
Abstract
Paragangliomas can be diagnosed accurately using magnetic resonance imaging and dynamic four-dimensional magnetic resonance angiography. Four-dimensional imaging uses the highly vascularised structure of these tumours, which results in a homogenous capillary blush and usually, due to the arteriovenous shunting, in an early draining vein. By these features the tumour can be differentiated from other neoplasms. The authors describe a case of a paraganglioma localised in the middle ear of an elderly patient. Magnetic resonance contraindications led to preoperative diagnostics with high resolution computed tomography of the temporal bone and additionally computed tomography perfusion imaging instead of magnetic resonance imaging with four-dimensional magnetic resonance angiography. Using the computed tomography perfusion dataset, regions of interest were placed in the carotid artery, the sigmoid sinus and the tympanic mass. In the computer-assisted analysis the tumour showed late arterial enhancement and delayed wash-out compared to the enhancement curves of the carotid artery and the sigmoid sinus. This corresponded to the highly vascularised nature of a paraganglioma. On postoperative follow-up imaging computed tomography perfusion showed almost no enhancement of a small residual tympanic mass, which was then considered to be granulation tissue. In conclusion, in the case of magnetic resonance contraindications the preoperative diagnosis of tympanic paraganglioma can be made using computed tomography imaging criteria alone. Computed tomography perfusion imaging may be helpful in these cases to detect residual or recurrent tumour.
Paragangliomas of the head and neck are highly vascularised rare tumours of neural crest origin. 1 These in most cases benign lesions without evidence of metastatic disease are named after the site of origin. In the case of tympanic paragangliomas the tumour derives from paraganglion cells of the tympanic plexus in the middle ear. Dynamic magnetic resonance angiography (MRA) has been used to differentiate paragangliomas from other neoplasms of the head and neck, using the characteristically early enhancement and incomplete wash-out of these lesions.2–4
We describe a patient with suspected paraganglioma of the middle ear and contraindications for magnetic resonance imaging (MRI) who presented for pre-surgical imaging. The location and extent of the tumour were determined using computed tomography (CT) of the temporal bone. CT perfusion imaging confirmed the high vascularisation of the lesion with the typical characteristics of a paraganglioma.
Case description
A 69-year-old woman presented with hearing impairment and a sensation of pressure in the right ear for several years and a marked deterioration for several months. Vertigo, tinnitus and otorrhoea were not present. Physical examination revealed a reddish pulsating mass in the right middle ear.
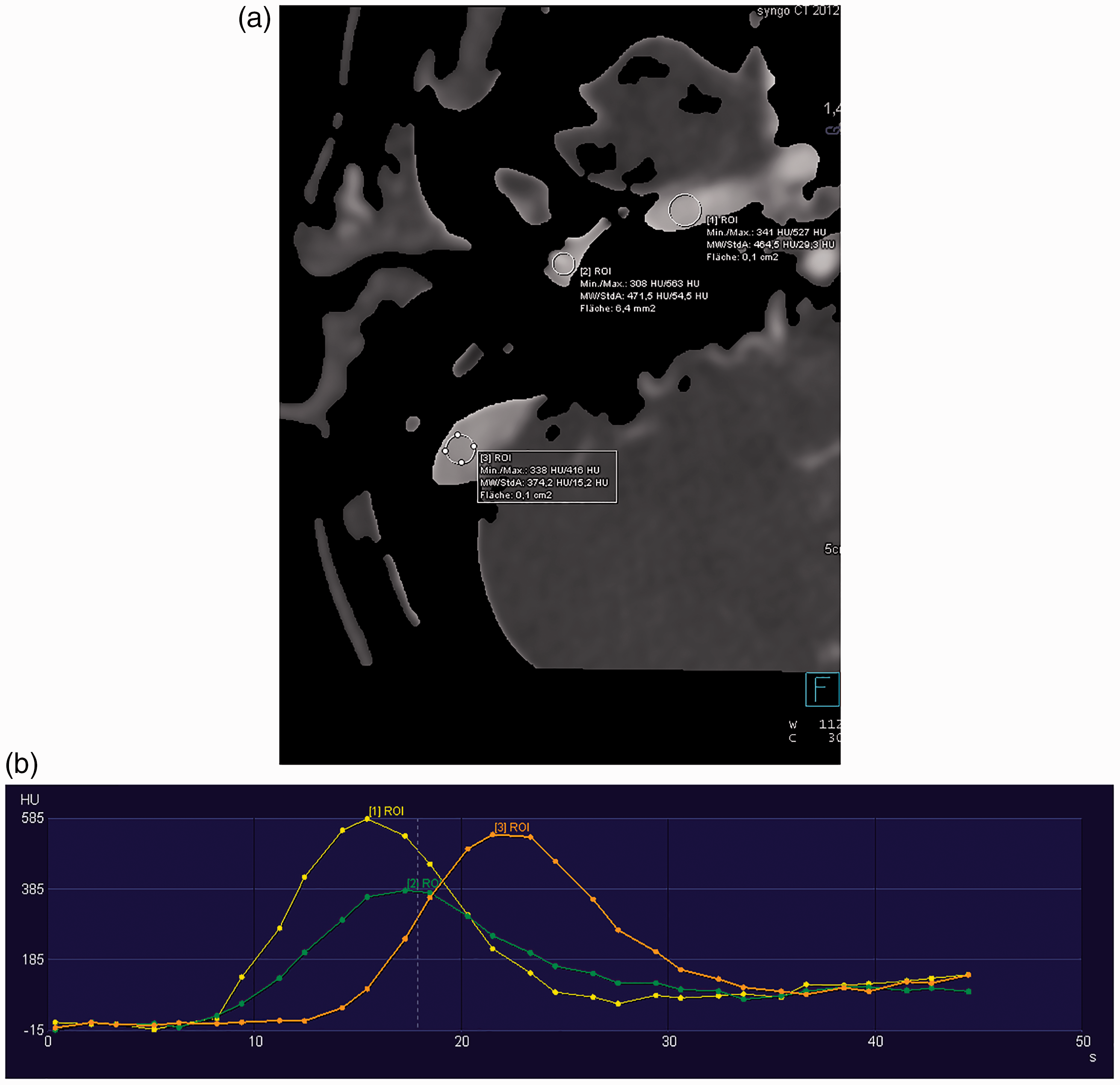
High resolution computed tomography (HRCT) of the temporal bone was performed with the following parameters: 64 slices, helical acquisition, 0.4 mm slice thickness, using a Somatom Defintion AS scanner (Siemens, Erlangen, Germany). Axial and coronal reformations in 1 mm slice thickness were created. CT confirmed a soft tissue mass in the right middle ear (Figure 1). MRI to support the suspected diagnosis of tympanic paraganglioma by four-dimensional (4D) dynamic MRA was not possible due to the implantation of a cardiac pacemaker several years ago. Instead, we performed CT perfusion imaging of the temporal bone with the following parameters: 64 slices, helical acquisition, 1.5 mm slice thickness, 1.5 seconds temporal resolution, using a Somatom Defintion AS scanner (Siemens). Post-imaging analysis was performed by placing regions of interest (ROI) in the right internal carotid artery (ICA; ROI 1), in the tumour of the middle ear (ROI 2) and in the right sigmoid sinus (ROI 3) (Figure 2(a)). Time-dependent curves were automatically generated (Figure 2(b)) by the post-processing software of the CT scanner (Syngo.via; Siemens Healthcare, Erlangen, Germany). The ROI in the ICA showed typical early arterial enhancement, the ROI in the sigmoid sinus showed a delayed peak corresponding to venous enhancement. The tympanic mass, however, showed late arterial enhancement with delayed wash-out. Density values did not reach the level of the arterial or venous vessels, which basically proved tympanic paraganglioma.
High resolution computed tomography of the temporal bone demonstrating a right tympanic soft tissue mass (arrow). (a) Computed tomography perfusion imaging: placement of the regions of interest (ROIs) after automatic bone removal in the right internal carotid artery (1), the right tympanic soft tissue mass (2) and the right sigmoid sinus (3). (b) Corresponding time-dependent enhancement with arterial enhancement of the tumour (ROI 2).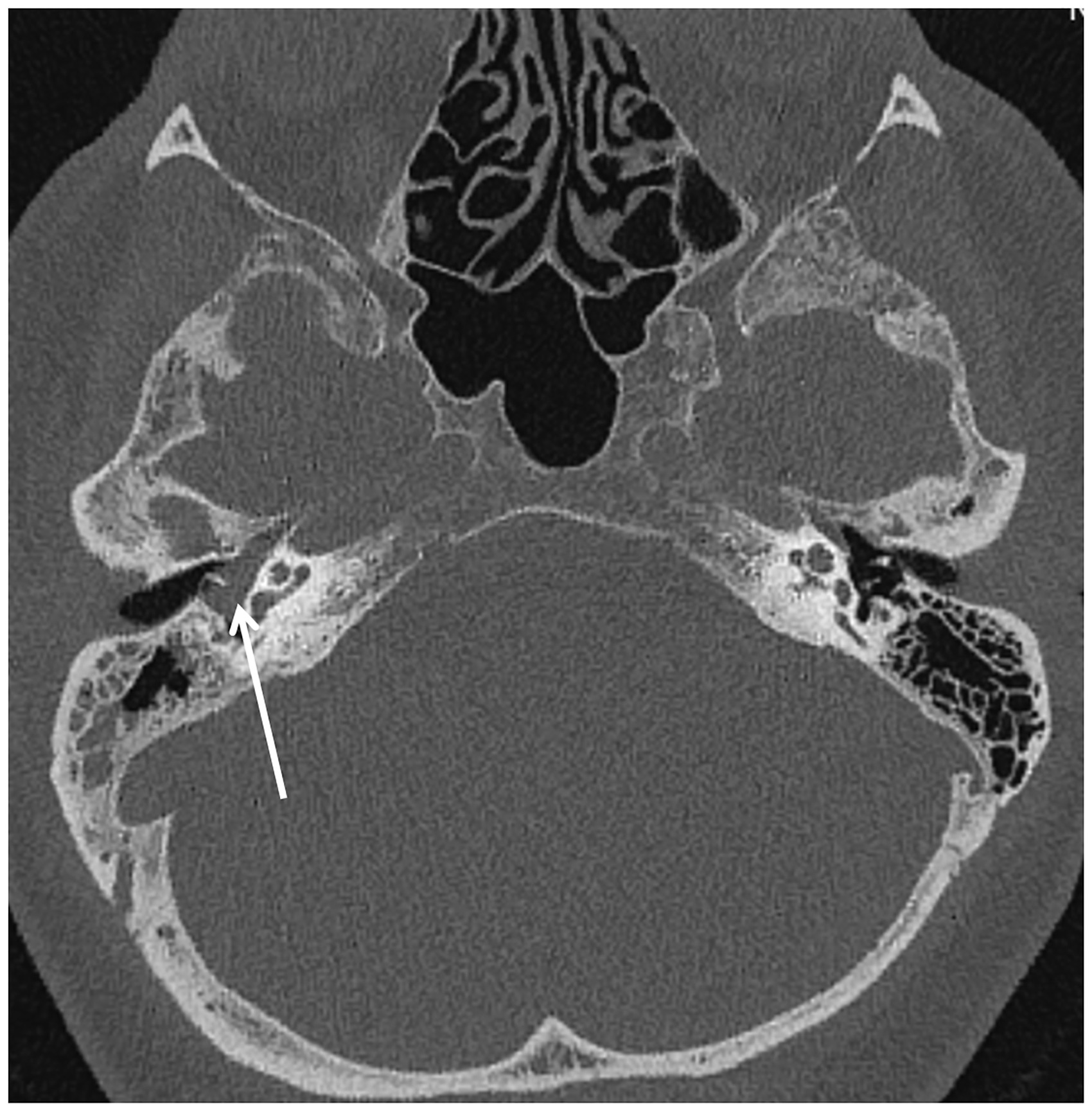
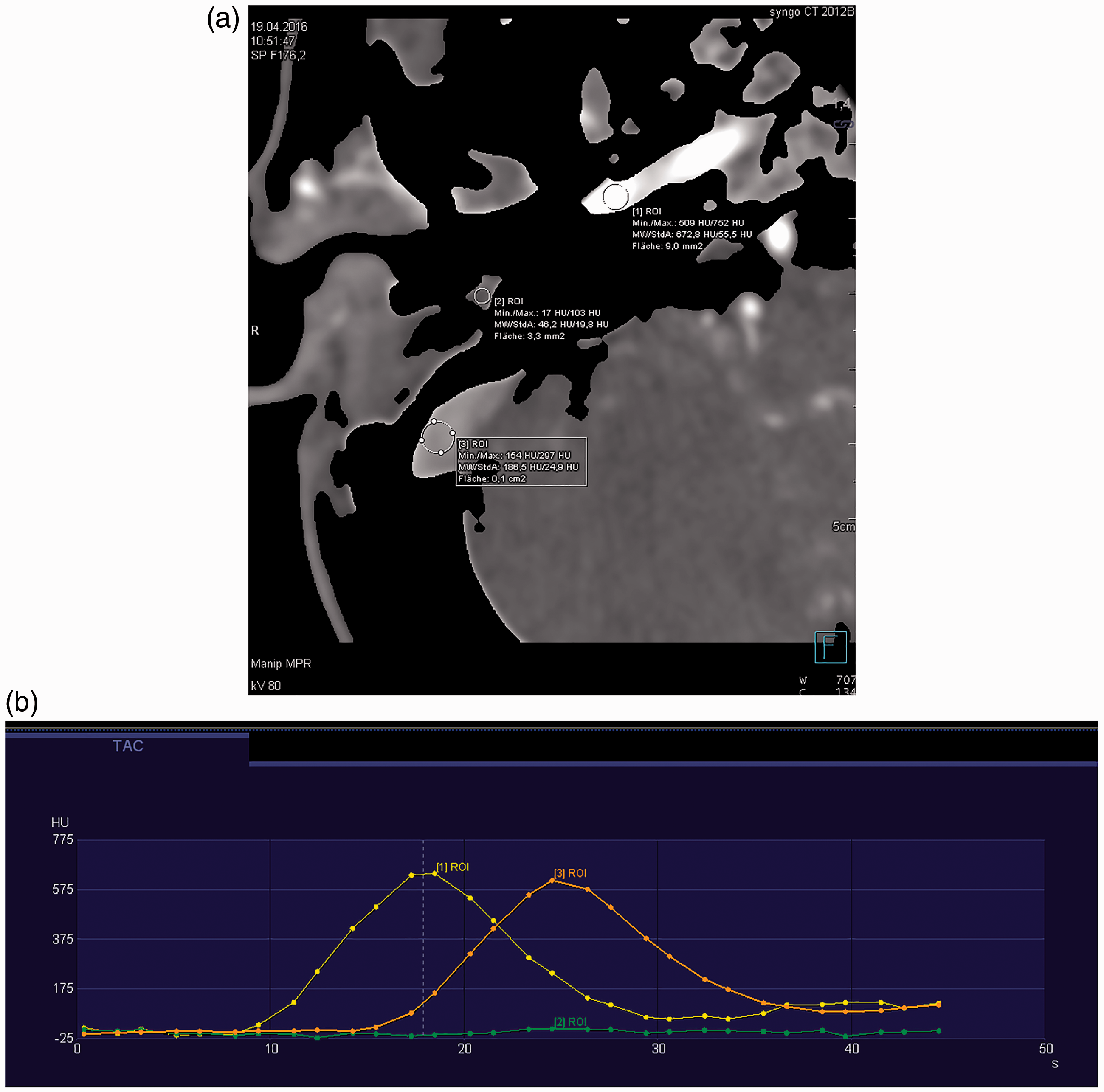
The tumour was removed by surgery via a retroauricular transmastoid approach. HRCT of the temporal bone 5 months after surgery showed a residual soft tissue mass in the tympanon (Figure 3). Repeated CT perfusion showed almost no enhancement of the lesion (Figure 4 (a and b)). The soft tissue mass was then considered to be granulation tissue.
High resolution computed tomography of the temporal bone on follow-up imaging 5 months after tumour removal via the transmastoid approach (arrow heads). A soft tissue mass is demonstrated in the tympanic cavity (arrow). (a) Computed tomography perfusion imaging 5 months after surgery: placement of the regions of interest (ROIs) in the right internal carotid artery (1), the right tympanic soft tissue mass (2) and the right sigmoid sinus (3). (b) Corresponding time-dependent curves with next to none enhancement of the tympanic soft tissue mass (ROI 2).
Discussion
CT perfusion imaging is used not only in acute stroke imaging but also to assess tumour vascularity.5,6 Microvascular changes in angiogenesis are considered to be reflected by increased vascularisation. 7 Tumour vessels show characteristic changes; for example, an increase in capillary permeability and tumour perfusion. Although there is a wide overlap between benign and malignant lesion as well as inflammatory processes, CT perfusion imaging is used for tumour characterisation, staging, prediction of patient outcome and therapy response. A temporal resolution of 1.5 seconds allows assessing time-dependent enhancement not only of brain tissue in the setting of acute stroke imaging but also of masses of the skull base. In addition, it provides a three-dimensional volume dataset with anatomical information of the skull base and dynamic information of the adjacent vessels.
Typical findings of paragangliomas on angiography are highly vascularised tumours with a homogeneous early blush, potentially enlarged feeding vessels and the presence of arteriovenous shunts and prominent draining veins. 8 The angiographic appearance and features can be used for embolisation before surgery, especially in larger lesions.9,10 These characteristics of paragangliomas are already used in MRI specifically to differentiate paragangliomas of the head and neck from other entities and to search for the recurrence of paragangliomas after surgery on follow-up imaging. 2
The current case illustrates in the case of magnetic resonance contraindications the value of CT perfusion imaging in a skull base paraganglioma. On HRCT of the temporal bone the location of the lesion and potential erosion of adjacent structures can already be seen. However, perfusion imaging depicted the specific characteristics of this tumour with high vascularisation and intratumoural arteriovenous shunts, resulting in an arterial enhancement as demonstrated in the time resolved enhancement in the ROIs of the ICA, the venous sinus and the tumour. This type of enhancement is the equivalent of the arterial blush of these lesions on angiographic examination. In addition, after the discovery of a tympanic soft tissue mass on follow-up imaging, potential residual tumour or recurrence could be excluded with CT perfusion. The almost complete lack of enhancement, especially during the arterial phase, was consistent with granulation tissue.
A potential but improbable differential diagnosis in our case could include metastatic disease in renal cell cancer or a rare case of extracranial haemangioblastoma when the high vascularisation of the lesion is considered.
Conclusion
In the case of magnetic resonance contraindications CT perfusion imaging may be considered to assess the typical early enhancement of skull base paragangliomas and to differentiate these lesions from other neoplasms or mimics such as atypical vascular structures. CT perfusion imaging can also be used to evaluate the potential recurrence of paraganglioma after surgery. The typical disadvantages of CT perfusion imaging such as radiation exposure and possible side effects of contrast media containing iodine have to be taken into account before using this technique. 4D MRA remains the method of choice to evaluate paragangliomas before and after surgery.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.