
Abstract
Objective
The objective of the study was to evaluate the mechanical properties of living human knee cartilage using our ultrasonic device, and to compare the measurements with respect to cartilage degeneration and aging.
Design
A total of 95 knees which had undergone arthroscopic knee surgery, from 88 patients, were included in the study, with informed consent. All procedures were reviewed and approved by the ethical committee of our hospital. In the study group, there were 41 men, 47 women, 39 right knees, and 56 left knees. The conditions primarily included knee osteoarthritis and anterior cruciate ligament rupture. The mean operative age was 44.1 years old (range = 10-83). We compared mechanical properties of the knee cartilage with respect to aging and gender, in comparison with normal cartilage. A P value of <0.05 represented statistical significance.
Results
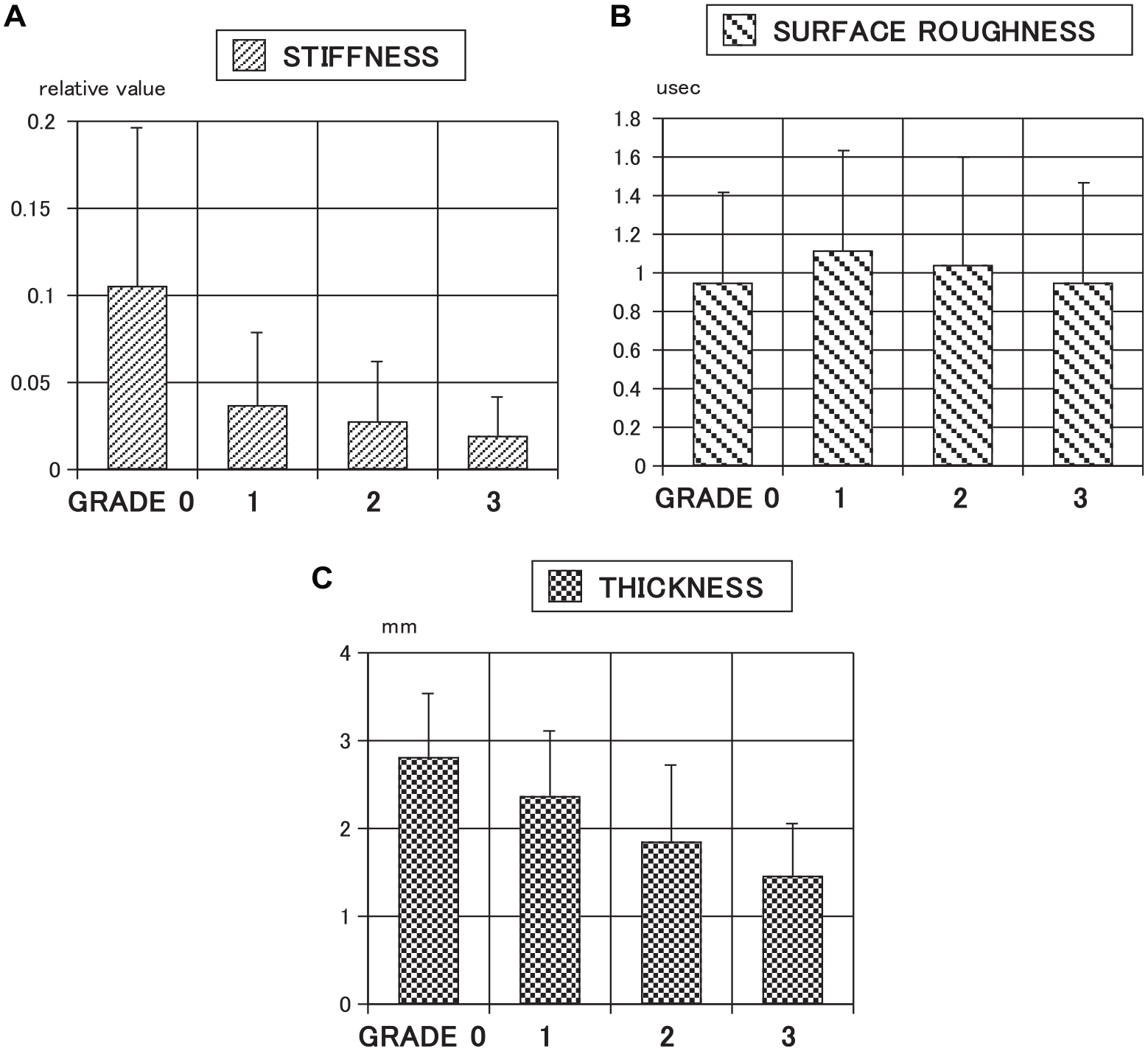
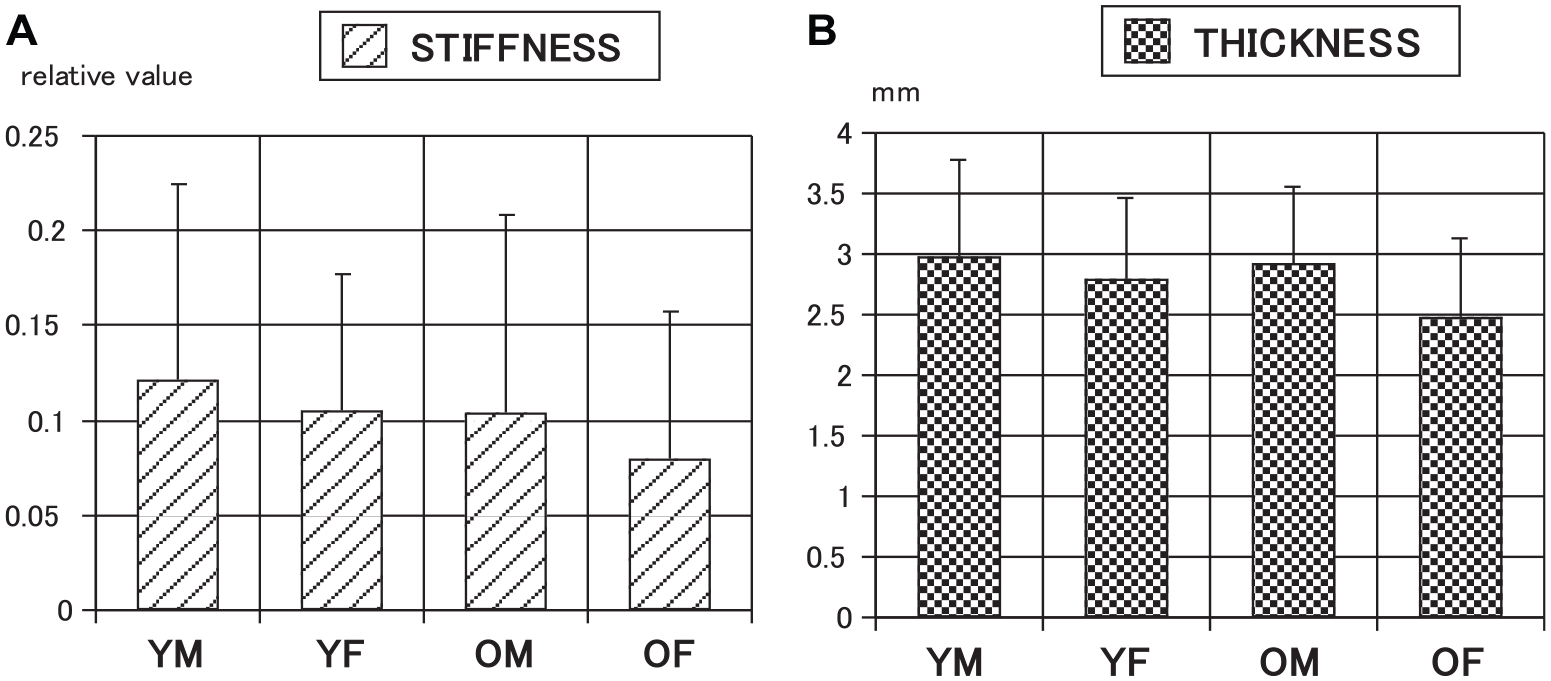
In the context of the International Cartilage Repair Society (ICRS) classification of cartilage degeneration (grade 0-3), the signal intensity in grade 0 was significantly larger than that in grade 1, 2, or 3. The thickness in grade 0 was significantly higher than that in grade 1, 2, or 3. Normal cartilage in older women had the lowest signal intensity and the least cartilage thickness among all the groups.
Conclusion
The ultrasonic system we developed was able to detect early degenerative changes in living cartilage in knees. The lowest signal intensity and least cartilage thickness in normal cartilage among older women were correlated to a large prevalence of knee osteoarthritis in women.
Level of Evidence:
Level IV, case series
Introduction
Articular cartilage is a special type of connective tissue consisting of solid and fluid phases. Its main function is to provide a low-friction surface with a reasonable degree of lubrication to the underlying subchondral bone.1,2 Hip or knee osteoarthritis, also referred to as degenerative joint disease, is a slow destructive process of joints that affects millions of people worldwide. Although the exact biochemical cause of osteoarthritis remains unknown, the process usually begins with abnormal joint structures or with unusually high stress placed on joint surfaces.3,4 The incidence of osteoarthritis is influenced by many factors, such as work, sports participation, musculoskeletal injuries, obesity, and gender. With the aging and increasing obesity of the world’s population, health professions need to prepare for a large increase in the demand for health services to treat hip and knee osteoarthritis. 5 A measurement system capable of detecting cartilage degeneration and aging would be very useful in diagnosing and managing cartilage disorders. Hybrid PET-CT and PET-MRI allow integration of high-resolution structural information on CT and MRI with metabolic information obtained from PET related to osteoarthritis disease process. 6
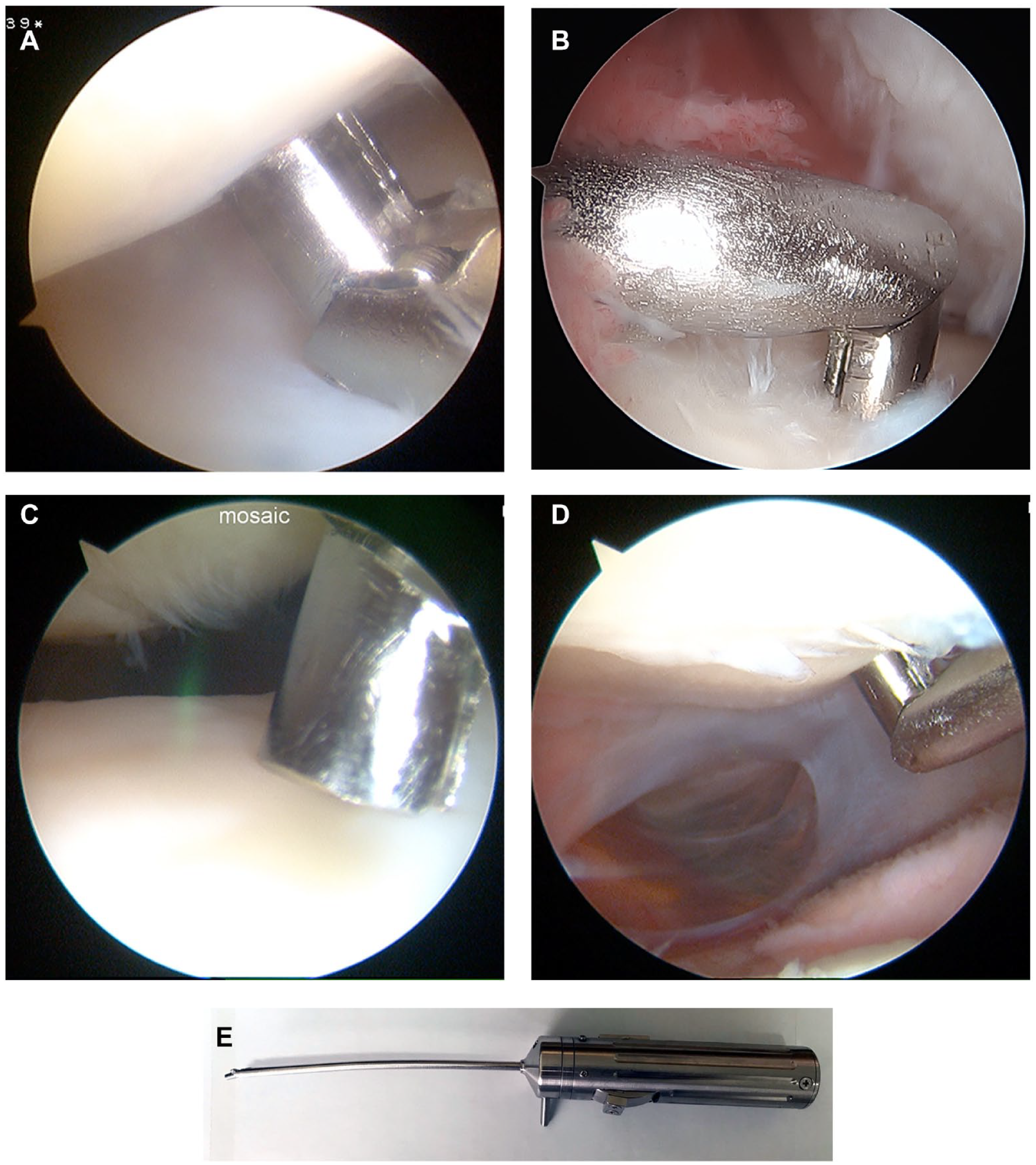
We developed an ultrasound assessment system to assess mechanical properties of cartilage, including stiffness, surface roughness, and thickness of joints such as knee.7,8 We also used an arthroscopic probe with a diameter of 3 mm, slightly smaller than that used in knee arthroscopy. Thus, we were able to assess the mechanical properties of living human knee cartilage using arthroscopy and the assessment system and probe we developed.
The objective of the present study was to evaluate the mechanical properties of living human knee cartilage using the ultrasonic system we developed, and to compare changes with respect to cartilage degeneration and aging. We compared the mechanical properties of living knee cartilage at different grades of the International Cartilage Repair Society (ICRS) classification (cartilage degeneration), and at grade 0, we compared the mechanical properties with respect to age and gender (cartilage aging).
Materials and Methods
During arthroscopy, acoustic evaluation is used to assess mechanical properties of cartilage, including stiffness, surface roughness, and thickness of the surrounding knee cartilage. The ultrasound assessment system we developed and used provides quantitative information on tissue properties.7
-10 Briefly, the system
8
consists of a digital oscilloscope, personal computer, and a transducer and pulser/receiver (Panametrics Japan, Tokyo, Japan). The diameter of the transducer, such as an arthroscopic ultrasonic probe, is approximately 3 mm. The central frequency of the ultrasound wave is 10 MHz. As the wave passes through interfaces between media of different acoustic impedances, reflections return to the transducer and generate electrical signals in the transducer proportional to the intensity.
11
Mori et al.
8
reported the validation study for this method.
(
Patients who satisfied the inclusion criteria (needed arthroscopic knee surgery and provided informed consent) over a 3-year period were enrolled. Written informed consent was obtained from all subjects before their participation. All procedures were reviewed and approved by the research ethics committee of our hospital, and the study was performed in accordance with the World Medical Association’s Declaration of Helsinki.
To assess cartilage degeneration, each point was examined via arthroscopic assessment using the ICRS classification (grades 0, 1, 2, and 3); mechanical properties were also assessed and compared with respect to the ICRS classification. In grade 0 per ICRS classification, which was considered normal cartilage, we compared mechanical properties of the knee cartilage with respect to aging and gender.
A two-sample one-sided and Mann-Whitney U test were used to perform statistical comparison of cartilage mechanical properties and ICRS classification to assess cartilage degeneration, or age and gender to assess cartilage aging. The level of statistical significance was set to P value < 0.05.
Results
Eighty-eight patients and 95 knee joints were enrolled. There were 41 men, 47 women, 39 right knee joints, and 56 left knee joints. The mean operative age was 44.1 years old (range = 10-83 years). The conditions were the following: 30 cases of knee osteoarthritis, 26 cases of ligament injuries, 17 cases of osteonecrosis, and 15 cases of cartilage injuries. In terms of ICRS classification, there were 663 points in grade 0, 87 points in grade 1, 93 points in grade 2, and 51 points in grade 3.
With respect to cartilage degeneration, the comparison of cartilage stiffness with ICRS classification is shown in
(
With respect to cartilage aging, the comparison of cartilage stiffness among the four groups is shown in
(
Discussion
The main findings of the present study are the following. In terms of cartilage degeneration, stiffness in grade 0 was significantly higher than that in grade 1, 2, or 3 (P < 0.0001). Stiffness in grade 1 was significantly higher than that in grade 3 (P = 0.0035). Surface roughness in grade 0 was significantly lesser than that in grade 1 (P = 0.0024). Thickness in grade 0 was significantly greater than that in grade 1, 2, or 3 (P < 0.0001). Thickness in grade 1 was significantly greater than that in grade 2 or 3 (P < 0.0001). Thickness in grade 2 was significantly greater than that in grade 3 (P = 0.0047). In terms of cartilage aging, stiffness in females of age more than 45 years was significantly lower than that in the other three groups. Thickness in females of age more than 45 years was significantly lesser than that in the other three groups. Stiffness in females of age less than 45 years was significantly lower than that in males of age less than 45 years. Thus, the ultrasonic system we developed was able to detect early degenerative changes in living cartilage in knee joints.
In assessing the mechanical properties of cartilage, Prakash et al. 12 showed that arthroscopic near-infrared spectroscopy (NIRS) could substantially enhance identification of damaged cartilage by enabling quantitative evaluation of cartilage biomechanical properties. Svard et al. 13 showed that cartilage degeneration could be identified both with mechanical indentation and T2-mapping in MRI. To evaluate changes in cartilage or meniscus thickness using MRI, Pelletier et al. 14 showed that a single intraarticular corticosteroid injection in knee osteoarthritis was safe with no negative impact on structural changes, but that there was a transient meniscal thickness reduction. Paranjape et al. 15 developed a cartilage stress test to measure the in vivo strain response of tibial cartilage in healthy human subjects to walking exercises. Karpinski et al. 16 showed that vibroarthrography could be an effective, low-cost and accurate diagnostic modality for the evaluation of cartilage damage in tibio-femoral joints and in patella-femoral joints. 17 Using our system, the stiffness, surface roughness and thickness of living human articular cartilage can be measured.
There have been some reports of measurement of cartilage characteristics using ultrasonic systems. Bedewi et al. 18 reported that women have a thinner cartilage than men, in a group of healthy adults. Another study showed that in a group of diabetes mellitus patients, females tended to have thinner femoral cartilage at both medial femoral condyles. 19 Schmitz et al. 20 found that individuals who walked with a greater peak internal knee-extensor moment during gait had a cartilage structure that is generally considered beneficial in a healthy population. Shimizu et al. 21 reported that their ultrasound measurement system offered potential for the detection of subtle change in cartilage. The measure of maximum magnitude was found to be particularly useful for quantitative assessment of the medial femoral condyle articular cartilage, and their system was useful for diagnosis of degenerate cartilage at the early stage. 21 Our system is able to measure stiffness, surface roughness, and thickness of living human articular cartilage, and it was able to detect early degenerative changes in living cartilage in knee joints.
As previously described, Mori et al.7,8 developed a device to measure the mechanical properties of the articular cartilages via ultrasound. Several studies that utilized this device reported significant results in terms of the mechanical properties of articular cartilages in humans and rabbits.9,10,22 -24 Hattori et al. 25 reported that the acoustic properties of living human cartilage differ between the knee and ankle joints, as observed using his arthroscopic ultrasonic probe and Mori’s system. Using Mori’s system and their arthroscopic ultrasonic probe, Nakagawa’s study demonstrated that the mean values of stiffness (relative value) and surface roughness at mosaicplasty in the Theracurmin® group were not significantly different from those in the placebo group. However, stiffness and surface roughness at second-look arthroscopy in the Theracurmin® group were significantly improved compared with the placebo group. 26 No significant differences existed in cartilage thickness between the two groups in the study. The study of Nicoliche et al. 27 demonstrated no increase in cartilage thickness in knees of rats with induced arthritis treated with curcumin, and it was similar to these results. Kuroki et al. 22 found that modified Mankin’s score was significantly correlated with stiffness and surface roughness.
In the relationship between cartilage degeneration and ultrasonic assessment, sonoelastography has been used to assess stiffness of the articular cartilage, hypothesizing that pathological cartilage was softer than normal cartilage.28,29 The measured instantaneous modulus in healthy cartilage was found to be significantly larger than that in diseased cartilage, and the thickness in healthy cartilage was significantly greater than that in diseased cartilage. 30 Although the very earliest osteoarthritis stages may result in an increase in cartilage thickness, the development and progression of clinical osteoarthritis are commonly characterized by structural changes, including erosion and loss of articular cartilage.31,32 Surface roughness metrics were found to be sensitive to degenerative morphologic changes, and may be useful in osteoarthritis characterization and early diagnosis. 33 Seitz et al. 34 reported that the medial compartment of the knee was much more affected by degenerative changes than the lateral compartment and suggested that the menisci were potentially degenerative earlier than the adjacent articular cartilage. We are able to measure stiffness, surface roughness, and thickness of human living articular cartilage using our system, and these three parameters were distinguishable between normal cartilage and degenerative stages per the ICRS cartilage classification.
In terms of the relationship of mechanical properties of cartilage with healthy cartilage or aging, Peters et al. 35 reported that cartilage shear modulus was strongly correlated to age, and Unal et al. 36 insisted that aggregate modulus of older specimens was significantly lower than that of young specimens. In terms of cartilage thickness, Wang and Liang 37 reported that the thickness of articular cartilage was gradually thinner at different ages. Bedewi 18 and Baboli et al. 38 showed that cartilage volume and thickness were significantly higher in male than female participants. Babayeva et al. 39 showed that femoral cartilage thickness was greater among athletes than among sedentary individuals, and suggested that sports participation was an independent factor associated with right and left mean femoral cartilage thickness. In the present study, in terms of cartilage aging, the stiffness in females of age more than 45 years was significantly lesser than that in the other three groups. The thickness in females of age more than 45 years was significantly lesser than that in the other three groups.
In terms of the relationship between early knee osteoarthritis and mechanical properties of the cartilage, Knecht et al. 40 reported that static modulus decreased below 80% of healthy controls and dynamic moduli below 30% of controls in early osteoarthritis. Fibril-reinforced poroelastic (FRPE) modeling revealed that non-fibrillar matrix modulus was higher in the healthy group compared with the early osteoarthritis and advanced osteoarthritis groups. The initial fibril network modulus was also higher in the healthy group compared with the early and advanced osteoarthritis groups.41,42 It was suggested that early degeneration could occur in the cartilage matrix prior to morphological changes, such as the loss of cartilage thickness. 43 Early degeneration was found to occur in various knee cartilage compartments after acute anterior cruciate ligament rupture, especially in the superficial layer of lateral tibia. 44 Storage modulus of osteoarthritis cartilage was shown to be significantly lower than that of healthy cartilage while having a higher capacity to hold water. Following mechanical testing, a significant increase in surface roughness of osteoarthritis cartilage was found. 45 Nakamura et al. 46 reported that stress relaxation optical coherence straingraphy could tomographically and nondestructively detect and visualize changes in the distribution of viscoelastic properties of articular cartilage in early osteoarthritis. In the present study, the ultrasonic system we developed was able to detect early degenerative changes in living cartilage in knee joints. In terms of cartilage aging, stiffness in females of age more than 45 years was significantly lesser than that in the other three groups. Thickness in females of age more than 45 years was significantly lesser than that in the other three groups. Mean cartilage stiffness and thickness in females of age more than 45 years were slightly similar to those of ICRS grade 1 cartilage. This may be one of the underlying factors for the overwhelmingly larger occurrence of knee osteoarthritis in females compared with males.
The limitations of the present study are in the relatively small number of cases (88), and the fact that it was an observational study and not longitudinal.
In conclusion, the ultrasonic system we developed was able to detect early degenerative changes in living cartilage in knee joints. The lowest signal intensity and least cartilage thickness in normal cartilage among older women were correlated to a large prevalence of knee osteoarthritis in women.
Footnotes
Authors’ Note
This manuscript has not been submitted or is not simultaneously being submitted elsewhere, and that no portion of the data has been or will be published in proceedings or transactions of meetings or symposium volumes.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from the institutional review board.
Informed Consent
Written informed consent was obtained from all subjects before conducting this study.