
Abstract
A male neonate presented a dural arteriovenous fistula (DAVF) at the confluence with paralysis of the orbicularis oris muscle. The interesting features in our case were the clinical symptoms (orbicularis oris muscle paralysis at birth), angioarchitecture (high-flow arteriovenous shunts at the confluence) and the size and hemodynamic flow (mid-sized venous pouch) of the fistula. Additionally, the embolization technique (i.e., occipital artery approach, closing shunts with pure glue) automatically resulted in the immediate and complete closure of accessory feeders without any additional treatment, and the midterm clinical outcome was good. We succeeded improving the symptoms of a neonate with a congenital high-flow DAVF by closing a fistula using a small amount of glue.
Introduction
Dural arteriovenous fistulas (DAVFs) are the most common cerebrovascular lesions found in all age groups. DAVFs rarely occur in neonates and children, and the underlying etiological mechanisms have not been reported to date.
Case Report
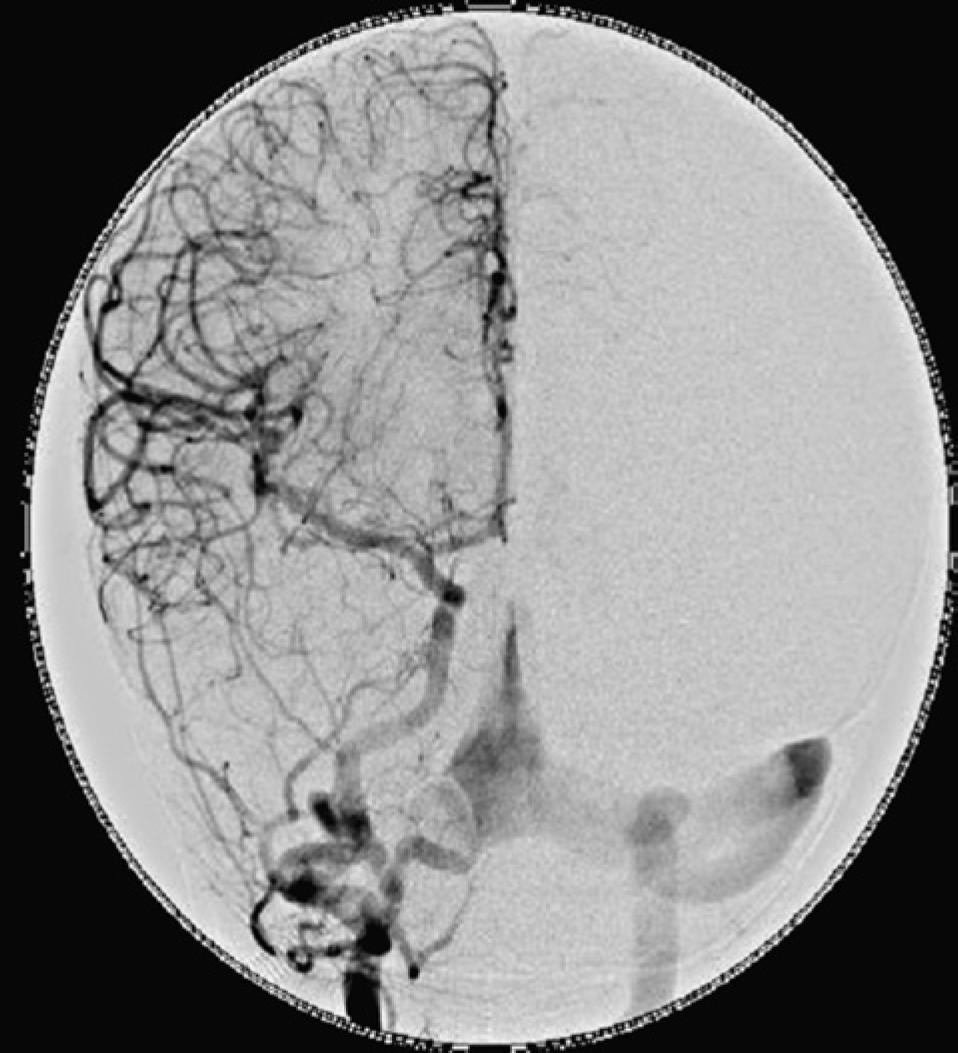
The patient, the first child of his 32-year-old mother, was born in cephalic presentation at a fetal age of 39 weeks and two days after a normal pregnancy. The birth weight was 2990 g, with a head circumference of 32.0 cm, and his Apgar score was 9/10 (1 min/5 min). The cardiac pulse rate was 130/min, and his blood pressure was 70/40 mmHg. This patient had a temperature of 36.6°C at birth, and his blood pressure was 64/30 mmHg. There were no abnormal skin findings. His anterior fontanelle was flat. Respiratory sounds were clear. Laboratory testing revealed a hemoglobin level of 11.4 g/dL, a white cell count of 1400/L, a platelet count of 48.3/L, an aspartate aminotransferase level of 51 IU/L, an alanine aminotransferase level of 19 IU/L, a lactate dehydrogenase level of 375 IU/L, a total protein level of 6.9 g/dL, and a C-reactive protein level of 0.02 mg/dL. The patient displayed hemifacial palsy when crying, including paralysis of the orbicularis oris muscle. His facial palsy gradually worsened, and the patient underwent brain MRI/MRA seven months after birth. Bilateral middle meningeal and right posterior cerebellar arteries feeding dural arteriovenous fistulas into the expanded confluence of sinuses were confirmed. The child was initially followed for ten months. However, his symptoms persisted and progressed gradually, and endovascular intervention was performed for closure. Digital subtraction angiography demonstrated that the meningeal artery of the occipital arteries on both sides (Figures 1-3) and right posterior inferior cerebellar artery (Figure 4) fed dural arteriovenous fistulas into the expanded confluence of sinuses. The largest fistulous shunt, the right occipital artery were high speed and embolized using NBCA 3 cc + Lipiodol 0.1 cc +1 g of Tantalum powder. The associated shunts from the right posterior inferior cerebellar artery and contralateral meningeal branch of the occipital artery automatically closed. The patient experienced no complications from this intervention, and the progression of facial paralysis subsequently ceased. No lactation problems were observed during ten months of follow-up. After the intervention, symptom progression stopped, although symptoms were still present during the 10-month follow-up period.
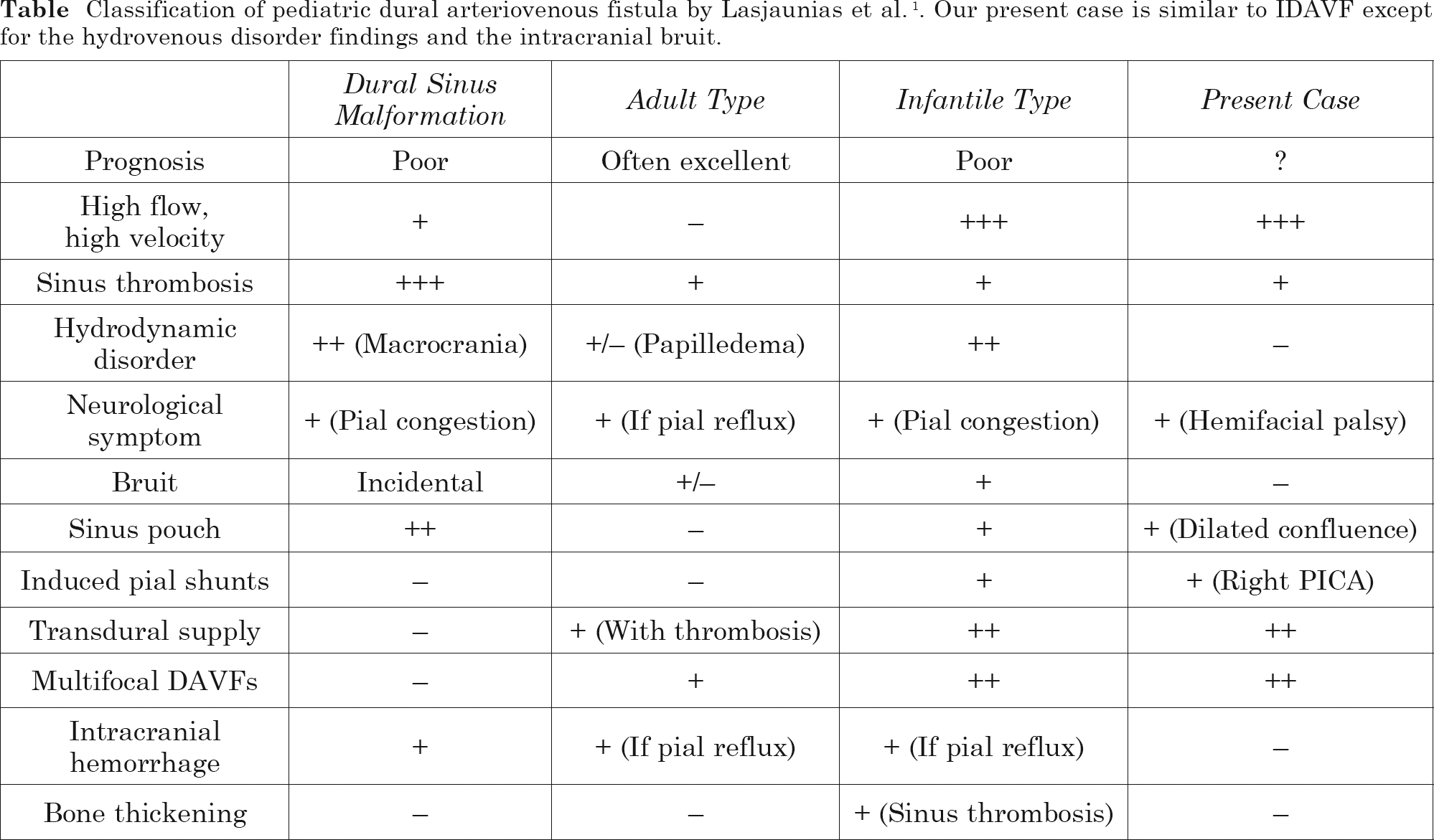
Right common carotid arteriography (lateral view): right occipital artery fed dural arteriovenous fistulas at the confluence. Common carotid arteriography (A-P view): right occipital artery fed dural arteriovenous fistulas at the confluence. Left occipital artery fed dural arteriovenous fistulas at the confluence (lateral view). Right vermian branch of posterior inferior cerebellar artery fed dural arteriovenous fistulas at the confluence (A-P view). Classification of pediatric dural arteriovenous fistula by Lasjaunias et al.
1
. Our present case is similar to IDAVF except for the hydrovenous disorder findings and the intracranial bruit.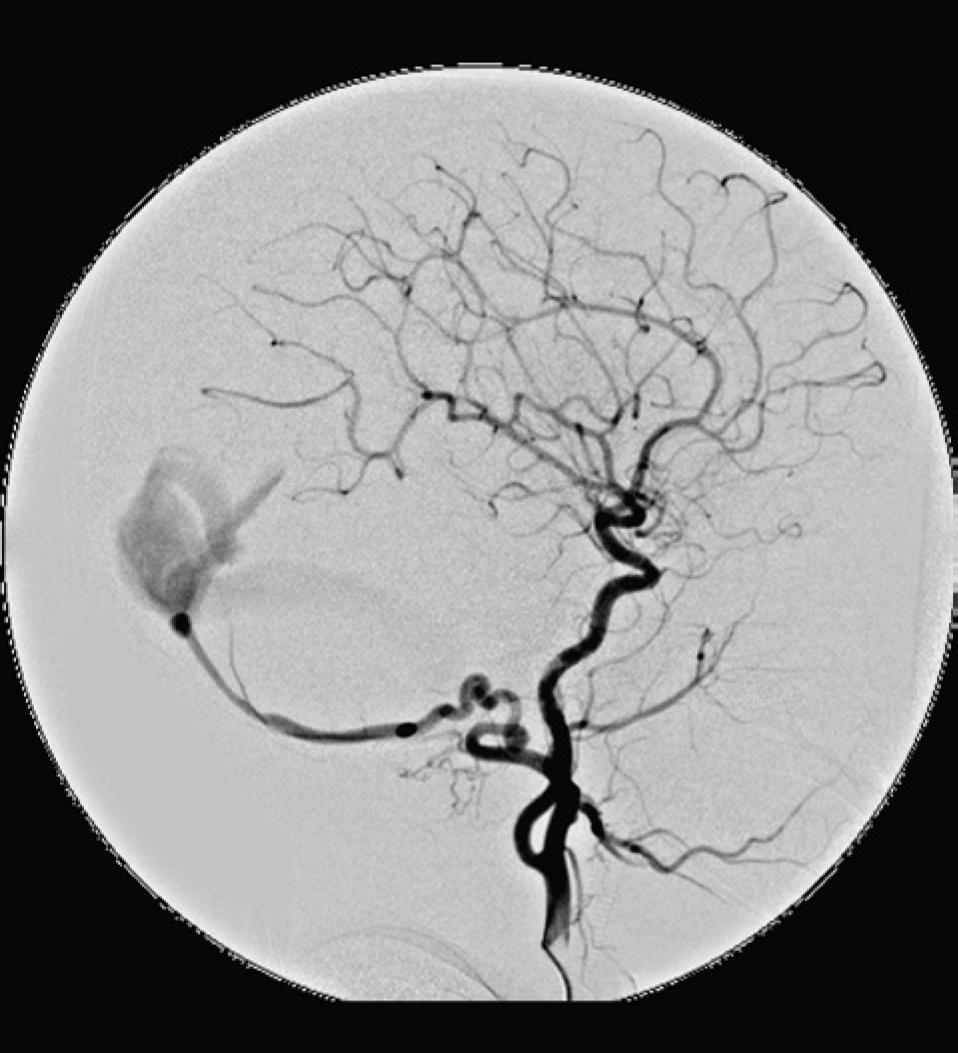


Discussion
Dural arteriovenous fistulas (DAVFs) are most common cerebrovascular lesions. Although they are found in all age groups, DAVFs rarely occur in neonates. Treatment for these lesions is typically endovascular, although a multimodal approach may be needed in some cases. Lasjaunias et al. 1 distinguished among three types of dural arteriovenous shunts that appear in children: (i) dural sinus malformations (DSM): congenital malformed sinuses with giant pouches or malformations of the jugular bulb where thrombosis or occlusion of the sinus outflow is a central clinical concern; (ii) infantile-type dural arteriovenous shunts (IDAVF): high-flow, often multifocal lesions with patent sinuses and induced pial arteriovenous shunts; and (iii) adult-type dural arteriovenous shunts (Table 1). In IDAVF, the sinus usually presents with a normal or slightly enlarged dural sinus with high-velocity flow through the AV shunt. In contrast, DSM presents with a dilated or giant pouch in the dural sinus that is usually associated with a low and/or relatively slow flow through the dural AV shunt. Adult-type DAVFs of the cavernous plexus or sigmoid sinus present with sinuses, which are normally small and sometimes partially thrombosed, and can be secondary to another local event. Clinically, IDAVF mimics other intracranial high-flow fistulas that present in infants because IDAVF shares many similar clinical symptoms with early cardiac failure and can result from high cardiac output and/or macrocrania, particularly in neonatal dural arteriovenous fistulas 1 .The DAVF in our patient presented as an IDAVF and involved the dorsal epidural venous system 2 . Although only 25 IDAVF cases have been reported in the literature, no IDAVF at the anterior condylar confluence have been described to date2-32.
In addition to the morphology of the dural sinus, IDAVF usually presents with macrocrania and mental retardation, while DSM manifests with more acute symptoms, such as convulsions, venous reflux, infarction, or hemorrhage. The symptoms correspond to chronic ischemia of venous origin, despite the absence of retrograde cortical venous drainage. The present case disclosed thrombosis of the right transverse sigmoid sinus with a mid-size dilated confluence. While our case presented with cranial nerve deficits immediately after birth, such instances have not been reported previously in the literature2-32. The etiology of the orbicularis oris muscle paralysis is hypothesized to be the arterial steal phenomenon produced by high flow dural fistulas at the confluence. The middle ear contains five distinct arteries: the anterior tympanic of the internal maxillary artery, the caroticotympanic artery of the internal carotid artery, the superior tympanic artery of the middle meningeal artery, the inferior tympanic of the ascending pharyngeal artery and the stylomastoid artery, which is a branch of the posterior auricular artery. In approximately half of the cases, the stylomastoid artery arise from a large superficial trunk, which supplies the occipital artery territory. In the remaining cases, the stylomastoid artery usually originates directly from the distal external carotid artery. Arterial steal produced by a high-flow shunt around the stylomastoid artery is strongly suspected as the etiological basis for the primary symptoms in the present case 33 .
The main shunt is a high-flow-induced pial arteriovenous shunt from the right PICA with convergence of the draining veins into the affected dural sinus. The dural sinus sump, or ven-turi sump effect creates a remote venous steal upstream that is not symptomatic but likely produces some degree of venous ischemia. The presence of the fistula leads to distal pial arteriovenous fistula, and new collaterals form due to the venturi sump effect, further exacerbating the initial shunt. As multiple feeders may converge into a single fistula, solid anatomical knowledge is essential to embolize only the necessary vessels with the least risk and optimal efficiency. In our experience, transarterial embolization represents the best method for controlling symptoms of multiple dural AV shunts.
Dural AVFs have not been shown to be familial or associated with other vascular malformations. Previous reports demonstrated the presence of mature arterial and venous configurations amid the absence of persistent embryonic vascular patterns. It has therefore been hypothesized that DAVFs in children develop after the third month of intrauterine life and may be acquired, although the acquisition may occur prenatally. The exact intrauterine events leading up to the development of neonatal DAVFs remain unknown, but a multifactorial process is likely33,34.
Conclusion
Among the interesting features of the dural arteriovenous fistula in our case were the clinical symptoms (orbicularis oris muscle paralysis at birth), angioarchitecture (high-flow arteriovenous shunts at the confluence) and the size and hemodynamic flow (mid-sized venous pouch) of the fistula. Additionally, the embolization technique (i.e., occipital artery approach, closing shunts with pure glue) automatically resulted in the immediate and complete closure of accessory feeders without any additional treatment, and the midterm clinical outcome was good.