Times, March 30, 2020). Furthermore, on a global scale, there is a shortage of mechanisms for nations to collaborate to prevent novel natural or manmade outbreaks from spreading. Except for relying on nations or other entities, the WHO does not have an independent capacity to monitor, analyze, and develop treatments for novel diseases. For manmade biological pathogens, although there is a Biological Weapons Convention underneath the United Nations prohibiting the development, production, stockpiling, acquisition, or retention of microbial or other biological agents or toxins as weapons, there are no robust mechanisms to verify the compliance of the state parties. All the above facts suggest the lack of preparedness at both the country and global levels to deal with novel and manmade outbreaks. A lot can be done by using scenario planning and foresight methodologies to help increase the preparedness for future novel and manmade diseases.
We also want to highlight that these analyses and recommendations are not just about the prevention of specific events because that overemphasizes our capacity to control the future (Miller 2018). They are also meant to help us to be comfortable to navigate uncertainty and wild cards such as pandemics as they happen and to put in place organizational capabilities in the present that would allow us to do so in the future (Fergnani 2021a, 2021b; Mendoca et al. 2004).
Conclusion
The current article relies on 30 pandemic films to derive a model on pandemic development and control. This model reveals that pandemics portrayed in films have three epidemic phases: emergence, transmission, and termination. Furthermore, the model suggests the activation of three social processes: the activation of efforts to curb the spread of the disease, of healthcare systems, political systems, and public awareness. Through the comparison between the current COVID-19 pandemic and the model, we can see a substantial resemblance between fiction and reality. Although there are still a lot of differences between the specifications of the outbreaks in films the actual outbreak, the model derived from films can serve us as a conceptual framework to understand this unfolding and interweaving process involving multiple stakeholders and parties. We categorize pandemic films into four scenarios in a 2x2 matrix where the two axes are natural versus manmade origin and known versus novel disease. This categorization helps guide the futures and foresight practice on future pandemic outbreaks, and hopefully, stimulates scholars to develop other insightful scenarios. Pandemics are not only natural events but also social events. Cinema is an effective art form to reflect our understanding of the complexity of pandemics’ unfolding process, as well as their impact and social coping efforts. Although films are fictional, they alarm us of looming crises, provide us inspirations on how future pandemics may unfold, and offer hopes to curb disasters. After the COVID-19, many pandemic films will likely be produced, hopefully, based on better scientific evidence and a deeper understanding of the underlying psych-social dynamics.
The current study has limitations and it also suggests some future research directions. First, the coverage of pandemics is limited in existing films. The crash of financial markets, the closedown of many businesses, the surge of unemployment, travel bans, flight suspensions, food shortages (Baldwin and Mauro 2020), changed international conflict patterns (Bloem and Salemi 2021), regulations, and legal controversies on the pandemic control (Sokołowski 2020), as well as both positive and negative environmental impacts of the pandemics (Rume and Islam 2020), which we have witnessed in the current COVID-19 pandemic, are not well depicted in existing films. In comparison to the often-used frameworks in foresight such as the PESTEL analysis (Yüksel 2012), healthcare activation, political activation, and the public awareness activation in our procedural model correspond to technological, political, and social factors in the PESTEL, respectively. The economic, legal, and environmental factors in the PESTEL have been rarely touched in pandemic films. We believe those important macro facets should be covered by future pandemic films to facilitate the creation of more comprehensive collective social imaginaries on pandemics.
Second, although existing pandemic movies vividly depict people’s emotional reactions, such as fear and panic, toward infectious diseases; as well as the social unrests against containment strategies such as curfew and quarantine; there is a lack of coverage in films on irrational reactions toward the outbreak: denials of the risk to be infected and the severity of the disease, distrust against scientific recommendations (e.g., mask-wearing and vaccine), and heightened hatred toward foreigners and immigrates. Such irrational human reactions, compounded with political drives and turmoil, can create strong social inertias hampering the pandemic control. Such deep-rooted irrationality within individuals and societies, which is revealed during the current COVID-19 pandemic, deserves future pandemic films to portray, analyze, and critique.
Third, the dominance of Hollywood in the global film industry has resulted in a disproportional number of films produced in U.S. Films as a cultural product reflect values, norms, customs, histories, as well as political and economic situations of the location where they are produced. We can see from Table 1, since 1975, there have been more films made from other countries. However, there is still a severe lack of representation of films from developing countries where most human population now live in. Better coverage of different countries, societies, and cultures can enlarge our repertoire of collective social imaginaries on pandemics.
The complexity and uncertainty of the current COVID-19 outbreak demand scholars to find novel ways to analyze it. The current article utilizes an unorthodox approach, using fictional films to help understand the current COVID-19. Doubtlessly, the current COVID-19 will not be the last major global outbreak. Engaged scholarship on the intertwined relationship between pandemic films and popular disease beliefs is greatly needed (Tomes 2002; Pappas et al. 2003). We hope that it can add a piece of knowledge to better fight the outbreak collectively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.