
Abstract
In epileptic patients with multiple sclerosis (MS), cortical lesions have been suggested to cause seizures. In brain magnetic resonance imaging (MRI), double inversion recovery (DIR) sequences are generally used to evaluate MS cortical disease burden. We present the case of a woman, diagnosed with MS, suffering from drug-resistant partial seizures initially attributed to MS. The patient underwent many MRI exams, but only by means of high-resolution three-dimensional DIR sequences was a focal cortical dysplasia discovered. The MRI findings and FDG-PET/CT supported the diagnosis. This case recommends the use of DIR sequences both in patients with suspect epileptogenic lesions not detected with routine MRI protocols and in epileptic patient with MS, before ascribing seizures to MS.
Keywords
Introduction
In patients with multiple sclerosis (MS) suffering from epilepsy, cortical lesions have been suggested to cause seizures. 1 Double inversion recovery (DIR) sequences allow MS cortical burden evaluation, since they increase the contrast among the grey matter (GM), the cerebrospinal fluid (CSF) and the white matter (WM): MS cortical plaques appear hyperintense on DIR. 2 Dysplastic cortex and cortex with a pathological increase of water content (e.g. oedema, post-critical alterations) also appear hyperintense on DIR. 3 We present the case of a woman diagnosed with MS and suffering from drug-resistant partial seizures. All the conventional magnetic resonance imaging (MRI) performed failed to demonstrate an area of cortical dysplasia which was discovered by DIR sequences.
Case report
A 32-year-old woman with left hemianopsia underwent to brain MRI which demonstrated a subtle cortical-subcortical FLAIR hyperintensity in the right medial occipital gyrus, initially interpreted as migrainous infarction. The same MRI showed some WM lesions also interpreted as migraine related. Despite this hypothesis, the hemianopsia recovered completely after one week. Subsequent MRI exams did not show signs of a previous occipital infarction.
After two years, the patient also suffered episodes of upper and lower limbs dysesthesia and disequilibrium/step hesitation/lateropulsion not associated each other. So she underwent to a new brain MRI that showed an increase in WM lesions with the characteristic pattern of MS. The presence of anomalous PEVs and CSF oligoclonal bands supported a diagnosis of relapsing remitting MS. A therapy with interferon-beta-1a was established, and since then, the clinical course of MS (EDSS 0) as well as WM lesions on MRI have remained stable.
Nevertheless, the patient continued to complain of transitory episodes of visual disturbance (left hemianopsia, visual hallucinations) until she suffered a generalised seizure. Even though an electroencephalogram (EEG) appeared normal, gabapentin was prescribed as an anti-epileptic. During the following years, no more generalised seizures were reported, but visual symptoms persisted. Therefore, therapy was changed to sodium valproate and carbamazepine.
At the age of 43, the patient presented to our institution for a routine control, during a period free from visual disturbances, and underwent a 3 Tesla MRI exam (Figure 1), including three-dimensional (3D) DIR, FLAIR, T2-weighted and T1-weighted sequences. For the first time, DIR images (especially with coronal reformatting) clearly showed a thickened and hyperintense cortex in the right lateral parieto-occipital region, a subtle subcortical hyperintensity (less clearly detectable on FLAIR) and a blurring of the GM/WM junction (confirmed on T1-weighted imaging). Perfusion showed a focal reduction of the cerebral blood volume (CBV) and MR spectroscopy (MRS) demonstrated a small reduction of N-acetylaspartate, with a slight increment of choline, without significant inversion of Cho/NAA ratio, in the lesion site.
First MRI examination at our institution (3 Tesla MRI scanner). DIR images show thickened and hyperintense right lateral parieto-occipital cortex, more evident on coronal reformatting, associated with subtle subcortical hyperintensity (arrows (a) and (d)). These findings are less evident on 3D FLAIR (arrows (b) and (e)). 3D Gradient Echo T1-weighted images confirm cortical thickening (arrowheads (c)) and show blurring of the grey matter/white matter junction (arrowheads (f)). Multivoxel spectroscopy demonstrates slight choline increment and N-acetylaspartate reduction without significant inversion of Cho/NAA ratio in the lesion site (g). DIR images show cortical (arrow (h)), iuxtacortical (arrowheads (h)), periventricular (empty arrows (h) and (i)), subcortical (dashed arrow (i)) and infratentorial (empty arrowheads (i)) multiple sclerosis lesions. MRI: magnetic resonance imaging; DIR: double inversion recovery.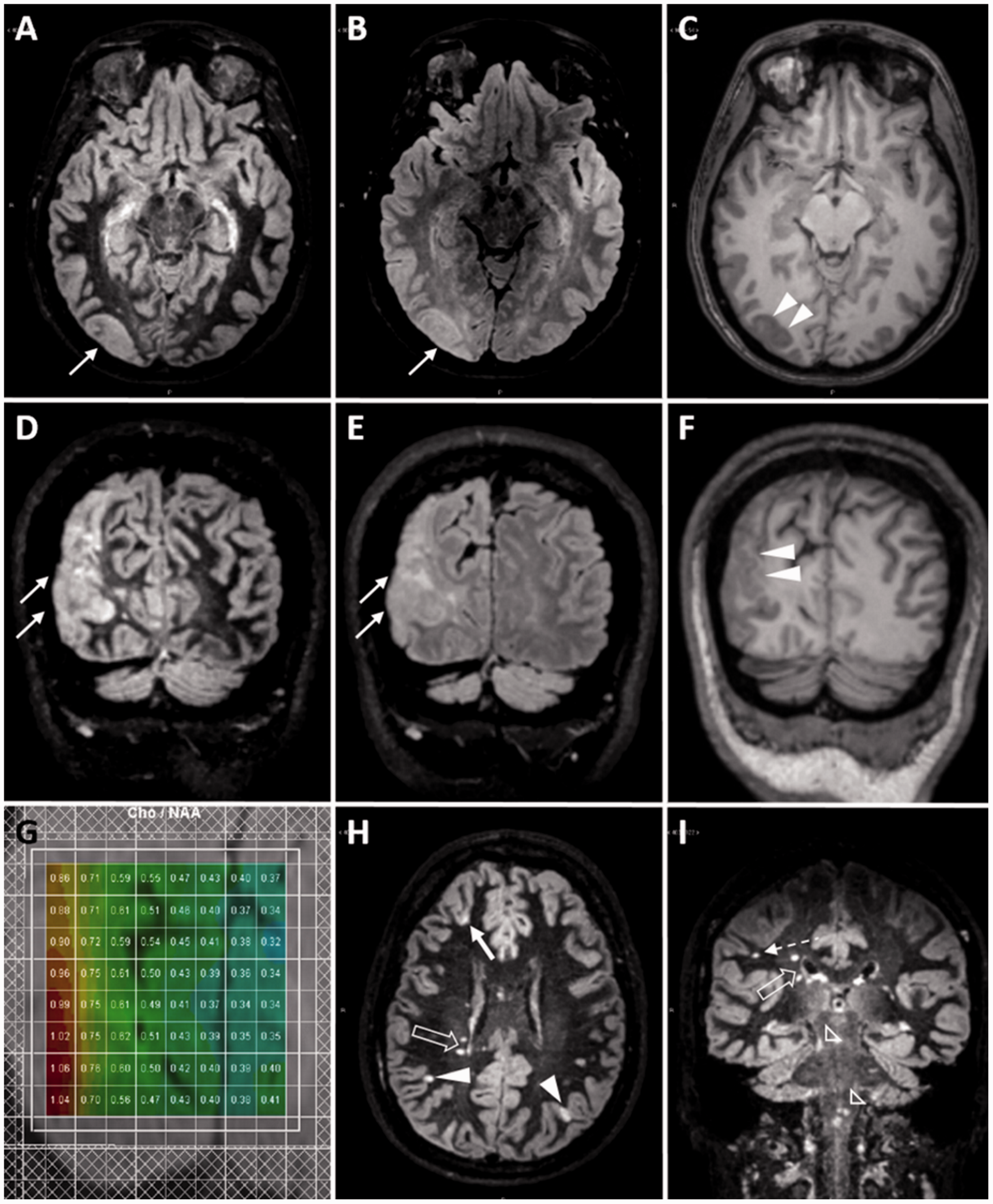
During another MRI exam, performed a few days after a period of persistent visual disturbances (one week duration), DIR sequences showed cortical hyperintensity and thickening also in the right medial occipital region, just next to the lateral parieto-occipital cortical thickening previously reported (Figure 2(a) and (b)). This new alteration disappeared completely two months later, resulting in an area of mild focal atrophy. On the contrary, the right lateral parieto-occipital cortical thickening was unmodified (Figure 2(c) and (d)). A FDG-PET/CT demonstrated glucidic hypometabolism confined to this site (Figure 2(e) and (f)). Interictal EEGs showed an irregular activity in the right parietal region (Figure 2(g)).
Second 3 Tesla MRI examination. DIR coronal image shows thickening and hyperintensity in the right medial occipital cortex (arrows (a)), in addition to the well-known right lateral parieto-occipital lesion (arrowheads (a)). On FLAIR images, the same alterations are less evident (arrows and arrowheads (b)). At follow-up (third 3 Tesla MRI examination, two months later), the medial occipital alteration disappeared, resulting in an area of focal atrophy with relative overrepresentation of the cortical spaces (arrows (c) and (d)) and dilation of the occipital horn of the lateral ventricle (dashed arrow (c) and (d)). At the same examination, the right lateral parieto-occipital cortical thickening persisted (arrowheads (c) and (d)). A cerebral FDG-PET/CT (arrowheads (e) and (f)) clearly shows glucidic hypometabolism confined to the right lateral parieto-occipital cortex. An interictal electroencephalogram shows an irregular theta activity with sharp waves in the right parietal region (g). MRI: magnetic resonance imaging; DIR: double inversion recovery.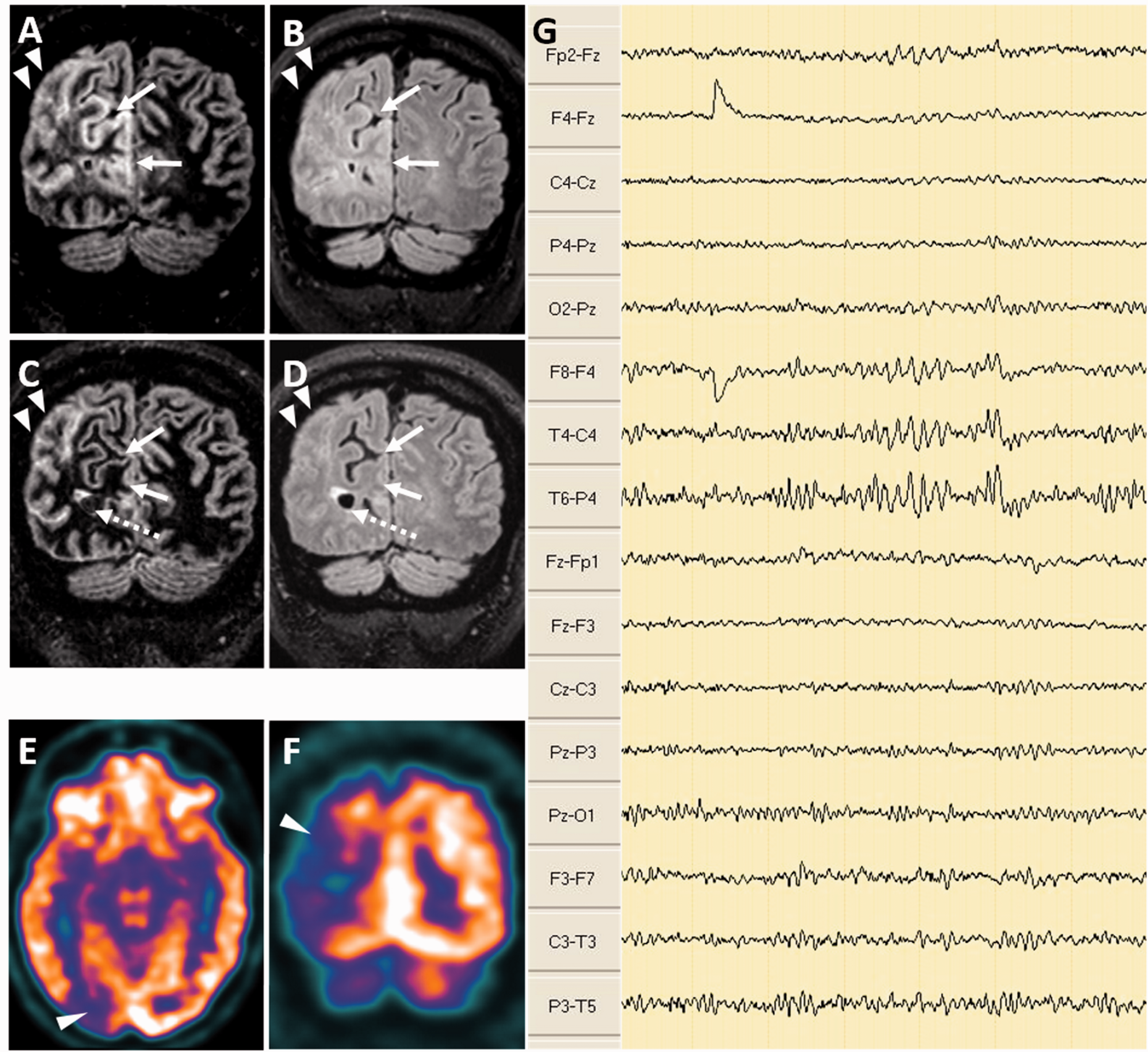
After this episode, the patient started therapy with levetiracetam. So far (about one year ago), no new visual disturbances have been described.
Discussion
With regard to the interpretation of the stable lesion in the right lateral parieto-occipital cortex, we excluded the outcomes after a past ischemic event because neither malacia nor localised atrophy was found. A low-grade cortical tumour was also excluded because the alteration lacked mass effect. The hypothesis of a large cortical demyelinating lesion suited the contemporary diagnosis of MS. However, to our knowledge, such a lesion does not fit any morphological aspect of MS cortical plaques described. 4 Genetic exams excluded CADASIL and MELAS.
Finally, we assumed the lesion as a focal cortical dysplasia (FCD) whose typical MRI findings are represented by cortical thickening (especially type II), blurring of the GM/WM junction (type I and II, especially type II), WM volume reduction (especially type I), hyperintensity on long-TR images and hypointensity on T1-weighted imaging (especially type II). 5 A T2-weighted hyperintensity involving the GM and the underlying WM up to the ventricle (transmantle sign) is the hallmark of FCD type IIb. 6 Abnormalities of the gyration and of the sulci associated with segmental/lobar hypoplasia up to atrophy can also be found (especially FCD type I).6,7 Other pathologies possibly associated to FCD 8 (e.g. hippocampal sclerosis, developmental tumours) were not found.
In absence of a clear transmantle sign, we interpreted the MRI alteration as a FCD type IIa (Taylor’s FCD without balloon cells).6,8,9 MRS findings were non-specific but reflected a neuronal/glial cell dysfunction suitable to FCD. 7 Unfortunately, no MRS was performed during or some hours after epileptic seizures to search for the presence of lactate, as some authors suggest that seizures activates anaerobic glycolysis in neuronal migration disorders.10,11 EEG confirmed an abnormal pattern in the region of the cortical anomaly showed by MRI. Clinically, the patient suffered from visual hallucinations, a hallmark of occipital epilepsy which can be caused by FCD. 12 The FDG-PET/CT hypometabolic pattern was also consistent with our hypothesis. 7
The transient right medial occipital alteration was interpreted as cortical oedema consequent to persistent partial seizures. The anatomic location of such oedema was consistent with the left visual disturbance of which the patient complained and probably corresponds to the area of migrainous infarction initially hypothesised. MRI detects reversible pathological findings in 20–70% of patients after generalised or partial seizures (post-ictal oedema). 13 DIR sequences, which are dedicated to cortical pathology, appeared useful to document this finding. The subsequent focal widening of the cortical sulci, observed in the same area, could be the consequence of a neuronal loss due to persistent seizures. 13
Regarding therapy, the patient continued interferon-beta administration because it was effective in MS control, even if it has been reported a possible increased risk of seizures related to this drug. 14 However, the therapy for epilepsy was changed to Levetiracetam, since recent findings in an animal model suggest the possible efficacy of Levetiracetam to treat the drug-resistant epilepsy associated with FCD. 15
Our patient had undergone many conventional MRI scans, but only by using high-resolution 3D DIR acquisition with multiplanar reconstructions was the subtle lesion in the lateral right occipito-parietal cortex identified. Moreover, DIR depicted transitory cortical alterations related to the seizure.
Conclusions
Even without a histologic confirmation, this case highlights the usefulness of DIR sequences to improve sensibility towards both inflammatory and dysplastic cortical lesions, and the use of DIR is recommended in patients with suspect epileptogenic lesions not detected with routine MRI protocols. In patients with MS suffering from drug-resistant epilepsy, before ascribing seizures to MS, it is mandatory to exclude a better explanation.
Footnotes
Acknowledgement
Thanks to Virginia Munerati, MD, for providing the patient’s EEG examinations.
Funding
The authors received no grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.