
Abstract
The advent of new and acute headaches poses a diagnostic challenge. The differential diagnosis comprises numerous diseases and syndromes, the prevalence of which varies depending on the geographical region. Due to increased magnitudes in international migration, the usual differential diagnostic spectrum has to be enlarged in individual cases. The presented case illustrates this dilemma and shows that, for example, tuberculosis deserves to be taken into consideration.
Introduction
The advent of new and acute headaches poses a diagnostic challenge. 1 The differential diagnosis comprises numerous diseases and syndromes, the prevalence of which varies depending on the geographical region. 1 Due to increased magnitudes in international migration, the usual differential diagnostic spectrum has to be enlarged in individual cases. The presented case illustrates this dilemma and shows that, for example, tuberculosis deserves to be taken into consideration.
Case report
A 27-year-old woman from Indonesia, living in Germany for four years, was seen in the emergency room because of increasingly severe persistent holocephalic headache that did not respond to indomethacin. The headache had started two weeks previously.
At the time of admission she was awake, oriented and showed normal findings on a neurological investigation, including cranial nerves, motor and sensory functions, coordination. Muscle tendon reflexes were equally elicitable at medium response levels in arms and legs. Pathological reflexes, Babinski’s group, were absent. Coordinative tests comprised finger-to-nose test, finger tapping, rebound manoeuvre, heel-to-knee test, Romberg’s, and heel-to-toe walk with closed eyes. Blood pressure, pulse and body temperature were unremarkable. No signs of meningism. There was no history of immunodeficiency, drug abuse or recent travelling. Body temperature was slightly elevated.
A cranial computed tomography (CT) scan was performed in the emergency department to exclude an intracranial bleeding. The images showed a space occupying hypointense cerebellar lesion with indistinct margins (Figure 1(a)). The fourth ventricle was restricted, and slight widening of the ventral horns of the lateral ventricles was taken as a sign of aqueductal stenosis. Thoracic X-rays taken in the supine position were normal. The cranial MRI taken at the intermediate care unit on the following day displayed multiple small confluent round or oval shaped and centrally hypo-intense lesions within the left cerebellar hemisphere (Figure 1(b)–(e)). The margins of these nodules showed strong contrast enhancement with marked perilesional oedema in T2-weighted images (Figure 1(b)–(e)). The mean apparent diffusion coefficient (ADC) of the lesions was 1.03 × 10−3 mm2/s and the minimal value was 0.91 × 10−3 mm2/s (Figure 1(g)–(i)). The N-acetyl-aspartic acid (NAA) peak was normal as demonstrated by MR-spectroscopy, whereas the amplitudes of the lactate/lipid peak complex and of the choline peak were increased relative to the NAA peak (Figure 1(f)).
Cerebral imaging findings in the patient. (a) Computed tomography revealed a hypodense cerebellar lesion. (b) T2-weighted image showed cerebellar oedema. T1-weighted images without (c) and with (d) and (e) contrast medium demonstrated multiple small confluent round or oval shaped and centrally hypointense lesions within the left cerebellar hemisphere. (f) MR-spectroscopy showed an increase of the amplitudes of the lactate/lipid peak complex and of the choline peak. No diffusional restriction was seen ((g)–(i)).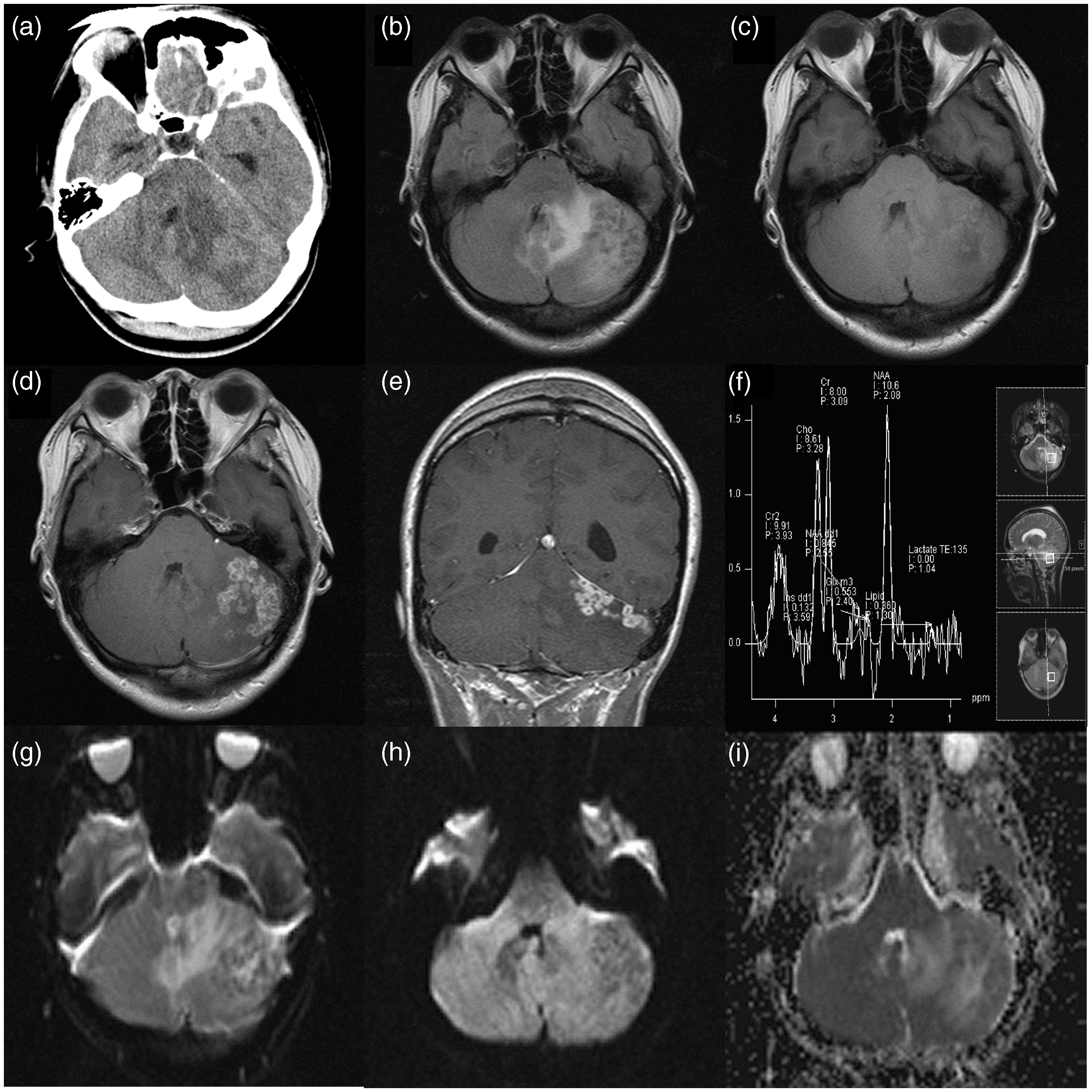
The differential diagnosis comprised an inflammatory (e.g. parasitic) pathogenesis as well as a neoplastic origin. Among the laboratory parameters, there was a minimal increase of the C-reactive protein level of 8.4 mg/l (reference <5 mg/l). The blood cell counts and the other blood serum parameters were within normal limits, including electrolyte values, creatinine, transaminase values, alkaline phosphatase, total protein, quick partial thromboplastine time. Microbiological and serological investigations for the presence of helminthosis were negative. Likewise the serological screening tests were negative for: cytomegalovirus, HIV, Borrelia, Treponema pallidum, toxoplasma, Aspergillus and Echinococcus. Ventricular cerebrospinal fluid that was taken after placement of a ventricular drainage was colourless and clear and showed normal values for cell count, cytology and protein values.
In order to clarify the nature of the cerebellar lesions, a biopsy was taken. Histological analysis revealed the picture of a necrotizing granulomatosis (Figure 2). Within necrotic areas, epithelioid cells were seen. Furthermore, there were multiple small and partly confluent granulomas. Ziehl–Neelson staining did not reveal the presence of acid-resistant bacteria. Tuberculosis was detected neither by polymerase chain reaction (PCR) nor by culture in cerebrospinal fluid (CSF), sputum, aspirates from bronchial lavage and gastric fluid. However, the PCR investigation of post bronchioscopic sputum revealed the presence of Mycobacterium tuberculosis.
Histopathological examination of the lesion showed a granulomatous inflammation with a central necrosis (haematoxylin and eosin stain).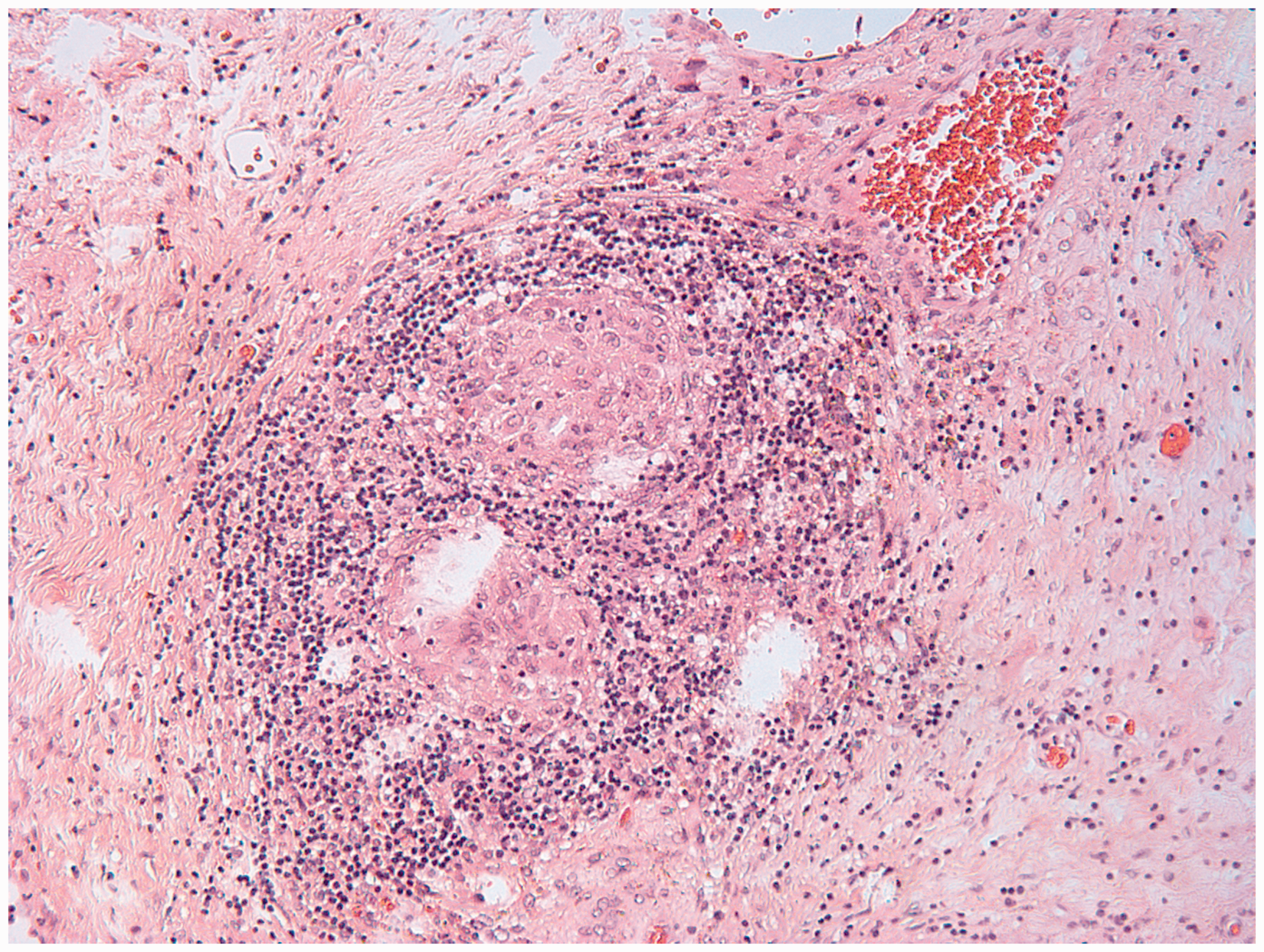
The thoracic CT scan demonstrated multiple confluent blotchy apical localized lesions (not shown). A tuberculostatic therapy was initiated. The headache improved within three weeks. The tuberculostatic therapy was ended after one year. The patient was in good general condition within the observation period of three years.
Discussion
In 5–15% extrapulmonary tuberculosis manifests with central nervous system (CNS) lesions. 2
CNS tuberculosis develops in two steps: subpial or subependymal lesions, the so-called Rich-foci, result from haematogenous spread. 3 These minute lesions can grow to form tuberculomas or tuberculous abscesses, 4 or they can rupture into the subarachnoid space giving rise to tuberculous meningitis. 3
Both subacute headache and the imaging findings should be suggestive for cerebral tuberculosis. However, in the present case suspicion of a cerebral tuberculosis was raised upon the pathoanatomic findings obtained from the biopsied cerebellar tissue. The definitive diagnosis came from the PCR results of post-bronchioscopy sputum, and was supported by thorax CT findings. Occlusive hydrocephalus is a classical manifestation of tuberculous meningitis. 5 In the present case, it was rather due to compression of the aqueduct by the cerebellar enlargement and not to meningitis, which could not be detected by CSF investigation.
In the present case, headache was presumably due to the increase in intracranial pressure resulting from cerebellar oedema and hydrocephalus. As in the present case, tuberculous CNS lesions may pose diagnostic pitfalls.
Therefore, radiological investigations play an important role in the clinical evaluation of some patients. As reported previously, MRI is highly sensitive for the detection of CNS lesions but might have a low specifity. 6 According to the literature, tuberculous CNS lesions are in T1-weighted images hypo- isointense with contrast agent enhancement and in T2-weighted images hypoisointense with perilesional oedema, like the presented case. These imaging features are non specific and other disorders, such as gliomas, metastatic tumours, abscesses, cysticercosis, mycotic and other granulomas can mimic the radiological features of tuberculous lesions. 7
In contrast to the present case, the majority of the reported tuberculous lesions were located supratentorial in the hemispheres. 7
To differentiate the tuberculous lesions from brain metastases perfusion weighted imaging might be useful. It has been shown that tuberculous lesions have significant lower rCBV ratios than metastatic lesions, whereas diffusion weighted imaging was not able to discriminate between the two groups. 8 Unfortunately, this imaging modality was not performed for the patient. According to previous reports, diffusion weighted imaging may also be helpful to differentiate several brain lesions.9,10 It was suggested that the ADC minimal value of 0.98 × 10−3 mm2/s was able to differentiate between tuberculous lesions and high grade glioma with a sensitivity of 93.8% and a specifity of 93.7%. 11 In our case, however, the lesions had lower ADC minimal values and, therefore, can be misdiagnosed as a glioma.
MR-spectroscopy is another modern imaging technique to characterize enhancing lesions of the brain. Peng et al. found that the enhancing rim showed a normal-to-mild elevation of the choline peak and a reduction of the peaks of creatine and NAA. 11 Furthermore, a choline/creatine ratio below 3.16 had a sensitivity of 87.5% and a specifity of 68.7% for the differentiation of high grade glioma and tuberculous lesions. 11 Our case also showed a reduced choline/creatine ratio. In a recent study, singlet peak at 3.8 ppm was found in 69% of the tuberculous lesions and only in 10% in the malignant tumour cases, which might be a useful new biomarker for diagnosis. 12 In our case a similar peak is notable, underlining the importance of this new finding. Furthermore, MR-spectroscopy might be useful to differentiate tuberculomas from neurocysticercosis, which is the most common inflammatory cause for cerebral granuloma. 13 Tuberculomas showed a high peak of lipid, more choline and less NAA than neurocysticercosis. 13
Delayed diagnosis seems to be frequent, especially when the usual microbiological tests do not support the diagnosis.3–5,14 Therefore, the advanced imaging techniques might help with the clinical evaluation of the cerebral lesion. However, the diagnosis should not be delayed and upon suspicion the proper antimycobacterial chemotherapy be started. In the present case, tuberculostatic treatment led to the rapid improvement and cure of this life-threatening disease. 4
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.