
Abstract
Objective
To compare cartilage quality after different surgical interventions for osteochondral lesions of the talus (OLT), evaluated by second-look arthroscopy. Secondary aims were to report concomitant diagnoses, and to correlate cartilage quality with clinical and radiological outcomes. This review hypothesizes that the cartilage repair after bone marrow stimulation (BMS) is inferior to the other available treatment options.
Methods
PROSPERO ID: CRD42022311489. Studies were retrieved through PubMed, EMBASE (Ovid), and Cochrane Library. Studies were included if they reported cartilage quality after second-look investigation after surgical treatment of OLT. The primary outcome measure was the cartilage quality success and failure rates (%) per surgical intervention group. Correlations between the cartilage quality and clinical or radiological outcomes were calculated.
Results
Twenty-nine studies were included, comprising 586 ankles that had undergone second-look arthroscopy on average 16 months after initial surgery. The success rate for BMS was 57% (95% confidence interval [CI] = 48%-65%), for fixation (FIX) 86% (95% CI = 70%-94%), for osteo(chondral) transplantation (OCT) 91% (95% CI = 80%-96%), for cartilage implementation techniques (CITs) 80% (95% CI = 69%-88%), and for retrograde drilling 100% (95% CI = 66%-100%). The success rate of BMS was significantly lower than FIX, OCT, and CIT (P < 0.01). There were no significant differences between other treatment groups. A moderate positive significant correlation between the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score and the International Cartilage Repair Society score (ICRS) was found (ρ = 0.51, P < 0.001).
Conclusions
Successful restoration of cartilage quality was found in the majority of surgically treated OLTs. However, BMS yields inferior cartilage quality compared with FIX, OCT, and CIT. Study Design. Systematic review and meta-analysis. Level of evidence. Level IV, systematic review and meta-analysis.
Introduction
An osteochondral lesion of the talus (OLT) is defined as damage to the talar cartilage and its underlying subchondral bone, 1 often caused by an ankle trauma. 2 Compared with other articular cartilage, ankle cartilage is composed of identical cell types and matrix component. 3 However, it differs in thickness, biomechanical, and biochemical properties, making it more susceptible for post-traumatic osteoarthritis. 3 Hence, the fraction of post-traumatic etiology is the greatest in the ankle compared with other lower-limb joints. 4 Since cartilage has limited intrinsic capacity to regenerate, 5 it is a challenge to treat OLTs.
When conservative treatment fails (in 38% of the cases), 6 a wide range of surgical options are available, such as bone marrow stimulation (BMS), retrograde drilling, internal fixation (FIX), osteo(chondral) transplantation (OCT), and chondrocyte implantation. However, up to now, there is no evidence for a superior treatment option for OLTs in terms of patient-reported outcomes.6,7 Clinical success rates of different treatments average between 75% and 85%, which means that 15%-25% of the patients has persistent symptoms after treatment for primary or secondary OLTs. 6
A potential explanation for these persistent symptoms is that the cartilage may not be fully restored to hyaline-like cartilage, resulting in increased stress to the subchondral bone and also may predispose patients for osteoarthritis, 75 which in turn is associated with physical and mental impairments.8,9 It is even thought that BMS leads—more so than other treatments—to cartilage regeneration of a nature other than hyaline-like cartilage. The confirmation of repair quality can be achieved through second-look arthroscopy, which allows a direct visual evaluation of the cartilage. 10 Although it is not a standard procedure in clinical practice, several studies have used second-look arthroscopy as an outcome measure, providing an opportunity to compare the treatments’ capability to stimulate the cartilage regeneration of the OLTs.11-13 Insight in how successful the different treatments are in restoration of the cartilage may aid the clinician—and the patient alike—in their shared clinical decision making to determine the right treatment for each individual patient. An overview of the literature might support this clinical decision.
Therefore, this systematic review aims to assess the success and failure rates of cartilage repair of OLTs, as assessed during second-look arthroscopy, between different surgical techniques. We hypothesize that the cartilage repair after BMS is inferior to the other available treatment options. In addition, qualitative descriptions of the macroscopic appearance of cartilage and concomitant diagnoses will be evaluated. The secondary aim is to determine the relationship between cartilage quality and clinical or radiological outcomes.
Methods
A systematic review of the literature was performed and was reported according to the methodology of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 14 The study was pre-registered at PROSPERO with ID: CRD42022311489.
Search Strategy
The PubMed, EMBASE (Ovid), and Cochrane Library databases were searched from inception up to November 25, 2023 for potentially eligible articles. The following keywords were used: “osteochondritis dissecans,” “osteochrondrosis,” “osteochondrolysis,” “talar,” “osteochondral,” “lesion,” including synonyms and MeSH terms. The full search strategy is outlined in Appendix 1.
Study Selection and Eligibility Criteria
Two independent reviewers (JV and JD) screened titles and abstracts using predefined criteria in Rayyan. 15 Subsequently, articles were screened for full text and included when they met the inclusion criteria ( Table 1 ). Discordant judgment in study inclusion was resolved by consensus discussion together with a third reviewer (KSE).
Inclusion and Exclusion Criteria.
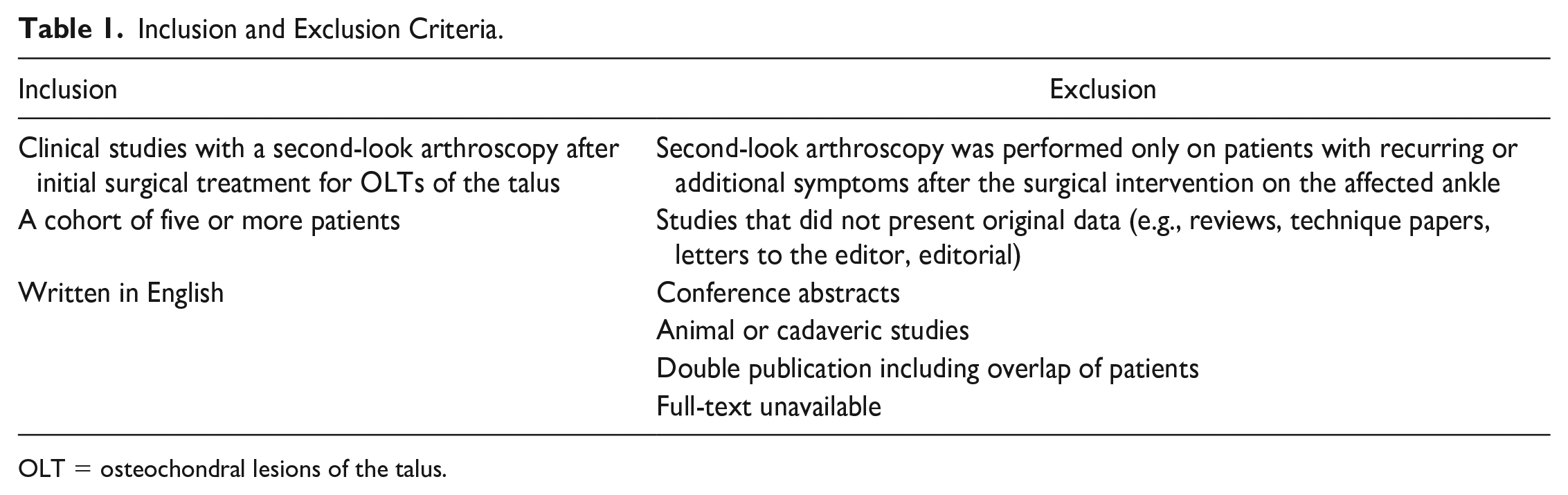
OLT = osteochondral lesions of the talus.
Methodological Quality Assessment
Methodological quality of the studies was evaluated using the validated Methodological Index for Non-Randomized Studies (MINORS) criteria 16 by two independent reviewers.
Data Extraction
The following study characteristics were retrieved: authors, year of publication, and study design. Also, the following patient characteristics were retrieved: gender, age, number of lesions, number of ankles, area, size, and location of the lesion, type of index surgical intervention, timing of second-look arthroscopy after index surgery, and methods for clinical and radiological assessment, and their corresponding outcomes.
Outcome Measures
The primary outcome was the success and failure rates of cartilage repair as assessed during second-look arthroscopy and based on formal scoring systems.
Secondary outcomes were descriptions of the second-look macroscopic evaluation of the cartilage outside of scoring systems and the presence of concomitant diagnoses. Furthermore, correlations between cartilage repair scores and clinical or radiological outcomes were either collected or calculated.
Treatment Classification
All included patient were assigned to treatment groups, using the grouping method as previously described by Steman et al. 17
Data Analysis
Primary outcome measure
We dichotomized all scoring systems in either “successful” or “failed” repair ( Table 2 ). The International Cartilage Repair Society (ICRS) score 22 was used as primary scoring system. Secondarily, the scoring systems by Nam et al. 18 and Takao et al. 19 were extracted if used as well. The overall dichotomized cartilage success and failure rates were pooled using a random effects model in R version 4.1.0 (R Core team, Vienna, Austria; metaprop function from the meta package 20 ). The Clopper-Pearson interval was used to assess 95% confidence intervals (CIs). Differences in treatment success were compared between treatments using a moderator test for subgroup analysis with an α < 0.05 indicating statistical significance. 21
Description and Dichotomization of Grading Systems Included in Analyses.
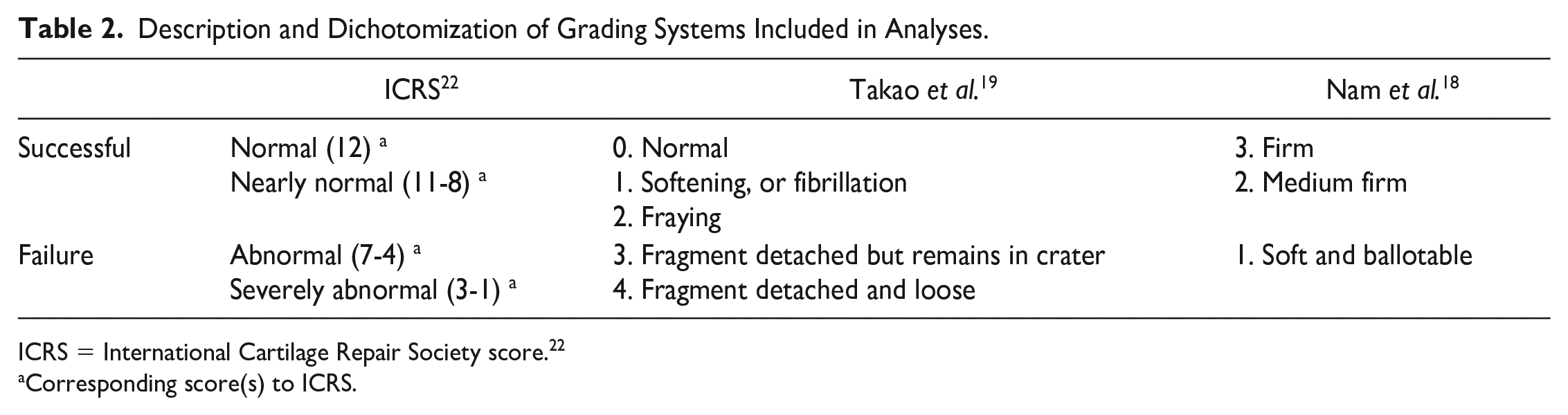
ICRS = International Cartilage Repair Society score. 22
Corresponding score(s) to ICRS.
Secondary outcome measures
Qualitative descriptions of macroscopic cartilage appearance were categorized in “degree of integration to border zone” or “general macroscopic appearance,” “degree of defect repair,” and “other qualitative valuations.” For clarification purposes, subcategories were created (such as “Cartilage Appearance,” “Integration,” “Stableness,” “Firmness”). A numeric and percentage wise presentation of the ankles was given per description.
Concomitant diagnoses found during second-look arthroscopy were collected and pooled per treatment group.
Reported correlations between cartilage quality and clinical and radiological outcomes were collected. If the correlations were not described, but individual data were present, correlations were calculated using SPSS (Version 26. IBM Corp. Armonk, NY). A maximum window of 3 months between the mean second-look arthroscopy timing and either the mean clinical follow-up timing or the mean radiological follow-up timing per study was allowed for this analysis. In case of normally distributed data, Pearson’s correlation coefficients were calculated. Otherwise, Spearman’s rank-order correlation test was used. 23
Results
Search Results
After removal of duplicates, the literature search resulted in 2,246 articles. After screening titles and abstracts, 521 articles were included for full-text screening. A total of 29 articles were included for analysis ( Fig. 1 ).
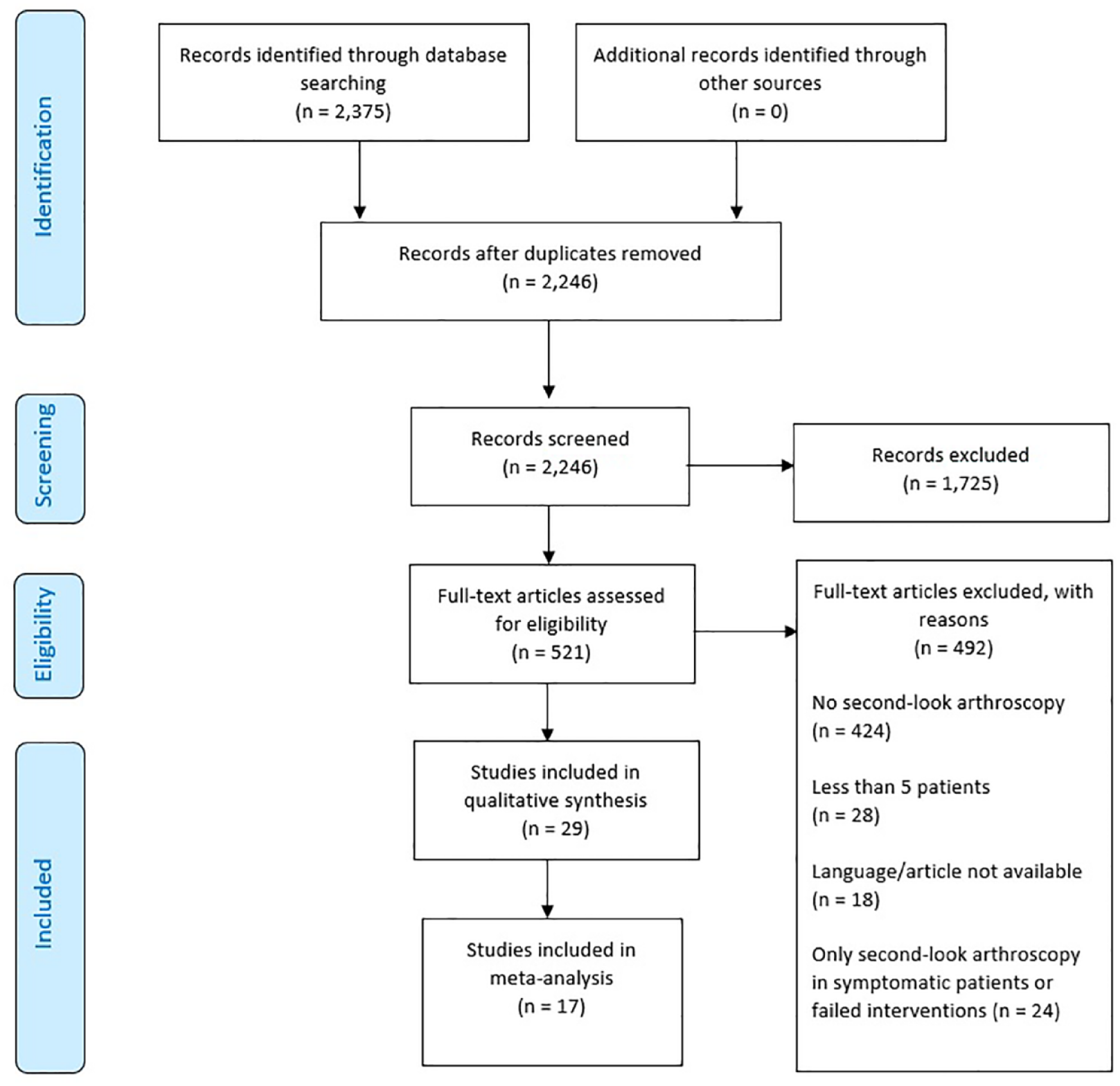
PRISMA 2009 flow diagram. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Methodological Quality
The overall methodological quality of non-comparative studies ranged from 13% to 63% and for comparative studies from 46% to 79%. The MINORS criteria for comparative and non-comparative studies are shown in Appendices 2 and 3, respectively.
Study Characteristics
The 29 studies reported a total of 872 lesions in 870 ankles in 862 patients. Of those 870 ankles, a total of 586 ankles (67%) underwent second-look arthroscopy and were included. The average age of the patients was 33 years (range among studies: 14-81 years) and 65% were men (range among studies: 31%-89%). The average preoperative lesion size was 181 mm2 (range among studies: 7-758 mm2). The use of preoperative radiological modality was reported in 26 studies (90%). The mean time of the second-look arthroscopy was 16 months (range among studies: 6-43 months) after the initial surgery (
Tables 3
and
Patient Characteristics.
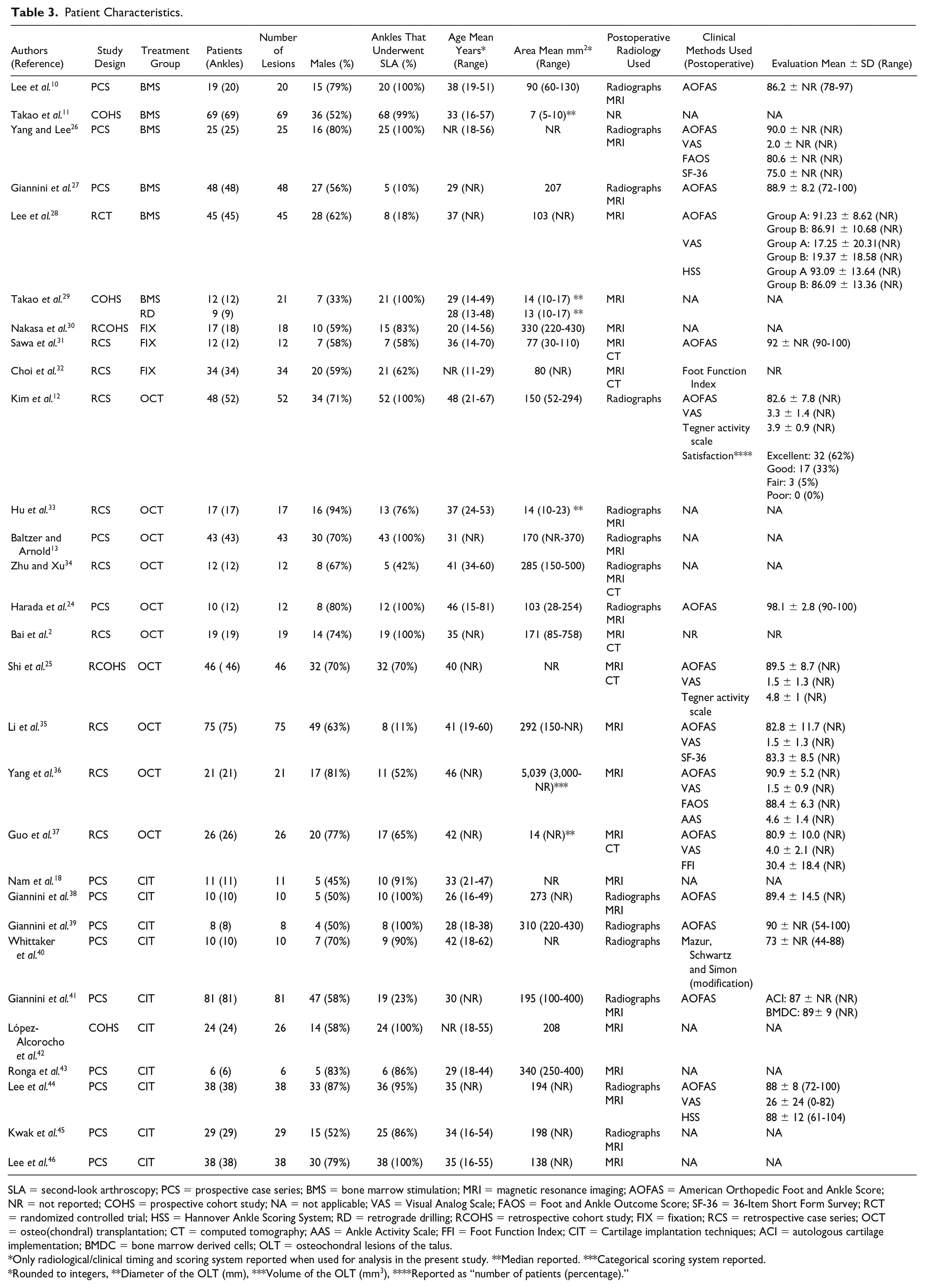
SLA = second-look arthroscopy; PCS = prospective case series; BMS = bone marrow stimulation; MRI = magnetic resonance imaging; AOFAS = American Orthopedic Foot and Ankle Score; NR = not reported; COHS = prospective cohort study; NA = not applicable; VAS = Visual Analog Scale; FAOS = Foot and Ankle Outcome Score; SF-36 = 36-Item Short Form Survey; RCT = randomized controlled trial; HSS = Hannover Ankle Scoring System; RD = retrograde drilling; RCOHS = retrospective cohort study; FIX = fixation; RCS = retrospective case series; OCT = osteo(chondral) transplantation; CT = computed tomography; AAS = Ankle Activity Scale; FFI = Foot Function Index; CIT = Cartilage implantation techniques; ACI = autologous cartilage implementation; BMDC = bone marrow derived cells; OLT = osteochondral lesions of the talus.
Only radiological/clinical timing and scoring system reported when used for analysis in the present study. **Median reported. ***Categorical scoring system reported.
Rounded to integers, **Diameter of the OLT (mm), ***Volume of the OLT (mm3), ****Reported as “number of patients (percentage).”
Study Characteristics.
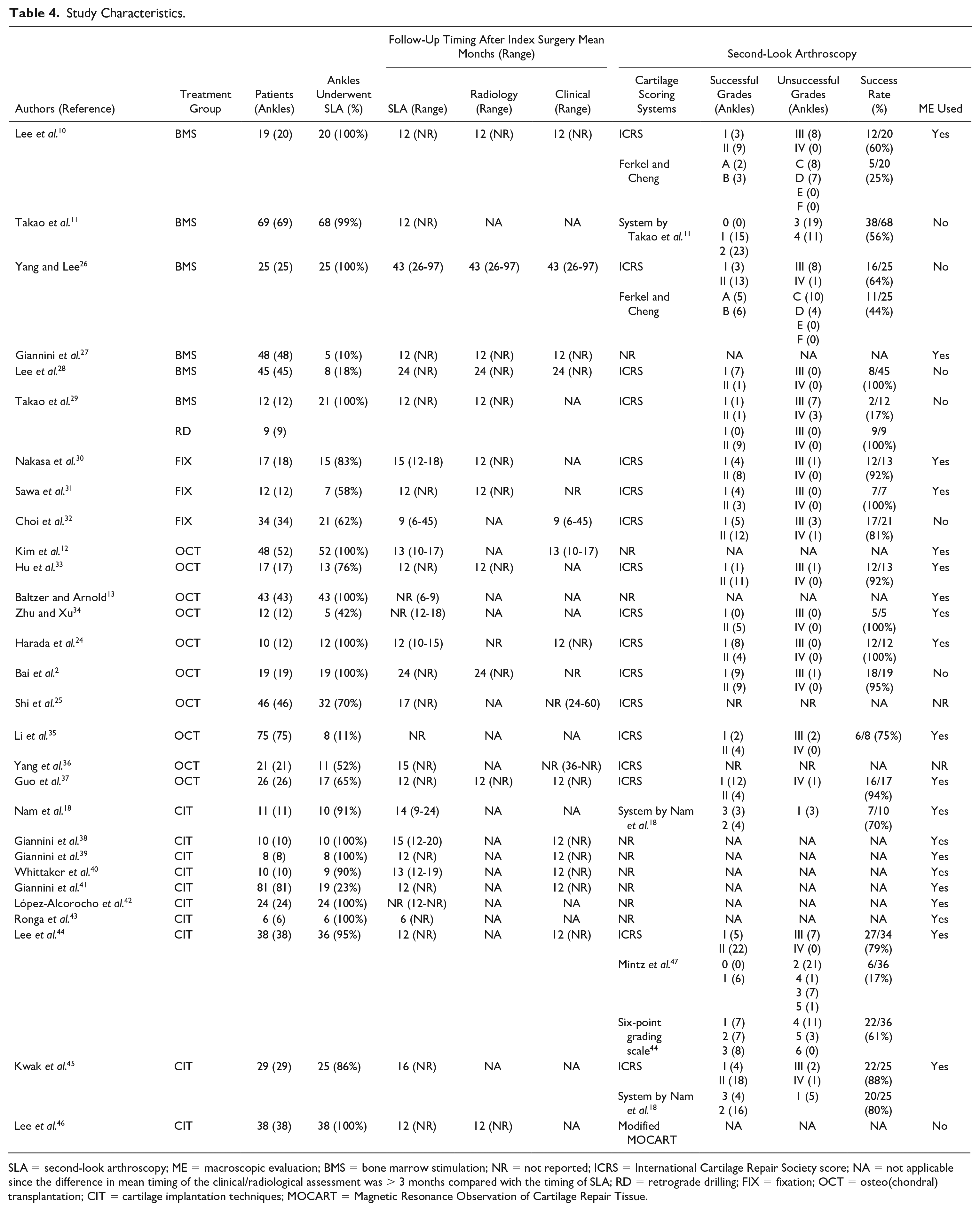
SLA = second-look arthroscopy; ME = macroscopic evaluation; BMS = bone marrow stimulation; NR = not reported; ICRS = International Cartilage Repair Society score; NA = not applicable since the difference in mean timing of the clinical/radiological assessment was > 3 months compared with the timing of SLA; RD = retrograde drilling; FIX = fixation; OCT = osteo(chondral) transplantation; CIT = cartilage implantation techniques; MOCART = Magnetic Resonance Observation of Cartilage Repair Tissue.
Treatment Groups
The patients received the following surgical treatments: BMS (n = 138), retrograde drilling (n = 9), FIX (n = 43), OCT (n = 212), and cartilage implantation techniques (n = 185) (Appendix 4). The weighted mean timing of second-look arthroscopy after BMS, FIX, retrograde drilling, OCT, and cartilage implantation techniques, was 20, 11, 12, 14, and 13 months, respectively.
Success and failure rates
Twenty studies used a cartilage scoring system ( Table 4 ). The ICRS was used most frequent (17 studies; 59%). The pooled overall success rate was 79% (21% failure, 95% CI = 69-87; I2 = 62%; Fig. 2 ). The success rate of BMS (57%, 43% failure, Fig. 2 ) was significantly lower than FIX (86%, 14% failure; χ2 = 9.09.48, P < 0.01), OCT (91%, 9% failure; χ2 = 16.38, P < 0.01), and cartilage implementation techniques (CITs; 80%, 20% failure; χ2 = 9.88; P < 0.01). BMS and retrograde drilling (100%, no failure, from one study only) did not differ significantly. There were no significant differences in success rates between the other treatment groups ( Fig. 2 ).
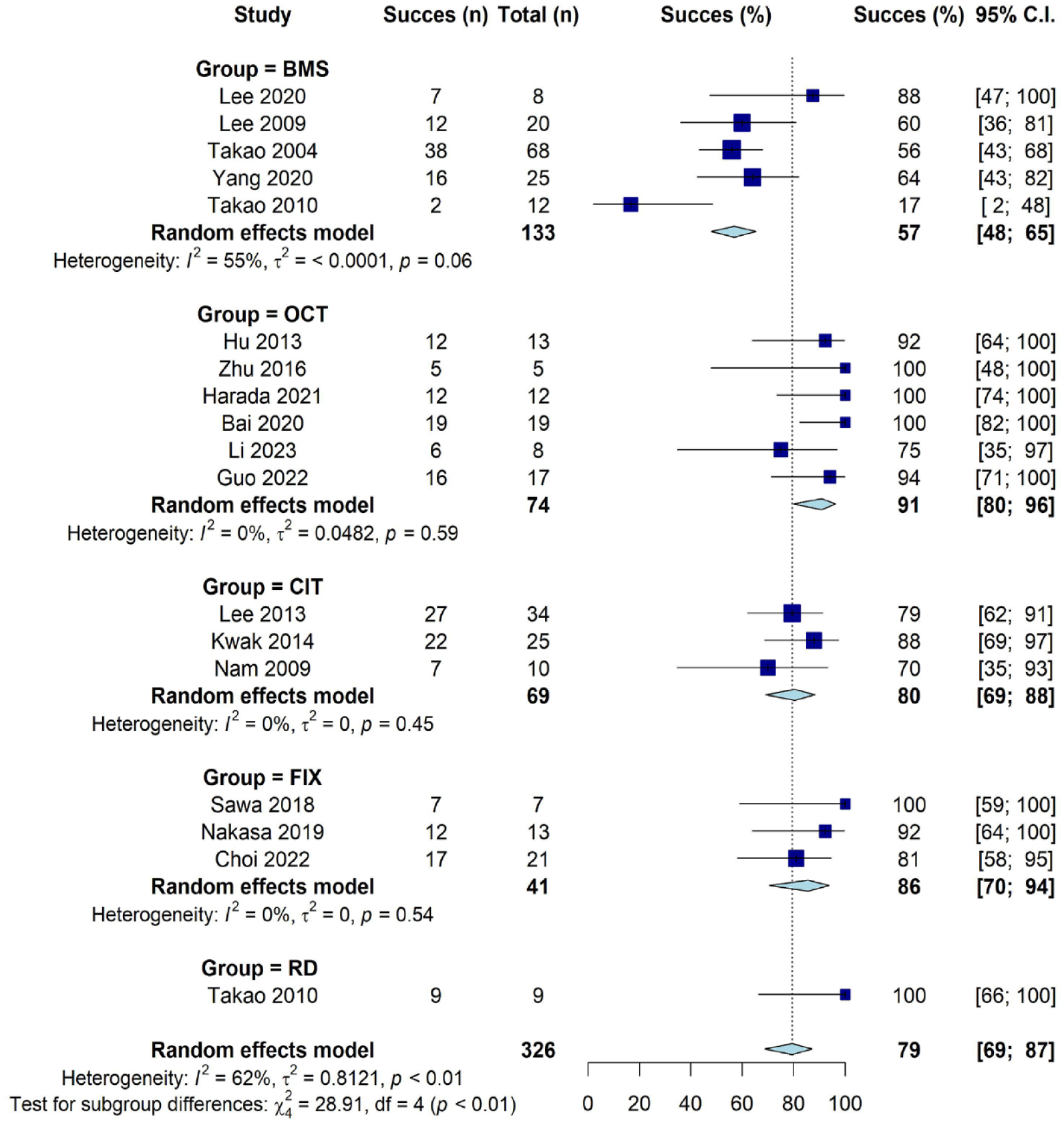
Forest plot of success rates of cartilage scoring systems by included studies. BMS = bone marrow stimulation; FIX = fixation; RD = retrograde drilling; OCT = osteo(chondral) transplantation; CIT = cartilage implantation techniques; ICRS = International Cartilage Repair Society score; CI = confidence interval.
Macroscopic Evaluation of the Repair Cartilage
Sixteen studies reported a qualitative description of macroscopic cartilage evaluation during second-look arthroscopy ( Table 5 ). Regarding the macroscopic appearance of the cartilage for OCT and CITs, the described quality of the repair cartilage in all ankles were either “cartilage-like” or “hyaline-like.”
Macroscopic Appearance.
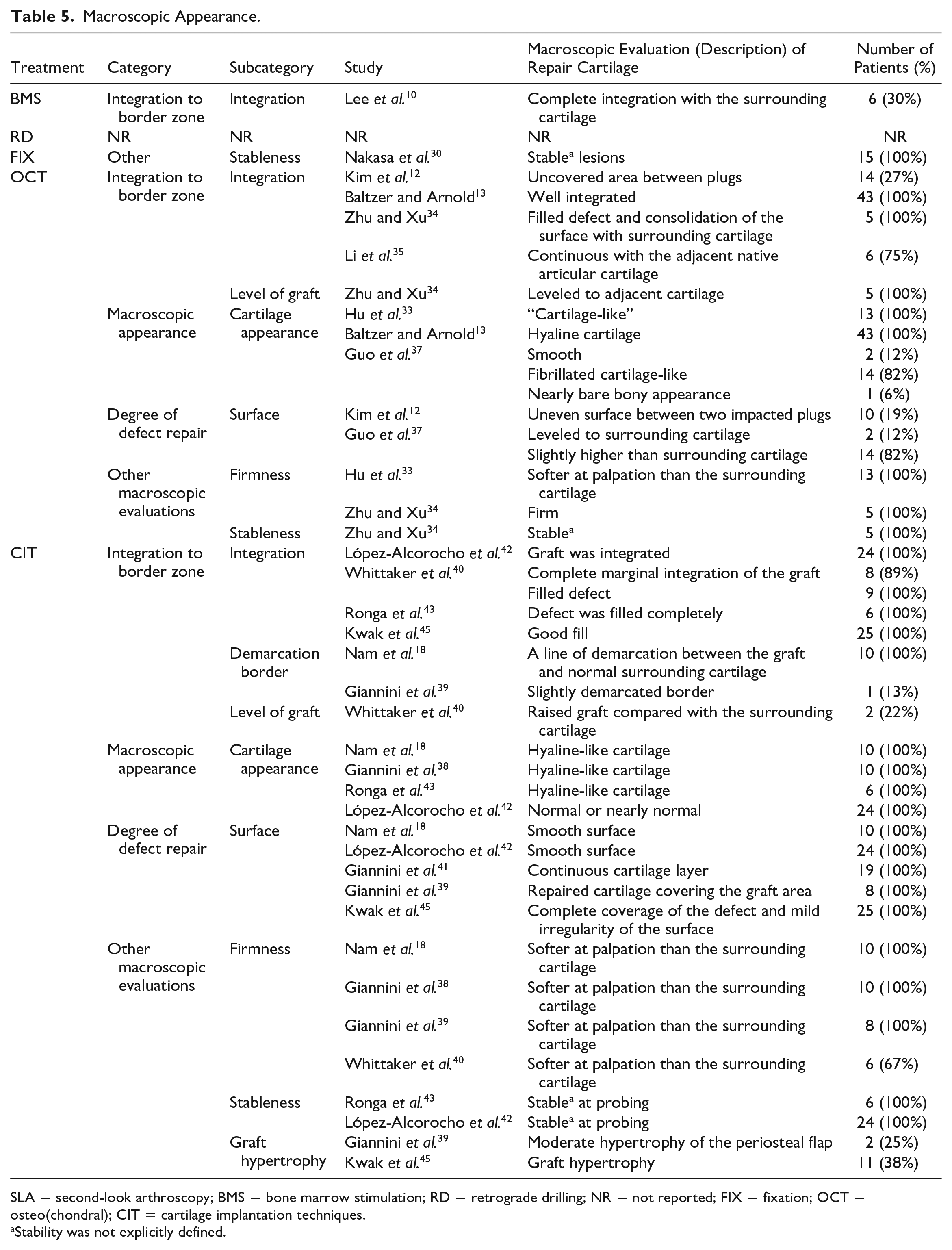
SLA = second-look arthroscopy; BMS = bone marrow stimulation; RD = retrograde drilling; NR = not reported; FIX = fixation; OCT = osteo(chondral); CIT = cartilage implantation techniques.
Stability was not explicitly defined.
Concomitant Diagnoses
Eleven studies with a total of 213 patients (25%) reported concomitant diagnoses at second-look arthroscopy ( Table 6 ). The most reported concomitant diagnosis was fibrous adhesion, which was found in 29% of the investigated OCT patients.
Concomitant Diagnoses Per Treatment.
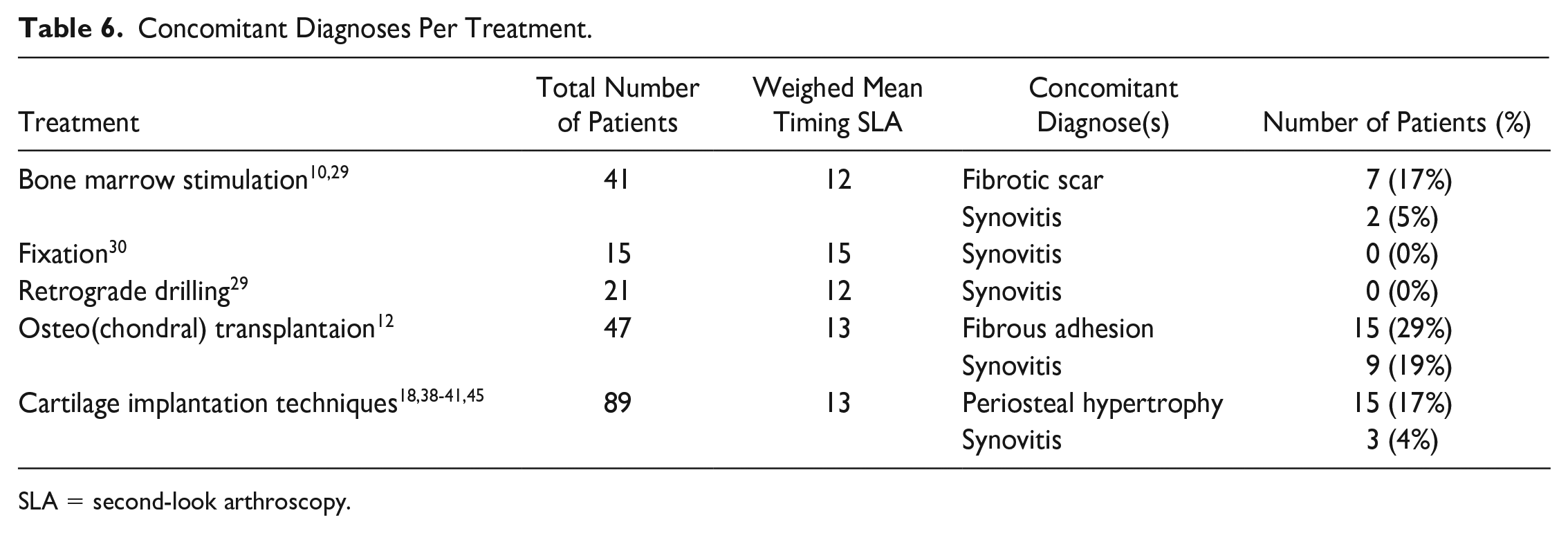
SLA = second-look arthroscopy.
Relation Between Second-Look Arthroscopy Cartilage Quality and Clinical Outcomes
Thirteen studies with a total of 258 patients (30%) reported clinical evaluation within 3 months of second-look arthroscopy ( Table 4 ). The weighted mean timing of the follow-up of clinical assessment was 15 months after the index surgery. From these 13 studies, four had eligible data to be used in this review.
In a BMS cohort, Lee et al. 10 reported higher mean American Orthopedic Foot and Ankle Society 48 (AOFAS) scores in the successful repair group compared with the unsuccessful repair group, 88.7 (n = 12) versus 82.5 (n = 9), P = 0.005, at 12-month follow-up.
Yang and Lee 26 reported that the mean Foot and Ankle Outcome Scores 49 (FAOS) was higher in patients with successful cartilage repair, 86.8 (n = 16) versus 75.6 (n = 9), P < 0.05, at 43-month follow-up. Furthermore, Kim et al. 12 found higher mean Visual Analog Scale 50 (VAS) scores of pain in the presence of adhesion of the cartilage, 4.5 (n = 15) versus 3.6 (n = 37), P = 0.025, at 13-month follow-up. Also, a lower mean AOFAS score was found in the presence of adhesion, 78.4 (n = 15) versus 81.4 (n = 37), P = 0.005. In case of a graft with uncovered areas, a higher mean VAS, 4.8 (n = 14) versus 3.5 (n = 38), P = 0.002, and a lower mean AOFAS score, 72.1 (n = 14) versus 82.1 (n = 38), P = 0.001, were found.
Choi et al. 32 reported that the ICRS and the Oswestry Arthroscopy score 51 were negatively correlated with the Foot Function Index 52 (Pearson’s correlation coefficient, r = −0.65, P = 0.001).
In a CITs cohort, Lee et al. 44 reported a higher mean Hannover Scoring System 53 (HSS) for the successful ICRS grades, 95 (n = 27) versus 85 (n = 9, P = 0.047). Neither the mean VAS nor mean AOFAS score was significantly different for successful versus unsuccessful grades.
Relation Between Second-Look Arthroscopy Cartilage Quality and Radiology
Eleven studies with a total of 266 patients (31%) reported radiological evaluation within a 3-month window from second-look arthroscopy ( Table 4 ). Seven of those studies, with a total of 164 patients (62%), reported a Magnetic Resonance Observation of Cartilage Repair Tissue 54 (MOCART) score.
Yang and Lee, 26 a BMS study, reported a median MOCART score of 68 (range = 30-95) corresponding to a median ICRS of 10 (range = 3-12) as well as a median Ferkel and Cheng 55 grade of C (range = A-D). In addition, this study reported a discrepancy between magnetic resonance imaging (MRI) and second-look arthroscopy findings in six of the 25 cases (24%).
Analysis of individual patient data of three OCT studies2,33, 37 showed a moderate positive significant correlation between the MOCART score and the ICRS (n = 42, ρ = 0.51, P < 0.001).
Discussion
The most important finding of this review was that second-look arthroscopy showed successful restoration of cartilage quality in the majority of patients after different surgical treatments for OLTs. Successful cartilage repair was found in 80%-100% of the patients in most treatment groups. The success rate of BMS (57%) was markedly lower, which may suggest inferior repair capabilities.
It is known that BMS elicits a repair response by recruiting blood- and bone marrow-derived mesenchymal stem cells to injury site, where they stimulate the regeneration of the cartilage. 56 A potential explanation for the fact that BMS yielded an inferior cartilage quality is that this surgical intervention does not preserve the native hyaline cartilage, but instead promotes the regeneration of cartilage. Regeneration often results in fibrocartilage, 57 which has been shown to deteriorate over time.58-61 Furthermore, the weighted mean timing of second-look arthroscopy was 20 months for BMS compared with 12-14 months for the other treatments groups, which could have added to the inferior appearance of cartilage. It is not known whether the quality of the cartilage after BMS will decrease further after a longer follow-up period. Moreover, selection bias may be present due to the general consensus that BMS should be the primary option for relatively small defects. 62 Another explanation may be that BMS has a potential negative effect on the quality of the subchondral bone plate, as shown by Reilingh et al. 63 and Seow et al. 59 An animal study on minipigs suggests that BMS in the knee leads to the irregularities of the subchondral bone plate as well as bone resorption after 6 months. 56 It is known that irregularities may influence joint mechanics, uneven loading of the cartilage, and in severe cases to joint impingement. 56
In quantitative analysis, we found high success rates for retrograde drilling (100%), FIX (86%), OCT (91%), and CITs (80%). These procedures all aimed to preserve the native cartilage,44,64,65 which may explain a satisfying macroscopic appearance upon second-look arthroscopic inspection. In the knee, similar numbers were reported when comparing autograft transplants with BMS after second-look arthroscopy (84% vs. 57%), which was confirmed by histological analysis of biopsies. 66 For chondrocyte transplantation techniques, a significantly higher success rate (80%) was found than with BMS. A systematic review on BMS versus autologous chondrocyte transplantation in the knee cautiously concluded that the quality of the cartilage is higher after autologous chondrocyte transplantation. 76 First-generation autologous chondrocyte transplantation studies found no significant differences in cartilage quality compared with BMS. 67 Also, no difference in regeneration of tissue was found on MRI between the two treatments on talar defects. 68 Reported qualitative analyses of the macroscopic appearance of the cartilage for OCT and CTIs was in line with the found high success rates in this review, as the quality of the repair cartilage in all ankles were described as either “cartilage-like” or “hyaline-like.”
The results of the cartilage quality of the retrograde drilling treatment are in line with pre-formed expectations, as the indication for this intervention is an intact layer of intra-articular hyaline cartilage and a degraded subchondral bone. The overlying cartilage will not be removed during the surgery, and therefore, no cartilaginous injury is expected to be uninjured directly after surgery.69,70 However, despite the perioperatively uninjured cartilage, second-look arthroscopy might still be relevant since an altered condition of the subchondral bone potentially affects the cartilage condition.
In general, macroscopic evaluation with second-look arthroscopy is limited to the surface of the repaired cartilage. Histological analysis is regarded as the gold standard in assessing cartilage quality, allowing assessment of the molecular structure of the cartilage, cellularity, integrity, and proteoglycan content throughout the entire thickness of the cartilage. 71 However, a biopsy potentially damages the regenerated tissue, and represents only a fraction of the repaired area. 77 Kok et al. 71 reported that the macroscopic ICRS poorly correlates to the histological O’Driscoll score in a goat model. Furthermore, a low number of histological scoring systems for repaired osteoarthritic cartilage are actually currently validated. 78 Second-look arthroscopy may be a less damaging alternative, and future studies should determine the correlation between second-look arthroscopy cartilage quality scoring systems, histological analyses, and clinical outcomes.
There were only four studies—two BMS studies, one OCT study, and one CIT study—that reported correlation between cartilage quality and clinical outcomes. The two BMS studies showed a moderate to strong positive correlation between the ICRS and the AOFAS and FAOS scores at 12 months postoperatively.10,26 Kim et al. 12 showed a significant difference of OCT between the successful quality versus unsuccessful quality of the cartilage with their respective clinical scores, in contrast to Lee et al., 44 who found a mix of significant and non-significant differences between clinical scores and successful versus unsuccessful grades.
These findings imply that there might be a relationship between the cartilage quality and these clinical outcomes. Therefore, the low BMS cartilage success rates (57%)—as shown in this review—would suggest that also low clinical success rates would be achieved for BMS. However, Dahmen et al. 6 reported clinical effectiveness—based on 52 studies—at medium-term follow-up (weighted means range from 26 to 52 months) for BMS (78%-86%). This indicates that good clinical outcomes at medium-term follow-up can be achieved despite an inferior success rate of the repair cartilage at a weighted mean of 16 months.
Eleven studies reported concomitant diagnoses in the ankle (ranging from 0% to 29%). In the OCT group, synovitis and adhesion were the most reported concomitant diagnoses during second-look arthroscopy. Kim et al. 12 reported that significant differences were found between clinical outcomes (AOFAS, and VAS) and the presence or absence of adhesion. However, they also reported that no significant differences were found between clinical outcomes (AOFAS and VAS) and the presence nor absence of synovitis at the time of second-look arthroscopy.
This review found a significant moderate positive correlation between the MOCART and the ICRS score in 42 patients. Moreover, Lee et al. 72 (n = 26 OLTs) compared MRI and arthroscopy 1 year after autologous chondrocyte implantation. They found that there was good reliability with respect to the categories “degree of defect repair,” “defect filling,” “cartilage repair,” and “synovitis.” However, one of the included studies reported a discrepancy between the MRI and second-look arthroscopy in 24% of the cases. Also, Lee et al. 72 found poor to moderate reliability between MRI and arthroscopy for the categories “integration to border zone,” and “adhesion.” Therefore, it might be insufficient to use an MRI to assess the quality of the cartilage, and more suitable to perform second-look arthroscopy. However, a second-look arthroscopy is much more invasive than MRI. So, the physician must weigh the added value of a second-look arthroscopy compared with the MRI in a shared clinical decision with the patient.
This review has several limitations. First, selection bias might be present, as different populations were included for different treatments, and hence treatment groups lack comparability. 62 Our main finding is that the quality of cartilage after BMS is inferior to other treatments. As BMS is usually the treatment that is implemented in relatively forgiving populations, with smaller size lesions and without history of prior surgery, it is not likely that selection bias is the reason for the poor outcome of this group. Second, The ICRS score was used as the main scoring system. Since the ICRS is validated for assessing the (repair) cartilage in the knee and is the most used system by the included studies in this review, the authors hypothesized that the scoring system was well applicable for scoring the ankle cartilage. 73 However, high-quality validation studies for the ankle cartilage are necessary to confirm these results. Also, only 59% of the included studies reported this scoring system. Third, to be able to include all studies that systematically graded cartilage quality, other scoring systems (by Takao et al. 19 and Nam et al. 18 ) were used when the ICRS was not present, introducing potential heterogeneity in the analysis. Fourth, the mean timing of the second-look arthroscopy was 16 months. As a result, no conclusions can be drawn about the longer-term cartilage condition. Fifth, the treatment groups are relatively small. Hence, our statistical outcomes could be underpowered. Sixth, this review did not include histological examination in the analysis, as this fell outside the scope of our preregistered review. However, good correlation between histology and arthroscopy has been reported. 74 Seventh, the overall quality of the studies ranged from 13% to 79%, introducing potential bias, mainly due to the study design of the included articles and the unbiased assessment of the study endpoints. Eighth, 31% of the studies only evaluated the cartilage qualitatively, making the description of the cartilage subjective, and hence less convenient to use their data for quantitative analysis. Finally, of the 29 included studies, only two studies2,24 reported that the assessed second-look arthroscopy was performed by a different observer than the surgeon who performed the initial surgery. In general, caution is advised with the interpretation of these outcomes. Since in clinical practice, clinical outcomes are leading in decision-making, failing to restore cartilage quality alone does not equal clinical failure. Therefore, further research is necessary to determine whether differences in cartilage quality lead to different clinical outcomes.
Conclusion
Second-look arthroscopy after surgical treatment of OLTs of the talus shows successful cartilage scores in the majority (79%) of patients. Treatment with BMS showed a significantly lower success rate. Evaluation of cartilage quality with second-look arthroscopy correlated moderately with clinical outcome. Further research with appropriate study designs is necessary to determine the differences between treatment groups and the place of second-look arthroscopy in clinical practice.
Supplemental Material
sj-docx-1-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-2-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-3-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-4-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-4-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-5-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-5-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-6-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-6-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-7-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-7-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Supplemental Material
sj-docx-8-car-10.1177_19476035241227332 – Supplemental material for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-8-car-10.1177_19476035241227332 for Second-Look Arthroscopy Shows Inferior Cartilage after Bone Marrow Stimulation Compared with Other Operative Techniques for Osteochondral Lesions of the Talus: A Systematic Review and Meta-Analysis by Jelmer T. Vreeken, Jari Dahmen, Tobias Stornebrink, Kaj S. Emanuel, Alex B. Walinga, Sjoerd A.S. Stufkens and Gino M.M.J. Kerkhoffs in CARTILAGE
Footnotes
Acknowledgments and Funding
Hereby, the authors offer their great and sincere thanks to Inger Siervelt (clinical epidemiologist at Specialized Center for Orthopedic Research and Education), for assisting them in taking the appropriate statistical strategies in this systematic review. They would also like to thank AMC’s clinical librarian, F.S. van Etten-Jamaludin, for her assistance in the present systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.