
Abstract
Objective
To assess the efficacy of arthroscopic debridement combined with platelet-rich plasma (PRP) therapy in treating advanced ankle osteoarthritis (OA).
Design
The data of 34 advanced ankle OA patients were retrospectively analyzed, with 17 patients undergoing arthroscopic debridement alone (No-PRP group) and 17 receiving debridement with PRP therapy (PRP group). The Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was evaluated preoperatively and at 3, 6, and 12 months postoperatively. The complications were assessed throughout the follow-up period.
Results
In the PRP group, all SAFE-Q subscales significantly improved at 6- and 12-month post-treatment compared with baseline (P < 0.05), whereas improvements in the No-PRP group were limited. For severe ankle OA patients, only the pain-related subscale of the SAFE-Q significantly improved from baseline in the No-PRP group (P < 0.05). In contrast, all SAFE-Q subscales demonstrated significant improvement at 12 months postoperatively in the PRP group (P < 0.05). The recurrence rates were 23.5% in the No-PRP group and 11.8% in the PRP group.
Conclusion
Arthroscopic debridement combined with PRP therapy for advanced ankle OA significantly improved all SAFE-Q subscales postoperatively, whereas debridement alone had limited benefits. This combination may offer an effective treatment for advanced ankle OA.
Keywords
Introduction
Patients with ankle osteoarthritis (OA) tend to be younger and more active than those with knee or hip OA and therefore are more severely affected by reduced quality of life and significant functional limitations. 1 To date, supramalleolar osteotomy, ankle arthrodesis, or total ankle arthroplasty have been required for advanced ankle OA, which is ineffective when treated conservatively. 2 However, these procedures are associated with a risk of complications, including loss of range of motion, activity limitations, and, in some cases, the need for revision surgery.3 -5 Moreover, these procedures are joint-sacrificing surgeries, making them less suitable for the treatment of relatively young and active middle-aged patients. There is a growing need for less invasive, safer, and long-lasting treatment options that, whenever possible, preserve the joint.
Platelet-rich plasma (PRP) is a safe autologous blood product that contains high levels of growth factors and cytokines that may alter biological processes involved in the pathogenesis and symptoms of OA. 6 The PRP therapy promotes chondrocyte proliferation and cartilage matrix formation and inhibits the expression of inflammatory factors.7,8 Inflammatory responses are thought to be major factors that cause and accelerate the development of OA. 9 Therefore, theoretically, PRP therapy may reduce inflammation during OA treatment, and intra-articular injection of PRP has become a treatment option for various types of joint OA, including ankle OA.10,11
Although arthroscopic debridement is minimally invasive and safe, it has been shown to be effective only in early-stage ankle OA.12,13 Therefore, it was hypothesized that arthroscopic debridement may be effective in patients with more severe ankle OA if combined with PRP therapy to suppress the inflammatory response. The purpose of this study was to compare whether combining arthroscopic debridement with PRP treatment for early to advanced OA of the ankle improves postoperative clinical outcomes.
Methods
Study Design and Patient Population
This was a retrospective comparative study using chart review for the retrieval of data from individual patients. A total of 38 patients treated with arthroscopic debridement for ankle OA between November 2017 and November 2023 by the senior author were included. The diagnosis of OA was confirmed by clinical history and imaging including radiographs and computed tomography (CT) scans, as previously described. 14 The Tanaka-Takakura classification was defined as follows: Stage I: early sclerosis and osteophyte formation, no joint narrowing; Stage II: medial joint space narrowing, no subchondral bone contact; Stage IIIa: medial joint space obliteration, subchondral bone contact; Stage IIIb: articular space obliteration over the talar domus, subchondral bone contact; Stage IV: joint space obliteration with complete bone contact. The inclusion criteria were (1) advanced ankle OA patients (Tanaka-Takakura classification of Stage II or greater), (2) follow-up for at least 12 months, (3) unresponsive to conservative treatment, and (4) presence of osteophytes with symptomatic impingement. Patients who underwent other additional surgeries and patients who underwent simultaneous bilateral surgeries were excluded.
A total of 34 patients (19 males and 15 females) fulfilled the inclusion criteria (
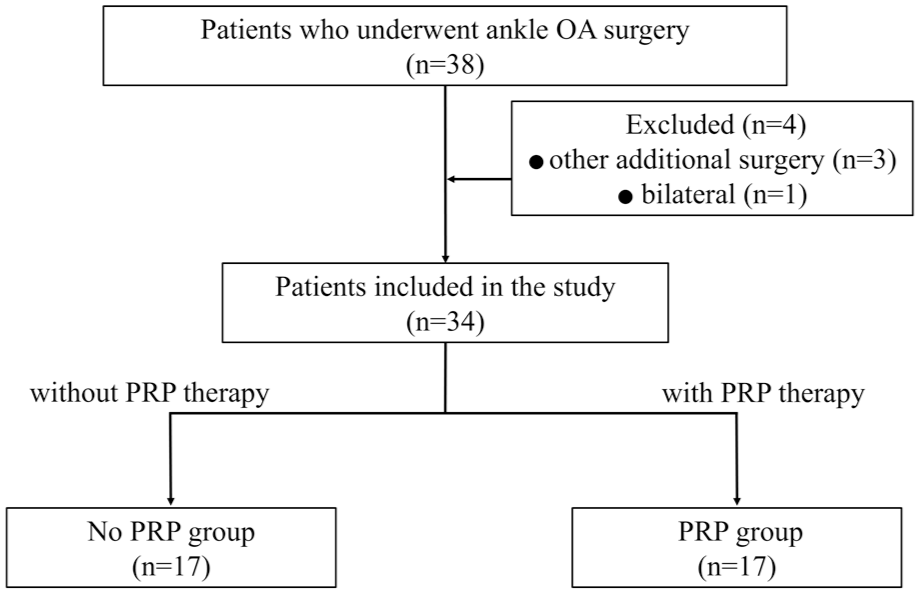
Flow diagram of the study. OA = osteoarthritis; PRP = platelet-rich plasma.
Surgical Technique
The senior surgeon performed all surgical procedures, under general anesthesia, in the supine position, with manual or temporary body traction of the ankle. Standard anteromedial and anterolateral portals were established, and a 2.7-mm, 30° arthroscope was utilized. To enhance dorsiflexion, meticulous debridement of bony and soft tissue impingements was performed in all patients to alleviate anterior impingement. Furthermore, pathological findings such as scar tissue, inflamed synovium, unstable cartilage, loose bodies, or intra-articular adhesions were thoroughly excised to optimize the condition of the ankle joint.
All patients were placed in an elastic bandage for 2 days after surgery. From the day after surgery, ankle range of motion (ROM) exercises were started, and walking was permitted with a patellar tendon support (PTB) brace depending on the pain level. Full weight bearing without the PTB brace was allowed according to pain control from 3 weeks after surgery. Balance and proprioception exercises were introduced at 4 weeks postoperatively. All the rehabilitation procedures were supervised by a licensed and experienced physiotherapist. All patients were able to walk without assistance from a cane or walker for at least 8 weeks after surgery.
Platelet-Rich Plasma Preparation and Applications
The preparation of PRP was expertly performed using the Arthrex ACP double-syringe system (Arthrex, Naples, Florida), strictly following the manufacturer’s protocol. This PRP was leukocyte-poor platelet-rich plasma (LP-PRP), as previously reported, with a low concentration of leukocytes and a 2- to 3-fold higher concentration of platelets. 15 The process began with the collection of blood from the patient via a double syringe with the kit. The blood was then subjected to controlled centrifugation at 1,500 rpm for 5 minutes, and its components were separated with precision. The syringe was kept in an upright position to avoid mixing the plasma and red blood cells. The double-syringe system facilitated the transfer of 4 to 7 ml of ACP into the small inner syringe, making it ready for use. Since the PRP was intended for use within 30 minutes of preparation, no acid citrate dextrose solution A was required to prime the system. PRP was administered intra-articularly at 4 ml via a needle inserted into the joint by direct vision after the arthroscopic procedure and wound closure.
Data Collection
Data on patient characteristics and clinical information including age, sex, body mass index (BMI), and follow-up duration were collected from medical records. Recurrence was defined as the progression of Tanaka-Takakura classification or subjective pain comparable to that observed before surgery. Clinical outcomes were evaluated preoperatively and 3 months, 6 months, and 12 months after surgery using the Self-Administered Foot Evaluation Questionnaire (SAFE-Q) scores. 16 These evaluations were not performed face-to-face but rather used a consultation system.
Statistical Analysis
Owing to the small sample size, the Mann-Whitney U test was chosen to compare 2 variables, including the baseline values for age, BMI, follow-up duration, and details of the SAFE-Q subscale scores at 3 months, 6 months, and 12 months postoperatively. Comparisons between groups for sex and recurrence rates were made using chi-square tests for categorical variables. The changes in the scores of each item of the SAFE-Q were compared via the 1-way analysis of variance followed by Dunnett’s test, with the preoperative scores serving as the control group. A P-value of < 0.05 indicated statistical significance. All the numerical data were reported as the means ± standard deviations and were analyzed using the Prism software (GraphPad Prism for Windows, version 9.0; San Diego, California).
Results
Demographic Data: Entire Cohort
The demographic data, including age, BMI, follow-up duration, and recurrence rate, showed no significant differences at baseline between the No-PRP and PRP groups (
Preoperative Characteristics of all Advanced Ankle OA Patients in the 2 Groups.
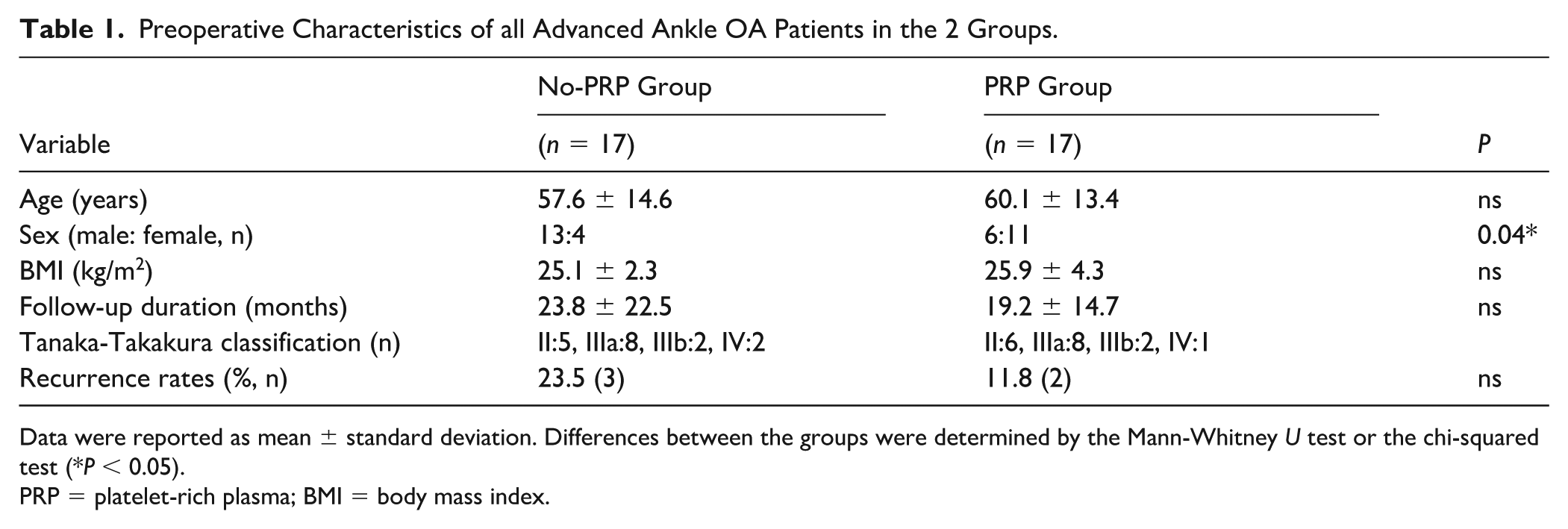
Data were reported as mean ± standard deviation. Differences between the groups were determined by the Mann-Whitney U test or the chi-squared test (*P < 0.05).
PRP = platelet-rich plasma; BMI = body mass index.
Clinical and Functional Outcomes: Entire Cohort
The preoperative SAFE-Q scores revealed no significant differences between the 2 groups in any of the 5 subscale scores (
Details of the SAFE-Q Subscale Scores in all Advanced Ankle OA Patients in the 2 Groups.
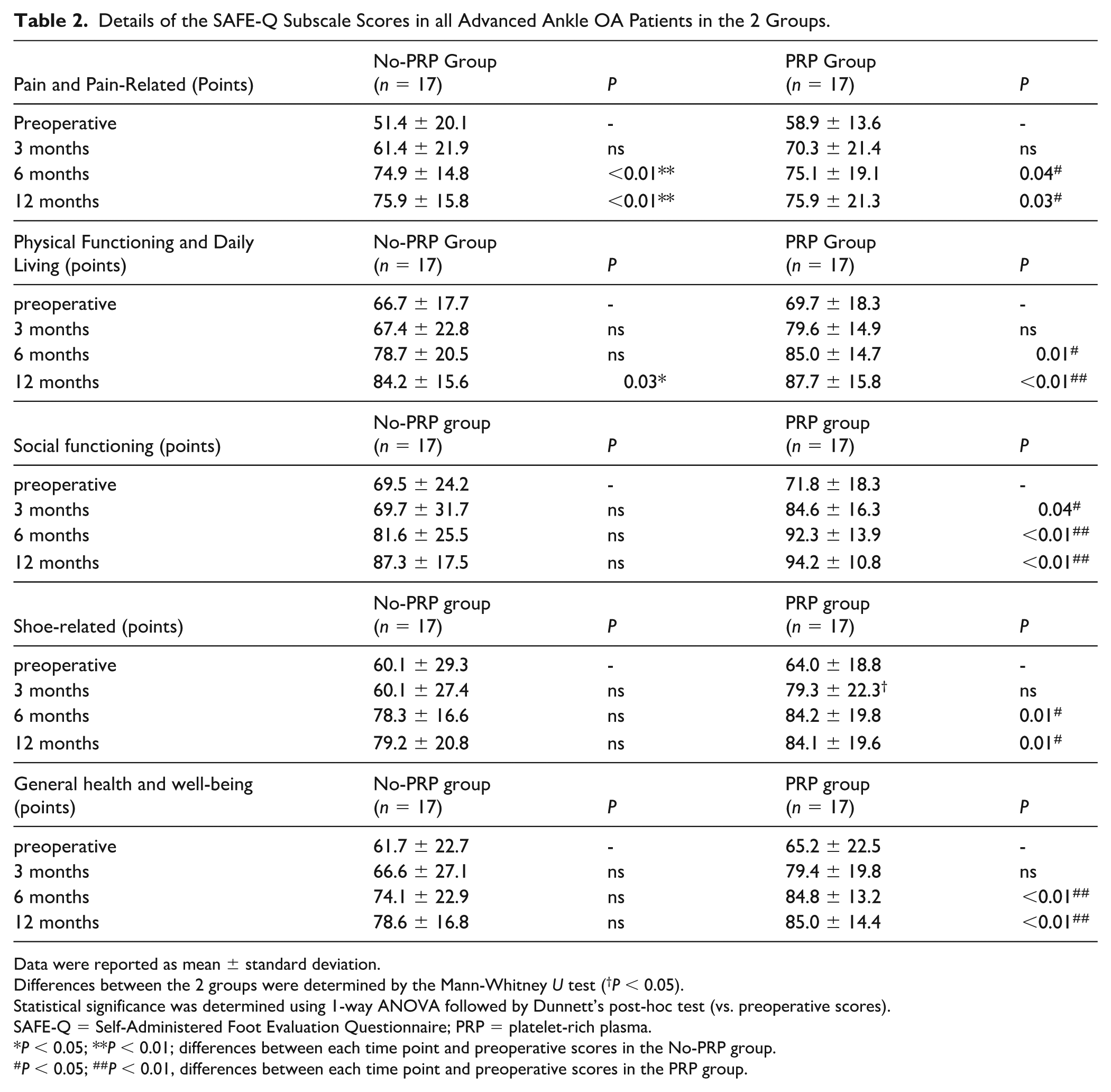
Data were reported as mean ± standard deviation.
Differences between the 2 groups were determined by the Mann-Whitney U test (†P < 0.05).
Statistical significance was determined using 1-way ANOVA followed by Dunnett’s post-hoc test (vs. preoperative scores).
SAFE-Q = Self-Administered Foot Evaluation Questionnaire; PRP = platelet-rich plasma.
P < 0.05; **P < 0.01; differences between each time point and preoperative scores in the No-PRP group.
P < 0.05; ##P < 0.01, differences between each time point and preoperative scores in the PRP group.
Demographic Data: Patients With Tanaka-Takakura Classification of Stage IIIa or Greater
A comparative analysis focusing on more advanced ankle OA patients with Tanaka-Takakura classification of Stage IIIa or greater revealed no statistically significant differences at baseline in age, sex, BMI, follow-up duration, or recurrence rates between the 2 groups (
Preoperative Characteristics of Tanaka-Takakura Classification Stage IIIa or Greater Ankle OA Patients in the 2 Groups.
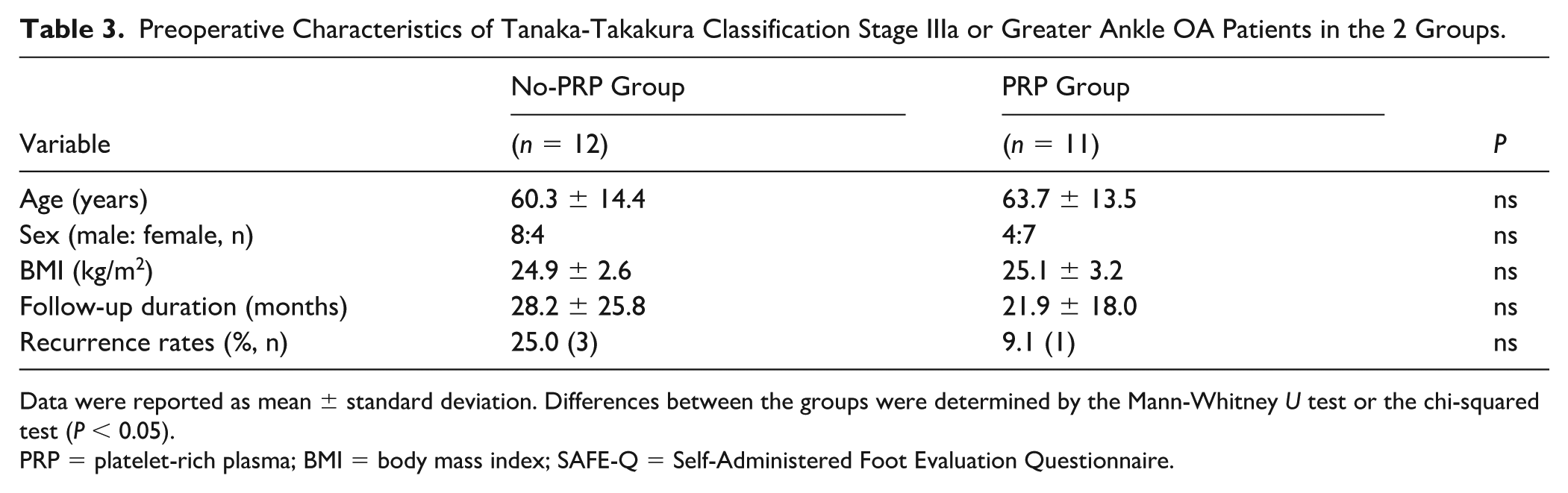
Data were reported as mean ± standard deviation. Differences between the groups were determined by the Mann-Whitney U test or the chi-squared test (P < 0.05).
PRP = platelet-rich plasma; BMI = body mass index; SAFE-Q = Self-Administered Foot Evaluation Questionnaire.
Clinical and Functional Outcomes: Patients With Tanaka-Takakura Classification of Stage IIIa or Greater
Patients with more advanced ankle OA (Stage IIIa or greater) were analyzed. The preoperative SAFE-Q scores revealed no statistically significant differences between the groups across any of the subscales (
Details of the SAFE-Q Subscale Scores in Tanaka-Takakura Classification Stage IIIa or Greater Ankle OA Patients in the 2 Groups.
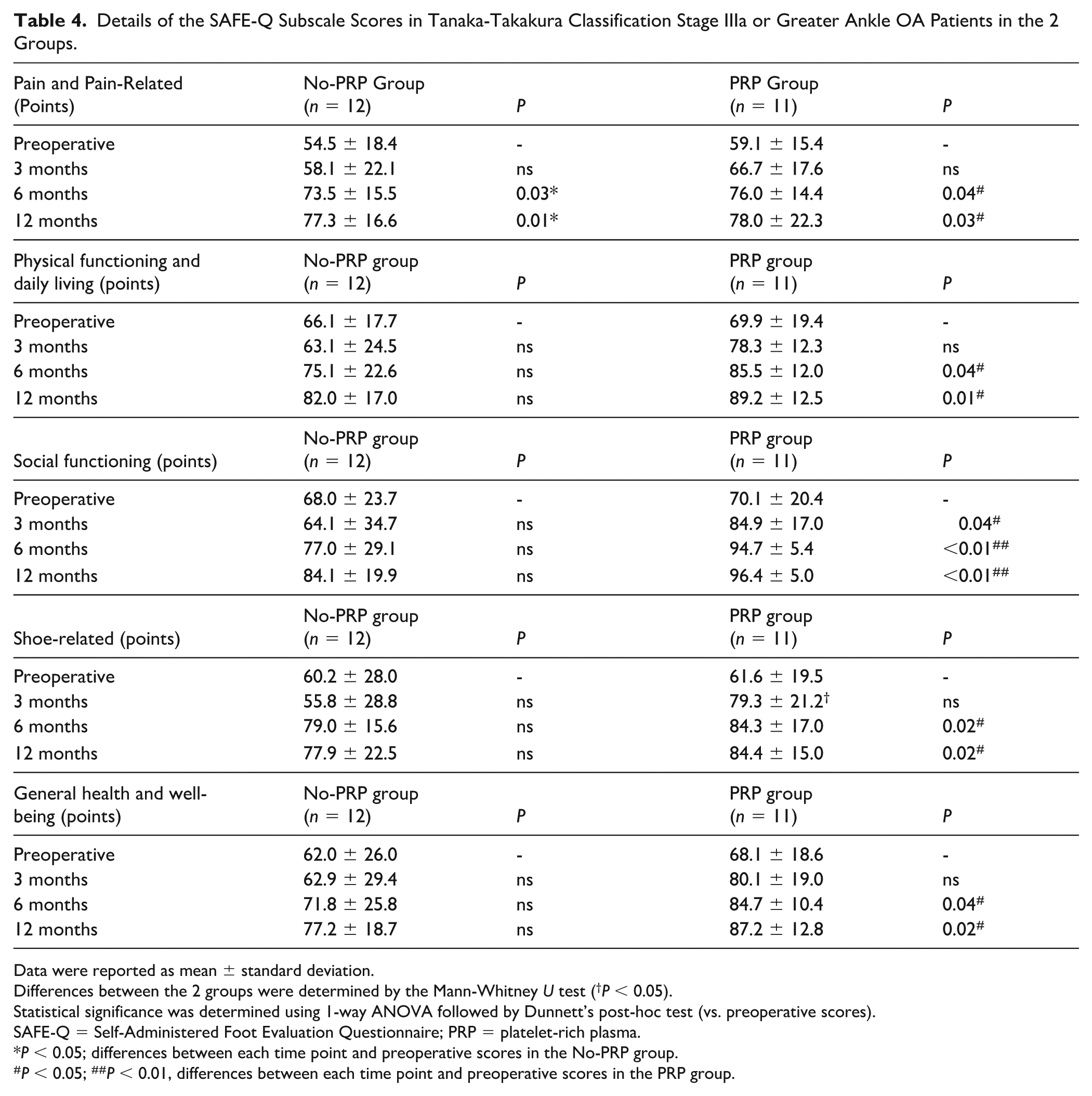
Data were reported as mean ± standard deviation.
Differences between the 2 groups were determined by the Mann-Whitney U test (†P < 0.05).
Statistical significance was determined using 1-way ANOVA followed by Dunnett’s post-hoc test (vs. preoperative scores).
SAFE-Q = Self-Administered Foot Evaluation Questionnaire; PRP = platelet-rich plasma.
P < 0.05; differences between each time point and preoperative scores in the No-PRP group.
P < 0.05; ##P < 0.01, differences between each time point and preoperative scores in the PRP group.
Complications and Recurrence
No complications other than the progression of OA or recurrence of pain were observed during the follow-up period. Regarding recurrent patients, in the No-PRP group, progression of OA according to the Tanaka-Takakura classification was observed in 4 patients on radiographs at the final follow-up (including 1 patient preoperatively classified as Stage II), with 2 patients undergoing reoperation. These reoperations consisted of arthroscopic debridement at 63 months postoperatively and ankle arthrodesis at 14 months postoperatively. Conversely, in the PRP group, OA progression according to the Tanaka-Takakura classification was noted in 1 patient (Stage II preoperatively), and 1 patient experienced recurrent pain, necessitating reoperation. These 2 reoperations consisted of arthroscopic debridement performed at 63 and 49 months postoperatively, respectively.
Discussion
To the best of our knowledge, this study is the first to demonstrate that arthroscopic debridement, which was previously recommended primarily for patients with early-stage OA, may be effective for patients with more advanced OA (Stage IIIa or greater) through the combined use of PRP therapy. Although this was a small retrospective cohort study, this study revealed that arthroscopic debridement, when combined with PRP therapy, improved pain relief, functional outcomes, and quality of daily life from the early postoperative period in patients with ankle OA. Furthermore, while arthroscopic debridement alone provides pain relief in patients with ankle OA (particularly those with more advanced OA), it does not significantly improve functional outcomes or the quality of daily life.
Arthroscopic debridement of the ankle joint reportedly provides good clinical outcomes and functional improvement in patients with ankle OA even 5 years after surgery; however, all of these studies have only addressed the impingement symptoms of early-stage OA.12,17,18 Glazebrook et al. 19 reported a tendency for the outcomes of arthroscopic debridement to worsen as the severity of ankle OA progresses. Moreover, 28% to 66% of patients with advanced OA who underwent debridement required some form of reoperation within 5 years.20,21 This study also demonstrated that while arthroscopic debridement alone provided pain relief, particularly in patients with more advanced OA (Stage IIIa or greater), it failed to achieve favorable outcomes in subjective evaluations such as functional improvement, social activity, and general health. In addition, 23.5% of patients with advanced OA experienced disease recurrence.
The PRP treatment is known to suppress cytokines that induce inflammation, such as interleukin (IL)-17 and tumor necrosis factor-alpha (TNFα). 22 Moreover, PRP has the potential to reduce and degrade the concentration of pro-inflammatory cytokines by inhibiting the activation of nuclear factor-kappa B induced by IL-1. 7 This suggests the possibility of mitigating postoperative inflammatory responses and enhancing analgesic effects. However, in this study, no statistically significant differences were postoperatively observed in pain and pain-related scores between the 2 groups.
Although PRP treatment has previously been reported to improve OA symptoms regardless of the severity of cartilage damage,23,24 its overall effectiveness remains a subject of debate. However, a previous report suggested that PRP therapy may be more effective in cases involving direct bone stimulation, such as microfracturing procedures for osteochondral lesions of the talus. 25 PRP promotes tissue repair by releasing a wide array of bioactive substances, including growth factors, cytokines, lysosomal components, and adhesive proteins derived from the concentrated platelets. These components initiate the hemostatic cascade, facilitate the synthesis of new connective tissue, and promote the reparative process. 26 Therefore, the addition of PRP to bone-stimulating procedures such as debridement may have a synergistic effect by enhancing the tissue repair capacity. Debridement combined with PRP has been reported to provide better pain relief and improvement of joint function than arthroscopic debridement for the knee joint. 27 Although most of these reports focused on the knee joint, this study also revealed that the combination of PRP improved not only the pain relief effect but also all items on the SAFE-Q, including function, social activity, and general health.
However, a certain period is required before the effect can be expected. Paget et al. 28 reported that in patients with OA of the ankle, intra-articular PRP injections did not significantly improve ankle symptoms and function over a 26-week period compared with placebo injections. In contrast, Ding et al. 29 reported that although injections of LP-PRP for patients with ankle OA did not show significant differences between the American Orthopaedic Foot and Ankle Society (AOFAS) score and visual analog scale (VAS) in the short term, a minimal clinically important difference was observed at ≥ 6 months. In this study, no effect of PRP was observed 3 months after surgery, but the effect was observed 6 months after surgery, and the effect was sustained even 12 months after surgery. However, the effects of PRP therapy are not permanent. PRP treatment for ankle OA has been reported to maintain its efficacy for a period of 6 to 18 months.10,30,31 Studies combining PRP therapy with treatments for the osteochondral lesions of the talus have demonstrated favorable outcomes for up to 2 years; however, the clinical performance tends to decline thereafter. 32 To the best of our knowledge, the long-term efficacy of combining ankle OA surgery with PRP therapy remains unclear. In this study, all the cases of relapses occurred more than 2 years after surgery, and there is room for debate regarding the effectiveness of PRP as an adjuvant therapy for ankle OA surgery in the long term.
This study has several limitations that must be considered. First, the sample size was small, which likely contributed to the lack of statistically significant differences in many outcomes, potentially resulting from a type II error. As reflected in the standard deviations, patient responses to treatment varied considerably. Larger prospective cohort studies with longer follow-up periods are necessary to elucidate the role of PRP therapy in arthroscopic debridement for ankle OA. Second, the baseline sex distribution was imbalanced. However, the progression of ankle OA is not related to sex. 33 Third, only LP-PRP was used in this study. Previous reports indicate that leukocyte-rich platelet-rich plasma (LR-PRP) results in elevated expression of IL-1Ra, IL-4, and IL-8 but is also associated with increased matrix metalloproteinase-9 (MMP-9) expression, suggesting enhanced anti-inflammatory effects coupled with heightened chondrotoxicity.34,35 While LP-PRP may be more advantageous for long-term cartilage preservation, the optimal leukocyte concentration for PRP therapy in ankle OA remains undetermined. Finally, preoperative and postoperative radiological evaluations were conducted via conventional weightbearing radiographs. Employing advanced imaging modalities such as magnetic resonance imaging (MRI), CT, or weightbearing CT could provide a more detailed understanding of the pathogenesis of OA progression in specific patients.
Conclusion
Compared with preoperative scores, the combination of arthroscopic debridement and PRP therapy for advanced OA of the ankle demonstrated significantly better outcomes across all SAFE-Q domains at 12 months postoperatively. In contrast, arthroscopic debridement alone showed statistically significant improvement only in the pain and pain-related scores, with no statistically significant enhancements observed in the other domains. Furthermore, the recurrence rate for advanced OA of the ankle was 23.5% with arthroscopic debridement alone, whereas the recurrence rate was 11.8% in the group receiving PRP therapy. Based on the data from this selected sample, the combination of arthroscopic debridement and PRP therapy may be an effective treatment; however, future blinded randomized controlled trials comparing PRP to placebo are needed to substantiate these findings.
Footnotes
Ethical Considerations
All patients provided written informed consent to participate in this study, which was approved by the Ethics Committee of the Japan Medical Association (approval number: R1-6).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.