
Abstract
Inflammatory pseudotumor (IP) is an uncommon idiopathic lesion that often imitates malignancy clinically and radiologically. Inflammatory pseudotumors have been found to occur in various sites but rarely in the head and neck. The histopathology, imaging, and treatment of three unique cases of head and neck inflammatory pseudotumors are described in this case series. Patients in Cases 1 and 2 presented with right level II neck mass and left parotid tail mass, respectively. The patient in Case 3 presented with otalgia, jaw pain and trismus, and a left parapharyngeal space mass. The tumors in Cases 1 and 3 significantly decreased in size with tapered courses of oral corticosteroids. The tumor in Case 2 was surgically excised without disease recurrence. Malignancy must be ruled out with incisional or excisional biopsy. Treatment includes surgical excision, oral corticosteroids, or both. The literature shows that radiotherapy and small-molecule inhibitors may be promising alternatives.
Introduction
First characterized by Brunn in 1939, 1 inflammatory pseudotumor (IP) is an exceedingly rare benign condition that often presents as a locally invasive mass. IP is named for its ability to mimic invasive malignancies on clinical presentation, imaging, and histology. IP most often occurs in the lungs and the orbit, with only 15% occurring in the nonorbital head and neck region.2,3 Here we describe three unique cases of extraorbital IPs in the head and neck, with discussion of diagnostic and management considerations.
Case reports
Case 1
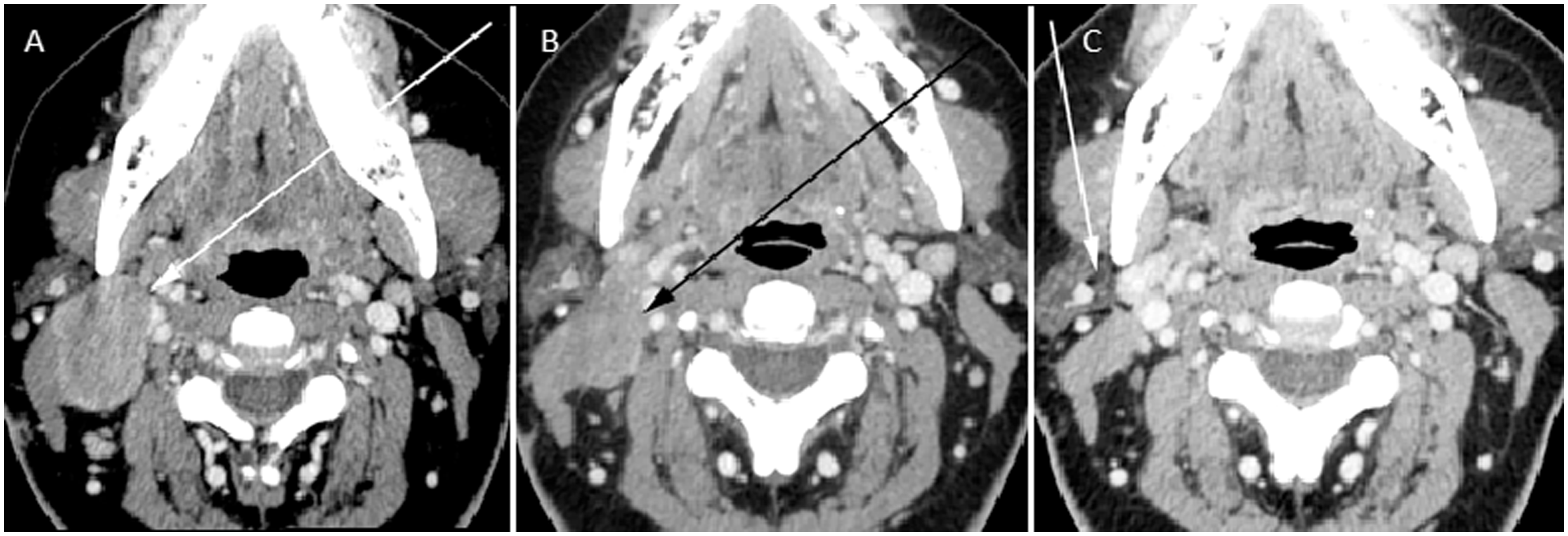
A 46-year-old woman with past medical history of diabetes mellitus presented with a progressively enlarging and painful right neck mass. Computed tomography (CT) imaging showed a 4 cm solid right level II neck mass (Figure 1(a)) and an adjacent 2.5 cm mass (Figure 1(b)). 18-Fluorodeoxyglucose positron-emission tomography (FDG PET) imaging revealed the dominant mass to be intensely FDG avid (Figure 1(e)). Multiple ultrasound-guided fine-needle and core biopsies of the mass revealed dense fibrous tissue and skeletal muscle with chronic inflammation, with no evidence of malignant cells or lymphoma. Incisional biopsy was performed with pathology showing densely sclerotic tissue and multifocal dense lymphoplasmocytic infiltrate without evidence of malignancy. Scattered intermixed eosinophils and histiocytes with occasional multinucleated giant cells were present. Immunohistochemical studies showed CD3 + and CD20 + cells, indicating mixed T-cells and B-cells. A subset of the cells were positive for immunoglobulin (Ig)G4 (20% IgG4/IgG ratio) but not definitive for IgG4-related sclerosing disease. The patient was started on a tapered course of oral prednisone. Three months later she reported an improvement in her neck pain and swelling, and CT imaging showed a 50% decrease in the size of the mass. Two additional courses of steroids were administered, with progressively decreasing mass size and eventual resolution of symptoms (Figure 2).
A 46-year-old woman with inflammatory pseudotumor of the right level II neck. (a) Axial CT scan of the neck with contrast reveals a 4 cm mass (arrow) as well as adjacent (b) abnormal shaped 26 mm lymph node with increase peripheral enhancement (arrow). Surgical changes are noted superficially to this abnormal lymph node overlying the sternocleidomastoid muscle. (c) Ultrasound imaging of the right level II neck mass (arrow) reveals a well-defined hypoechoic lesion. (d) Color Doppler flow imaging overlaid on the gray-scale ultrasound image of the right level II mass (arrow) reveals increased flow to the mass. (e) FDG PET CT imaging displays significant hypermetabolism of the mass (arrow). CT: computed tomography; FDG PET: 18-fluorodeoxyglucose positron-emission tomography. A 46-year-old woman with inflammatory pseudotumor of the right level II neck. (a) Axial CT scan of the neck with contrast three weeks after presentation shows no appreciable interval change in the right level II neck mass (arrow). (b) Repeat axial CT scan of the neck with contrast four months following presentation and following a course of oral tapered corticosteroids reveals modest improvement in size of the lesion (arrow). (c). Reassessment CT scan of the neck with contrast eight months from presentation and after a total of three courses of oral tapered corticosteroids shows resolution of the right level II neck mass. CT: computed tomography.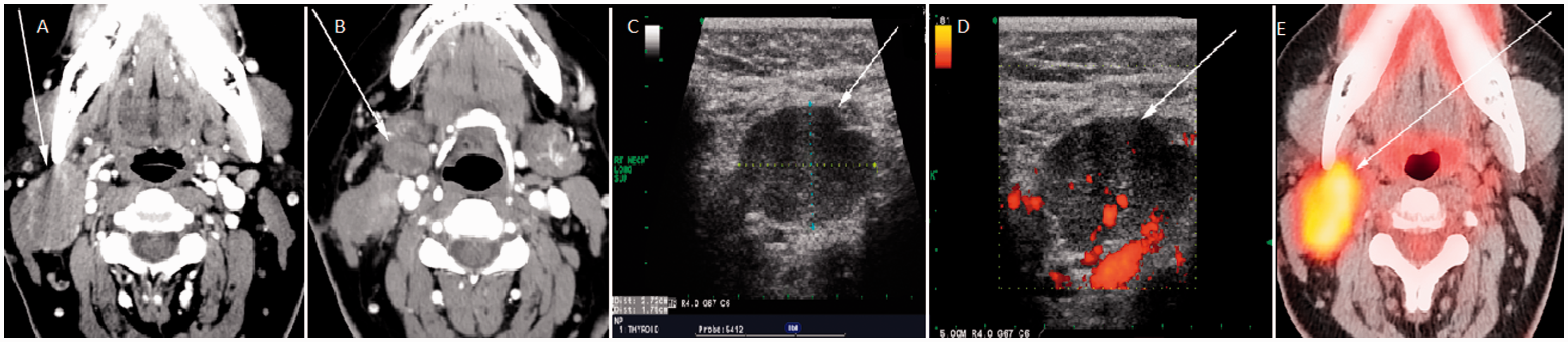
Case 2
A 41-year-old male with a six-week history of enlarging 3 cm left parotid tail mass presented with neck swelling and minimal tenderness that did not improve with two weeks of Amoxicillin/clavulanic acid followed by an additional 10 days of clindamycin. CT scan showed a left level 1B multilobulated neck mass between the parotid tail and submandibular gland that extended superficially to the platysma muscle (Figure 3(a) and (b)). Fine-needle aspiration (FNA) and core needle biopsy illustrated acute and chronic inflammation with histiocytes, granulation tissue, and fragments of skeletal muscle, but malignant cells were absent. Excisional biopsy showed spindle cell proliferation with chronic lymphoplasmacytic infiltration and acute inflammation, favoring an infectious or inflammatory myofibroblastic process. Flow cytometry and immunohistochemical stains showed a polytypic plasma and B-cell population without evidence of lymphoma or IgG4 disease. Tissue cultures were positive for Aggregatibacter actinomycetemcomitans. CT scan 10 months post-excision showed no evidence of disease (Figure 4).
A 41-year-old male with inflammatory pseudotumor of the left submandibular space. (a) Axial and (b) coronal CT scan of the neck with contrast shows a 3 cm left submandibular mass (arrow) adjacent to the parotid tail with inflammatory stranding of the surrounding soft tissues and thickening of the overlying platysma muscle. (c) Gray-scale ultrasound imaging of the mass (arrow) reveals a well-defined, largely hypoechoic mass with (d) mildly increased flow (arrow) on overlaid color Doppler imaging. CT: computed tomography. A 41-year-old male with inflammatory pseudotumor of the left submandibular space. Baseline imaging (a) CT scan of the neck with contrast reveals the left submandibular space mass and surrounding inflammatory changes (arrow). (b) Repeat CT scan of the neck with contrast four months after surgical excision shows post-operative inflammatory changes with no evidence of residual tumor. (c) Surveillance imaging approximately 22 months after presentation shows no evidence of disease. (d) Hematoxilin and eosin stain showing dense fibrosis and inflammation adjacent to the salivary gland (e). Higher power illustrating germinal center formation. CT: computed tomography.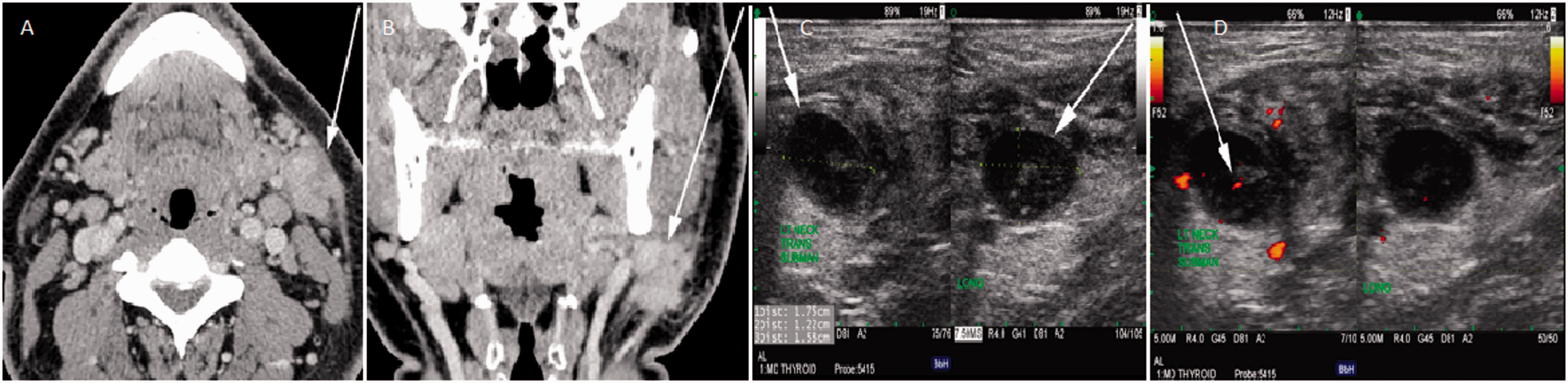

Case 3
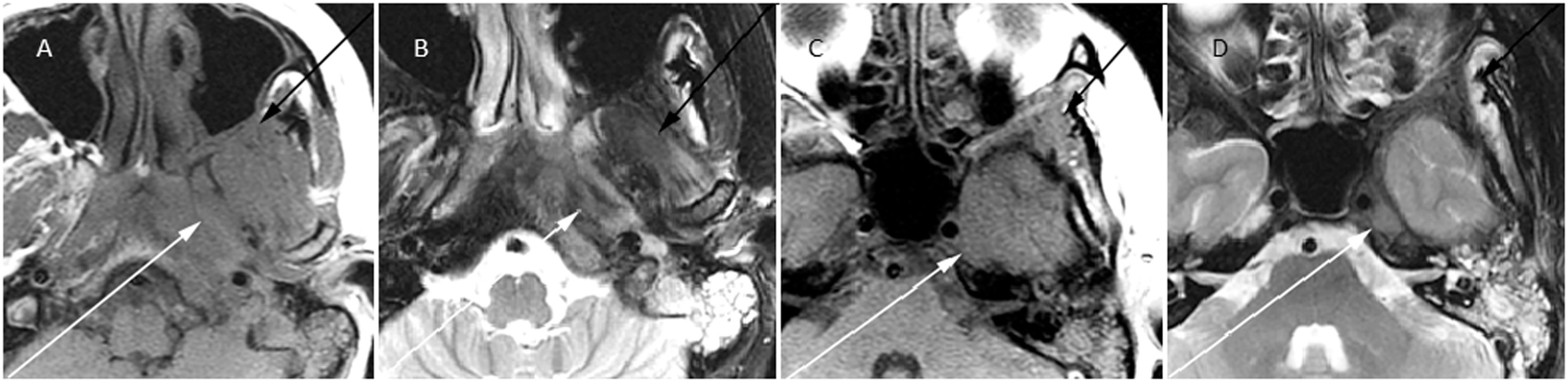
A 32-year-old female with no significant past medical history presented with left otalgia, jaw pain, and trismus. She received several courses of antibiotics for treatment of left otitis media. CT and magnetic resonance imaging (MRI) revealed a 3 cm left parapharyngeal space mass extending to the adjacent nasopharynx and skull base with left neck level Ib lymphadenopathy (Figures 5 and 6). CT-guided biopsy of the mass suggested fibromuscular connective tissue with no evidence of malignancy. FNA and core needle biopsies of enlarged left neck lymphadenopathy revealed polymorphous lymphoid population consistent with reactive lymph nodes. Endoscopic biopsies of the nasopharynx, pterygoid musculature, pterygopalatine fossa, and left skull base revealed a fibroproliferative inflammatory process with fibroblastic proliferation, fibrous stroma, and scant lymphocytic infiltrate. Immunohistochemical studies of these specimens revealed negative CD20, CD3, CD30, CD68, lysozyme, κ, and λ stains, excluding the possibility of a hematolymphoid neoplasm. The patient was prescribed a two-month course of tapered oral prednisone, whereupon she had significant improvement in pain and trismus.
A 32-year-old female with inflammatory pseudotumor of the left masticator space. Axial image (a) and coronal reformat (b) of a CT scan of the neck with contrast displays a non-enhancing infiltrative mass (arrow) centered in the left masticator space with extension along the Eustachian tube, ipsilateral longus coli muscle and skull base. ((c)–(f)) Hematoxilin and eosin stain showing dense fibrotic stroma with interspersed inflammatory infiltrate. CT: computed tomography. A 32-year-old female with inflammatory pseudotumor of the left masticator space. Axial T1WI (a) and T2WI (b) of the left masticator space at the level of the condyle of the mandible better delineates the abnormality seen in Figure 5 with isointense (T1) and hypointense (T2) abnormality extending throughout the muscles of the masticator space (black arrows), along the Eustachian tube and the left petrous bone and carotid space (white arrows). Axial (c) T1WI and (d) T2WI of the left skull base at the level of the internal auditory canal shows the abnormality extends along the left sphenoid bone (black arrows) and the carotid space at the petrous apex (white arrow). T1WI: T1-weighted imaging; T2WI: T2-weighted imaging.
Discussion
IP is rare, and is often considered a diagnosis of exclusion related to idiopathic inflammation. Since patients with IP generally present with clinical and radiological features concerning for malignancy, the first priority is to establish a diagnosis. In Cases 1 and 3, incisional biopsy was required for diagnostic purposes. Complete excision would have resulted in significant morbidity, including resection of cranial nerves, major blood vessels, and adjacent muscles. Diagnostic incisional biopsy was followed by corticosteroids, which resulted in a significant clinical and radiographic response (Case 1). In Case 2, the tumor was excised completely with minimal morbidity.
Within the spectrum of IP, there are a variety of disease entities. IgG4 sclerosing disease is one such subtype that involves lymphocytes, IgG4-positive plasma cells, and fibrosis. This has been reported in several sites in the head and neck and has a favorable response to corticosteroids if diagnosed early. 4 Centers for Disease Control (CDC) criteria for IgG4 disease requires: a clinical exam showing localized swelling, blood studies showing elevated serum IgG4, and histology showing lymphocyte and plasmacyte infiltration with IgG4 + /IgG + cells > 40%. 5 The patient in Case 1 displayed localized tissue swelling and histopathologic exam with lymphocytic infiltrate, but an IgG4/IgG cell ratio of only 20%. Although these findings are not consistent with the diagnosis of IgG4 disease, the patient did respond to multiple courses of corticosteroids, which is characteristic of IgG4 disease.
Other disease subtypes within the umbrella of IP include benign tumors such as calcifying fibrous tumors as well as inflammatory myofibroblastic tumor (IMT). More aggressive and malignant tumors with similar histopathologic features include IMT-like de-differentiated liposarcoma and Epstein–Barr virus (EBV)-associated IP-like follicular dendritic cell tumor. Numerous studies have attempted to characterize and prognosticate these IP subsets. Coffin et al. showed that half of IMTs express cytoplasmic anaplastic lymphoma kinase (ALK), a receptor tyrosine kinase. 6 All patients with metastatic IMTs were ALK negative. Furthermore, nuclear expression of p53 occurred in 80% of IMTs, but only in 25% of the metastatic subset. As a result, ALK and p53 expression may predict a favorable prognosis. On the other hand, presence of ganglion-like cells, aneuploidy, and perinuclear ALK expression portend a more aggressive course.7,8
Infection, trauma, and foreign bodies are among the numerous etiologies that may be involved in the pathogenesis of IP. Organisms such as mycobacteria, Rhodococcus equi and Klebsiella rhinoscleromatis have been shown to cause IPs.9,10 The tissue culture in Case 2 grew A. actinomycetemcomitans, an organism found in periodontal disease. Case reports have demonstrated this bacteria to occur in association with a mediastinal mass imitating malignancy. 11 Actinomyces, a closely related species, has been implicated in submandibular IP mimicking scrofula. 12 These microbes incite inflammation, resulting in the characteristic pathology seen in Case 2: spindle cell proliferation with chronic lymphocytoplasmic infiltration along with atypical epithelioid histiocytes (Figure 4(d) and (e)).
The most critical feature of IP on pathologic exam is the presence of spindle cells, plasma cells, and lymphocytes. 10 Fibroblasts, myofibroblasts, histiocytes, and inflammatory infiltrate may also be present. 13 In a literature review of 84 cases of IPs, three basic patterns were recognized: (a) myxoid, vascular, and inflammatory; (b) spindle cells with lymphocytes and plasma cells; and (c) dense collagenous type resembling scar tissue. However, as opposed to hematologic malignancy, mitotic figures and necrosis are usually absent. 10 Pathology in Cases 1 and 3 showed densely sclerotic/fibrous tissue, whereas pathology in Case 2 showed the classic spindle cell proliferation with chronic lymphoplasmacytic infiltration and acute inflammation. Lymphocytic infiltration, the seminal feature of IP, was present in all of the cases.
Immunohistochemical exam of IP often reveals positive stains for cytokeratins, smooth muscle actin, ALK, CD20, and an increased population of IgG4-positive plasma cells. 10 Immunostaining of Case 1 revealed CD3+, CD20+, CD138+, and IgG4+, indicating mixed populations of polytypic B- and T-cells without evidence for malignancy. Similar to Case 1, flow cytometry and staining of tissue obtained in Case 2 revealed a polytypic plasma and B-cell population without evidence of lymphoma or increased plasmacytic dendritic cells. Immunohistochemical studies of the mass in Case 3 showed negative CD20, CD3, CD30, CD68, lysozyme, κ, and λ stains, excluding hematological neoplasm. The absence of CD3 and CD20 staining in Case 3 underlines the scarcity of B- and T-cell populations within the mass, which was composed mostly of fibrous stroma and collagenous material (Figure 5(c) and (d)).
IP is nonspecific on imaging and presents as an infiltrative soft tissue mass, which can be mistaken for a variety of disease processes. Plain radiographs can display regional changes including hyperostosis or bony erosion, suggesting a destructive process. The lesions on ultrasound are variable and may display decreased echogenicity (as in this case), or even increased echogenicity. Doppler ultrasound can display patterns of hyper-vascularity (as seen in Figures 1(d) and 3(d)). 10 CT findings are nonspecific, and can be seen as homogeneous (Figure 3(a)) or heterogeneous (Figure 2(a)), as well as variable densities compared to the surrounding skeletal muscle. The lesions are typically seen as T1 and T2 hypointense on MR imaging (Figure 6). T1-weighted imaging following gadolinium contrast typically reveals marked enhancement.
Orbital IPs present with fat infiltration, edema, and bone remodeling. 14 Sinonasal IPs can be more aggressive; bony erosion and subsequent remodeling and hyperostosis are often present. Temporal bone IPs present with destruction of the mastoid but sparing of the inner ear and ossicles, which helps to rule out a malignant process. Dural thickening, enhancement, or calcification may be visualized. 15 Neck soft tissue and parapharyngeal IPs (as seen in Case 1 and 3, respectively) are exceedingly rare and have not been well described. Pathologic lymph nodes, when they occur (see Case 1), present with homogeneous attenuation and enhancement on CT. T2-weighted MRI can show hypointense lymph node involvement. 16 Alternative modalities such as FDG-PET have been implemented with some success. Fujita et al. confirm that increased FDG uptake is demonstrated during active disease, with remission following corticosteroid therapy (see Case 1, Figure 1(e)). 16
IP treatment includes corticosteroids, surgical resection, or both. Approximately 80% of IPs respond to corticosteroid treatment but there is a 50 to 60% chance of disease recurrence. Maintenance-dose corticosteroids are recommended for at least six months to prevent recurrence of disease. 17 Patients unresponsive to systemic corticosteroids may benefit from intralesional steroids. 18 A favorable response with corticosteroids is seen especially in IPs that are predominated by lymphocytes and plasma cells. In Case 1, the lymphoplasmocytic predominant mass responded to corticosteroids. Resection should be considered when alternative noninvasive treatments have failed; if the diagnosis cannot by established by FNA and core biopsy alone; or if the mass can be resected with minimal morbidity. In Case 2, surgical resection was necessary because of lack of definitive diagnosis. Recurrence of head and neck IPs after attempts at surgical excision approaches 10 to 20%. 10
Alternative treatments include radiotherapy, small-molecule inhibitors, and Igs. In a clinical trial involving orbital pseudotumors, 75% of patients responded to radiotherapy treatment. 19 It is not known if the same response would be seen in extraorbital IP cases. Small-molecule inhibitors have shown results in small subsets of patients. For example, rituximab is a chimeric anti-CD20 antibody that provoked a sustained response in a recurrent IP of the mandible. 20 Crizotinib, an ALK inhibitor, induced a partial response in a patient with ALK-translocated inflammatory myofibroblastic tumor. 21
Conclusion
In conclusion, three cases of extraorbital IPs in the head and neck are described. IPs of the head and neck mimic malignancy in clinical and radiographic presentation and must be distinguished from malignancy by comprehensive histopathologic evaluation. Incisional or excisional biopsy is often required to establish the diagnosis and rule out malignancy. Tumors that can be completely excised without long-term morbidity may be treated with complete surgical excision. Tumors for which complete resection would result in morbidity may be treated more conservatively with corticosteroids and close follow-up.
Footnotes
Acknowledgment
Informed consent was obtained from each of the three individuals in this case series.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.