
Abstract
A persistent trigeminal artery (PTA) is the most common carotid-vertebrobasilar anastomosis. PTA variants terminating on cerebellar arteries instead of the basilar artery have been reported previously. We present the first case of a PTA communicating with a fetal posterior communicating artery identified on a magnetic resonance angiogram. An understanding of these anatomical variants is important to clarify pathological processes that can help guide neurosurgical and endovascular procedures.
Keywords
Introduction
A persistent trigeminal artery (PTA) is the most common carotid-vertebrobasilar anastomosis. The incidence of PTA and its variants is estimated to be 0.68%. 1 PTA was first reported in a cadaver by Quain in 1844. 2 Sutton later described PTA on arteriography in 1950. 3 The Saltzman’s classification of PTA is widely recognized. 4 Weon et al. have extended the categorization scheme to include PTA variants terminating on the cerebellar arteries. 5 We report a case of a PTA with a previously unrecognized configuration that does not conform to the current classifications.
Case report
An 18-year-old female with a past medical history of idiopathic intracranial hypertension, obesity, metabolic syndrome, polycystic ovarian syndrome, and hypothyroidism presented with severe pressure-like headache for five days. The headache radiated down her neck and was associated with nausea, vomiting and photophobia. It was worse than her prior headaches, which usually resolved with a combination of aspirin, acetaminophen and caffeine. The review of symptoms was otherwise unremarkable, and no significant findings were found on physical examination. A lumbar puncture demonstrated elevated intracranial pressure (25 cm of H2O) and was followed by symptomatic improvement. However, it remained unclear if the headache was due to recurrent idiopathic intracranial hypertension, migraine, or another etiology.
Magnetic resonance imaging (MRI) of the brain with and without contrast was within normal limits. A non-contrast time-of-flight magnetic resonance angiogram of the brain (Philips Achieva 3 T) demonstrated a left PTA, a left fetal posterior communicating artery (PCoA) and a communication between the two near their origin from the left internal carotid artery (ICA) (Figures 1 and 2).The basilar artery (BA) proximal to the PTA was hypoplastic. The right posterior cerebral artery (PCA) was supplied by the BA. No associated vascular anomaly was identified.
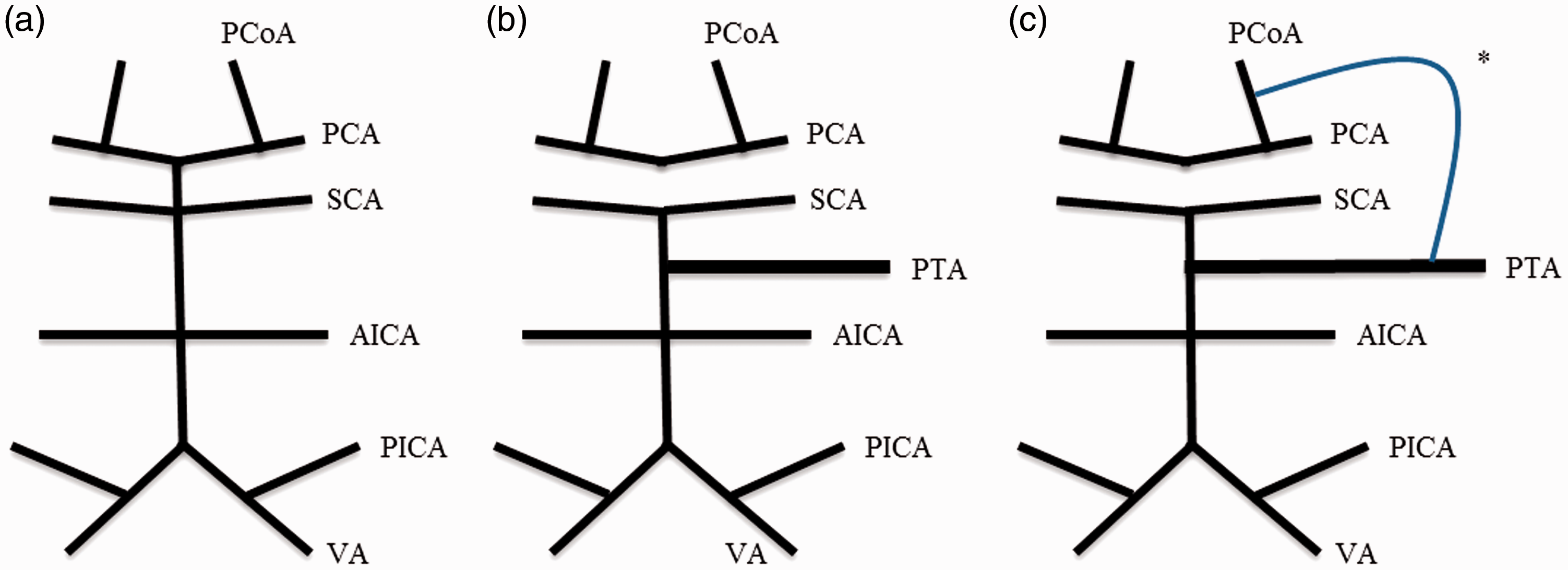
Non-contrast time-of-flight magnetic resonance angiogram of the brain. (a) Pre-cavernous internal carotid artery, (b) Left persistent trigeminal artery (PTA), (c) Moderate hypoplastic basilar artery proximal to PTA insertion, (d) PTA-fetal posterior communicating artery anastomosis, (e) Posterior cerebral artery. Schematic of posterior circulation. (a) Normal anatomy, (b) Saltzman type II, and (c) persistent trigeminal artery (PTA)-fetal posterior communicating artery (PCoA) anastomosis. PCA: posterior cerebral artery; SCA: superior cerebellar artery; AICA: anterior inferior cerebellar artery; PICA: posterior inferior cerebellar artery; VA: vertebral artery; PTA: persistent trigeminal artery; *PTA-fetal PCoA anastomosis.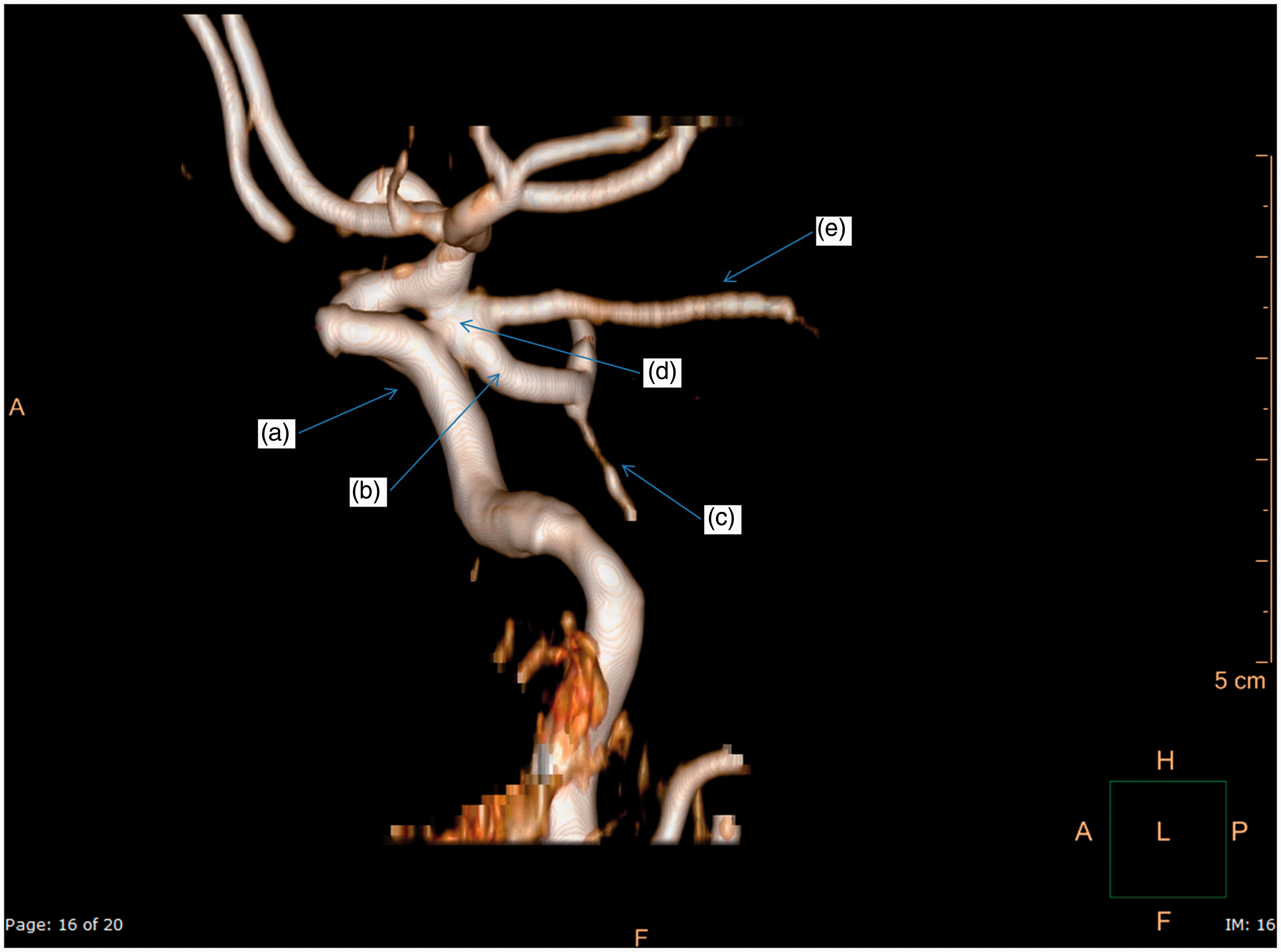
The patient was admitted and placed on a regimen of topiramate 100 mg nightly, acetazolamide 1000 mg twice a day, and furosemide 20 mg daily. Her condition improved and she was discharged to home after two days. Outpatient follow-up at 12 weeks documented complete resolution of symptoms.
Discussion
According to the current understanding of embryogenesis, no known connection exists between the primitive trigeminal artery and the primitive caudal ICA (precursor of the PCoA). At the 4–5 mm embryonic stage (five weeks’ gestation), the hindbrain is supplied by two parallel neural arteries that have four anastomoses with the primitive cranial ICA (from cranial to caudal): the trigeminal artery, the otic artery, the hypoglossal artery, and the proatlantal artery. At the 5–8 mm stage, the neural arteries coalesce in the mid-line to form the BA. As the PCoA develops a communication with the BA, the fetal carotid-basilar anastomoses regress. 6 The trigeminal artery is the largest of the four anastomoses and persists the longest. This overlap in chronology of the trigeminal artery and the PCoA may be related to the PTA- fetal PCoA communication seen in the present case. Termination of the PTA on the cerebellar arteries, the pontine perforators and the trigeminal ganglion have also been described earlier. 6
Saltzman classified PTA into two types. The type I PTA terminates on the BA, which, in turn, supplies the PCA and the superior cerebral artery (SCA); the BA proximal to the PTA insertion as well as the PCoA is hypoplastic. The type II PTA terminates on the BA, which supplies the SCA; a persistent fetal PCoA supplies the PCA.4,7 Weon et al. have extended this classification to PTA variants terminating on the SCA, the anterior inferior cerebellar artery and the posterior inferior cerebellar artery. 5 The current case does not conform to any of the published classifications. The BA proximal to the PTA was hypoplastic (similar to Saltzman type I), but a fetal PCoA was also present (similar to Saltzman type II). To the best of our knowledge, this is the first report of a PTA-fetal PCoA anastomosis.
PTA and its variants may supply important anatomical structures, possibly alter the cerebral blood flow patterns, and provide a potential route for the ICA thromboemboli to the posterior circulation. 7 Acetazolamide provides a vasodilatory stimulus and may increase cerebral blood flow depending on the degree of intrinsic or existing compensatory vasodilation. 8 In the presence of a persistent trigeminal artery, whether or not the increase of blood flow applies to the alternative route may depend on the responsiveness of the variant vasculature to the medication or amount of intrinsic compensatory vasodilation as compared to the normal vasculature of the circle of Willis. The medication-induced vasodilatory effect may then determine the amount of blood flow and relative extent of visualization of the PTA on imaging. An understanding of these anatomical variants is important to clarify pathological processes that can help guide neurosurgical and endovascular procedures.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.