
Abstract
Across six studies (N = 904), we suggest a novel mechanism for race disparities in pain treatment: Perceiver deficits in discriminating real from fake pain for Black (relative to White) individuals. Across Studies 1–4, White participants (Studies 1–4) and Black participants (Study 2) were better at discerning authentic from inauthentic pain expressions for White targets than for Black targets. This effect emerged for both subtle (Studies 1 and 2) and intense (Studies 3 and 4) pain stimuli. Studies 5 and 6 examined consequences for medical care decisions by examining pain treatment recommendations by laypeople (Study 5) and pain authenticity judgments by medical providers (Study 6). This work advances theory in pain perception, emotion judgment, and intergroup relations. It also has practical significance for identifying unexplored mechanisms causing racial disparities in medical care.
Pain management in the United States is inequitable. Medical providers must quickly and accurately decide who needs intervention and of what intensity. These decisions are typically based on rapid evaluation of presented symptoms, including patients’ nonverbal signals (Roter et al., 2006). Herein, we test the novel hypothesis that perceivers fail in accurately reading the nonverbal signals of pain for Black relative to White people, which undermines treatment accuracy and equity.
Black Americans often receive less aggressive pain treatment than White Americans (Pletcher et al., 2008). Black patients evaluated at emergency departments are about half as likely to be prescribed opioids as comparable White patients (Singhal et al., 2016), and for those Black patients who are prescribed opioids, they tend to accompanied by greater restrictions (e.g., drug tests; Becker et al., 2011). These disparities are pervasive, existing across pain types and treatment contexts (Green et al., 2003).
Psychologists have identified several mechanisms underlying racial disparities in pain treatment (and medical care more broadly), including prejudice (Penner et al., 2010; Sabin et al., 2008), stereotyping (Hoffman et al., 2016; Moskowitz et al., 2012), empathy gaps (Drwecki et al., 2011), and differential health care access (Mayberry et al., 2000). Moreover, these instances of disparate care are theorized to undermine Black patients’ trust in and utilization of healthcare (Dovidio et al., 2008). However, these processes largely speak to discrepancies in amount or quantity of treatment administered. In addition to less pain treatment, inaccurate treatment occurs, such as Black patients being subject to unnecessary surgery (Lee & Ko, 2009) or inappropriately prescribed opioids for migraine symptoms (Schpero et al., 2017). These disparities in treatment accuracy affect patient care, leaving patients vulnerable to both under- and overtreatment. Inappropriate treatment of pain diminishes the quality of life (McCarberg et al., 2008) and fuels the rapidly expanding opioid epidemic (Bohnert et al., 2011). Whereas previous work explains less aggressive treatment, we propose that accuracy deficits may reflect a heretofore undocumented racial deficit in reading other’s pain authenticity. The current work examines perceivers’ ability to discern pain expression authenticity for Black as compared to White targets and implications for equitable pain treatment.
Expressions of pain attract attention (Vervoort et al., 2013), communicate distress, and can elicit sympathy and help (Craig, 2015). Because pain expressions stimulate sympathetic action, people may express inauthentic pain for numerous reasons including interpersonal or financial incentives, avoiding responsibilities, or gaining access to opioids (Fordyce, 1976; Rigg et al., 2010). Although pain expressions are perceptually distinct from other expressions (Craig et al., 1992), perceivers often struggle to discern real from fake pain expressions (Hill & Craig, 2002; Poole & Craig, 1992), a challenge that we hypothesized may be especially fraught for judgments of racial minority group members.
Specifically, perceivers are often better at reading nonverbal cues from own-race, majority group, or high-status people (Lloyd & Hugenberg, 2021). For example, there are robust own-race advantages in face recognition (Hugenberg et al., 2010), anxiety detection (Gray et al., 2008), emotion recognition (Elfenbein & Ambady, 2002), and smile authenticity (Friesen et al., 2019). Similarly, advantages for high status and majority group members are documented in face memory (Ratcliff et al., 2011), emotion recognition (Elfenbein & Ambady, 2002), and lie detection (Lloyd et al., 2017). Because Black Americans are low-status minority group members in the United States (Fiske, 2012) and are commonly treated by White providers (∼75% of U.S. doctors are White; Castillo-Page, 2010), we theorized Black individuals are at greater risk for having their pain expressions misunderstood (Fiske, 2012). Specifically, we hypothesized that perceivers would demonstrate poorer ability to distinguish authentic from inauthentic pain expressions for Black relative to White individuals.
Overview
Across our studies, participants viewed videos or pictures of Black and White individuals experiencing actual pain or faking pain, and participants attempted to distinguish between real and fake signals (i.e., made “real pain” vs. “fake pain” decisions). Accordingly, we adopted a signal detection approach to disentangle the effects of race on pain authenticity sensitivity (i.e., ability to discriminate real from fake pain) and response bias (i.e., propensity to over or under perceive pain authenticity). Sensitivity is of key interest in the current work, because it indexes perceptual abilities to distinguish between signals (e.g., between real and fake pain expressions; Macmillan & Creelman, 1991). In contrast, response bias can be understood as a function of response preferences or the payoff matrix (e.g., tendency to use the real response more frequently for White than Black targets). By separating sensitivity from response bias, we can understand how target race influences perceivers’ ability to distinguish fake from real pain, separately from perceivers’ response tendencies.
Whereas previous work has focused almost exclusively on race-based biases in perception of pain, the current work is novel in its focus on sensitivity in pain authenticity judgments. Across six studies, we tested whether perceivers struggle to disentangle real from fake pain for Black relative to White targets (i.e., lower sensitivity for Black than White targets), across White and Black perceivers, low- and high-intensity pain experiences, and laypeople and medical professionals. We also tested whether this sensitivity effect appears to undermine appropriate pain treatment for Black individuals.
Open Practices and Ethics Statements
These data are available on a permanent third-party archive (https://osf.io/t76jv/). Human subjects and copyright protections prevent video and image materials from being made openly accessible, however, instructions for acquiring materials are described in the Supplemental Online Materials (SOM). All studies were approved by the Miami University Institutional Review Board (protocol #01365r—Pain Detection).
Study 1
White participants viewed videos of Black and White individuals displaying real or fake pain and attempted to discern expression authenticity. We anticipated observing better pain authenticity detection sensitivity for White than Black targets.
Method
Statistical Power and Participants
No previous research has examined target race effects on pain detection. However, previous work explored how variables such as empathy and experience with others’ pain correlate with pain intensity judgment accuracy (Ruben & Hall, 2013). Because empathy or experience could be mechanisms by which target race impacts pain authenticity judgments, we drew from Ruben and Hall (2013) to estimate sample size. Their work revealed a r = .29 correlation for empathetic concern and r = .16 correlation for experience with others’ acute pain as predictors of accuracy. A priori power analyses indicated that between 45 (r = .29) and 151 (r = .16) participants would be needed to achieve 80% power for the primary analysis, a paired samples t tests comparing Black and White targets on sensitivity (Faul et al., 2009). In August 2017, 151 online participants were recruited via Amazon Mechanical Turk (MTurk; paid $2.00). In Study 1, we included only participants who identified as non-Hispanic White in the analyses (N = 111; 58 women, 53 men; mean age = 38.0 years, SD = 11.7). No other participants were excluded from analyses. 1 A sensitivity power analysis conducted in G*Power (1 − β = .80; Faul et al., 2009; paired sample t test; α = .05) indicated this sample could detect an effect size of dz = 0.27 or greater.
Stimuli
Pain authenticity videos were selected from the Denver Pain Authenticity Stimulus Set (D-PASS; Lloyd et al., 2021), which contains videos of Black and White, men and women, and exhibiting real and fake expressions of pain. Pain was induced using a pressure algometer until participants reached their pain tolerance. In fake pain videos, targets pretended to feel pain without pressure. Stimuli included 64 5-s videos without sound. Videos included one real and one fake expression from 32 targets (eight Black men, eight Black women, eight White men, and eight White women). Videos were coded using Noldus Face Reader Software (Skiendziel et al., 2019) to quantify expression of pain and nonpain related action units. There were no race differences in pain or nonpain-related action units overall (collapsing across veracity), for real videos or for fake videos, ts(27) < 1.24, ps > .227. 2 More stimuli details are presented in the SOM.
Procedure
Participants were randomly assigned to one of the two counterbalanced video sets containing 32 videos (16 genuine and 16 fake). Each video set contained one video from each target. Stimulus order was randomized within set. Following each video, participants rendered a “real” or “fake” decision.
After the pain detection task, participants completed auxiliary questionnaires assessing individual differences in race-related motives (Plant & Devine, 1998), contact with White and Black individuals (Kunstman et al., 2013), trait-level empathetic concern (M. H. Davis, 1980), and prior personal experience with pain (Ruben & Hall, 2013). These questionnaires were exploratory and analyses are presented in the SOM. At the conclusion of all studies, participants provided demographics (i.e., age, gender, ethnicity, and race) and were debriefed.
Results
We used signal detection analyses to parse sensitivity (our primary interest) from response bias. Our a priori prediction was that perceivers would exhibit lower sensitivity for Black target, relative to White target, pain authenticity.
Sensitivity
Pain authenticity sensitivity (d´), or the ability to discern real from feigned pain, was calculated separately for Black and White targets by first calculating the proportions of hits (i.e., correct identifications of feigned pain expressions) and false alarms (i.e., calling genuine pain expressions fake). Full or empty cells (i.e., cells with a proportion of 1 or 0, respectively) were replaced with .95 or .05, respectively (Macmillan & Kaplan, 1985). 3 These proportions were standardized following signal detection theory guidelines 4 and sensitivity was calculated by subtracting the standardized measure of false alarms from the standardized measure of hits. Thus, greater sensitivity values indicated better discrimination between real and fake expressions of pain.
Overall sensitivity
A one sample t test indicated that overall sensitivity (M = 0.05, SD = 0.54, 95% CI [−0.06, 0.15]) did not differ from chance (d´ = 0), t(110) = 0.88, p = .382, d = 0.17, 5 consistent with findings that people struggle to discern real from fake pain (Hill & Craig, 2002; Poole & Craig, 1992).
Target race effects
Our primary analysis, a paired samples t test, found that perceivers were better at discerning feigned from genuine expressions of pain for White (M = 0.19, SD = 0.81, 95% CI [0.04, 0.34]) than for Black (M = −0.10, SD = 0.77, 95% CI [−0.24, 0.05]) targets, t(110) = 2.67, p = .009, 95% CI [−0.51, −0.07], dz = −0.25. Notably, perceivers discerned genuine from fake expressions significantly better than chance for White targets, t(110) = 2.49, p = .014, d = 0.47, but not for Black targets, t(110) = 1.36, p = .176, d = −0.27.
Response Bias
Pain authenticity response bias or the tendency to have a lower or higher psychological threshold to render a particular response was calculated using criterion (c) from signal detection theory. Criterion scores were determined separately for White targets and Black targets by adding the standardized measures of hits and false alarms before dividing by −2. Thus, greater c values indicate more “real” responses and fewer “fake” responses.
Overall response bias
We first conducted a one sample t test comparing overall response bias (i.e., average response bias across White and Black targets) to 0 (indicative of no response bias). This analysis indicated that overall perceivers showed a fake bias (M = −0.11, SD = 0.47, 95% CI [−0.20, −0.02]) or a tendency to use the fake response more often than the real response, t(110) = 2.45, p = .016, d = −0.47. This finding extends previous research indicating that people underestimate others’ pain intensity (Prkachin et al., 1994).
Target race effects
A paired samples t test comparing response bias for Black and White targets showed no differential response bias for Black (M = −0.09, SD = 0.53) and White (M = −0.13, SD = 0.55) targets, t(110) = 0.91, p = .364, 95% CI [−0.05, 0.15], dz = 0.09. This response bias effect also was not significant in four of the five subsequent studies. Thus, response bias results for subsequent studies are reported in the SOM.
Study 2
Study 1 provided preliminary evidence for effects of target race on discerning pain authenticity, a novel mechanism by which pain treatment disparities may arise. These sensitivity findings could be explained by both own-race advantage and majority-group advantage hypotheses, because both accounts predict that White perceivers would have greater sensitivity for White compared to Black targets. Both hypotheses are supported by previous findings, and the two accounts are often conflated in research designs (like Study 1) where only majority group participants are recruited.
A competitive test of the own-race advantage and majority-group advantage hypotheses requires examining both majority and minority group perceivers, which was the focus of Study 2. Two outcomes seemed plausible. First, both Black and White participants could demonstrate better own-race than cross-race pain detection (i.e., an own-race advantage), predicting a perceiver race by target race interaction. Alternately, both Black and White perceivers could demonstrate greater sensitivity for White than for Black targets, predicting a main effect of target race (i.e., a majority-group advantage).
Method
Statistical Power and Participants
Power needed to detect a cross-over interaction (as predicted by the “own-race advantage” hypothesis) is equal to that needed to detect the original target race main effect (Frost & Ledgerwood, 2020). Using the target race sensitivity effect from Study 1 (i.e., d = 0.25), an a priori power analysis indicated that 128 participants would be needed to achieve 80% power (Faul et al., 2009). Participants were recruited from MTurk (paid $2.00) in October 2017. A study qualification ensured that participants who completed Study 1 were not permitted to participate in Study 2. To ensure adequate recruitment of Black participants, we conducted two waves of data collection. First, we recruited 124 participants, 93 of whom identified as non-Hispanic White (satisfying recruitment requirements) and nine identified as non-Hispanic Black. We then recruited an additional 93 participants who qualified if (1) they did not partake in the first wave of data-collection, (2) they responded “Black” on a race qualification-survey completed sometime within the previous 5 years. Our final sample included 93 non-Hispanic White and 79 non-Hispanic Black online participants (89 women, 83 men; mean age = 37.0 years, SD = 10.6). A sensitivity power analysis (1 − β = .80; α = .05; paired sample t test) indicated this sample could detect an effect size of dz = 0.21 or greater.
Procedure
Participants completed the same pain detection task described in Study 1 and completed an adapted version of the Childhood Experience Questionnaire (M. M. Davis et al., 2016) and the Identity Centrality Scale (Luhtanen & Crocker, 1992). Analyses involving these exploratory individual difference measures are reported in the SOM.
Results
Overall Sensitivity
Overall pain authenticity sensitivity (M = −0.06, SD = 0.60, 95% CI [−0.15, 0.03]) did not differ from chance, t(171) = 1.38, p = .169, d = −0.21.
Participant and Target Race Effects
A 2 (participant race: Black, White) × 2(target race: Black, White) mixed-model analysis of variance (ANOVA; target race was the repeated factor) on sensitivity revealed only a main effect of target race, F(1, 170) = 6.44, p = .012,
Black and White perceivers more accurately distinguished between fake and real pain for White than Black targets, providing initial support for a majority-group advantage in pain detection. However, the null interactive effect between perceiver and target race does not rule out the possibility of moderation by perceiver race. Indeed, our sample estimate was based on the expectation of a cross-over interaction, but other interaction patterns could exist but were not adequately powered.
Study 3
The previous studies employed controlled pain authenticity videos, yielding experimental control but limiting external validity. It is unknown whether the observed findings would generalize to more extreme expressions of pain, including the intensity of pain typically treated by medical professionals and likely to engender pain treatment disparities. In Study 3, we developed a second stimulus set featuring high-intensity pain stimuli.
Phase 1: Stimuli Creation
During stimuli creation, still images of professional soccer players experiencing injury versus “diving” during play were compiled and standardized. “Diving” players fake injury for on-field advantage, which is common in men’s professional soccer (Rosenbaum et al., 2010). Despite such fabrications, severe injuries are also common in soccer (American Orthopaedic Society for Sports Medicine, 2010), allowing us to collect images of high-intensity genuine and fabricated pain expressions.
We collected images of the same player exhibiting both genuine and fake expressions of physical pain. This approach ensured that identity of the target was controlled across veracity and eliminated potential confounding factors such as player reputation or stable facial characteristics. The final image set was selected based on image quality and pretesting of targets’ apparent race; well-known players were not included. In total, 24 images of 12 unique players (six Black, six White) exhibiting real and fake pain served as the stimuli. Stimulus creation details are available in the SOM.
Phase 2: Primary Data Collection
Method
Statistical power and participants
The average weighted effect size examining the difference between sensitivity for Black and White targets in Studies 1 and 2 (r = .10) was used for a priori power analysis, indicating that 199 participants were required to obtain 80% power in a paired samples t test. Two-hundred and one U.S. residents were recruited via MTurk (86 women, 115 men; mean age = 35.5 years, SD = 11.0; paid $0.50) in March 2018. Because participant race did not moderate the Study 2 effects, we retained all participants (154 White, 22 Black, 16 Asian, six Latinx, two American Indian or Alaska Native, and one bi- or multiracial). Results are unaffected if Hispanic and non-White participants are excluded. A sensitivity power analysis (1 − β = .80, α = .05; paired sample t test) indicated this sample could detect an effect size of dz = 0.20 or greater.
Procedure
Participants engaged in a pain detection task where they viewed images of soccer players displaying real or fake pain. Participants were randomly assigned to view one of the two image sets each containing 12 of the 24 total images (six real, six fake) with one image from each target player.
Results
Because each participant viewed only 12 stimuli, signal detection analyses were not feasible. Instead, we calculated pain authenticity accuracy as our metric of pain detection ability. The proportion of correct responses was calculated separately for Black and White targets.
Overall accuracy
Overall pain authenticity accuracy (M = 0.61, SD = 0.17, 95% CI [0.08, 0.13]) was significantly greater than chance (.5), t(200) = 9.11, p < .001, d = 1.39. Overall accuracy was much better than in the previous studies, which is sensible given the high-intensity pain stimuli (Galin & Thorn, 1993).
Target race effects
Perceivers exhibited a greater proportion of correct pain authenticity responses for White (M = 0.63, SD = 0.25) than for Black (M = 0.59, SD = 0.20) targets, t(200) = 2.05, p = .042, 95% CI [−0.09, −0.00], dz = −0.16. In sum, participants had greater difficulty discriminating real from fake pain for Black than White targets, even in high-intensity pain circumstances vital to patient care.
Study 4
Controlling for player identity in Study 3 offered advantages but also restricted stimuli to individuals who both had a serious injury and were recorded simulating injury. This prohibited signal detection analyses and raises alternate explanations. Notably, target race effects could be attributed to differences in injury severity. For example, if White targets experienced more serious injuries, and more serious injuries are easier to read (Galin & Thorn, 1993), this could explain race differences in pain authenticity accuracy. Study 4 addressed this alternate explanation by creating a second high-intensity stimulus set matching for injury severity across race.
Phase 1: Stimuli Creation
We compiled real and fake pain images of male soccer players with the goal of matching injury severity. Real images were matched across race based on specific experienced injury (e.g., anterior cruciate ligament tear) and consequences of injury. Specifically, the number of days injured, t(18) = 0.16, p = .872, 95% CI [−96.38, 112.58], ds = 0.07, and the number of games missed, t(18) = 0.20, p = .847, 95% CI [−12.90, 10.95], ds = −0.09, did not differ across target race. The final image set was selected based on image quality and pretesting of apparent race while eliminating highly recognizable players. Details are available in the SOM. In total, we selected 40 images (20 Black, 20 White; 20 real, 20 fake) of different soccer players exhibiting real or fake pain.
Phase 2: Primary Data Collection
Method
Statistical power and participants
Based on Study 3’s power analysis, 203 U.S. residents were recruited from MTurk (85 women, 117 men; mean age = 37.0 years, SD = 12.0; 147 White, 24 Black, 12 Asian, 12 Latinx, four bi- or multiracial, three American Indian or Alaska Native, one did not provide race information; paid $1.00) in March 2018. A sensitivity power analysis (1 − β = .80; α = .05; paired sample t-test) indicated this sample could detect an effect size of dz = 0.20 or greater.
Procedure
The pain detection task was similar to Study 4. Participants viewed 40 images of male soccer players exhibiting real or fake pain, presented in a random order.
Results
Study 4 employed signal detection analyses, mirroring Studies 1 and 2.
Overall sensitivity
Overall pain authenticity sensitivity (M = 0.42, SD = 0.44, 95% CI [0.36, 0.48]) was better than chance, t(202) = 13.43, p < .001, d = 1.89.
Target race effects
Perceivers were again better at discerning feigned from genuine expressions of pain for White (M = 0.64, SD = 0.70) than for Black (M = 0.19, SD = 0.50) targets, t(202) = 7.64, p < .001, 95% CI [−0.56, −0.33], dz = −0.54. Study 4 replicated Study 3 matching extremity and type of injury across race.
Study 5
Studies 1–4 demonstrated that participants were better at distinguishing pain expressions for White people than Black people. Study 5 investigated whether these inaccuracies influence pain treatment recommendations by asking laypeople to render treatment recommendations in response to the soccer player stimuli.
Method
Statistical Power and Participants
Participants were recruited from an introductory psychology pool and compensated via course credit. The study was conducted during the final weeks of the academic year (May 2018), and consequently, we collected as much data as possible, yielding 154 participants (74 women, 80 men; mean age = 19.4 years, SD = 1.2; 110 White, four Black, 33 Asian, six bi- or multiracial, and one other). A sensitivity power analysis (1 − β = .80; α = .05; 2 × 2 repeated measures ANOVA) indicated this sample could detect an effect size of dz = 0.18 or greater.
Procedure
The Study 4 procedure was modified in three ways. First, participants were not explicitly told that expressions were real or fake, allowing them to doubt the authenticity of the expression while still recommending treatment and to believe pain is genuine but choose not to treat it (e.g., a bruise may be believed but not treated). Second, participants provided belief judgments on a continuous scale, reporting how much they believed the expressions was genuine, ranging from 1 (not at all) to 7 (completely). Third, participants made pain treatment recommendations by estimating how much drug treatment would be necessary to relieve each target’s pain on a 4-point scale (World Health Organization, 1986; 1 = no drug treatment, 2 = nonopioid drug treatment [e.g., Aspirin], 3 = weak opioid drug treatment [e.g., Codeine], 4 = strong opioid drug treatment [e.g., Morphine]).
Results
Belief Ratings
For the belief ratings provided in Study 5, greater pain perception accuracy is indicated by greater belief for real relative to fake expressions. We computed participants’ mean belief ratings across target Race and Expression Veracity, which were analyzed in a 2 (target race: Black, White) × 2 (expression veracity: real, fake) repeated-measures ANOVA. A target race by expression veracity interaction was observed, F(1, 153) = 251.67, p < .001,
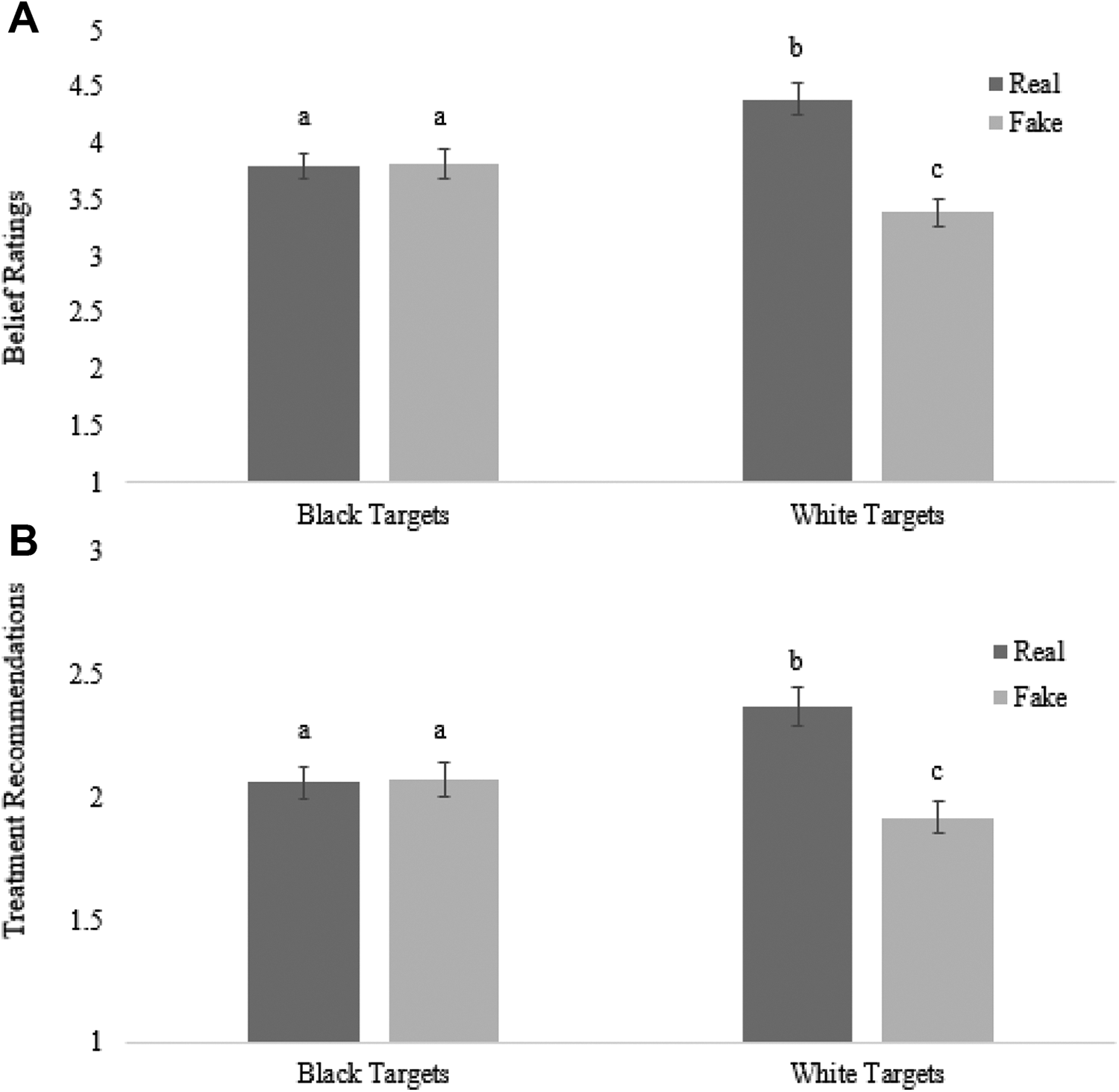
Target race by expression veracity interactions on belief ratings (A) and treatment recommendations (B), respectively. Note. Error bars indicate 95% CIs. Different superscripts indicate significant pairwise comparisons within each analysis.
Treatment Recommendations
We next examined treatment recommendations using a 2 (target race: Black, White) × 2 (expression veracity: real, fake) repeated-measures ANOVA on treatment recommendations, which again yielded a main effect of target race, F(1, 153) = 13.96, p < .001,
Mediation Analyses
We examined whether the target race effects on treatment accuracy were mediated by pain perception accuracy. We calculated pain perception accuracy scores (belief ratings for real minus fake expressions) and treatment accuracy scores (treatment recommendations for real minus fake expressions) separately for Black and White targets. We then conducted a within-participants mediation analyses with 10,000 bootstrapped resamples (Montoya & Hayes, 2017), with pain perception accuracy serving as the mediator and treatment accuracy as the outcome variable. As seen in Figure 2, the 95% CI for the indirect effect did not include zero, ab = −0.43, 95% CI [−0.52, −0.34], indicating accurately detecting pain authenticity mediated race differences in treatment accuracy.
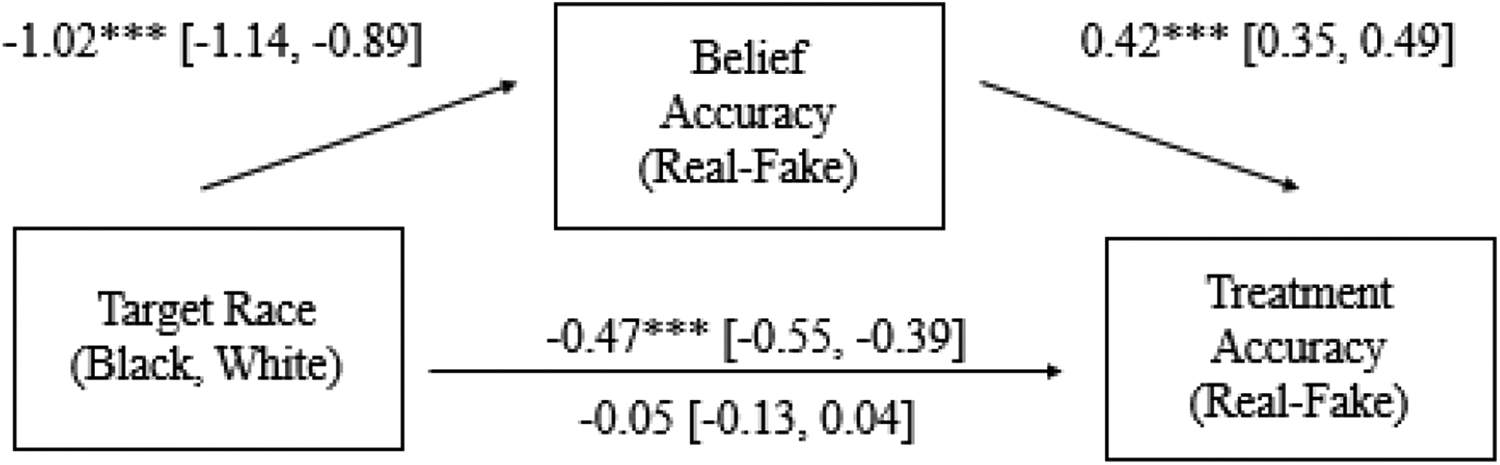
Mediation model depicting the effect of target race (black-white) on pain treatment accuracy (larger numbers = greater treatment recommended for real relative to fake expressions) as mediated by pain perception accuracy (larger numbers = greater belief in real relative to fake expressions). Note. Path estimates represent unstandardized regression estimates alongside their 95% confidence intervals. ***p < .001.
Study 6
Because medical providers determine pain treatment, it is imperative to study these effects with actual practitioners. Clinicians might not show target race effects on sensitivity observed in Studies 1–5 because they have greater expertise judging others’ pain (Ruben & Hall, 2013). However, it is also plausible that clinicians would show deficits in pain detection similar to laypeople. Indeed, intergroup biases are often observed even amongst individuals who overtly reject racism (Pearson et al., 2009), who have robust experience in intergroup contexts (Al Ramiah & Hewstone, 2013), and even amongst medical providers (Sabin & Greenwald, 2012).
Method
Statistical Power and Participants
A power analysis using the average weighted effect size from Studies 1–4 comparing Black and White sensitivity (r = .14) indicated that 103 participants were required to obtain 80% power for the primary analysis a paired samples t test. Participants were recruited May–June 2018 and compensated via entry into a raffle for one $500 and 15 $100 Amazon gift cards.
Medical providers were recruited via professional forums or newsletters and via snowball sampling. A priori inclusion criteria were that participants must reside in the United States and make either pain treatment recommendations or decisions in their role as a medical provider. The final sample consisted of 107 medical providers (69 women, 37 men; mean age = 34.0 years, SD = 12.3; 88 White, 12 Asian, 3 Black, one Native Hawaiian/Pacific Islander, one bi- or multiracial, one other; one did not provide demographics). Clinicians varied in years of experience (M = 10.95, SD = 12.08) and occupation (e.g., medical residents). For more details, see the SOM. A sensitivity power analysis (1 − β = .80, α = .05; paired sample t test) indicated this sample could detect an effect size of dz = 0.27 or greater.
Procedure
Participants first completed the pain detection task described in Study 1. The lab stimuli were used because they tended to show smaller effect sizes and allowed for signal detection analyses, providing a conservative test. Next, participants completed exploratory individual difference measures, including the Empathetic Concern subscale of the Interpersonal Reactivity Index (M. H. Davis, 1980), a questionnaire assessing medical experience, and a measure of contact with Black and White patients. Analyses involving these exploratory measures are included in the SOM. Finally, participants indicated whether they made treatment decisions or recommendations, which served as inclusion criteria.
Results
Study 6 employed signal detection analyses, mirroring Studies 1, 2, and 4.
Overall Sensitivity
Average sensitivity (M = −0.02, SD = 0.66, 95% CI [−0.15, 0.10]) did not differ from chance, t(106) = 0.36, p = .72, d = −0.07.
Target Race Effects
Medical providers were better at discerning feigned from genuine expressions of pain for White (M = 0.07, SD = 0.79) than for Black (M = −0.12, SD = 0.82) targets, t(106) = 2.08, p = .040, 95% CI [−0.35, −0.01], dz = −0.20.
General Discussion
Across six studies, perceivers struggled to discern real from fake expressions of pain for Black relative to White targets. This effect occurred for both laypeople and medical providers, for both White and Black perceivers and for both high- and low-intensity pain. A meta-analysis across studies indicated this effect is reliable, quantified by sensitivity (Studies 1, 2, 4, and 6), decision accuracy (Study 3), or pain perception accuracy (Study 5), Z = −6.09, p < .001, weighted r = .21.
Our findings indicate that Black Americans are not just undertreated for pain, they may also receive poorly calibrated pain treatment. Current interventions for medical treatment disparities focus on reducing physician bias (e.g., Burgess et al., 2007). Although these interventions may be effective in improving aspects of doctor–patient interactions, they are unlikely to improve doctors’ ability to discern Black patients’ pain authenticity. Instead, interventions that implicate improving sensitivity for Black patients (e.g., performance feedback, training attention to diagnostic cues to authenticity) may prove more effective in improving health care outcomes for all people.
Although the current work extends our understanding of race-based health disparities by suggesting potential interpersonal sensitivity influences in equitable care—specifically pain, the underlying cause of this sensitivity difference is an open question. We describe this effect as a perceiver-level effect, consistent with relative inattentiveness to minority members (Mackie, 1987) and low-status targets (Ratcliff et al., 2011). However, target-level influences are possible too. For example, dialect theory (Elfenbein & Ambady, 2002) asserts differences in emotion expressions across (sub)cultures. Accordingly, Black patients’ pain is met with less empathy (Drwecki et al., 2011), and Black Americans are stereotyped as drug-seeking (Hausmann et al., 2013). These discrimination experiences may lead to suppression or exaggeration of pain. However, computerized ratings of facial expressions were equivalent for intensity, failing to provide support for this target-level explanation.
The current work did not indicate systematic effects of target race on response bias in judgments of pain authenticity. Indeed, a meta-analysis examining the effects of target race on response bias showed no reliable effect, Z = −0.28, p = .779, weighted r = −.02 (see SOM). These null effects may seem inconsistent with previous work establishing race-based biases in pain perception (Mende-Siedlecki et al., 2019; Trawalter et al., 2012) and treatment (e.g., Hoffman et al., 2016; Pletcher et al., 2008). However, in our work, response bias largely refers to bias in judgments of authenticity, which has not previously been explored. Further, in Study 5 where treatment recommendations biases were assessed, we replicated previous work indicating less intensive pain care recommendations for Black than White targets. But in addition to this main effect of target race effect on treatment quantity, we also document a target race effect on treatment accuracy (the interaction of race and veracity on treatment), which was more than 10 times larger than the main effect of target race. We do not deny the undertreatment of Black people’s pain. Instead, we also argue that failure to distinguish authenticity may also have important effects in pain care disparities.
Conclusion
Appropriate care relies on accurately reading patient pain cues. In the current work, we document a consistent inaccuracy in reading Black people’s pain. Regardless of populations, stimuli, and tasks, Black people’s pain was judged and treated less accurately than White people's. These findings both contribute to our understanding expression perception, and they also identify a novel mechanism by which real-world racial disparities in pain treatment may occur.
Supplemental Material
Supplemental Material, sj-docx-1-spp-10.1177_19485506211045887 - Race Deficits in Pain Detection: Medical Providers and Laypeople Fail to Accurately Perceive Pain Authenticity Among Black People
Supplemental Material, sj-docx-1-spp-10.1177_19485506211045887 for Race Deficits in Pain Detection: Medical Providers and Laypeople Fail to Accurately Perceive Pain Authenticity Among Black People by E. Paige Lloyd, Audrey R. Lloyd, Allen R. McConnell and Kurt Hugenberg in Social Psychological and Personality Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Philanthropic Educational Organization and National Science Foundation (BCS-1748461).
Supplemental Material
The supplemental material is available in the online version of the article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.