
Abstract
Personality is relatively stable in adulthood but could change in response to life transitions, such as caring for a spouse with a terminal illness. Using a case–control design, spousal caregivers (n = 31) of patients with terminal lung cancer completed the NEO Five-Factor Inventory (NEO-FFI) twice, 1.5 years apart, before and after the patient’s death. A demographically matched sample of community controls (n = 93) completed the NEO-FFI on a similar time frame. Based on research and theory, we hypothesized that bereaved caregivers would experience greater changes than controls in interpersonal facets of extraversion (sociability), agreeableness (prosocial and nonantagonistic), and conscientiousness (dependability). Consistent with hypotheses, bereaved caregivers experienced an increase in interpersonal orientation, becoming more sociable, prosocial, and dependable (Cohen’s d = .48–.67), though there were no changes in nonantagonism. Changes were not observed in controls (ds ≤ .11). These initial findings underscore the need for more research on the effect of life transitions on personality.
Spousal caregivers of patients with terminal illnesses simultaneously experience transitions to new roles and often-unprecedented stressors surrounding loss. Recognizing that spousal caregivers are susceptible to elevated morbidity and mortality, they have been described as “hidden patients” (Löckenhoff, Duberstein, Friedman, & Costa, 2011). Transitions can lead to increased depression and anxiety, and some caregivers experience prolonged grief during bereavement (Braun, Mikulincer, Rydall, Walsh, & Rodin, 2007; Prigerson et al., 2009). Caregivers may also experience existential changes, such as finding a greater sense of meaning and purpose (Kim, Carver, Schulz, Lucette, & Cannady, 2013). It has been suggested that during the bereavement process, some caregivers may experience broad changes in personality (Caspi & Moffitt, 1993; McCrae & Costa, 1993), particularly in terms of how they interact with others (Shapiro, 2001; Shear & Shair, 2005). As the first study of which we are aware to quantify longitudinal changes in the five established domains of personality in a sample of bereaved caregivers, this study has implications for understanding the malleability of personality in response to life transitions in middle and older adulthood and efforts to enhance family-centered end-of-life care.
The Five-Factor Model (Costa & McCrae, 1992) provides a useful taxonomic frame for describing human dispositional variation along five broad personality domains: neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. A meta-analysis of 150 longitudinal studies showed that most personality development occurs prior to age 30, becoming highly crystallized in middle and older adulthood with 5-year longitudinal correlations surpassing r = .70 (Roberts & DelVecchio, 2000). Even during this peak of stability, however, personality can change due to life transitions, such as starting a job or getting married and success or failure in making these transitions (Hill, Turiano, Mroczek, & Roberts, 2012; Hudson, Roberts, & Lodi-Smith, 2012; Roberts & Mroczek, 2008; Specht, Egloff, & Schmukle, 2013).
Despite the importance of caregiver personality for mental health and physical functioning (Kim, Duberstein, Sorensen, & Larson, 2005; Löckenhoff et al., 2011), existing studies have provided inconclusive evidence that spouses experience any personality change surrounding the death of their partner (McCrae & Costa, 1993; Specht, Egloff, & Schmukle, 2011). One study (McCrae & Costa, 1993) found no differences between bereaved and married spouses on extraversion and openness, but the other three traits were not examined. Another showed that experiencing the death of a spouse was associated with less stable longitudinal correlations for agreeableness (Specht et al., 2011). Neither study could explore the influence of the caregiving–bereavement transition on personality change. In both studies, the samples of bereaved spouses were quite heterogeneous—not all were involved with caregiving, and the causes of death varied considerably (i.e., various chronic and acute illnesses, accidents, suicide, and homicide).
It has been suggested that life transitions that are characterized by relatively clearer social norms and rituals are more likely to engender personality change and that transitions characterized by relatively unclear norms are more likely to foster personality continuity (Caspi & Moffitt, 1993). Consistent with this view, the sociogenomic model of personality (Roberts, 2009) emphasizes that repeated reinforcement of state changes in constituent components of personality (i.e., thought, behavior, and affect) is needed to foster personality development incrementally over time, and social norms are an important source of ongoing reinforcement. Acknowledging that social norms surrounding death from natural illness in the United States continue to evolve (Carr, 2012), these norms are arguably somewhat better established for terminal illnesses with a predictable course (e.g., lung cancer) than for sudden deaths by accident, homicide, or suicide (Aldred, Gott, & Gariballa, 2005; Cerel, Jordan, & Duberstein, 2008). Therefore, we focused this initial investigation on terminal lung cancer and hypothesized that the process of losing one’s partner to lung cancer would lead spousal caregivers to experience personality change.
Drawing upon bereavement research and theory (Shapiro, 2001; Shear & Shair, 2005), we hypothesized that bereaved spousal caregivers would be particularly likely to experience changes in interpersonal facets of personality spanning extraversion, agreeableness, and conscientiousness. Caregivers may seek additional social support during bereavement (Ownsworth, Henderson, & Chambers, 2010), and the loss of a spouse could lead to significant restructuring of social networks (Bergman & Haley, 2009), perhaps with implications for the sociability component of extraversion. As well, bereaved caregivers commonly engage in “benefit finding” (Kim et al., 2013), such as developing a greater sense of tender-mindedness, compassion, responsibility, and character growth, perhaps reflected in aspects of agreeableness and the dependability facet of conscientiousness. In contrast to these changes in social behavior, bereavement research and theory makes no explicit predictions about openness to experience and suggests that changes in emotional stability are more commonly acute than enduring (Prigerson et al., 2009).
The current study is the first to examine personality change during the caregiving–bereavement transition in spouses of patients with terminal illnesses. A case–control design was used to examine personality changes over approximately 1.5 years in 31 spousal caregivers of patients with terminal lung cancer and a demographically matched control group of 93 continuously married adults in the community. Our primary hypothesis was that spousal caregivers would be more likely than community controls to experience personality change, as demonstrated by a higher percentage of participants experiencing reliable changes (Reliable Change Index [RCI] ≥ 1.96; Jacobson & Truax, 1991) across the NEO Five-Factor Inventory (NEO-FFI) personality facets. Second, based on research (Bergman & Haley, 2009; Kim et al., 2013; Ownsworth et al., 2010; Specht et al., 2011) and theory (Shapiro, 2001; Shear & Shair, 2005), we expected change to be confined primarily to interpersonal aspects of personality. Thus, we hypothesized that bereaved spousal caregivers would experience greater mean shifts and less stable longitudinal correlations than controls for interpersonal facets.
Method
Participants and Procedures
Self-reported personality data were collected longitudinally from a sample of spousal caregivers of patients with terminal lung cancer. For relatively rare events such as mortality, “case–control” study designs are often used (Rothman, Greenland, & Lash, 2008). Such designs assess individuals experiencing a relatively rare event and compare them to a generally similar control group. We utilized a control group of continuously married adults in the same community. As advocated in the guidelines for case–control studies, we selected a control group larger than the number of cases to provide reliable estimates and increased power for comparisons. A control group 3 to 4 times the size of controls is typically recommended, with larger control groups generally showing only small improvements in power. The control group was frequency matched 1 (Rothman et al., 2008) on age, gender, education level, and marital status at study entry (see Table 1), meaning that these variables were comparable across the two groups and thus could not account for observed group differences on any study outcome variables.
Baseline Characteristics for Bereaved Spousal Caregivers and Matched Community Controls.
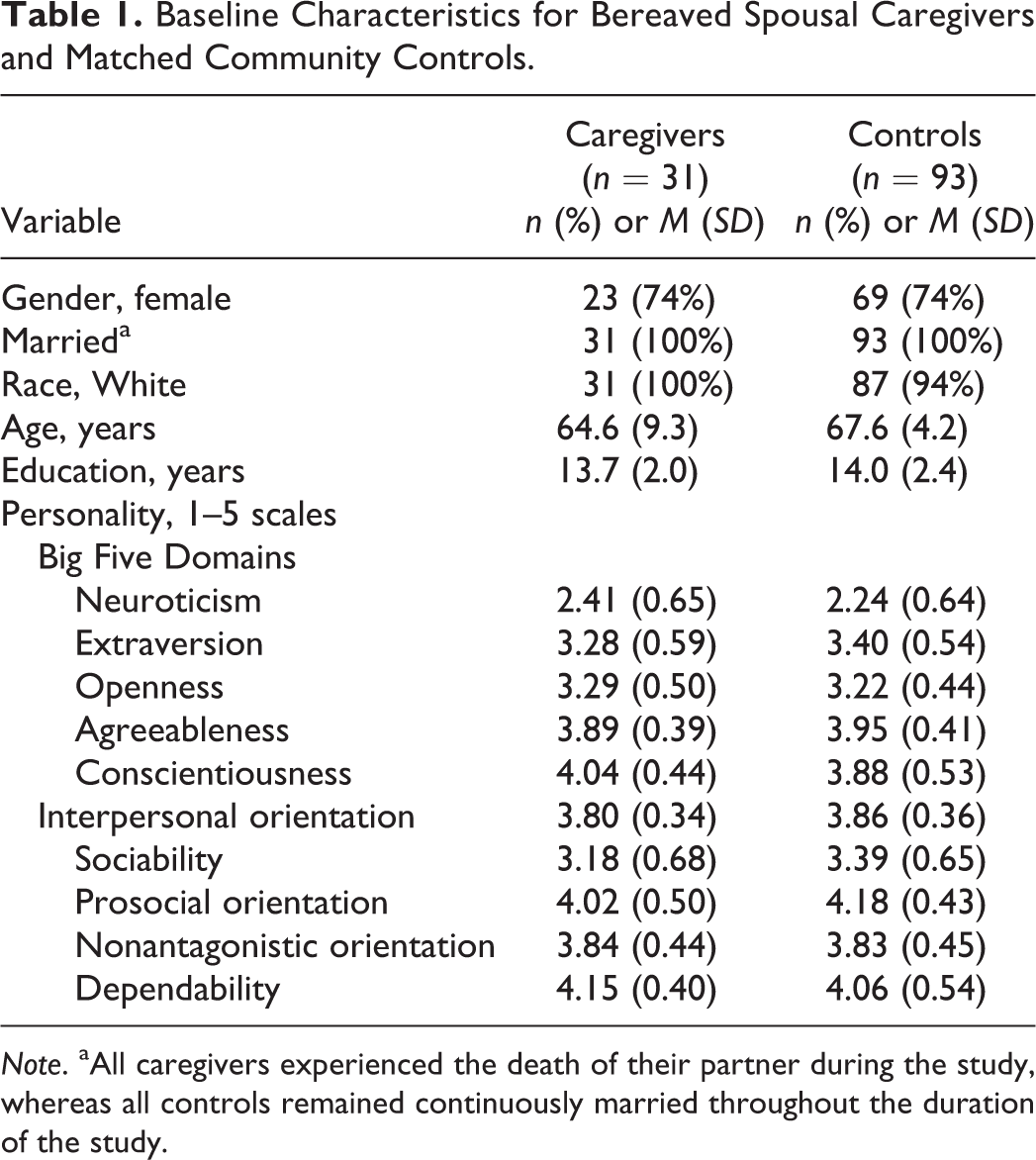
Note. aAll caregivers experienced the death of their partner during the study, whereas all controls remained continuously married throughout the duration of the study.
The sample of spousal caregivers (n = 31) consisted of all participants who completed personality measures, before and after the patient’s death, as a part of a broader psycho-oncology study of 120 caregivers conducted with approval of the institutional review board (IRB) at the University of Rochester cancer center (Kim et al., 2005). They first completed the NEO-FFI (Costa & McCrae, 1992) at study enrollment, which was 8.15 (standard deviation [SD] = 14.14) months after the patient’s diagnosis and again 18.00 (SD = 7.47) months later, which was 6.91 (SD = 1.35) months after the patient’s death. In this sample, mean survival was 1.59 (SD = 1.50) years after diagnosis. Data on mortality in the entire cohort are unavailable but refusal to participate in the postloss interview was believed to be exceedingly rare. Nearly half the inception cohort had Stage I disease (Kim et al., 2005) and most of these patients were alive 18 months after study entry. In contrast, most of the patients in this postmortem sample had either Stage III (35%) or Stage IV (42%) disease at the time of study entry. Moreover, in comparison to caregivers who only completed assessments at study entry, those in the present analyses were higher on openness (p = .02) but were otherwise comparable with respect to personality and demographics (all ps >.20).
The control group consisted of 93 demographically matched continuously married adults from the Rochester community. They were selected from participants recruited through primary care in one of the two broader IRB-approved studies of health and aging (Chapman et al., 2009; Lyness, Yu, Tang, Tu, & Conwell, 2009). They completed the NEO-FFI at study enrollment and again 16.06 (SD = 7.42) months later, with all remaining married at follow-up. Controls and caregivers were comparable with respect to basic demographics at study entry (proportion married, female, over age 70, college educated, and White), mean levels on the Big five personality traits at study entry, and the duration of the follow-up period between personality assessments.
Measures
The 60-item NEO-FFI (Costa & McCrae, 1992) was used to assess personality. As supported in factor analytic studies (Chapman, 2007; Saucier, 1998), the NEO-FFI measures the Big five domains of personality as well as 13 subscales assessing narrower facets. These scales included Neuroticism (self-reproach and negative affect), Extraversion (sociability, positive affect, and activity level), Openness to experience (aesthetic interests, intellectual interests, and unconventionality), Agreeableness (prosocial orientation and nonantagonistic orientation), and Conscientiousness (dependability, orderliness, and goal striving). The NEO-FFI has shown evidence for reliability and validity in studies of personality in middle and older adulthood, including among caregivers of patients with serious illnesses (Chapman, Lyness, & Duberstein, 2007; Patrick & Hayden, 1999). Internal consistency reliability was comparable across time points and samples, with a median Cronbach’s α of .81 for domains and .67 for facets, close to the .70 of longer NEO Personality Inventory–Revised facets and in line with reports from general samples (Chapman, 2007; Saucier, 1998). Additional descriptives are available in Table 1 and in the Online Appendix (Table S1; see Online Supplemental Material found at http://spps.sagepub.com/supplemental). For our secondary hypothesis, we used an overall indicator of Interpersonal Orientation, which was the summated composite of four interpersonal facets: sociability, prosocial orientation, nonantagonistic orientation, and dependability (Saucier, 1998). These interpersonal facets have been shown to correlate with other interpersonal constructs (e.g., warmth, altruism, trust, and dutifulness) and have implications for adult social functioning (Chapman, 2007; Hitchcock, 2008; Saucier, 1998). In the present sample, Cronbach’s α was .73 and .77 for caregivers and .76 and .79 for controls, at baseline and follow-up, respectively (average α = .76).
Statistical Analyses
The first hypothesis involved examining the percentage of participants in each sample experiencing reliable change in any of the personality facets. The RCI (Jacobson & Truax, 1991) was used to examine whether observed change in a facet score exceeded the level of change that would be expected due to measurement error, given the SD and reliability of the measure (see Robins Fraley, Roberts, & Trzesniewski, 2001; also McCrae, Kurtz, Yamagata, & Terracciano, 2011). RCIs of 1.96 or greater (corresponding to an α level of .05) in absolute magnitude reflected reliable change. A Z-test of proportions was used as an omnibus test to compare the percentage of bereaved spousal caregivers and the percentage of controls experiencing reliable personality change.
The second hypothesis examined the magnitude and direction of changes in interpersonal facets of personality. Change was operationalized using two standard approaches (Roberts & Mroczek, 2008). To quantify mean levels of change, we calculated Cohen’s d and used independent samples t-tests and multivariate analysis of variance (MANOVA) as appropriate to evaluate the statistical significance of between-group differences. Greater absolute values for Cohen’s d indicate greater change in a group as a whole. To assess relative change, we calculated Pearson’s r, with lower values reflecting greater change in the rank ordering of a group of persons, regardless of the group’s mean shift. Regression was used to evaluate the statistical significance of between-group differences in correlations, as indicated by a significant group by personality interaction term. When mean and relative changes were present simultaneously, we also examined the proportion of participants experiencing 1 and 2 SD changes, with between-group differences evaluated using Z-tests. The case–control design controlled for demographic differences via frequency matching, and sensitivity analyses provided statistical adjustment for time since diagnosis, the length of the follow-up, and cancer staging. Finally, to guard against Type I errors, the binomial probability test was used to examine whether the number of interpersonal facets with observed differences significantly exceeded the number that would be expected by chance.
Results
Omnibus Test of Personality Change
Consistent with our broad first hypothesis, bereaved caregivers were more likely than controls to experience reliable personality change (see Figure 1). Specifically, 87.1% of bereaved caregivers (95% confidence interval [CI] = [75.3%, 98.9%]) experienced reliable personality change versus 54.8% of controls (CI = [44.7%, 64.9%]), Z = 3.20, p = .001. This difference of 32.3% was qualified by a broad CI [12.7%, 51.9%].
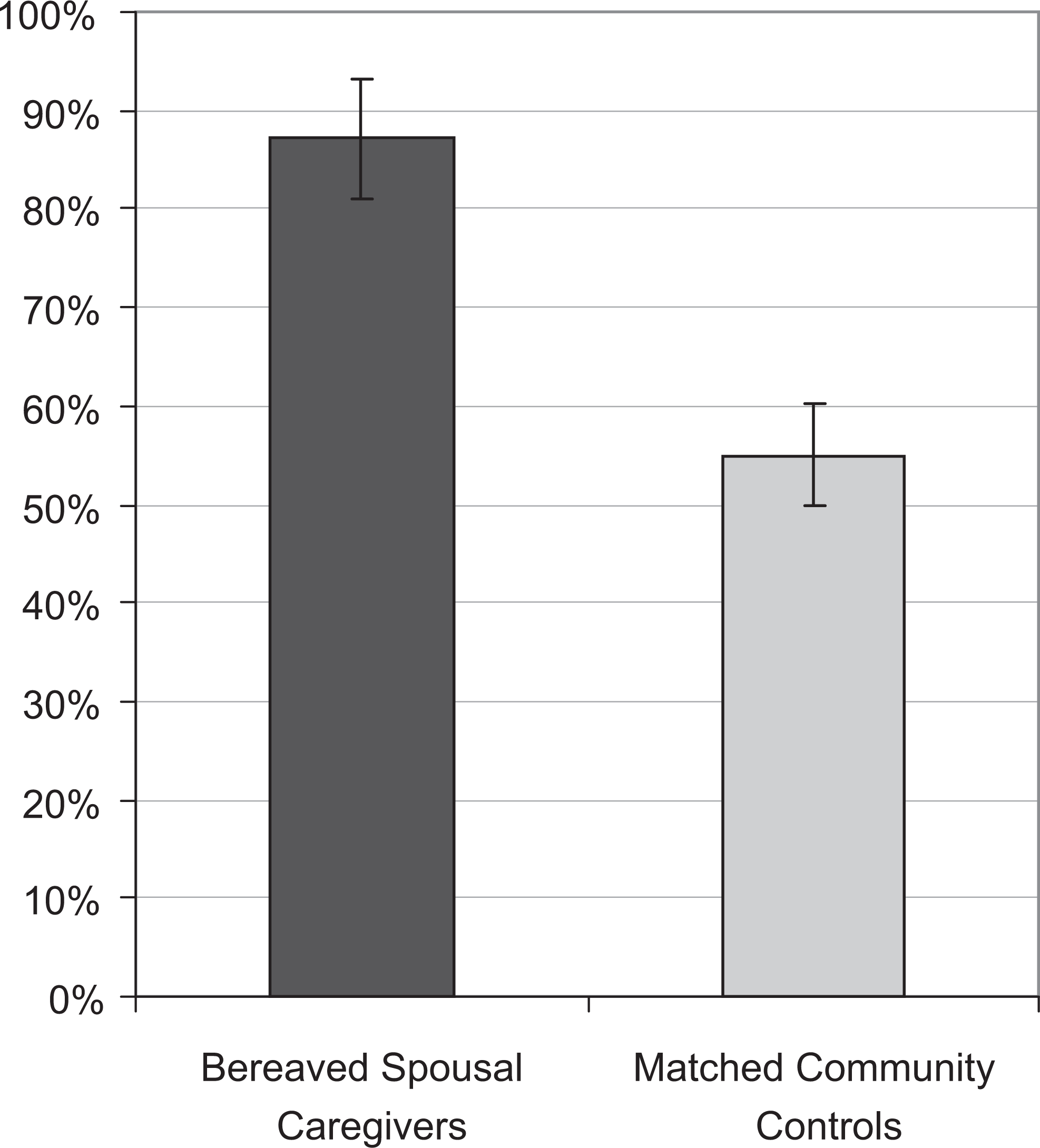
Percentage of participants experiencing reliable changes (RCI ≥ 1.96) in any of the NEO-FFI personality facets. Supporting our first hypothesis, bereaved spousal caregivers were significantly more likely to experience personality change than matched community controls over the 1.5-year follow-up period. Error bars indicate the standard error of the mean.
Areas of Personality Change
As hypothesized, bereaved spousal caregivers experienced changes in interpersonal orientation, whereas there were no significant changes in controls on any facet. Table 2 shows mean changes and longitudinal correlations. Bereaved caregivers experienced an increase in d = .67 (CI = [0.33, 1.01]) on the interpersonal orientation summated composite, indicating an average increase of ⅔-SD in interpersonal orientation. In MANOVA, the overall effect for between-group differences in change on the four interpersonal facets was significant, Wilks’s Λ = .884, F(4, 119) = 3.87, p = .005, as were individual effects for sociability, prosocial orientation, and dependability (ds from .48 to .50; see Table 2), but not for nonantagonistic orientation. Thus, relative to controls, bereaved caregivers experienced increases in most but not all aspects of interpersonal orientation.
Bereaved Spousal Caregivers and Matched Community Controls Differ in Amount of Personality Change Experienced During the 1.5-Year Longitudinal Study.
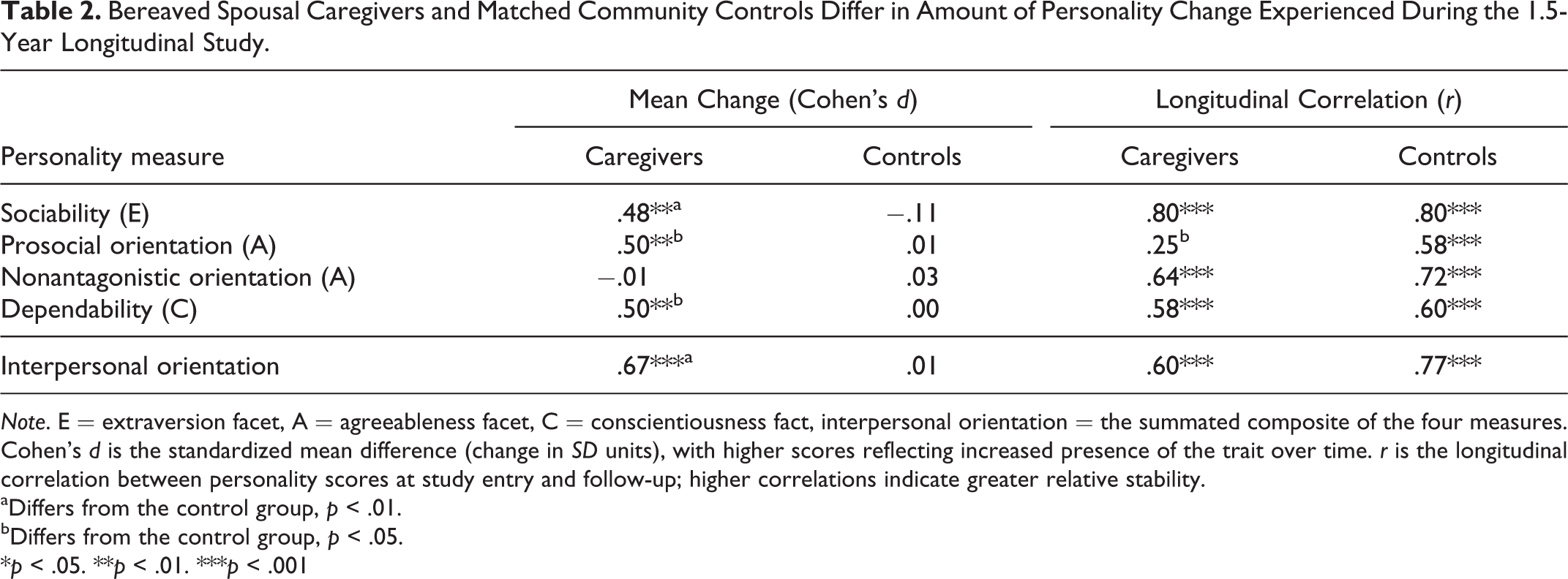
Note. E = extraversion facet, A = agreeableness facet, C = conscientiousness fact, interpersonal orientation = the summated composite of the four measures. Cohen’s d is the standardized mean difference (change in SD units), with higher scores reflecting increased presence of the trait over time. r is the longitudinal correlation between personality scores at study entry and follow-up; higher correlations indicate greater relative stability.
aDiffers from the control group, p < .01.
bDiffers from the control group, p < .05.
*p < .05. **p < .01. ***p < .001
Longitudinal correlations differed by group for prosocial orientation, with caregivers (r = .25, CI = [−0.11, 0.55]) having lower relative stability than controls (r = .58, CI = [0.43, 0.70]) in terms of who was highest to lowest on prosocial orientation (see Table 2). Combined with the mean increase in prosocial orientation, this relative instability meant that some caregivers experienced a larger increase in prosocial orientation than others, with 42% (CI = [26%, 59%]) of caregivers experiencing a 1 SD increase, and 16% (CI = [7%, 33%]) experiencing a 2 SD increase (greater than values of 11% and 2% for controls, Zs ≥ 2.98, ps ≤ .002).
Among the noninterpersonal personality facets measured, both caregivers and controls showed evidence for stability, with no statistically significant differences between groups (Table S2; see Online Supplemental Material found at http://spps.sagepub.com/supplemental). The average magnitude of mean changes was |d| = .10 (from −.24 to .27, all ps n.s.) for caregivers, and |d| = .08 (from −.17 to .18, all ps n.s.) for controls. The average longitudinal correlation was r = .67 (from .53 to .87, all ps < .002) for caregivers, and r = .69 (from .57 to .76, all ps < .001) for controls.
The number of interpersonal facets with hypothesized and observed group differences (three of four) exceeded the rate expected by chance (.05 × 4 facets = 0.20 facets by chance), p < .001. In summary, bereaved spousal caregivers were hypothesized and observed to experience changes in personality facets associated with social behavior.
Discussion
Bereaved spousal caregivers were more likely than controls to experience personality change, and these changes involved an increase in interpersonal orientation on facets spanning three domains of the Five-Factor Model (Costa & McCrae, 1992), namely agreeableness, extraversion, and conscientiousness. In fact, 87% (CI = [75%, 99%]) of bereaved caregivers experienced reliable personality change in at least one facet of personality (see Figure 1). Further, the average increase in interpersonal orientation was sizable in magnitude, approximately ⅔-SD (see Table 2). Arguably, caregiver changes in agreeableness were most dramatic, with two in five caregivers experiencing more than an SD increase in prosocial or courteous characteristics. Bereaved caregivers also experienced increased sociability, an extraversion facet, as well as increased dependability, a conscientiousness facet. As the first known study to examine personality changes during the caregiving–bereavement transition, our findings extend prior research (Braun et al., 2007; Kim et al., 2013; McCrae & Costa, 1993; Specht et al., 2011) by showing that interpersonal aspects of personality are sensitive to change during the caregiving–bereavement transitions.
This research has theoretical implications for understanding the impact of life transitions on personality development in the second half of life. Over the past several decades, the stability of personality has been subject to much debate (Roberts, 2009). It is now known that personality is relatively stable in the absence of major life perturbations, but potentially malleable in response to some types of life transitions involving health, relationships, and work (Roberts & Mroczek, 2008; Roberts, Walton, & Viechtbauer, 2006). Prior studies have found little (Specht et al., 2011) to no (McCrae & Costa, 1993) bereavement-related changes in personality. Those studies lumped together heterogeneous causes of death that may have affected personality in different ways and to different degrees (Caspi & Moffitt, 1993), neutralizing group-level effects. Our research suggests that when examining more uniform circumstances—participants were all spousal caregivers of patients with terminal lung cancer—bereavement-related personality changes are observable and can be sizable and multifaceted.
In contrast to our finding of personality change, some areas of caregiver personality were more stable. For example, trait-level neuroticism may remain stable throughout the bereavement process, despite state-level changes in caregiver emotional distress (Braun et al., 2007). Similarly, findings for openness indicate that caregivers’ preferred styles of thinking are not modified during caregiving–bereavement transitions. Moreover, one aspect of interpersonal orientation, the nonantagonistic facet of agreeableness, also remained stable. Based on item content and criterion correlations of the interpersonal facets in past studies (Chapman, 2007; Saucier, 1998), this suggests that the caregiving–bereavement transition may reflect changes in affiliativeness and altruism more so than hostility and argumentativeness.
Although bereaved spousal caregivers were significantly more likely than controls to experience personality change, many controls were found to experience idiosyncratic personality changes. As a group, controls did not experience mean-level changes in any of the 13 NEO-FFI facets, indicating that while changes were common, the specific nature of change varied from participant to participant. Prior studies have not typically reported the percentage of participants experiencing reliable personality changes, though our results indicate this might be a fruitful area of research.
Future studies can build on these findings by examining the implications of caregiver personality change for family functioning and the grieving process. In the context of terminal illnesses, spousal caregivers are often emotionally burdened by the challenges of treatment decision making and communicating with clinicians, other family members, and their ill spouses. Following the death of a spouse, widowed individuals must navigate social terrain without their partner. Changes in caregiver personality could complicate or ease these processes. As well, there is a need for research on the implications of personality change for prolonged grief (Prigerson et al., 2009). Further analyses of personality change following other somewhat homogeneous life transitions, such as unplanned early retirement or bereavement following suicide, accident, or sudden natural deaths are also warranted. Research is needed to understand how different types of life transitions affect personality continuity and change (Caspi & Moffitt, 1993).
This research also holds promise for informing interventions in the context of caregiving and other expectable (vs. unpredictable) life transitions. Existing theories of self-knowledge (Hoerger, Chapman, Epstein, & Duberstein, 2012; Wilson, 2009) suggest that people have a limited understanding of how they will be affected by future life transitions. Notably, while individuals acknowledge prior changes in personality, they seem to experience great difficulty imagining future personality change (Quoidbach, Gilbert, & Wilson, 2013). Yet, foreknowledge is instrumental for guiding planning and facilitating adjustment. In the same way that popular education about the “stages” or states of grief has helped many individuals (Maciejewski, Zhang, Block, & Prigerson, 2007), improving caregiver understanding of the potential effects of the caregiving–bereavement transition on personality could ease the adjustment of caregivers to their changing roles. Information about personality change could be embedded within health education materials or psychosocial interventions for caregivers to promote self-care (Hoerger et al., 2013; Maciejewski et al., 2007). Clinicians (psychologists, nurses, and physicians) should be aware of the possibility of personality change in the context of the caregiving–bereavement transition.
This study had several strengths, chiefly the uniqueness of the data, the use of a well-validated measure of personality, and the case–control design. Nonetheless, as the first study to examine changes in the five established domains of personality during the caregiver–bereavement transition, there were several limitations. As with any study involving self-reports of personality, the observed changes could be influenced by motivation to see oneself in a particular light. Informant reports of personality have strengths and weaknesses (e.g., Hoerger et al., 2011) but could make a significant methodological contribution to the burgeoning literature on personality change. Second, the present analyses could underestimate personality changes experienced by bereaved caregivers, as the power to detect significant effects was constrained by the total sample size (n = 124). Third, the investigation included two time points of observation separated by only 18 months and a control sample drawn from primary care. Multiwave studies and different controls (e.g., spouses with minimal roles in caregiving and spouses of terminal patients who survive the follow-up period) would be needed to quantify the duration of personality change and to determine whether change occurs steadily, cyclically, or suddenly, and whether changes are mainly due to the diagnosis of potentially life-limiting illness, the burdens of caregiving, or loss. For example, given that the initial assessment occurred after the patient’s diagnosis, it is possible that the process of personality change had begun by the time spouses were recruited into the study. (If that is the case, the present findings represent underestimates.) Calls for the inclusion of personality data in Electronic Medical Records (Chapman, Roberts, & Duberstein, 2011) and Medicare Welcome packets (Friedman, Veazie, Chapman, Manning, & Duberstein, 2013), if heeded, could mitigate this problem in future research. Fourth, definitive mortality data were unavailable for the entire cohort, so while we cannot rule out the possibility that those opting to complete the follow-up were more likely than nonparticipants to become interpersonally oriented, we can definitely conclude that, at least, a subset of bereaved caregivers became decidedly more interpersonally oriented. Finally, with larger samples, future studies could explore whether findings are moderated by caregiver factors (e.g., amount of time spent with the patient, extent of other support, and health) or whether there are reliable changes in the personality factor structure during the caregiving–bereavement transition.
In closing, this study makes an initial contribution to the rapidly expanding body of research on personality change. For decades, personality research arguably operated from a defensive posture, focusing on fending off criticisms about cross-situational consistency, behavioral prediction, and construct validity. Acknowledging countervailing views, researchers in the post-Mischelian era are now free to address more nuanced questions about the nature of personality change (Roberts, 2009). By providing preliminary evidence that spouses of terminally ill patients can experience personality changes during the caregiving–bereavement transition, our research consequently sparks curiosity about the mechanisms underlying personality change.
Conclusion
This preliminary study suggests that spousal caregivers of patients with terminal cancer experienced an increase in interpersonal orientation during the caregiver–bereavement transition, as demonstrated by personality change in aspects of extraversion, agreeableness, and conscientiousness. Further research examining the caregiving–bereavement transition and other life transitions (e.g., divorce, retirement, and unemployment) in large samples could clarify how life transitions affect personality development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Mental Health (T32MH018911, K07MH001135, R01MH061429), National Institute on Aging (K08AG031328), and National Cancer Institute (R01CA106370).