
Abstract
Background
Hallux rigidus (HR) is a degenerative joint disorder of the first metatarsophalangeal joint (MTPJ), causing joint pain and stiffness. Surgical treatments, including cheilectomy, microfracture (MF) and dorsal oblique osteotomy (DOO), have been well described in current literature. However, the addition of matrix-induced chondrogenesis (MIC) via scaffold implantation with bone marrow aspirate concentrate (BMAC) is novel and hypothesized to significantly improve cartilage healing.
Objectives
This study aimed to (1) describe the COMM procedure—a novel combination of cheilectomy, DOO, MF, and MIC, as well as to (2) evaluate its early clinical outcomes in a series of 12 HR cases.
Study Design & Methods
This is a retrospective study of 11 patients (12 feet) with HR treated with the COMM procedure in our hospital from May 2022 to June 2023 by 3 fellowship-trained foot and ankle surgeons. All the patients have completed their 1-year clinical review, where we evaluated their Numeric Pain Rating (NPR), European Foot and Ankle Society (EFAS), and Short Form-36 (SF-36) scores (Physical Function [SF-PF] and Mental Health [SF-MH]), as well as satisfaction. Preoperative and postoperative scores were compared to determine the effect of treatment.
Results
There was statistically significant improvement in all scores (P < 0.05). EFAS Foot and/or Ankle and Sports scores improved from 9.3 to 20.0 and 3.8 to 9.4, respectively. SF-PF and SF-MH scores improved from 47.9% to 67.9% and 54.0% to 66.0%, respectively. Mean NPR at rest and during activity improved from 4.8 to 0.2 and 7.6 to 2.5, respectively. The mean postoperative satisfaction was 8.0, with 10 representing maximal satisfaction.
Conclusions
Despite being a small series, our study has shown good clinical outcomes and promising satisfaction rates among all patients who have undergone our COMM procedure.
Keywords
Introduction
Hallux rigidus (HR) is a degenerative joint disorder that debilitates the first metatarsophalangeal joint (MTPJ), resulting in recurrent pain, restricted motion and loss of function. 1 It is second only to hallux valgus as the most prevalent pathology of the first ray, affecting up to 10% of the adult population. 2 Various factors, such as trauma, repetitive micro-injury, infection or inflammation, hypermobility of the first ray, and achilles tendon shortening can contribute to HR. 3 Symptoms typically emerge unilaterally around the age of 40, although with time bilateral involvement may occur in up to 80% of cases. 4 Osteophyte formation and cartilage degeneration commonly occur dorsally in the early stages before eventually progressing to involve the entire joint, limiting dorsiflexion, and causing swelling, stiffness, as well as discomfort. 5
Initial management is typically non-invasive, involving physiotherapy to improve stiffness, anti-inflammatory medications for symptomatic relief, footwear, such as insoles, as well as activity modifications to limit the joint movement that triggers pain. With failure of conservative treatment, there are several surgical interventions to consider, for which the primary objectives are to alleviate pain, enhance functionality and improve overall quality of life. The choice of procedure, be it joint preserving or sacrificing, is largely determined by the etiology, severity, and patient expectations. For instance, joint-sparing treatments of moderate HR, such as cheilectomy and dorsal oblique osteotomy (DOO), have been well described in current literature. DOO achieves longitudinal joint realignment and decompression by shortening the metatarsal shaft, a safe and dependable procedure with relatively low incidence of complications. 6 Cheilectomy decompresses the joint by removing degenerate bone and cartilage. 7 However, the success rates of these procedures dwindle with disease progression, and reasonably so as they do not repair the damaged articular cartilage. For patients with moderate to severe HR, there remains no consensus on the single most effective surgical strategy. In comparison, the addition of a matrix-induced chondrogenesis (MIC) technique in the form of scaffold implantation with bone marrow aspirate concentrate (BMAC) in the first MTPJ8 -10 can be hypothesized to significantly improve cartilage healing compared with cheilectomy, microfracture (MF) or DOO alone.
This study aimed to (1) describe the novel COMM procedure—a combination of cheilectomy, DOO, MF, and MIC, as well as to (2) clinically evaluate its early clinical outcomes in a series of 12 HR patients treated with this approach.
Materials and Methods
This was a retrospective study of 11 consecutive patients (12 feet) with a diagnosis of isolated Grade 2 and 3 HR as per the Coughlin-Shurnas classification 11 and treated with the COMM procedure. The inclusion criteria were patients who have failed a minimum of 6 months of conservative treatment and yet to undergo other surgical procedures to treat the same condition. We excluded any patients who had (1) complete destruction of the first MTPJ with end stage arthritis, (2) hallux valgus deformity, (3) previous surgeries performed to the hallux, (4) other foot deformities that require concomitant procedures to be performed, and (5) pre-existing conditions to the hallux, such as podagra.
All the patients underwent the COMM procedure by 3 fellowship-trained foot and ankle surgeons, using either Chondro-Gide or Hyalofast after failing a trial of conservative treatment at our tertiary hospital in the period from May 2022 to June 2023, and completed their 1-year clinical review. Chondro-Gide (Geistlich Pharma, Wolhusen, Switzerland) is a porcine bilayer collagen type I/III membrane, 12 while Hyalofast (Anika Therapeutics, Bedford, MA) is a degradable polymer derived from hyaluronic acid benzyl ester that has induced chondrogenesis in mesenchymal stem cells when combined with autologous synovial fluid. 13 The exclusion criteria comprised patients under 18 years or over 75 years of age, those who were severely obese (body mass index > 40), revision surgery, and non–osteoarthritis-related cases, such as gout.
Functional outcomes were evaluated via the following clinical questionnaires and patient-reported outcome measures (PROMs):
Numeric Pain Rating (NPR) at rest and during activity—graded from 0 to 10, where 0 = no pain, 10 = maximum pain.
Degree of postoperative satisfaction—graded from 0 to 10, where 0 = no satisfaction, 10 = maximum satisfaction.
European Foot and Ankle Society (EFAS) score, which is further classified into Foot and/or Ankle (EFAS-FA) and Sports (EFAS-S) scores—graded from 0 to 24 and 16, respectively, where 0 = worst condition of the foot, 10 = best condition. 14
Short Form-36 (SF-36) score, in particular the Physical Function (SF-PF) and Mental Health (SF-MH) domains—graded on a percentage scale of 0-100, where 0 = worst score, 100 = best score. 15
The EFAS score was used in its capacity as a validated foot and ankle surgery functional assessment of mobility 12 while to date, the SF-36 is the most used measure of health-related quality of life (HRQoL) which comprises both physical function and mental health domains. 15 Peterson et al. 16 suggested that tabulating SF-36 subscores were potentially more sensitive than inquiring about activities of daily living (ADLs).
Surgical Technique
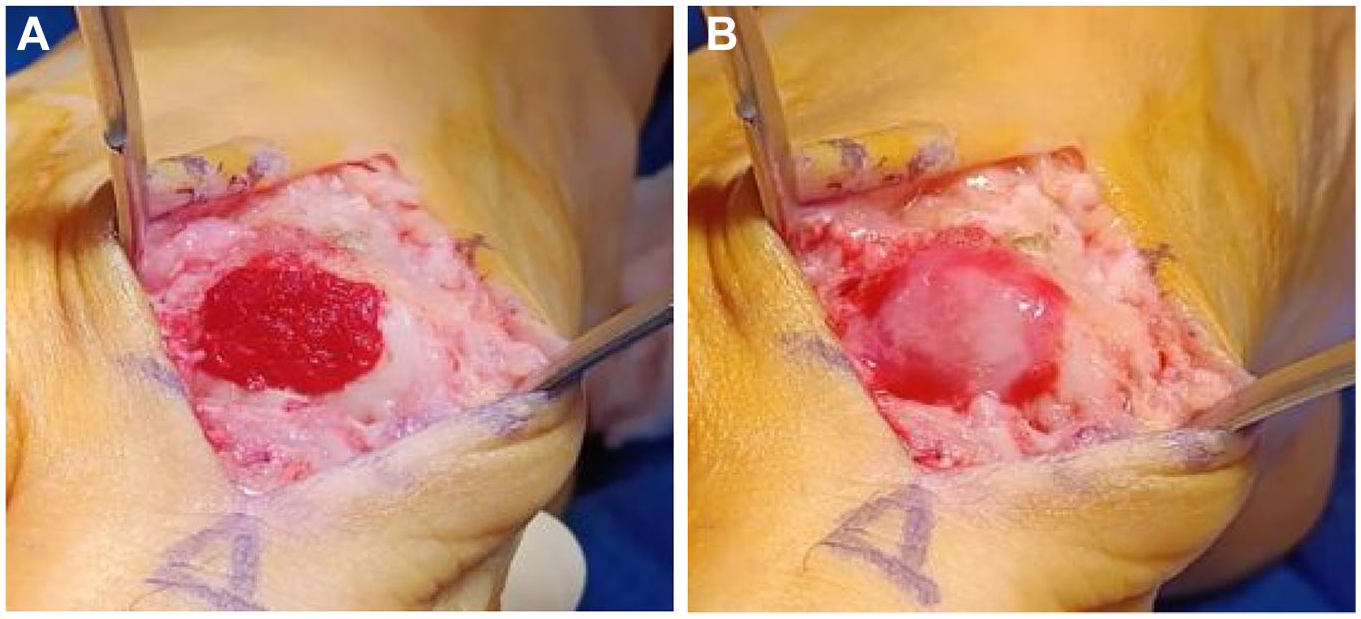
BMAC was first harvested from the ipsilateral proximal tibia prior to inflating the pneumatic tourniquet. A dorsal incision was made over the midline of the first MTPJ with meticulous dissection down to the joint. Medial and dorsal cheilectomy was performed for both the proximal phalanx and the head of the first MT to remove any bony prominence and blocks to dorsiflexion. The MTPJ was then hyperflexed to achieve complete visualization of the articular surface, where the defect was prepared using a curette until a stable rim is felt. MF was then performed using 1.2 mm Kirschner (K)-wires prior to placing the scaffolds (

DOO (
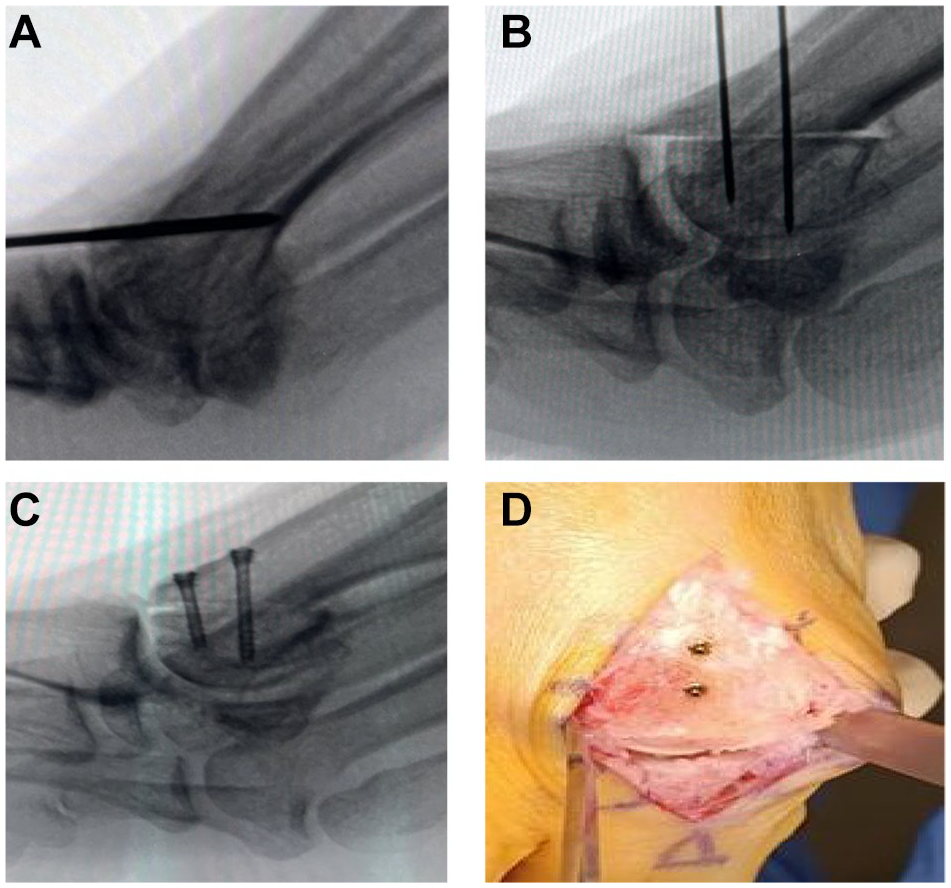
Following which, the scaffold (either Chondro-Gide or Hyalofast) was cut to size and soaked with BMAC before being placed on the first MT head to fill the articular defect. Tisseel glue, a fibrin sealant, was then applied over to secure the scaffold (
Postoperative Care
Postoperatively, a forefoot offloading shoe was used and patients were kept on heel-weight bearing (HWB) for 4-6 weeks as per the MIC technique protocol.18,19 Patients were advised against tiptoeing or excessive hallux loading during this period, though gentle range of motion (ROM) was allowed to prevent stiffness of the joint. Progressive return to activities was allowed thereafter.
Statistical Analysis
The outcomes of surgical intervention were assessed using the aforementioned questionnaires at 1 year postoperatively.
The data were collated and statistically analyzed. The preoperative and postoperative scores were compared using a paired sample Student’s t test to determine the effect of treatment. The level of significance was set at 5% (P < 0.05).
Results
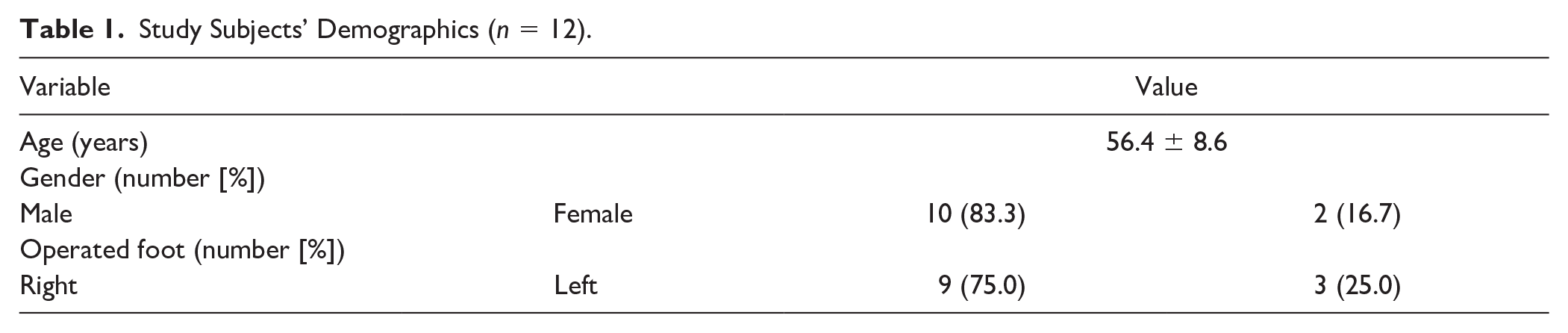
The study involved 11 consecutive patients (12 feet) with HR undergoing the COMM procedure of the first MTPJ. The mean age (using n = 12) was 56.4 years. The surgical procedures were performed on 9 right feet and 3 left feet, with 1 patient operated upon bilaterally. Patient demographics of this case series are presented in
Study Subjects’ Demographics (n = 12).
At 1-year clinical review postoperatively, there was significant improvement in all functional outcome scores recorded (
Clinical Outcomes.
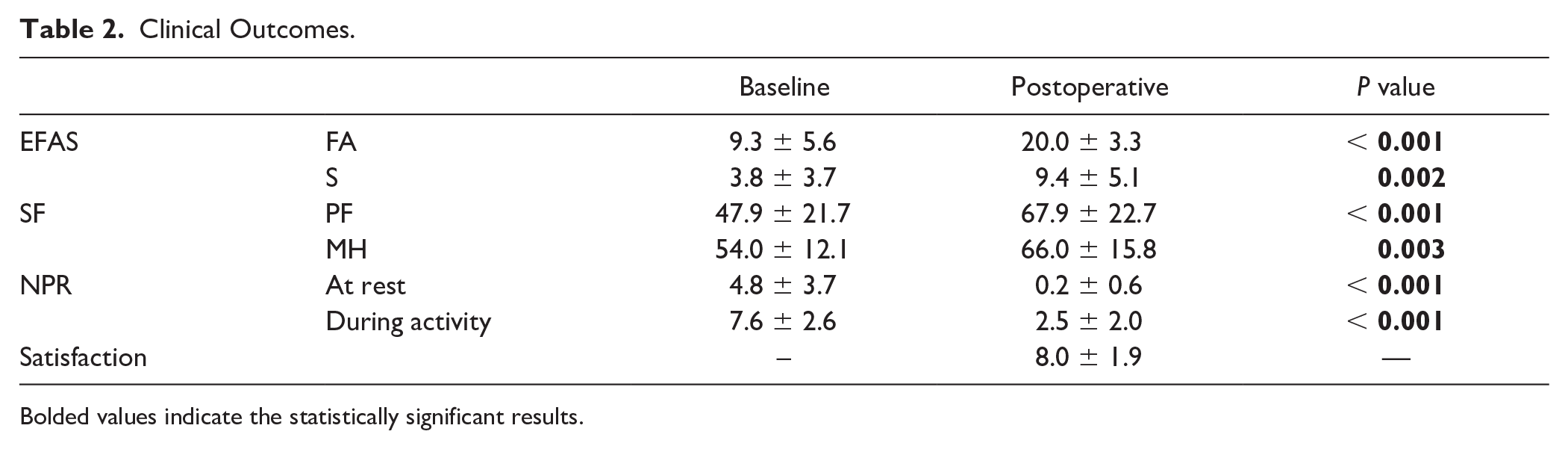
Bolded values indicate the statistically significant results.
The mean EFAS-FA and EFAS-S scores improved from 9.3 to 20.0 (P < 0.001) and 3.8 to 9.4 (P = 0.002), respectively.
The mean SF-PF and SF-MH scores increased from 47.9 to 67.9 (P < 0.001) and 54.0 to 66.0 (P = 0.003), respectively. This increase of 20.0% and 12.0% in the SF scores represented a significant improvement in HRQoL.
The mean NPR was used to compare the subjective perceptions of preoperative and postoperative pain. In this study, the mean NPR improved from 4.8 to 0.2 when at rest and 7.6 to 2.5 during activity postoperatively (P < 0.001).
Most patients considered themselves very satisfied with the surgery, with a mean postoperative satisfaction being 8.0.
One patient exhibited mild dehiscence (1 cm) of his surgical wound 3 weeks postoperatively, but no surgical intervention was required as the wound healed well with timely care.
Discussion
Most patients seek treatment for HR to reduce pain and improve their daily functional activities. To achieve those objectives, the surgical goals are focused at correcting the underlying deformity, promoting regeneration of the diseased articular cartilage, preventing recurrence and most importantly, optimizing long-term function under minimal rehabilitation requirements. 20 Surgery is recommended when conservative treatment fails, though there is no single best intervention to date. Various procedures have been established, each with varying merits and drawbacks. While metatarsophalangeal arthrodesis remains the gold standard for advanced HR, they fail to fully preserve gait biomechanics due to a reduction in ROM 9 and introduce implant-related complications. On the contrary, joint-sparing procedures like cheilectomy and DOO do not share these disadvantages and remain effective in the early stages (grades I-II). 21 The available literature describes 2 studies of MIC for HR, which yielded a marked improvement in clinical condition, including increased ROM in the first MTPJ.9,22 We hence believe combining these procedures together can synergistically optimize the mechanical conditions for joint motion, alleviate symptoms, and improve function, thereby postponing the need for more invasive procedures.
As the severity of the HR worsens, the incidence of excessive elevation in the first MT increases regardless of the underlying cause (hence the historical nomenclature of “hallux flexus”). In this regard, the learning curve for DOO is short and the technique is relatively straightforward, although it requires at least 50% of healthy cartilage on the articular surface. 23
Cheilectomy of the dorsal osteophytes has good predictability of success in alleviating pain and restoring function in patients with mild HR. 11 Coughlin and Shurnas et al. 11 examined the long-term outcomes (with an average follow-up duration of 9.6 years) following cheilectomy of the first MTPJ and observed a significant reduction in pain level, as measured by the Visual Analog Scale (VAS), from 8.0 to 1.5. A propensity-score-matched study by Lee et al. 24 showed that both DOO and cheilectomy were comparable in terms of clinical outcomes and satisfaction rates.
Nevertheless, symptoms can persist if underlying articular cartilage were damaged. This may be addressed by promoting fibrocartilage regeneration via MIC, which has proven to be a promising adjunct in improving the overall clinical outcomes of weight-bearing joints, such as the hip, 25 knee, 26 and talus. 17 Efrima et al. 17 showed in his 5-year follow-up study that symptomatic osteochondral lesions of the talus could have significant clinical improvements, with the most notable gains occurring within the first 2 years. As a single-step surgical procedure for cartilage repair, a scaffold infused with BMAC is patched over the cartilage defect to offer mechanical stabilization for the super clot and to promote chondrogenic differentiation. The evidence indicates enhanced tissue repair both radiologically and histologically after MIC.27,28 Majority of patients also expressed good satisfaction and significant reduction in pain.17,18,21,25,26 Therefore, scaffold implantations have been conjectured to provide comparable pain relief and restoration of function at any stage of HR, yet preserving the joint for further surgical procedures should the condition worsen.
Likewise, MF creates mini subchondral perforations to release stem cells and growth factors from the bone marrow into the defect, and is often combined with the above procedures to promote clot formation and cartilage repair. 29 MF has demonstrated its effectiveness in offering relief and potentially delaying degeneration when incorporated with cheilectomy. 30
Ostensibly, each intervention has its role to play in addressing a different facet of the underlying pathology in moderate to severe HR. In view of their ease of implementation in a single stage surgery, the COMM procedure, which comprises cheilectomy, DOO, MF, and MIC using scaffold implantation with BMAC can comprehensively provide superior outcomes and long-lasting relief. Cheilectomy is usually combined with DOO, for which Malerba et al. 23 postulated can optimize joint ROM. In a randomized controlled trial study by Volz et al., 12 MIC with Chondro-Gide when compared with MF alone revealed superior clinical outcomes after 5 years. In another study, Bong et al. 26 recruited 21 patients and performed MF surgery with autologous MIC for their knee chondral lesions, which noted significant improvements in clinical scores postoperatively. These likely arise from the MF technique securing the super clot within the defect, thereby decreasing the risk of dislodgement. In our study, there was a notable improvement in all indicators—NPR at rest and during activity, as well as the various PROMs. Our findings appear superior compared with the aforementioned studies in terms of postoperative pain at rest (0.2), postoperative EFAS (20, increment of 10.7), and postoperative complications (only 8.3% wound-related), though the dearth of long-term data prohibits definitive confirmation.
One patient exhibited mild dehiscence (1 cm) of his surgical wound 3 weeks postoperatively, but no surgical intervention was required as the wound healed well with timely wound care. He was the only case whereby the resting NPR, SF, and EFAS scores deteriorated globally. Notwithstanding, he was neutral in terms of overall satisfaction (scoring a 6). This wound breakdown is likely attributable to the thin skin and poor vasculature supplying the operated extremity.
This retrospective study investigated 12 cases treated with a novel technique for HR, evaluated clinically. The innovative approach in this anatomical region is noteworthy, and the results in mid- to long-term follow-up will be particularly valuable. However, this study does present some limitations. The sample size is small, and the current follow-up period presented in this paper is relatively short. In addition, the absence of a control group limits the study’s comparative value. Including a comparison with the same osteotomy without the use of MIC in subsequent studies would significantly enhance robustness. In addition, this study did not evaluate the patient’s active and passive ROM of the first MTPJ or postoperative radiographical parameters. Finally, 2 different types of scaffolds were used in this case series, and due to the sample size, this study would not be able to conclusively compare between the scaffolds implanted.
Nonetheless, as the focus of this paper is to describe our technique and outcomes using a small case series, we believe that the results from this study serve as a baseline for more research moving forward. Further studies will include longer term follow-up with a comparative group, confounding factors, such as the size of cartilage defect and type of scaffold used, and assessment including postoperative radiographs and ROM.
Conclusion
The single stage COMM procedure including cheilectomy, DOO, MF, and MIC is a promising strategy to treat moderate to severe HR by substantially alleviating pain and enhancing HRQoL as well as function. Despite being a small case series, our study has shown good early clinical outcomes and encouraging satisfaction rates among the patients. Longer-term follow-up will unveil a more comprehensive evaluation of this technique. Future studies could potentially expand the sample size and differentiate outcomes based on defect size, as well as compare against other interventions broached upon above.
Footnotes
Acknowledgements and Funding
Not applicable—no other contributors or funding sources in publication. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
Daran HUANG contributed to conceptualization, methodology, data curation, investigation, software, writing—original draft preparation, reviewing, and editing.
Wenxian PNG contributed to visualization, conceptualization, methodology, investigation, supervision.
Inderjeet Singh RIKHRAJ contributed to visualization, conceptualization, methodology, investigation, supervision.
Eric Wei Liang CHER contributed to visualization, conceptualization, methodology, investigation, supervision, writing—reviewing and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the SingHealth Centralised Institutional Review Board (REF: 2020-2381).