
Abstract
Objective
This study aimed to evaluate the clinical and biological outcomes of a one-step regenerative treatment using bone marrow aspirate concentrate (BMAC) on a hyaluronic acid scaffold combined with intraarticular platelet-rich plasma (PRP) for treatment of full-thickness cartilage lesions in the knee.
Design/Methods
A total of 165 patients (mean age 26.4 years) with full thickness cartilage defects were included in the study. In a single-step procedure, bone marrow was aspirated from the iliac crest and centrifuged to obtain BMAC concentrate. PRP was prepared from whole blood. The BMAC concentrate was seeded onto a hyaluronic acid scaffold and implanted into the debrided cartilage defect and PRP was added intraarticularly. Clinical outcomes were assessed using the Knee Injury and Osteoarthritis Outcome Score (KOOS) and a semiquantitative grading scale (Excellent, Good, Fair) at one-year follow-up. All patients underwent MRI preoperatively and at one year follow-up, with cartilage repair evaluated using the MOCART-2.0 scoring system.
Results
Significant improvements were observed in all KOOS subscales at one year. Semiquantitative grading revealed excellent outcomes in 50% of patients, good in 28%, and poor in 22%. MRI analysis showed an average MOCART-2.0 score of 71, with 36% of patients achieving excellent cartilage repair (MOCART 2.0 >80).
Conclusion
The combined use of BMAC on a hyaluronic acid scaffold and intraarticular PRP resulted in improved subjective clinical outcomes and demonstrated favourable biological cartilage healing responses at one year postoperatively. This one-step cartilage repair technique appears to be a clinically valid option for treatment of full-thickness cartilage lesions in the knee.
Introduction
Autologous chondrocyte implantation (ACI) has long been regarded as the gold standard for advanced cartilage repair, offering the most extensively documented clinical outcomes and demonstrating superiority over bone-marrow-derived cartilage repair techniques.1 -4 However, the implementation of more stringent regulatory requirements for cell-based therapies in Europe has markedly reduced the availability of ACI, prompting the adoption of alternative cartilage repair strategies.
Single-stage, cell-based procedures have emerged as an appealing option due to their potential cost-effectiveness and the reduced surgical burden of requiring only one surgical intervention.5 -7 One-step repair using multipotent cells derived from Bone Marrow Aspirate Concentrate (BMAC), combined with biological scaffolds, has demonstrated short- to mid-term clinical outcomes comparable to those of ACI, including in the management of large chondral defects and lesions with osteochondral involvement. 8
Recent reports suggest that BMAC-based treatment using a hyaluronic acid–based scaffold seeded with BMAC (HA-BMAC) can yield promising long-term results, with small case series showing sustained clinical improvement for up to 14 years.9 -13
One systematic review on the HA-BMAC based cartilage repair concluded that the scientific evidence for the clinical benefit of the technique still is limited and that larger and better-quality clinical studies are needed on the topic. 14 There remains therefore a critical need for studies involving larger patient cohorts to provide more generalizable data on both the clinical effectiveness and the biological cartilage repair response achieved with HA-BMAC-based therapies.
The present study aimed to evaluate clinical outcomes and biological repair responses in a large prospective cohort treated with a one-step cartilage repair procedure combining HA-BMAC with Platelet-Rich Plasma (PRP) for full-thickness cartilage lesions of the knee.
Material and Methods
Study Design
This study was designed as a single-center retrospective case series. Consecutive patients who underwent cartilage repair using a HA-BMAC technique between 2013 and 2024 were identified from a prospectively maintained institutional database capturing validated patient-reported outcomes and routine postoperative MRI assessments. Demographic, surgical, and imaging data were extracted from electronic medical records. Ethical approval was obtained from the regional ethics committee (ID: 1-45-70-118-24).
Patient Selection
Surgical Technique
The operative extremity and ipsilateral iliac crest were prepared in a sterile fashion. Initial diagnostic arthroscopy confirmed eligibility for HA-BMAC-based cartilage repair and allowed treatment of associated pathology.
A 20-mL bone marrow aspirate was harvested from the ipsilateral iliac crest using a trocar-based aspiration system, then processed in a commercially available centrifugation device (BioCUE® Bone Marrow Aspirate Concentration System; Biomet), yielding a 2-4 mL nucleated cell–rich BMAC.
A mini-arthrotomy was performed to expose full-thickness chondral lesions. Unstable cartilage was removed, and lesion borders were shaped to stable vertical margins. The defect base was uniformly debrided to remove the calcified cartilage layer without breaching the subchondral plate.
A hyaluronic acid–based fibermesh scaffold (Hyalofast; Anika Therapeutics) was trimmed to defect size, saturated with the BMAC, and allowed to soak for 5-10 minutes. The BMAC-loaded scaffold now a HA-BMAC graft was fixed to the defect bed using fibrin glue (Tisseel; Baxter). After a 5-minute polymerization period, the knee was cycled through full flexion–extension under direct visualization to confirm construct stability (
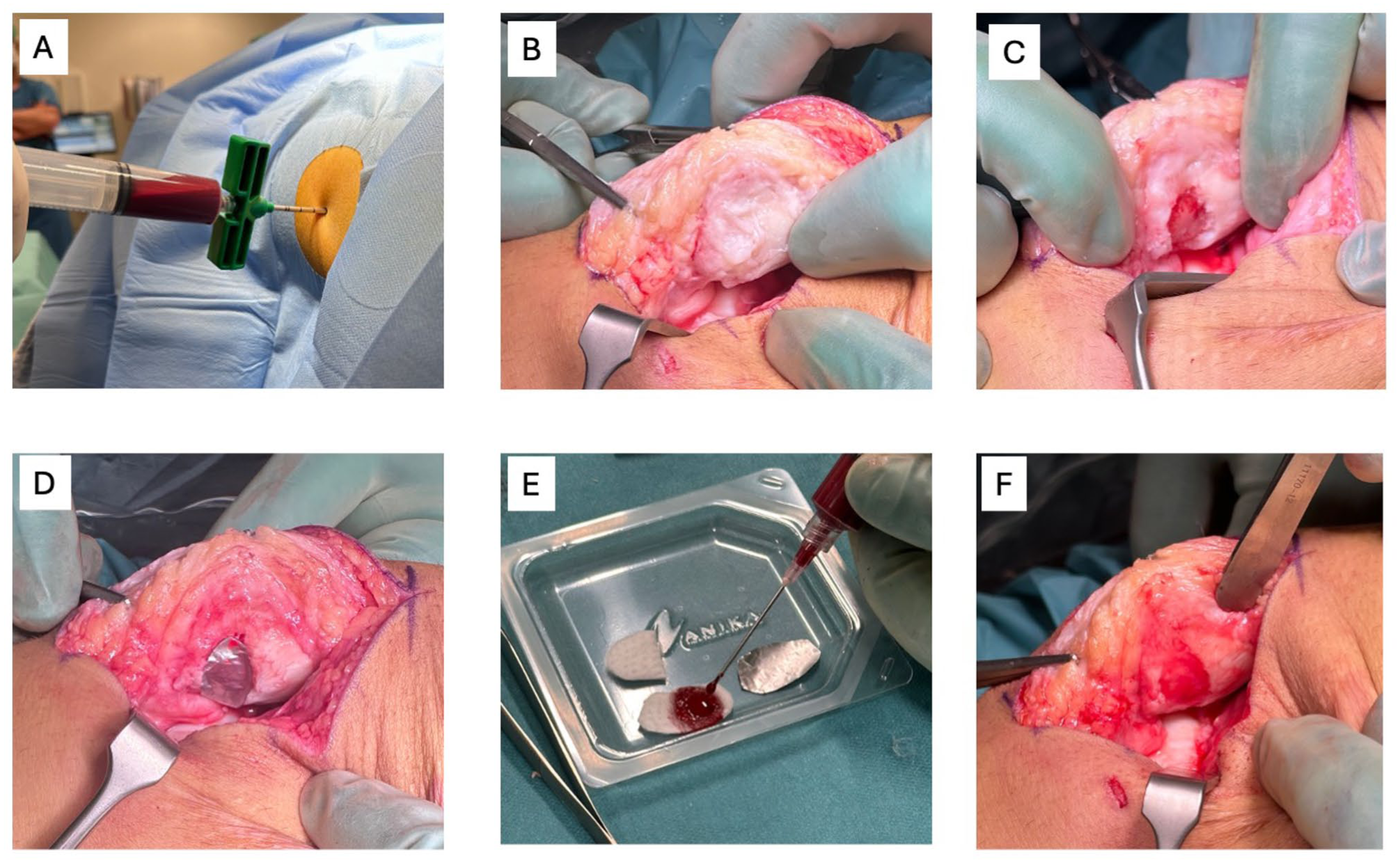
HA-BMAC Surgical technique: Bone marrow aspirate extracted from the iliac crest, which is then processed in a commercially available system to isolate bone marrow aspirate concentrate. (A) Bone marrow aspiration from iliac crest (B) Retropatellar cartilage lesion. (C) Debrided patella cartilage lesion. (D) Aluminium foil templating of the cartilage defect. (E) Bone marrow aspirate concentrate added to the hyaluronic acid–based scaffold to form (HA-BMAC) implant. (F) HA-BMAC implant inserted and fibrin glue secured in the chondral defect of the patella.
For PRP injection, 20 mL of whole blood bone was taken from a peripheral vein. The blood was then processed in a commercially available centrifugation device (GPS® III Platelet Concentration System; Biomet), yielding 2-3 mL of PRP. The PRP was injected intraarticulary after capsular closure for initial growth factor stimulation of the HA-BMAC graft.
Postoperative Rehabilitation
A standardized rehabilitation protocol was used for all patients. A hinged brace limited range of motion (ROM) to 0°-20° for the first 2 weeks.
Quadriceps strengthening began at week 6, and stationary cycling at week 8. All patients underwent physiotherapist-supervised rehabilitation for 12 weeks.
Clinical Outcome Measures
Patient-reported outcomes were collected preoperatively and at 12 months using the KOOS (Knee Injury Outcome Score) 15 and Tegner activity score. 16 The completeness of KOOS scores were 30%.
An unvalidated semiquantitative global clinical outcome assessment was also recorded at 12 months and categorized as:
(A) Symptom-free knee with high functional level; (Excellent)
(B) Significant symptom improvement with occasional activity-related pain or swelling; (Good)
(C) Limited improvement with persistent symptoms restricting function. (Poor)
Postoperative complications and reoperations were documented based on patient files in the which were reviewed in 2025 giving variable follow-up for reoperations of 1-10 years in the cohort.
MRI Evaluation
Preoperative 3-T MRI scans were assessed using the AMADEUS (Area Measurement And Depth and Underlying Structures) scoring system to quantify chondral and osteochondral defect severity. 17 Intraoperative cartilage injury severity grading was performed according to the ICRS (International Cartilage Repair Society) grading system. 18 Hyaline cartilage or repair tissue were analyzed using the MOCART 2.0 (magnetic resonance observation of cartilage repair tissue, 0 = worst, 100 = best) score in all patients at 12 months postoperatively. 19 The completeness of MRI was 96%.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation. Categorical variables were reported as median and 25%. AMADEUS and MOCART 2.0 scores were presented as mean ± standard deviation. Changes in KOOS subscores from baseline to follow-up were analyzed using two-tailed paired t-tests. Comparison of MOCART 2.0 scores between anatomical locations were analyzed using two-tailed paired t-tests. Comparison of high-level MOCART 2.0 scores > 80 were analyzed using Chi-Square test. between anatomical locations were analyzed using two-tailed paired t-tests. A P-value <0.05 was considered statistically significant. Analyses were performed using STATA version 18 (StataCorp, College Station, TX).
Results
A total of 165 consecutive patients treated with HA-BMAC-based cartilage repair were included. Patient demographics, previous surgeries, and concomitant procedures are summarized in
Patient Characteristics, Previous Surgeries and Concomitant Surgical Procedures.
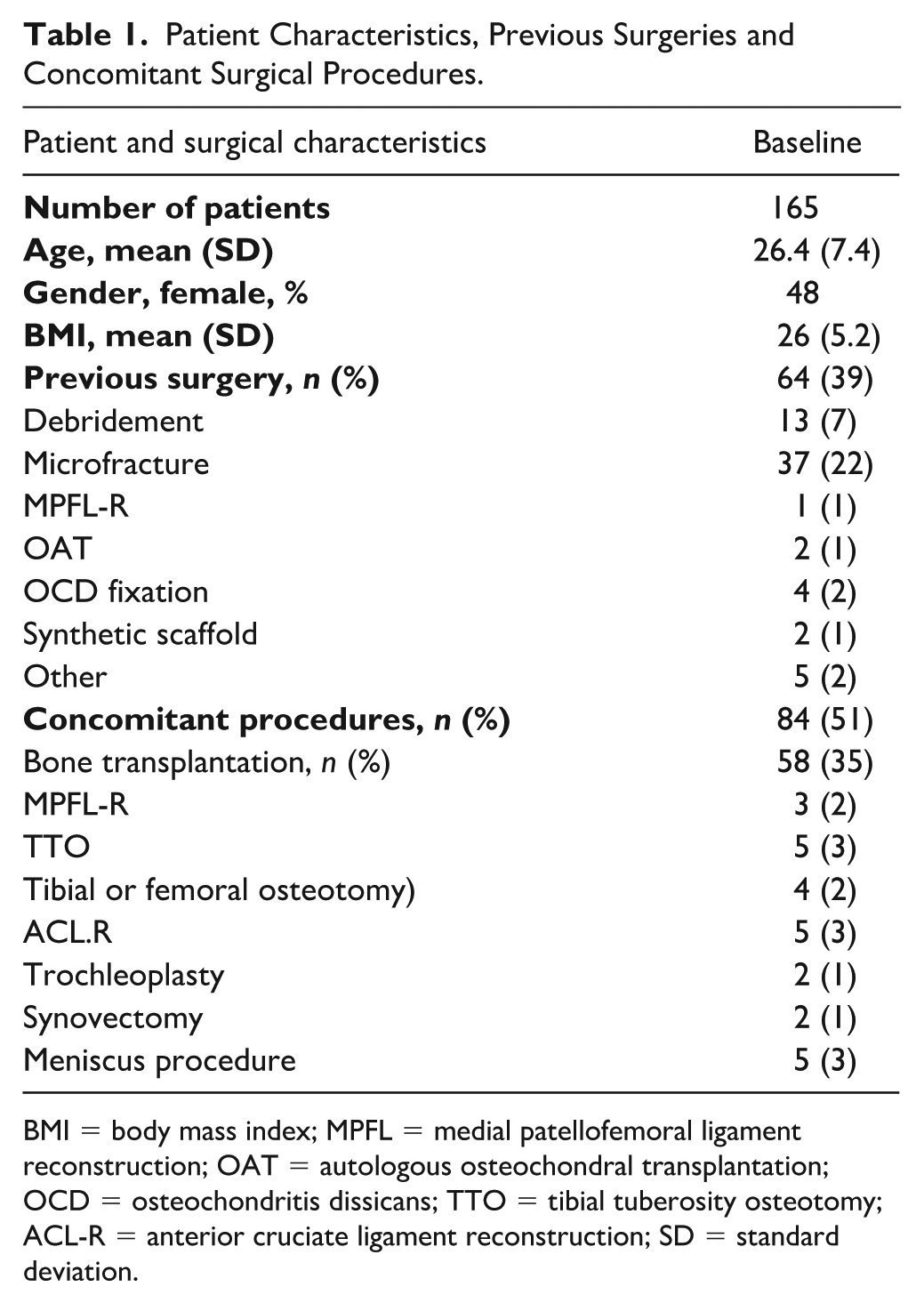
BMI = body mass index; MPFL = medial patellofemoral ligament reconstruction; OAT = autologous osteochondral transplantation; OCD = osteochondritis dissicans; TTO = tibial tuberosity osteotomy; ACL-R = anterior cruciate ligament reconstruction; SD = standard deviation.
Cartilage Lesion characteristics.
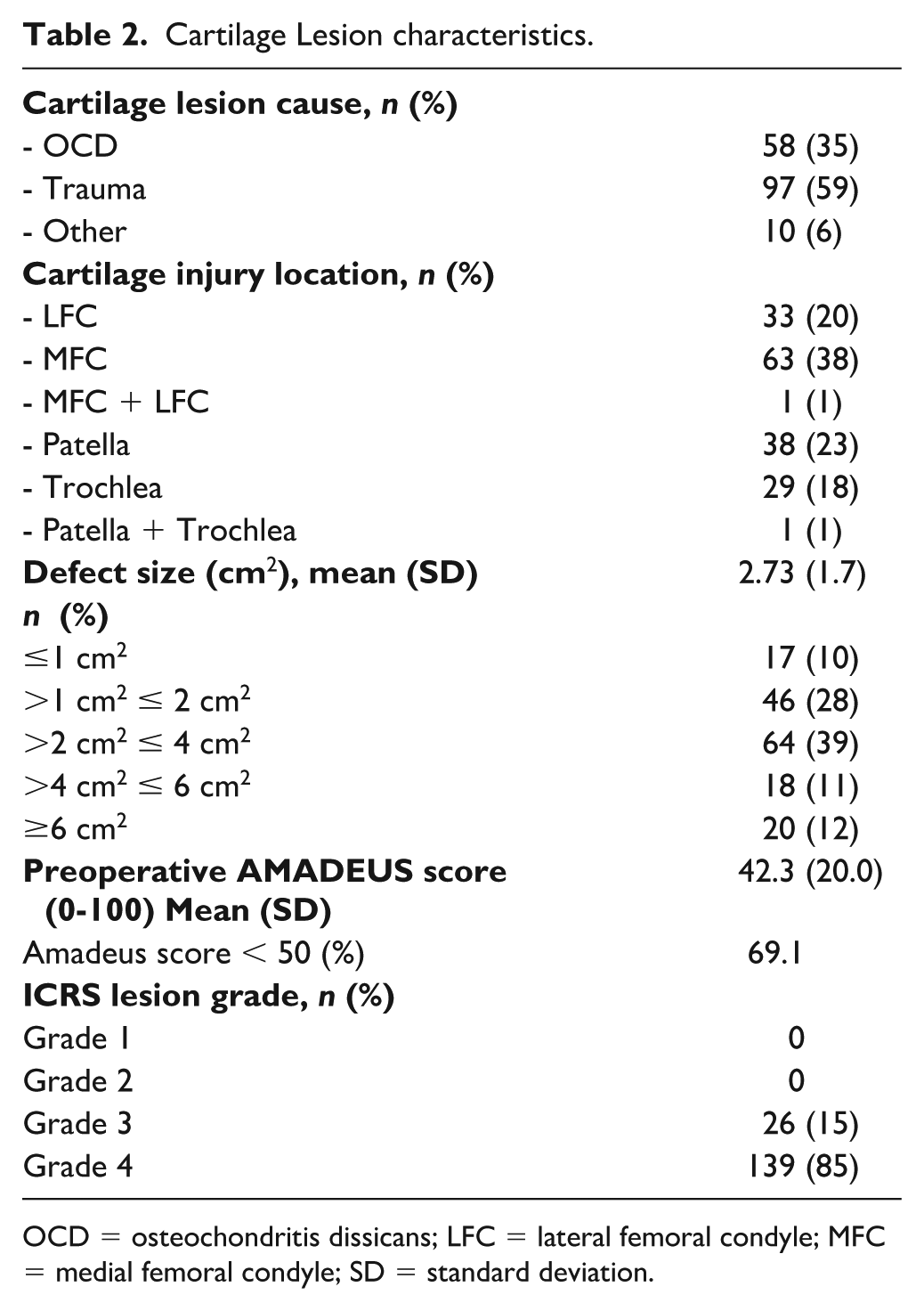
OCD = osteochondritis dissicans; LFC = lateral femoral condyle; MFC = medial femoral condyle; SD = standard deviation.
Patient-Reported Outcomes
Significant improvements were observed across all KOOS subscales from baseline to 12-month follow-up, with median score increases ranging from 21 to 30 points—exceeding the established minimal clinically important difference for each subscale.
20
The greatest improvements were seen in KOOS–Sport (+30 points) and KOOS–Symptoms (+27 points), indicating marked enhancement in symptom burden and sport-related functional capacity. Detailed overall KOOS results are shown in
KOOS Outcomes at Baseline and 1-Year Follow-Up.
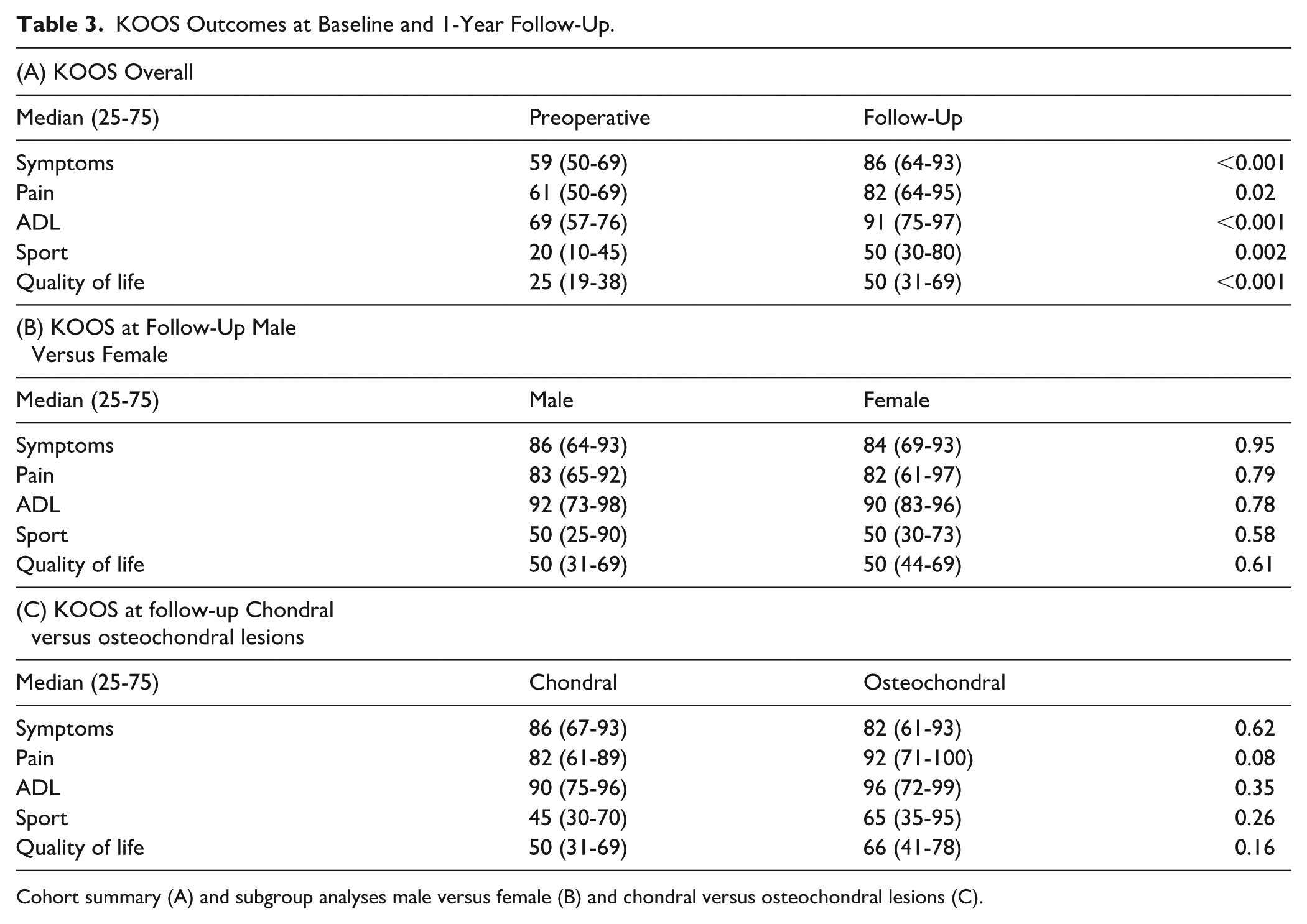
Cohort summary (A) and subgroup analyses male versus female (B) and chondral versus osteochondral lesions (C).
Subgroup comparisons revealed no statistically significant differences between males and females (
Based on the semiquantitative global clinical outcome assessment at 12 months,
Radiological Outcomes
Preoperative lesion severity assessed by the AMADEUS score showed a mean score of 43.8, with 69% of lesions rated <50, indicating substantial baseline defect severity.
The mean MOCART 2.0 score at 12-month follow-up was 70.9 ± 24.1 across all anatomical locations (patella, trochlea, femoral condyles). There were no significant differences in mean MOCART 2.0 scores or proportions with high MOCART 2.0 score of 80 or above between anatomical cartilage lesion locations.
MOCART 2.0 Scores Overall and for the Different Cartilage Lesion Locations.
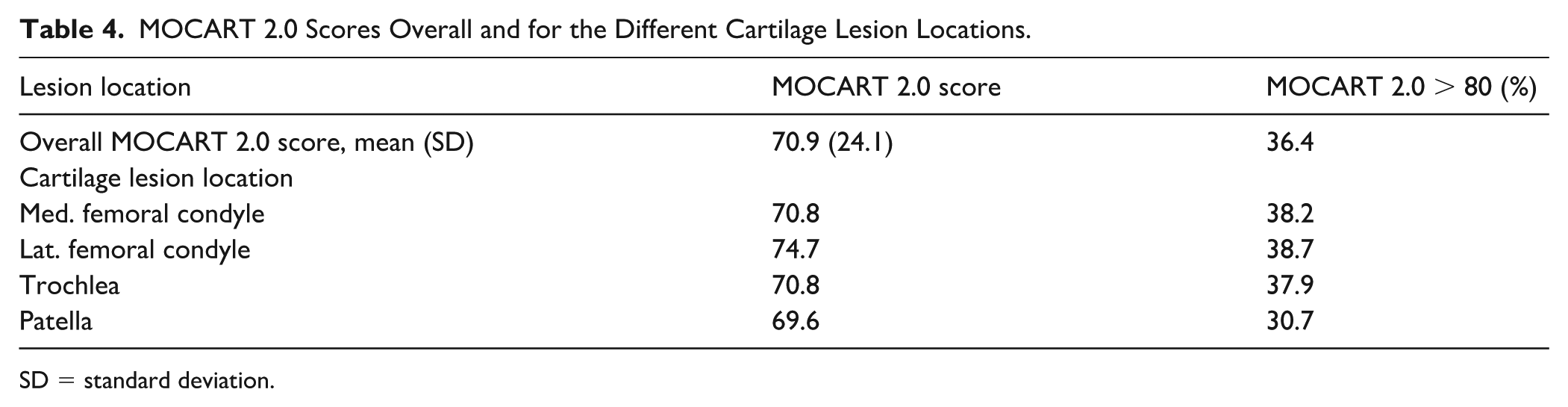
SD = standard deviation.
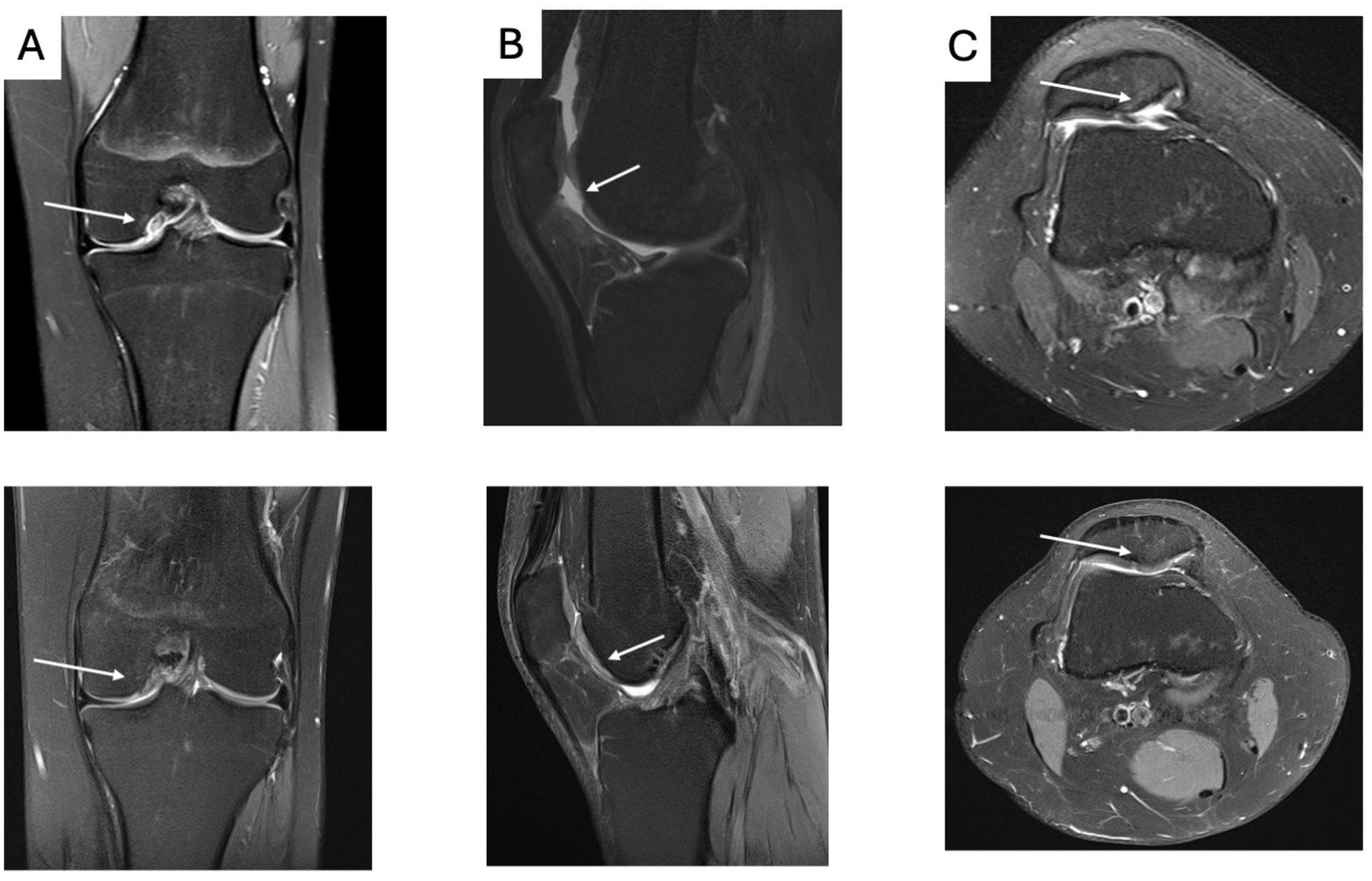
MRI knee examples of preoperative and 1-year follow-up of patients with excellent repair healing responses based on MOCART score 90 or above.
Complications and Reoperations
A total of
Additionally, 3 patients underwent reoperations unrelated to the index cartilage repair (meniscal surgery or ACL reconstruction following new knee injuries).
Discussion
The primary finding of this study was that cartilage repair with HA-BMAC in combination with intraarticular PRP resulted in good clinical outcome based on highly clinically relevant improvement in patient-reported outcomes as well as favorable biological repair outcome evidenced by MRI documented cartilage repair formation.
The clinically relevant improvements in patient-reported outcomes observed at 1-year follow-up in the present study are consistent with the findings of Gobbi et al.,9 -11 who reported similarly favorable improvements at 2-year follow-up in their cohort undergoing BMAC-based cartilage repair. Their studies also utilized KOOS and other PROMs to assess subjective outcomes. The comparable magnitude of improvement reinforces the evidence that HA-BMAC cartilage repair has a positive impact on patient-reported outcomes.
The studies by Gobbi et al. did not present MRI documentation for cartilage repair tissue quality but have presented a few arthroscopic second-look evaluation and histology from biopsies takes at second-look procedures. The second-look evaluation in 4 out of 15 patients found smooth and well repair tissue in all 4 cases. Histology demonstrated well integrated repair tissue with various degrees of hyaline and fibrocartilage tissue composition.9 -11 The varying tissue composition also found in the present study based on the variable MRI findings regarding structure and signal intensity of the repair tissue might reflect the histological findings of the Gobbi study.
Other cartilage repair methods have been MRI evaluated with the MOCART 2.0 scoring system that was used in the present study. Autologous minced cartilage transplantation has been investigated in several studies by Saltzman et al.21,22 They found overall MOCART 2.0 scores improving from 64 to 70 points from 2 to 5 years of follow-up. The findings of MOCART 2.0 score at 71 after 1 year in the present study could suggest similar or slightly better cartilage tissue can be obtained with the HA-BMAC cartilage repair technique compared to minced cartilage transplantation. But more direct comparative studies will be needed to clarify if HA-BMAC cartilage repair performs better than other cartilage repair techniques.
The present study did not have a control treatment group with another relevant cartilage repair methods that could have benchmarked the presented HA-BMAC based repair outcomes against another cartilage repair methods. The finding of improved subjective outcomes and favorable MRI based cartilage healing responses are thus associations with the HA-BMAC technique and do represent indications of superiority over other cartilage repair techniques. Previous studies have however compared HA-BMAC with both microfracture and ACI. In a study be Gobbi et from 2016 25 HA-BMAC repairs and 25 microfracture repairs were compared. The study found that HA-BMAC based repair had better subjective PROM scores outcome than microfracture that also was maintained over time better than microfracture based repairs. 8 Is the study comparing HA-BMAC and ACI almost similar subjective outcome improvements and MRI based healing responses. 23 The findings suggest that HA-BMAC based cartilage repair outcomes might be superior to microfracture based repair and similar to ACI based repair.
The separate impact of the BMAC cells and hyaluronic acid scaffold for the overall cartilage repair response is difficult to assess. A study by Tan et al. investigated isolated implantation of a hyaluronic acid scaffold as isolated cartilage repair technique in 46 patients with grade 4 cartilage lesions. This study found clinically relevant improvement in KOOS PROM scores that were similar to the improvements found in the present study for KOOS pain and symptoms but not as good as found for KOOS sport and KOOS quality of life. No overall imaging data were presented in that study. This comparison indicated to a hyaluronic scaffold implantation alone for cartilage repair can provide clinically relevant subjective outcome improvement, but the combination of scaffold and BMAC results in better overall subjective outcome improvement including sports function and quality of life. 24
In the present case series reoperation due to HA-BMAC graft overgrowth was seen in 9% of cases and was the primary complication related to the HA-BMAC implantation. The were 3 graft failures (1.8%) leading to revision reoperation. The studies by studies by Gobbi and Whyte 8 presented no reoperations due to graft hypertrophy but failures needing revision was somewhat higher with 3 out of 23 patients (13%). Graft overgrowth during cartilage repair have however been reported for autologous minced cartilage transplantation in 1 out of 23 (4%) cases. 21 ACI as another cell-based cartilage repair technique has reported 25% incidence of graft hypertrophy. 25 The relatively high incidence of HA-BMAC graft hypertrophy in the present study indicates that the combination of HA scaffold and BMAC produces a potent tissue formation response that can result in an adverse event with too extensive new tissue formation. Although no systematic cause for the tissue overgrowth could be identified it is potentially important that implantation of HA-BMAC implant is performed with the implant slightly recessed in the cartilage defect to reduce the risk of tissue overgrowth.
BMAC-based repair treatment has been criticized for the lacking control of the bone marrow cell components in BMAC-based surgical techniques. The constituents of BMAC vary highly between individuals and even vary for the same individual at different times, which potentially can result in heterogeneous cell compositions in different patients that can affect the healing stimulation from the BMAC cells.14,26 This issue can be part of the relatively variable healing responses seen after HA-BMAC cartilage repair in the present and previous studies. In a study by Fossum et al. the impact of cultured chondrocytes was investigated in a RCT comparing collagen scaffold covered cartilage lesions where cultured chondrocytes were added in one group and microfracture was performed in the other group. The study did not find any subjective outcome superiority with the more advance usage of cultured chondrocytes. 27 These results add to the issue of significance of cellular contributions to cartilage repair where scaffolds alone can provide similar outcomes.
The clinical implications of the present cartilage repair study are that the use of HA-BMAC combined with PRP consistently resulted in improved clinical outcome as well as favorable biological healing responses thereby confirming previous studies promising results with this technique. This could indicate that HA-BMAC combined with PRP is a clinical valid cartilage repair method that can be more widely used due its consistently good outcomes both regarding subjective outcome and cartilage lesion healing response.
The most significant strength of this study is its large number of patients (n = 165), which represent the largest patient cohort presented to date with HA-BMAC cartilage repair. Another strength was that almost all patients had MRI cartilage repair evaluation at 1-year follow-up allowing for better imaging based biological healing response evaluation.
This study has some limitations. Primarily no control group was included in the study. This could have put the outcome data in perspective to another relevant cartilage repair method. In addition, there was a low completeness of patient-reported outcomes was low completeness, which could have introduced selection bias. The PROM data should therefore be evaluated with caution. Further could associated procedures such as osteotomies and ligament reconstruction contribute varyingly to the subjective clinical outcome. Additionally, MRI data of cartilage repair tissue does not evaluate the biomechanical structural integrity of the tissue nor the histological tissue composition. This could result in the MRI based analysis classifying the cartilage repair tissue at a better quality than the true repair tissue structural quality. In addition, investigating MRI-based cartilage repair outcome at 1-year follow-up represents a relatively early healing stage. HA scaffold, BMAC, and PRP are used together in the present cartilage repair technique; this means that the specific contribution of each component cannot be determined from study outcomes.
Conclusion
The combined use of HA-BMAC combined with PRP resulted in improved subjective clinical outcomes and favorable biological healing responses at 1 year postoperatively. This one-step cartilage repair technique appears to be a clinically valid option for treatment of full-thickness cartilage lesions in the knee.
Footnotes
Ethical Approval
Ethical approval was obtained from the regional ethics committee (ID: 1-45-70-118-24).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded entirely by the orthopedic department at Aarhus University Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Aggregated data are available from the corresponding author. Individual patient data are not available due the ethical data transfer rules at Aarhus University Hospital.