
Abstract
We present three cases of anomalous origin of the left vertebral artery (LVA) detected during the evaluation of stroke. The VA usually enters the transverse foramen of the sixth cervical vertebra (C6), but an anomalous LVA originating from the aorta frequently enters at a higher level. In our series, ultrasound of the LVA showed entry at C4 in two patients and at C5 in one patient. These findings suggested anomalous LVA origin, and three-dimensional computed tomography demonstrated the LVA arising from the aorta proximal to the left subclavian arteries. Carotid duplex ultrasound is useful for the diagnosis of this anomaly.
Introduction
The vertebral artery (VA) most commonly arises from the superoposterior aspect of the subclavian artery (SA), ascends between the longus colli and scalenus anterior muscles, runs behind the common carotid artery (CCA), and enters the transverse foramen (TF) of the sixth cervical vertebra (C6). However, a left vertebral artery (LVA) originating directly from the aortic arch is a relatively common anomaly with an incidence of approximately 5%, and usually arises between the left CCA and left SA.1–3 This anomaly is embryologically explained by development of the proximal VA from a persistent left cervical intersegmental artery more cranial than the seventh, instead of from the dorsal division of the seventh cervical intersegmental artery as is normal. 3 Anatomical variation of the VA is underdiagnosed because it is generally asymptomatic. However, accurate assessment of the VA is clinically important when planning surgical or interventional procedures on the thorax or neck to avoid the risk of complications due to an anomalous course.
Although carotid duplex ultrasonography is considered to be a good modality for assessing the extracranial VA, previous literature has not mentioned its use for detecting variant origin of the LVA. Regarding the level at which the VA enters the TF, an LVA arising directly from the aorta differs from a normal artery and frequently enters the TF at a level above C6.2–4 This article describes three cases of anomalous origin of the LVA from the aorta, in which duplex ultrasound provided useful information about the course and entry level of the vessel that pointed to an anomalous origin.
Case reports
Case 1
A 77-year-old woman with hypertension, diabetes mellitus and dyslipidemia was admitted to our hospital because of progressive weakness of the right extremities. On admission, she had dysarthria and right hemiparesis including the face. Brain magnetic resonance imaging (MRI) revealed acute ventral pontine infarction, while intracranial MR angiography found no apparent abnormalities of the vertebrobasilar circulation. Duplex ultrasonography demonstrated that the bilateral VAs ascended anteriorly to the TF at C6 to C5 and close to the ipsilateral CCA, entering the TF at C4 (Figure 1(a), (b)). These findings suggested the possibility of anomalous origin of the LVA. Three-dimensional computed tomography angiography (3D-CTA) was performed to assess vascular lesions of the vertebrobasilar system, revealing that the LVA originated from the aorta between the left CCA and left SA although the right vertebral artery (RVA) branched from the right SA. Both VAs entered the TF at C4 (Figure 1(c), (d)). There was no significant VA stenosis. Since no source of embolism was identified, she was treated with aspirin to prevent stroke recurrence.
Longitudinal (a) and transverse (b) ultrasound gray-scale images. The left vertebral artery (arrow) runs close to the ipsilateral common carotid artery (CCA) and thyroid gland at the C5 level, and enters the transverse foramen (TF) at C4. Three-dimensional computed tomography (CT) angiography ((c), (d)). The left vertebral artery arises from the aortic arch between the left CCA and subclavian artery, and enters the TF at C4.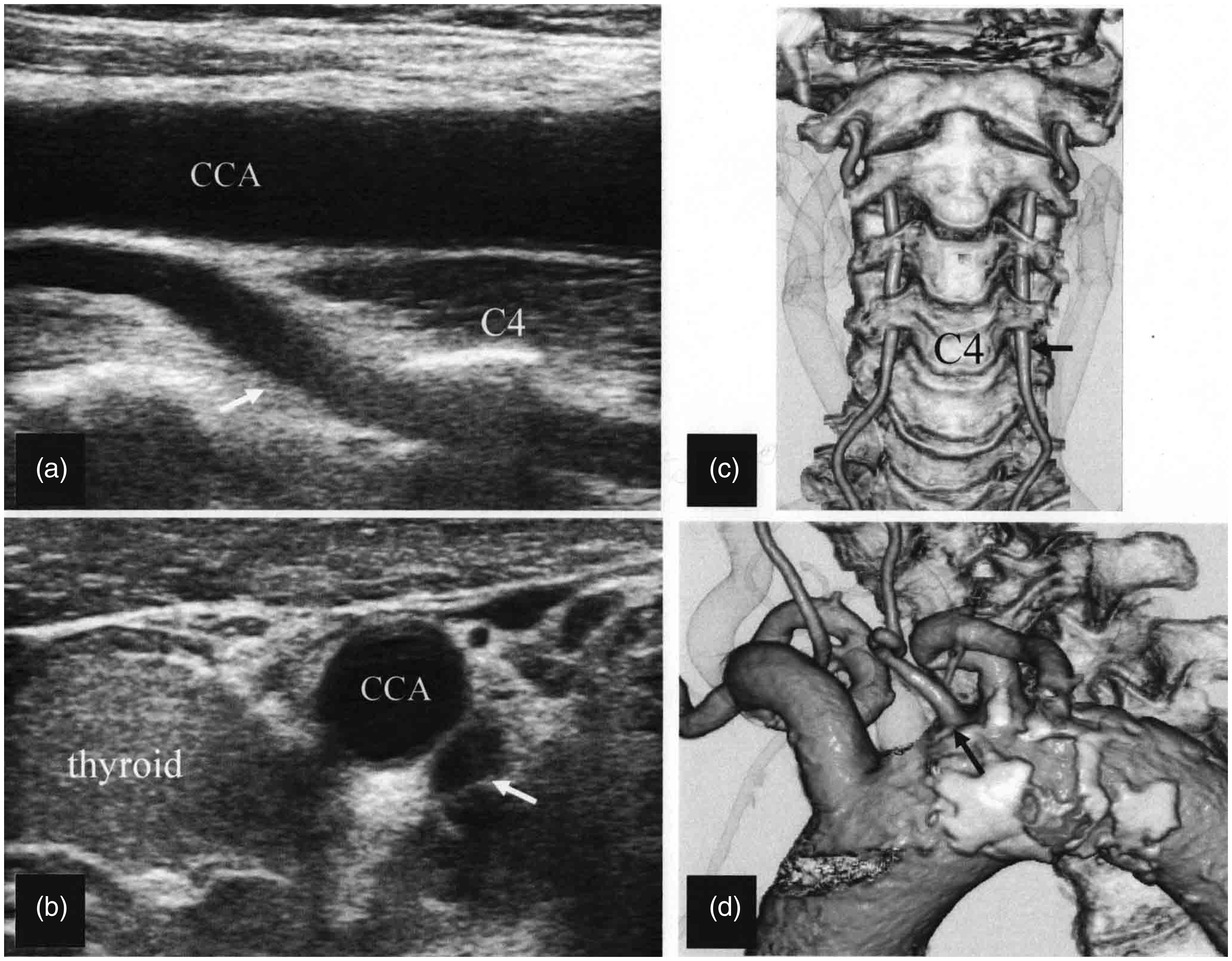
Case 2
A 52-year-old man presented for evaluation of the cause of multiple infarcts in the left internal carotid artery territory, which had occurred one year previously. Physical examination revealed no abnormal neurologic findings. MR angiography suggested stenosis of the supraclinoid portion of the left internal carotid artery, which seemed to be associated with his infarcts since no source of embolism was revealed by cardiac evaluation. Duplex ultrasonography showed the LVA running anteriorly to the TF at C6 to C5 before entering the TF at C4 (Figure 2(a), (b)), while the right (R)VA followed a similar course on the other side and entered the TF at C3. 3D-CTA was performed to assess stenosis of the left internal carotid artery, and it revealed the unusual courses of the bilateral VAs. The LVA had an anomalous origin from the aorta proximal to the origin of the left SA, although the origin of the RVA was normal, and both VAs entered the TF at high levels as mentioned above (Figure 2(c)).
Longitudinal (a) and transverse (b) ultrasound gray-scale images. The left vertebral artery (arrow) runs anteriorly to the transverse foramen (TF) at C5, very close to the ipsilateral common carotid artery (CCA) and internal jugular vein, and enters the TF at C4. Three-dimensional computed tomography (CT) angiography (c). The left vertebral artery arises anomalously from the aorta and enters the TF at C4.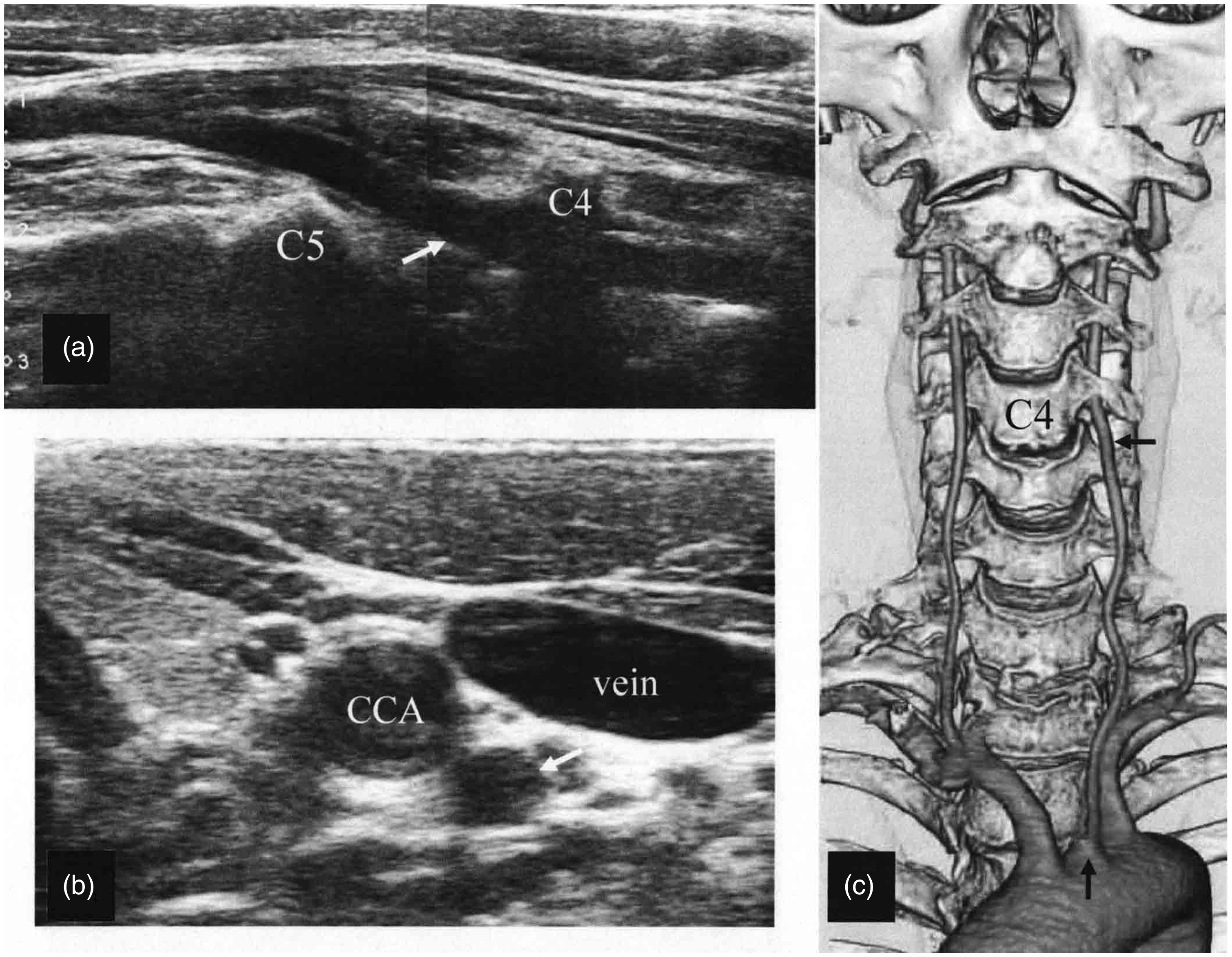
Case 3
A 51-year-old man was a smoker with hypertension and dyslipidemia. He presented to our hospital with transient episodes of difficulty in walking. While neurological examination was normal, brain MRI revealed recent infarcts in the right cerebellum and putamen with no significant stenosis of the large intracranial or extracranial vessels. Duplex ultrasonography detected the LVA running very close to the ipsilateral CCA and internal jugular vein at the C6 level (Figure 3(a), (b)), after which it entered the TF at C5, while the RVA entered at the usual level of C6. 3D-CTA for evaluation of atherosclerotic plaque in the thoracic aorta identified an anomalous LVA arising directly from the aorta between the left CCA and SA, and confirmed that it entered the TF at C5 (Figure 3(c)). Cardiac evaluation found no embolic source. Although the etiology of stroke was obscure, antiplatelet therapy was initiated.
Longitudinal (a) and transverse (b) ultrasound gray-scale images. The left vertebral artery (arrow) runs very close to the ipsilateral common carotid artery (CCA) and internal jugular vein at the C6 level, and enters the transverse foramen at C5. Three-dimensional computed tomography (CT) angiography (c). The left vertebral artery arises directly from the aorta and enters the TF at C5.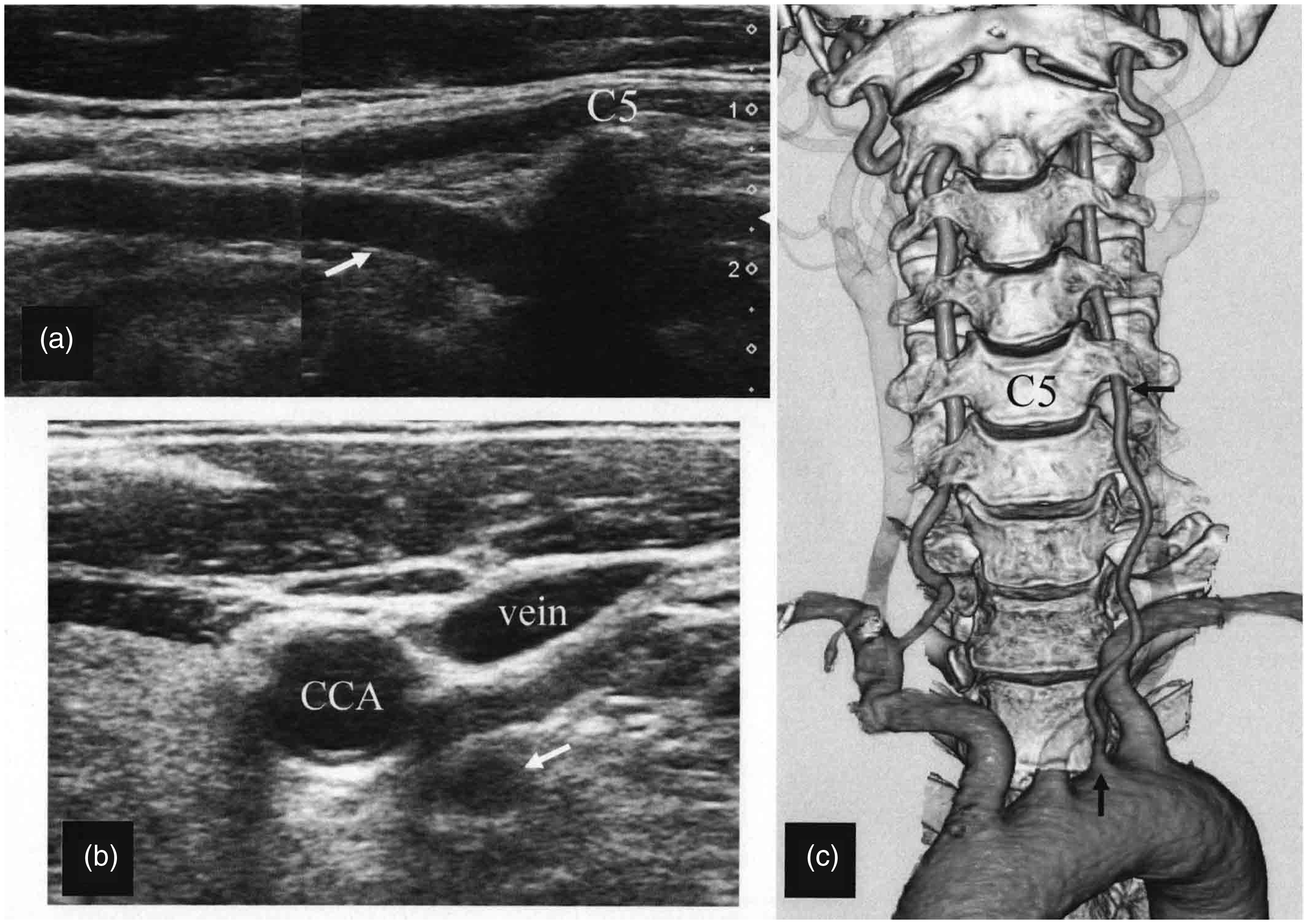
Discussion
In these three patients, we strongly suspected anomalous origin of the LVA because ultrasound demonstrated that the LVA entered the TF at C4 or C5, and the diagnosis was confirmed by 3D-CTA. Entry of the VA into the TF at C6 occurs in approximately 90% of patients, while entry occurs at C4 in 0.5 to 3.0%, at C5 in 3.3 to 7%, and at C7 in 0.3 to 5.5%. The VA very rarely enters the TF at high levels like C2 or C3.4–6 Unlike vessels with a normal origin, an LVA arising from the aortic arch is likely to enter the TF at a higher level than C6. In a series of 30 LVAs with aortic origin reported by Yamaki et al., 2 the level of entering the TF was C6 for 10 vessels (33.3%), while it was higher for 20 vessels (66.7%), being C5 in 43.3%, C4 in 16.7%, and C3 in 6.7%. Therefore, by detecting an unusual level of entry into the TF, an anomalous origin of the LVA can be found with a high frequency. When the LVA enters the TF above C6, the prevalence of an anomalous origin directly from the aortic arch is 66% according to Uchino et al. 3
For detecting a VA with high entry into the TF, carotid ultrasound bears comparison with 3D-CTA. 7 Because it runs anterior to the TF at C6, a VA entering the TF at a high level runs close to the thyroid gland, ipsilateral CCA, and internal jugular vein, and it occasionally crosses the CCA and vein. Although there have been a few reports about use of carotid ultrasound for evaluation of the VA entry level, no attention has been paid to detection of an anomalous LVA origin. Yanik et al. 8 reported the ultrasound findings of an RVA arising from the right CCA and entering the TF at C3. However, it may be difficult to use level of RVA entry as an indication of anomalous origin, because the RVA very rarely arises from any vessel other than the right SA.2–4
Some authors have raised the possibility that anomalous origin of aortic arch vessels may be associated with cerebral disorders through alterations of cerebral hemodynamics, but a relation between these anomalies and the risk of cerebral disorders has not been proved.1,9 Komiyama et al. 10 suggested that there was an association between anomalous origin and LVA dissection, but the number of such cases was small (four of their own cases and one reported by Dudich and colleagues 11 ).
In conclusion, our three cases suggest that using ultrasound to assess the level of LVA entry into TF can assist with identification of anomalous origin of this vessel from the aorta. By focusing on this ultrasound finding in clinical practice, more patients with anomalous LVA origin will be identified, and it will become clear whether and to what extent this anatomical variant is relevant to cerebrovascular disorders.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.