
Abstract
Megalencephalic leukoencephalopathy with subcortical cysts, or Van der Knaap leukoencephalopathy, is a rare disease which is characterised by macrocephaly and neurological disorders with autosomal recessive inheritance. Magnetic resonance imaging is very helpful for determining distinctive findings and distinguishing other diseases. We present the radiological findings of two sisters (aged 6 and 10 years) diagnosed with Van der Knaap leukoencephalopathy.
Introduction
Megalencephalic leukoencephalopathy with subcortical cysts or Van der Knaap leukoencephalopathy is an autosomal recessive disease with macrocephaly and neurological disorders. Magnetic resonance imaging (MRI) of brain demonstrates white matter changes and subcortical cysts which are characteristic findings. 1 We present radiological findings of two sisters (aged 6 and 10 years) diagnosed with Van der Knaap leukoencephalopathy.
Case report
A 6-year-old female patient had been admitted to the paediatric clinic with complaints of difficulty in walking and severe weakness of her left leg. Her family history revealed that her 10-year-old sister also had the same symptoms. The parents of the patients were first-degree relatives.
In physical examination, head circumference of the 6-year-old patient was found to be 56 cm and evaluated as greater than 97 percentile. The head circumference of the 10-year-old patient was found to be within normal limits. Following these findings, two sisters were referred to the radiology department of our hospital for MRI assessment of the brain.
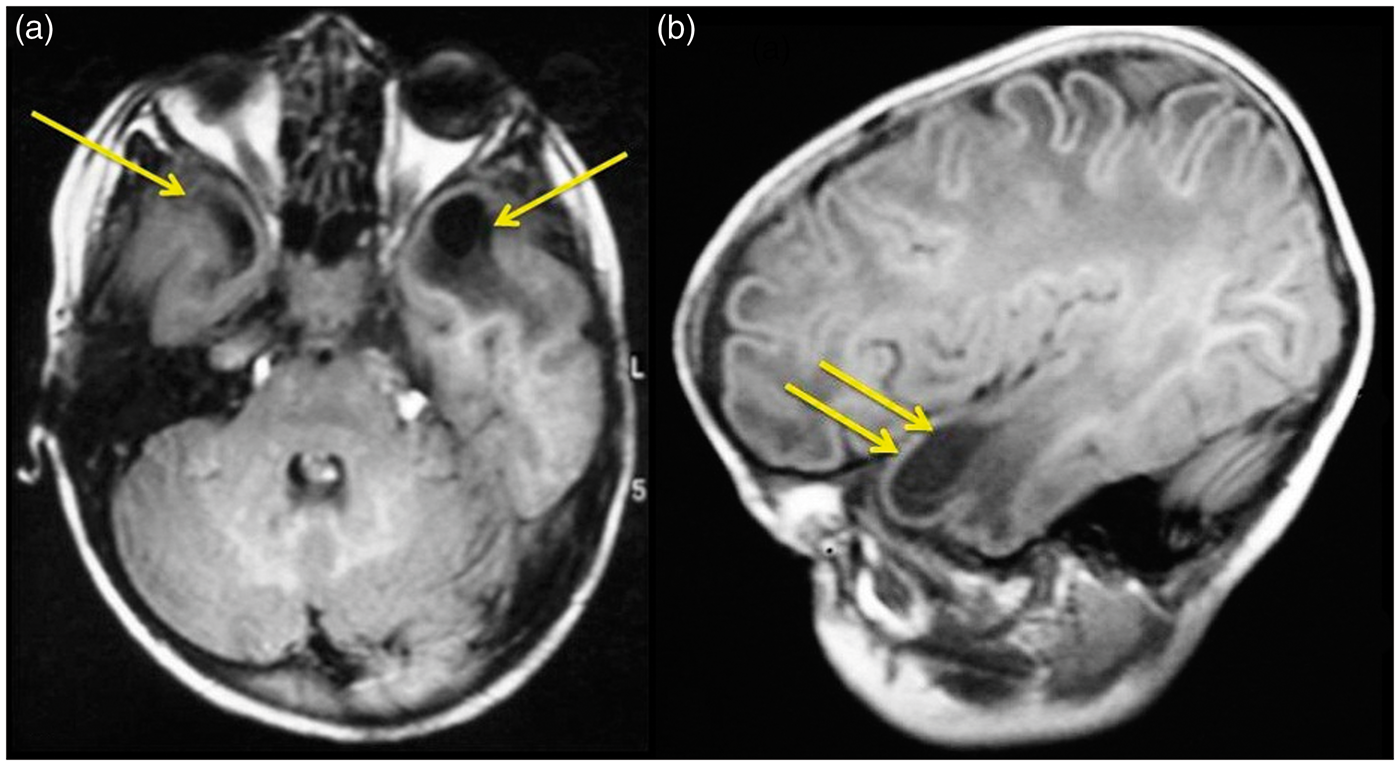
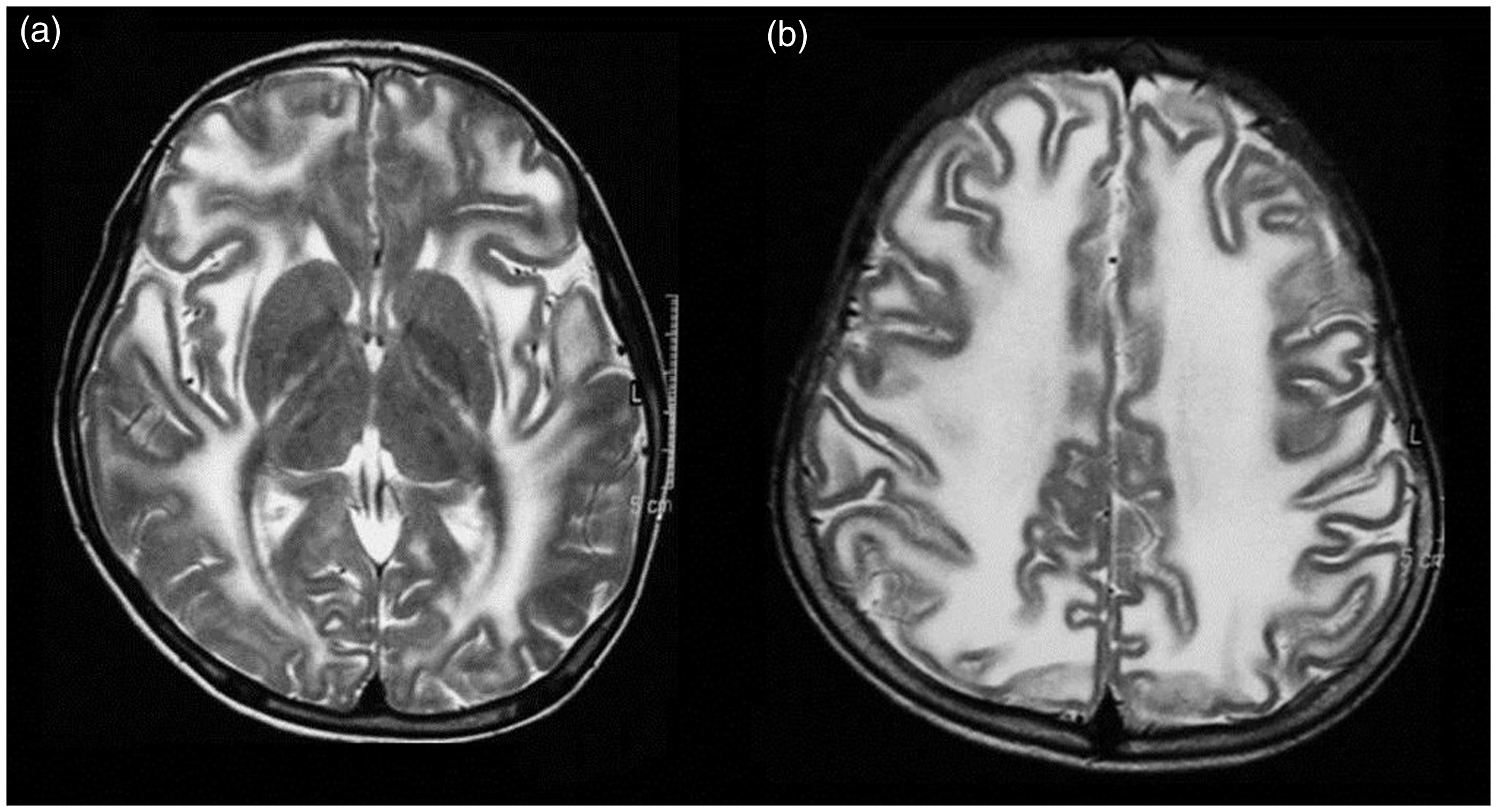
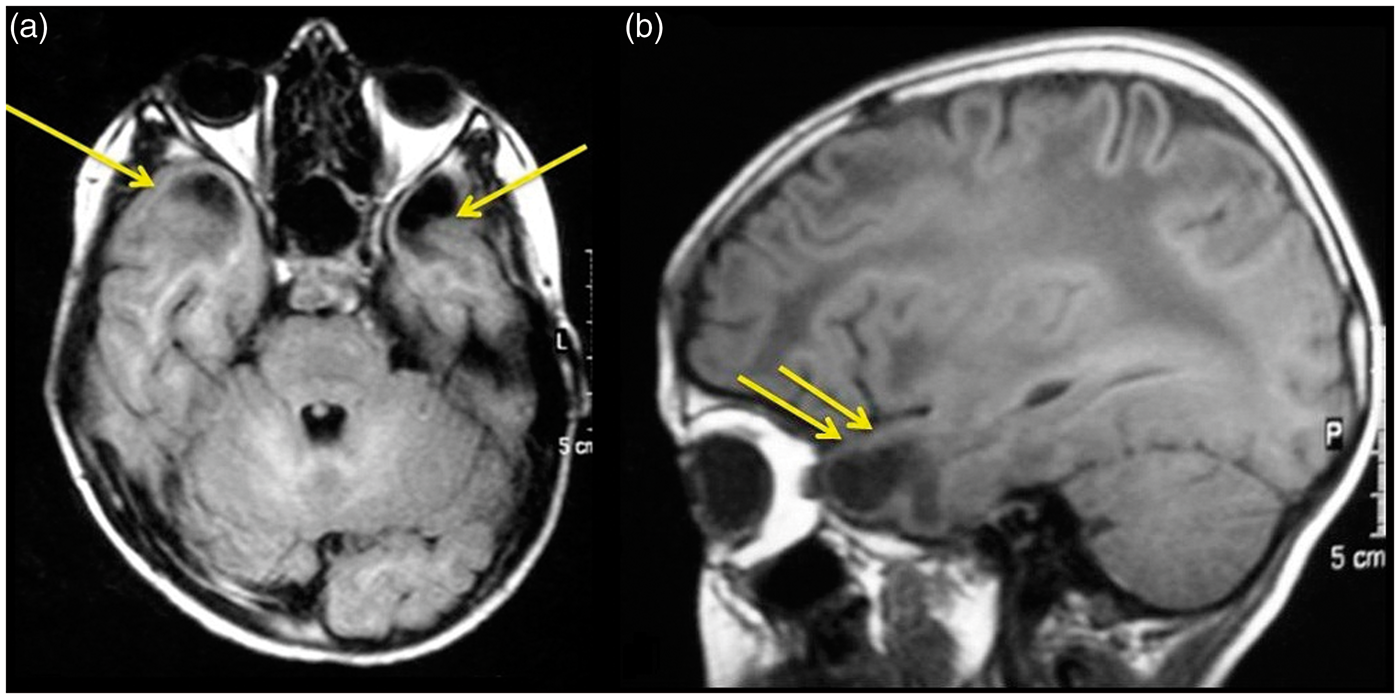
Brain MRI revealed a diffusely increased T2-FLAIR signal intensity in supratentorial white matter (Figures 1 and 3), and subcortical cysts located at anterior temporal lobe in both cases (Figures 2 and 4). MRI also revealed that basal ganglia and brain stem were preserved. With these clinical and MRI findings, both patients were diagnosed with Van der Knaap leukoencephalopathy.
Discussion
Van der Knaap leukoencephalopathy is a syndrome diagnosed by clinical and MRI findings. A distinctive feature of the disease is the quite slow progress of functional impairment, although there is severe involvement of white matter. The frequency of kinship of the parents of the patients and detection of more than one child in the same family as affected by the disease suggest an autosomal recessive mode of inheritance.
1
Our cases are sisters, and this condition supports hereditary nature of the disease.
First case (6-year-old girl), on transverse T2-weighted MR images of different levels ((a) and (b)); symmetrical and diffuse increased intensity spreading to subcortical fibres and involving internal capsule at white matters of both cerebral hemispheres is detected. Signal intensities of basal ganglia are normal (a). First case (6-year-old girl), on transverse FLAIR (a) and sagittal T1-weighted (b) images; hypointensities (yellow arrows) related to paranchymal cystic lesions at both anterior temporal lobes are seen. Second case (10-year-old girl, sister of first patient), on transverse T2-weighted images of different levels (a and b); symmetrical and diffuse intensity increase spreading to subcortical fibres and involving internal capsule at white matters of both cerebral hemispheres is detected. Signal intensities relating to basal ganglias are seen to be preserved (a). Second case (10-year-old girl, sister of first patient), on transverse FLAIR (a) and sagittal T1-weighted (b) images; hypointensities (yellow arrows) related to paranchymal cystic lesions at both anterior temporal lobes are seen.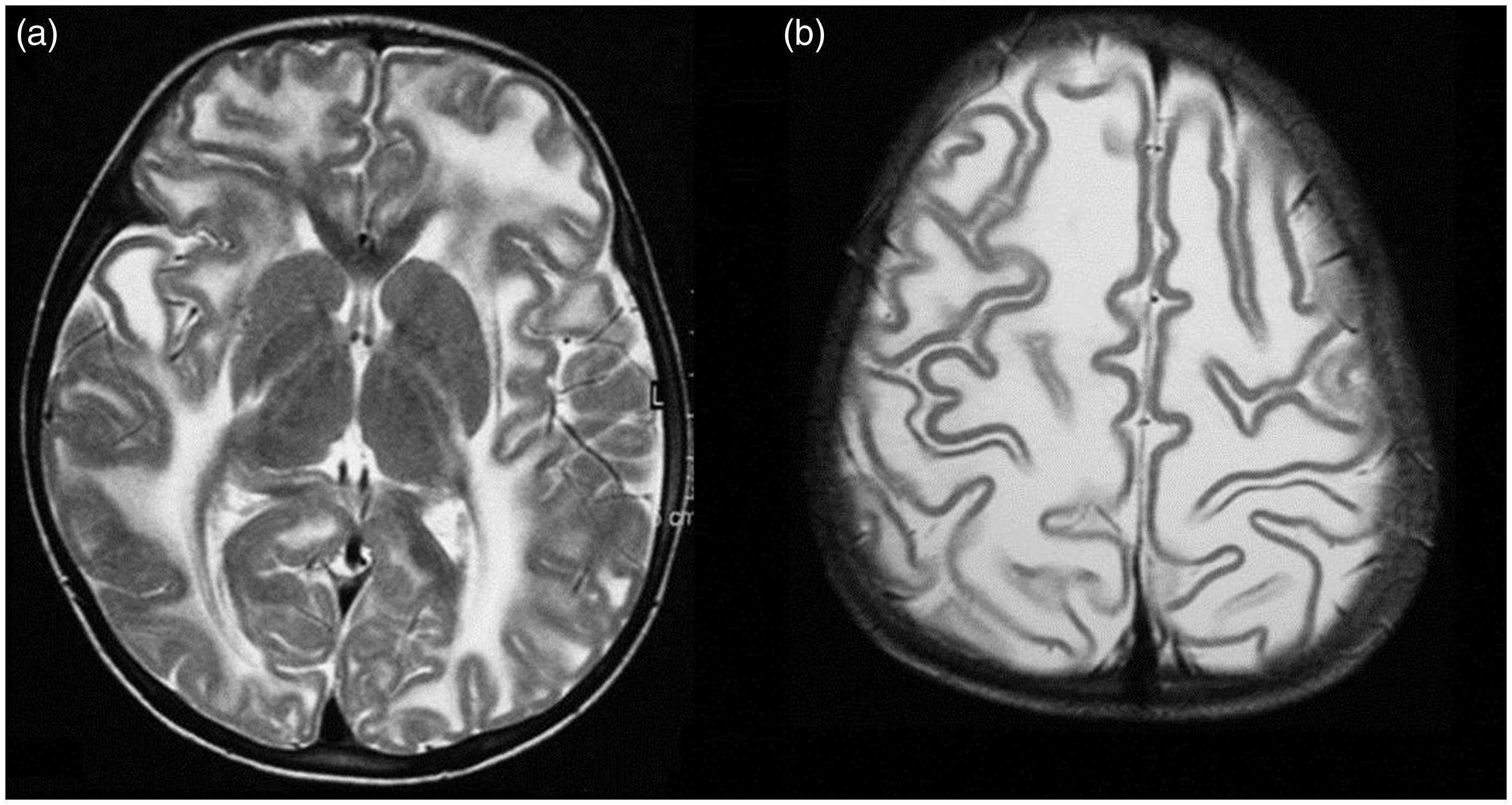
One of the main clinical features of Van der Knaap leukoencephalopathy is macrocephaly. Macrocephaly is often present at birth or develops during the first year of life. Head circumference can be as great as 4 to 6 SD above the mean. 2 Macrocephaly was detected in one of our cases. Initial development is normal, although macrocephaly and severe involvement of white matter exist. Motor functions worsen in the following years due to slowly increasing ataxia and spasticity.2,3 Both of our cases had difficulty in walking. Learning disability exists in half of the patients at primary school age. 4 Extrapyramidal symptoms (e.g. dystonia, athetosis) may occur in some patients at the late stages. Early onset seizures are usually present and respond to antiepileptic therapy.4,5
There is no fine correlation between MRI findings and clinical course of the patients. 6 The characteristic MRI findings of Van der Knaap leukoencephalopathy are cystic degeneration of bilateral anterior temporal and frontoparietal lobes, increase in volume of supratentorial white matter and diffuse involvement characterised with the presence of abnormal signal.7,8 Central white matter structures (corpus callosum, internal capsule and brainstem) are less often affected. Subcortical U fibres are affected in most of the patients. Basal ganglions and thalamus are preserved, although cerebellar white matter and dentate nucleus are minimally affected. Swelling of white matter may diminish in time in some patients; size and number of subcortical cysts may increase and cerebral atrophy may develop. 7 On MRI of our cases, cystic degeneration of the bilateral anterior temporal region and diffuse T2 hyperintensity at cerebral white matter were detected, and these findings are compatible with Van der Knaap leukoencephalopathy.
Other causes of infantile megalencephalic leukoencephalopathy (Canavan disease, Alexander disease, type 1 glutamic aciduria, GM 1 gangliosidosis, L-2-hydroxyglutaric acidemia) differ from Van der Knaap leukoencephalopathy by their clinical, biochemical and neuroradiological features.9,10 Involvement of thalamus and globus pallidus seen in Canavan disease 11 and typical findings detected in Alexander disease (e.g. periventricular contrast enhancement, caudate nucleus and thalamus involvement) 12 were not encountered in our cases. We could rule out L-2-hydroxyglutaric acidemia due to extent of the lesion, and the absence of increased L-2-hydroxyglutaric acid levels in blood, cerebrospinal fluid (CSF) and urine. 13 Multifocal leukoencephalopathies with bilateral anterior temporal cysts have a non-progressive course and macrocephaly does not exist. 14 Bilateral temporal cysts have been reported in a case of subacute sclerosing panencephalitis. 15 Vanishing white matter disease has to be included in the differential diagnosis due to its MRI findings. 16 In this disease, a part of diffusely involved white matter liquefies and gains a signal intensity close that of CSF. It is possible to differentiate the disease from Van der Knaap leukoencephalopathy by the absence of a severe volume increase of white matter, and also by clinical history and typical MRS findings (almost complete disappearance of all metabolites). The clinical and neuroradiological findings in our cases were not compatible with these diseases.
MLC 1 protein, suggested as the cause of Van der Knaap leukoencephalopathy, has been revealed to be expressed by neurons and astrocytes, and it is also suggested that the myelin defect observed in the patients does not exist due to oligodendrocyte dysfunction. 17
To date, a metabolic defect causing Van der Knaap leukoencephalopathy has not be detected. The disease can be diagnosed by clinical and radiological findings, as in our cases and, if possible, verified by genetic analysis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.