
Abstract
We describe a case of combined mechanical thrombectomy of the right middle cerebral artery and stent angioplasty of the right internal carotid artery in a severe stroke caused by arterio-arterial embolism due to a traumatic dissection of the internal carotid artery. The patient was admitted with an NIHSS score of 19 and was discharged from hospital with a score of 2. Three months later neurological examination disclosed no pathological findings. The case demonstrates the crucial role of interventional procedures in the treatment of severe stroke where intravenous thrombolysis has little prospect of success.
Introduction
A tandem occlusion of the internal carotid artery (ICA) and middle cerebral artery (MCA) due to arterial dissection is a rare event, and systematic prospective studies whether treatment should be endovascular or by means of IV thrombolysis are lacking. We report a successful interventional approach with stent angioplasty of the internal carotid artery and mechanical thrombectomy of the MCA in a patient with arterial dissection of the right ICA and thromboembolic occlusion of the right MCA.
Case Report
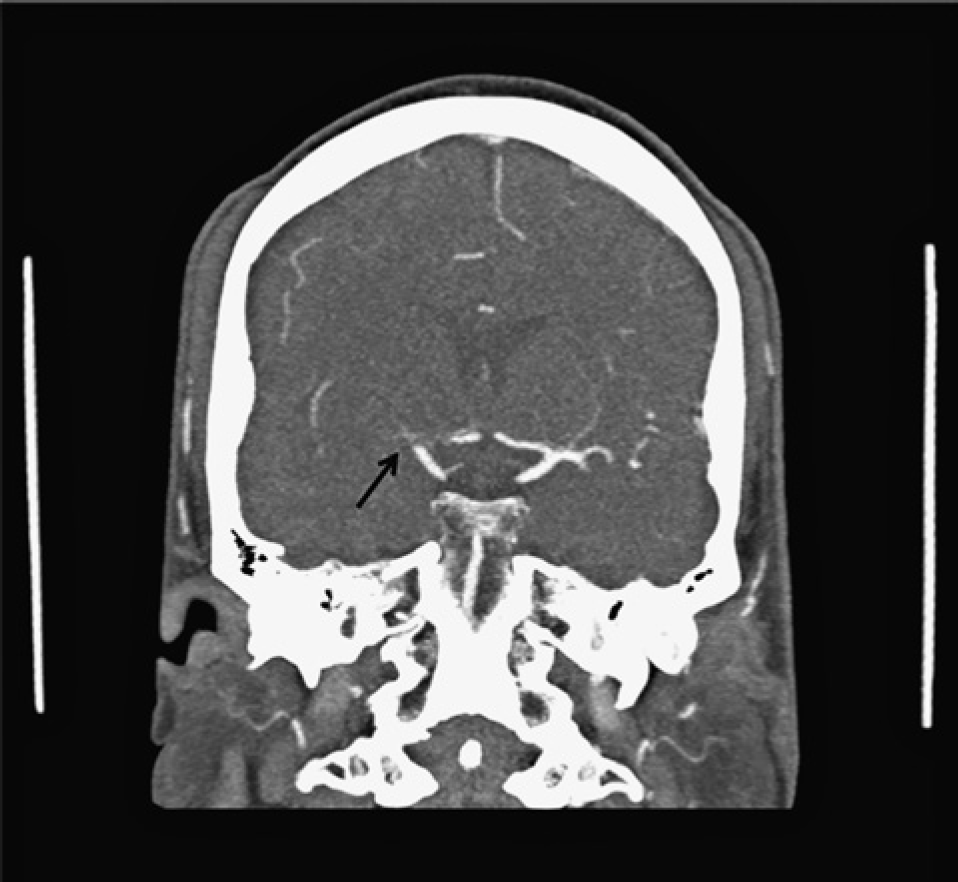
A 59-year-old man was referred to our hospital approximately 30 minutes after acute onset of hemiparesis of the left side during a beach volleyball game. Clinical examination revealed severe dysarthria, sensomotoric hemiplegia of the left side and neglect to the left side (NIHSS score of 19). CT scan of the brain demonstrated a dense media sign on the right side (Figure 1), intracranial CT angiography (CTA) demonstrated an occlusion of the right MCA and presumably of the carotid T (Figure 2). Extracranial CTA also demonstrated an absent contrast filling of the right ICA from its origin which was discussed to be either caused by stasis of blood flow due to distal occlusion or dissection of the internal carotid artery. After interdisciplinary discussion the decision was made for an interventional approach with mechanical thrombectomy of the occluded M1 segment. Thirty minutes before the intervention started, 10 mg rt-PA was administered intravenously as a bridging therapy.
Interventional Procedure
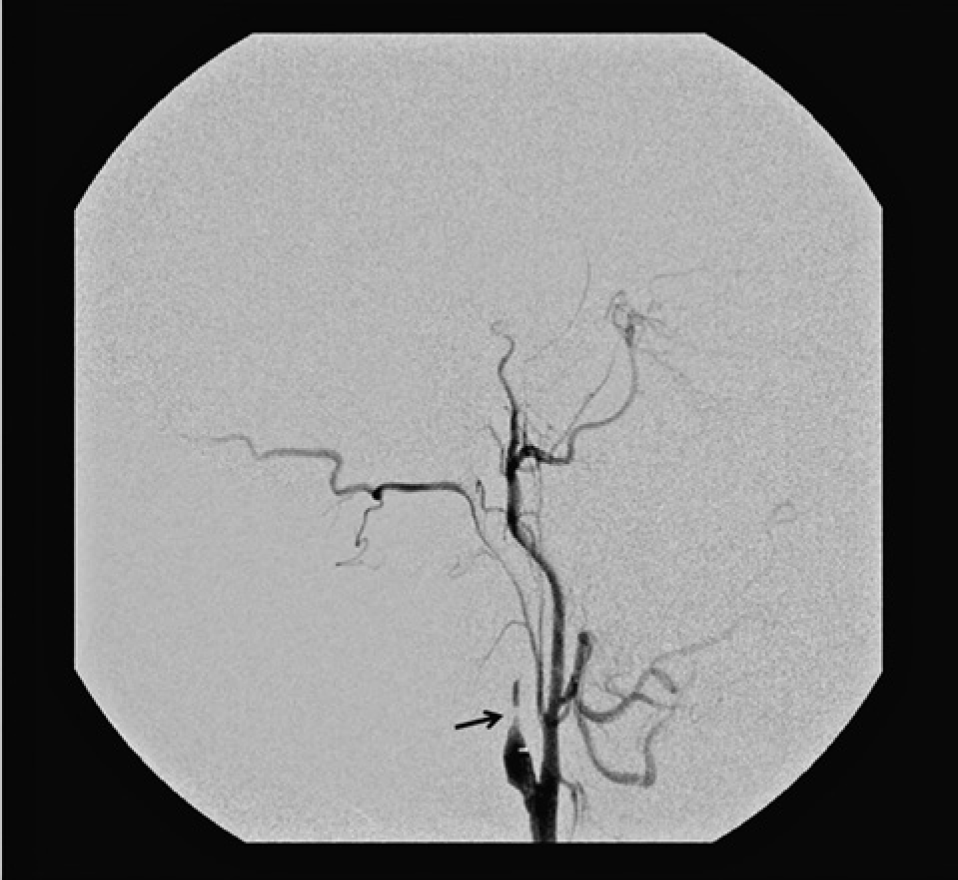
The intervention started approximately two hours after onset of clinical symptoms and was performed under general anaesthesia by two neuroradiologists (MS-H with assistance from AW). After insertion of a 5 Fr sheath (Terumo) into the right common femoral artery, a 5 F vertebral catheter (Terumo) was placed in the common carotid artery. Digital subtraction angiography runs demonstrated a tapered lumen of the origin of the right ICA consistent with an acute dissection (Figure 3).
Initial CT scan of the brain showing a dense media sign on the right side (arrow). CT angiography demonstrates an occlusion of the right middle cerebral artery and presumably of the carotid T (arrow). Tapered lumen of the origin of the right internal carotid artery consistent with an acute dissection (arrow). Occlusion of the middle cerebral artery (arrow).
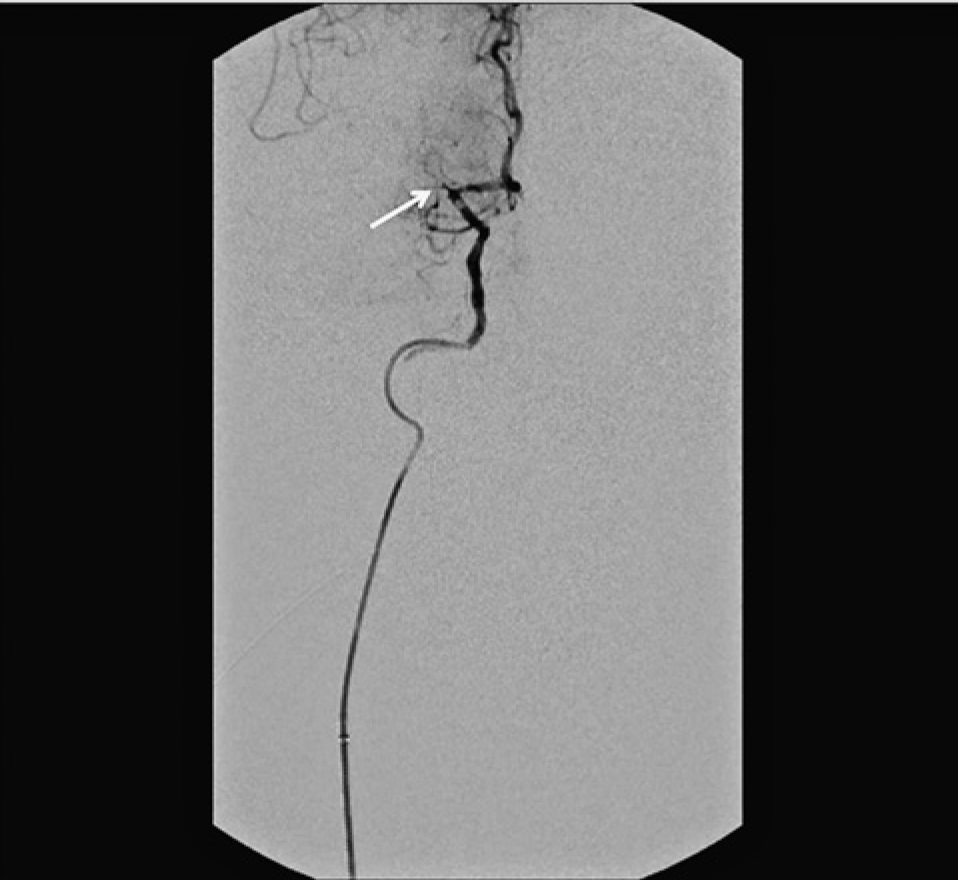
The 5 Fr sheath was then replaced by a 6 Fr and 90 cm long interventional sheath (Terumo) placed in the common carotid artery under guidance of a 0.038 inch and 260 cm long hydrophilic guidewire (Terumo). Then the true lumen of the dissected ICA was carefully probed with a 0.035 inch hydrophilic guidewire (Terumo) and subsequently a 6 F Fargomax catheter (Balt Extrusion) was carefully advanced through the extracranial part of the internal carotid artery. A contrast series demonstrated that the Fargomax catheter was placed in the true lumen and also showed that the MCA was occluded (Figure 4). After that a 300 cm Transend floppy 0.014 inch micro-guidewire (Stryker) was advanced through the Fargomax catheter and was placed with its tip in the anterior cerebral artery.
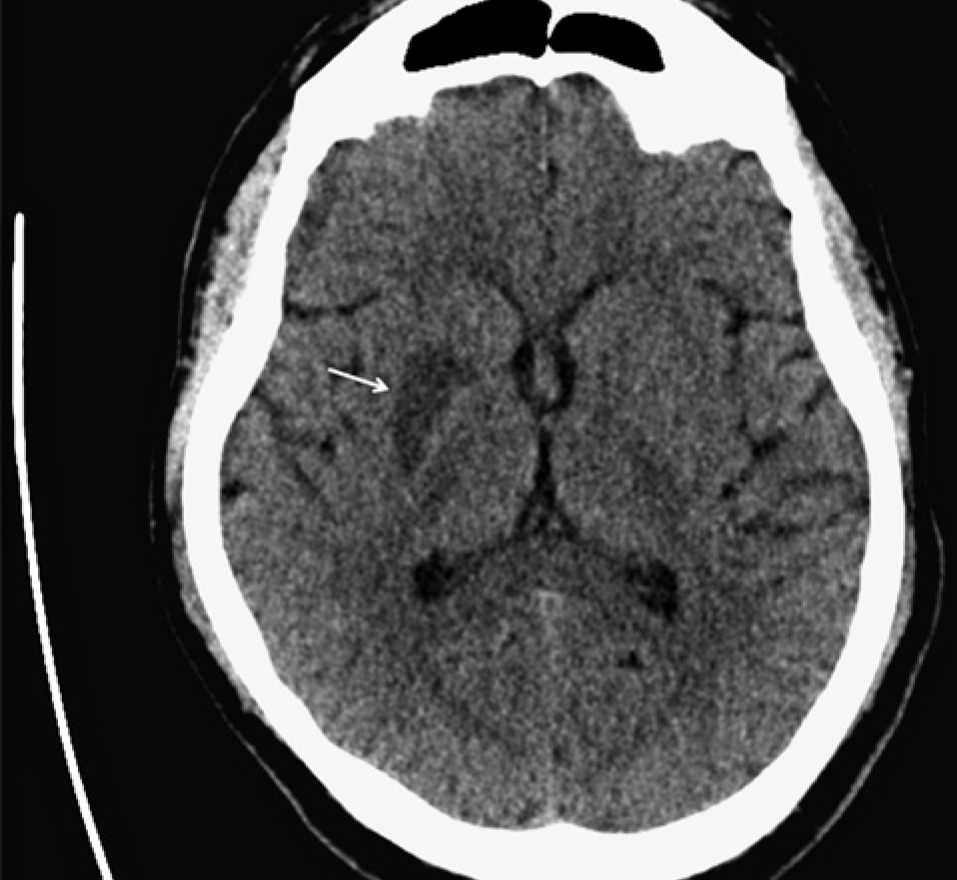
Flow restoration of the internal carotid artery on the right side after deployment of two stents (arrows). Complete recanalization of the right middle cerebral artery after successful clot retrieval with the Solitaire stent (arrow). CT brain scan on the day after intervention showing an infarction of the corpus striatum of the right side (arrow). CT angiography of internal carotid artery stents three months after interventional therapy (arrows).

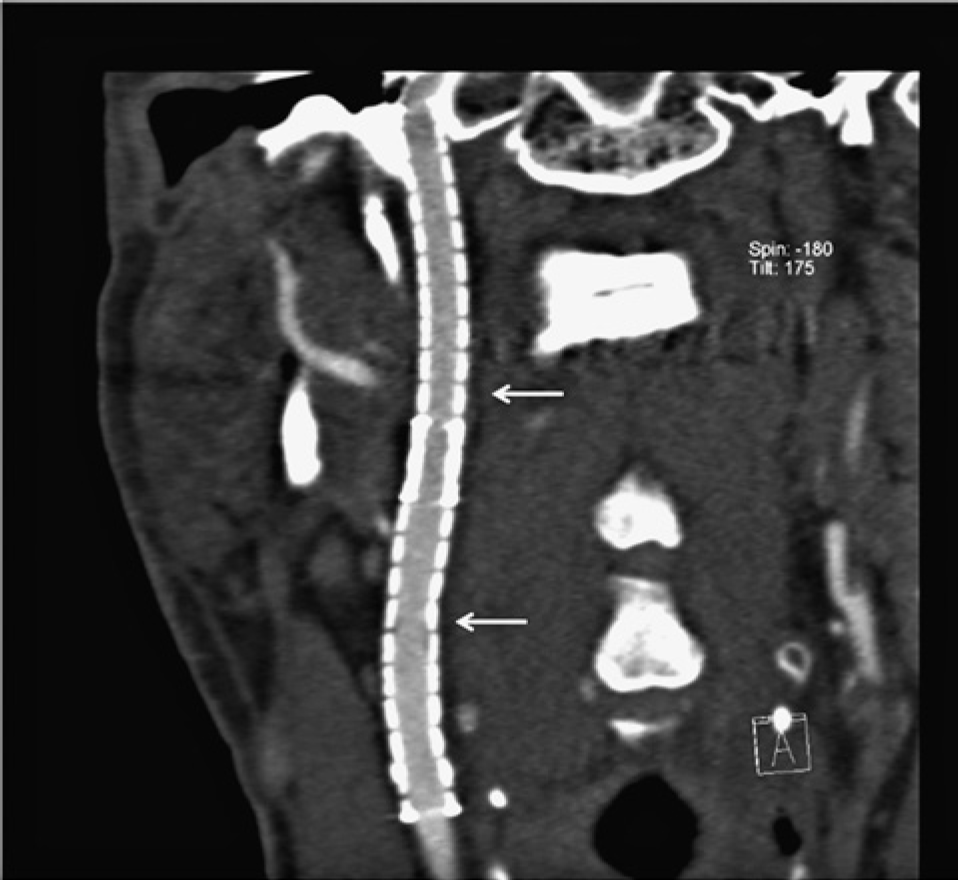
Subsequently, the Fargomax catheter was removed. Over the Transend floppy guidewire, two Protégé RX Stents (eV3) with a diameter of 6 mm and a length of 60 mm were placed in the true lumen of the dissected ICA with a short overlap. After the flow of the ICA was restored (Figure 5), the Fargomax catheter was again placed in the distal part of the internal carotid artery. The right MCA was carefully navigated with a Transend EX 14 0.014 inch microguidewire (Stryker) with its tip placed distally in the M2 segment.
A Prowler Select Plus microcatheter (Cod-man) was placed in the MCA with the tip being distal to the occluded segment, verified by a contrast series. After removal of the mi-croguidewire, a Solitaire stent (eV3) was advanced through the microcatheter and was placed in the occluded part of the MCA. Then, the Solitaire stent was deployed by removal of the microcatheter and flow restoration was documented with a contrast series. After approximately three minutes, the stent was retrieved under continuous aspiration with a 50 ml syringe.
The clot occluding the M1 segment could be retrieved successfully with the first manoeuvre and a control contrast series demonstrated a recanalized MCA (Figure 6).
Finally, dilatation of the ICA stents was performed with a Sterling balloon (Boston Scientific). After the intervention was completed, the common femoral artery was sealed with an 6F AngioSeal vascular closure device (St. Jude Medical).
Further Course
After the intervention the patient was transferred to the intensive care unit. On the first day after therapy, he displayed a high-grade hemiparesis of the left side and Horner's synd rome on the right side. Control CT of the brain conducted the day after interventional therapy demonstrated an infarction of the corpus striatum of the right side but no intracranial haemorrhage (Figure 7). With intense physio and speech therapy, the patient's condition further improved and he was discharged from hospital after 14 days with a mild hemiparesis and hypaesthesia of the left side and a minimal Horner's syndrome of the right side (NIHSS score 2).
The antiplatelet therapy regimen was clopidogrel 75 mg per day for six weeks and ace-tylsalicylic acid 100 mg per day lifelong. After three months, neurological examination disclosed no pathological findings except some disturbances in monopedal jumping (NIHSS score 0). Control CTA after three months demonstrated correct deployment of ICA stents without in-stent stenosis (Figure 8).
Discussion
In case of acute stroke, any treatment has the goal of immediate restoration of blood flow to prevent larger tissue damage of the brain. In the reported case, we faced two issues: a proximal large vessel occlusion due to arterial dissection of the right ICA and a distal thromboembolic occlusion of the right MCA, which was most likely caused by arterio-arterial embolism. As the patient was quickly transferred to hospital and diagnosis was made within three hours after symptom onset, he would have been eligible for the approved standard therapy of intravenous thrombolysis. However, intravenous thrombolysis in tandem occlusions has been shown to have poor outcomes, which holds especially true for arterial dissections, attributable to the inherent hemodynamic compromise 12 . Therefore, we chose an interventional approach. Stenting as a treatment of dissections of the extracranial ICA has been shown to be a safe procedure, as reported by a systematic review 3 . There are further reports on emergency stenting of dissected internal carotid arteries that also demonstrate a favourable outcome in most treated patients4,5. Stroke treatment by means of mechanical thrombectomy is increasingly used and different devices have been developed to date 6,7. A further approach comprises so-called stent retrievers, i.e. fully retrievable self-expanding stents that are deployed at the site of occlusion to catch the thrombus and remove it under continuous aspiration into the guiding catheter. The Solitaire stent was originally designed for the treatment of wide-necked intracranial aneurysms. From the first successful use of the Solitaire stent as a thrombectomy device in the year 2008 8 , many reports now document the safety and feasibility of this mechanical thrombectomy device9,10. As the combined event of an ICA dissection and thromboembolic occlusion of the MCA is a rare finding, systematic prospective randomized studies dealing with the question of whether systemic intravenous thrombolysis or interventional treatment is the better choice are currently lacking. Nevertheless, some recent reports confirm that combined stent-assisted angioplasty and mechanical thrombectomy in acute tandem occlusions is a safe procedure and should be taken into consideration for treatment if an experienced neuroradiologist is available 11,12.