
Abstract
Introduction
Orbital meningoencephalocele formation is primarily a result of congenital defects in the pediatric population and trauma of the anterior cranial fossa in adults. We present a unique case of nontraumatic nasal and orbital meningoencephaloceles presenting as bilateral proptosis with exotropia secondary to chronic hydrocephalus.
Clinical presentation
A 20-year-old male with a history of tuberous sclerosis, X-linked intellectual disability, and epilepsy presented to the emergency department with two days of nausea, emesis, seizures, and two months of progressive proptosis. Initial radiographs of the skull showed a “copper beaten” appearance, indicating chronically elevated intracranial pressure. Computed tomography imaging of the head demonstrated bilateral defects in the cribriform plate and anterior cranial fossa. Magnetic resonance imaging of the brain revealed triventricular hydrocephalus with meningoencephalocele extension into the nasal cavity and frontal horn herniation into the extraconal space of the orbits. The hydrocephalus was managed with ventriculoperitoneal shunt placement with rapid and complete resolution of the proptosis.
Conclusion
No reports have described bilateral proptosis as the presenting finding of orbital and nasal meningoencephaloceles in the absence of trauma or congenital defect. This case study demonstrates the management of meningoencephalocele formation secondary to chronic hydrocephalus.
Introduction
Both in adult and pediatric patients, proptosis is most commonly due to inflammatory processes, such as Graves’ orbitopathy. 1 Non-autoimmune causes of proptosis are generally seen in the pediatric population, and include orbital cellulitis, capillary hemangioma, optic nerve enlargement/glioma, Langerhan cell histiocytosis, and rhabdomyosarcoma.2–6 Rare causes of proptosis include congenital anomalies and trauma leading to orbital roof defects with subsequent meningoencephalocele formation.7–12 Post-traumatic hydrocephalus has been noted in two case reports of abnormal presentations of proptosis.13,14
Hydrocephalus in the absence of head trauma has been postulated as a cause of proptosis in very few instances. In 1935, van der Hoeve reported a case in which spontaneous pulsating proptosis was a consequence of hydrocephalus. 15 The increased intracranial pressure caused widening of the optic foramen, followed by herniation of the brain through this opening. A recent case of unilateral blepharoencephaloventriculocele formation was reported as a result of chronic hydrocephalus in a 12-year-old patient who was diagnosed with cerebral aqueduct stenosis at age 1, but was lost to follow-up for a decade. 16
In this report, we describe the case of a 20-year-old male presenting with severe bilateral proptosis secondary to orbital and nasal meningoencephalocele formation, which resolved following cerebrospinal fluid (CSF) diversion. To the best of our knowledge, chronic hydrocephalus causing bony defects in the anterior cranial fossa with the resultant formation of nasal and orbital meningoencephaloceles and subsequent bilateral proptosis in the absence of trauma has not previously been reported.
Case report
Clinical history
The patient is a 20-year-old male with X-linked intellectual disability and a history of tuberous sclerosis complex with significant involvement of the central nervous system. The patient underwent a right frontal craniotomy for resection of a subependymal giant cell astrocytoma (SEGA) at age 9, and subsequently a right temporal lobectomy for intractable epilepsy as a result of cortical tubers three years later. Everolimus maintenance therapy was initiated after he was diagnosed with SEGA drop metastases at the age of 13. The patient was known to have baseline supratentorial ventriculomegaly, low-lying cerebellar tonsils, and thinning of the calvarium with lucent changes in the orbital roofs eight months prior to clinical presentation.
He presented to the emergency department at age 20 with a two-day history of nausea, emesis, three tonic seizures, and a two-month history of progressive proptosis (Figure 1). On neurologic examination, the patient was alert and non-verbal at baseline. Bilateral lower extremities were contracted in plantar flexion and internal rotation. Sensation, coordination, and gate were not assessable. Ophthalmological examination revealed bilateral proptosis and exotropia in primary gaze with poorly responsive pupils. Extraocular movements were intact. Both optic nerves were pale without edema, with a cup-to-disc ratio of 0.2 in both eyes. Bilateral retinal hamartomas were also present. Optic nerve pallor was thought to result from Wallerian degeneration from cortical tubers versus long-term increased intracranial pressure, resulting in an inability to rule out an acute increase in intracranial pressure.
Clinical photograph at presentation showing bilateral proptosis with exotropia (a). One month postoperatively, proptosis and exotropia had almost completely resolved (b).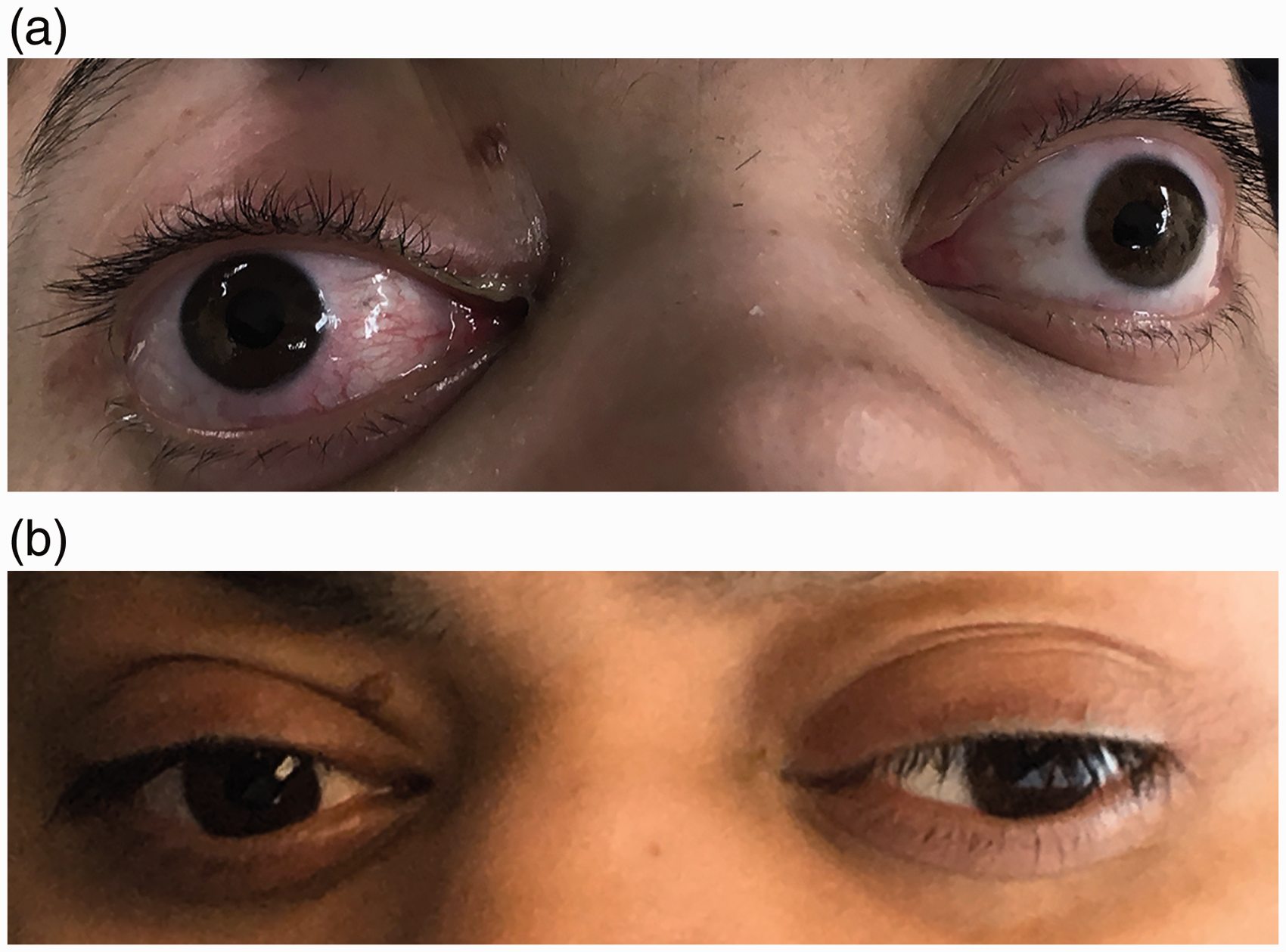
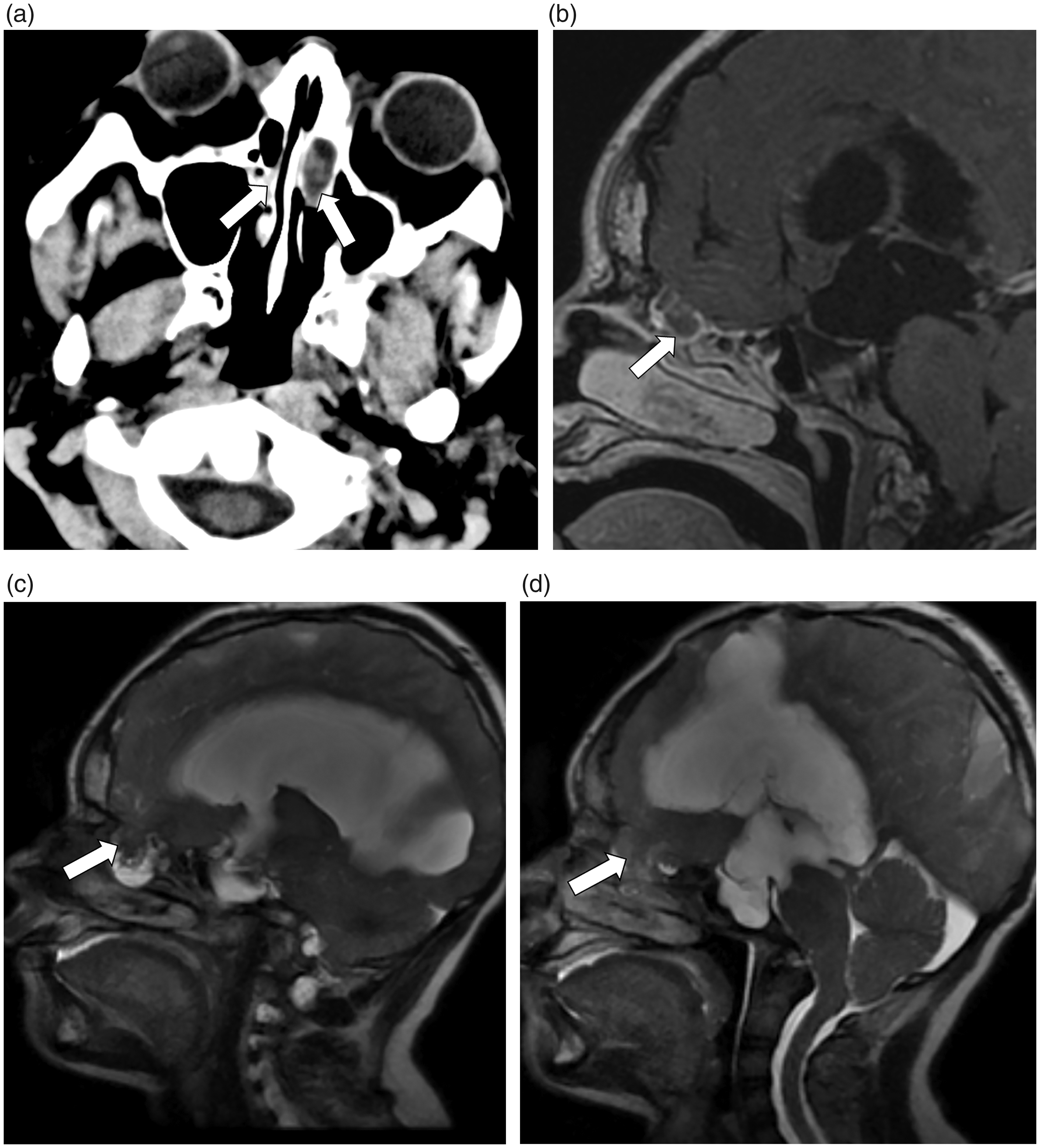
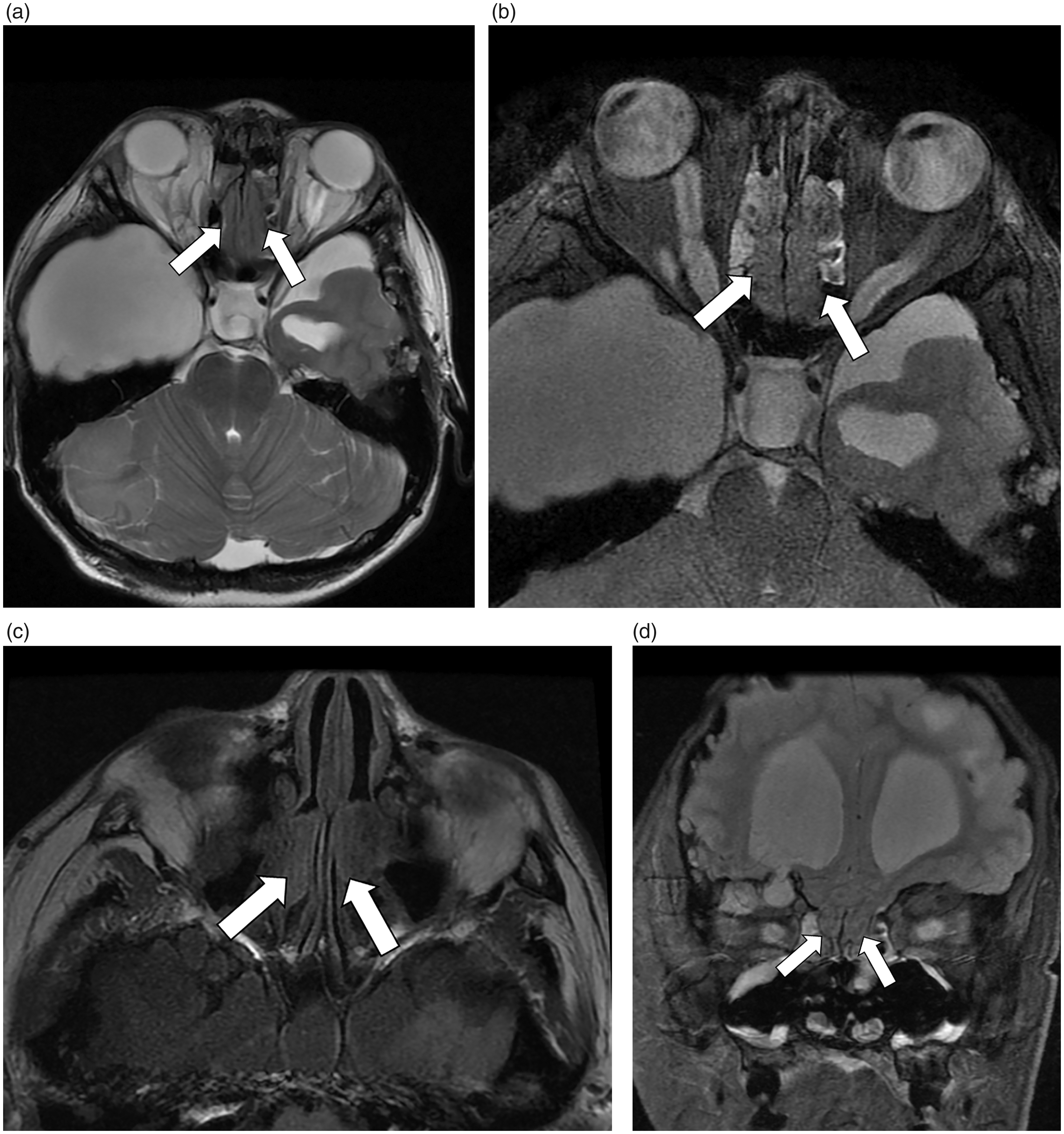
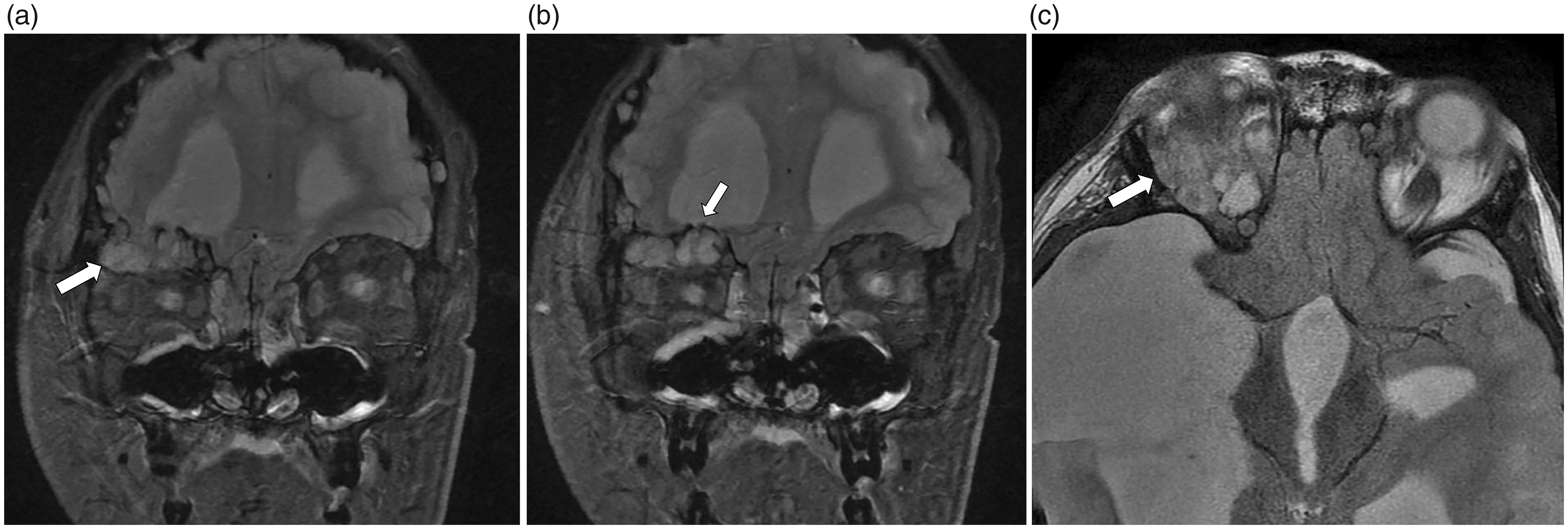
Initial scout radiographs showed a “copper beaten” appearance of the skull, which was corroborated by computed tomography (CT) imaging (Figure 2). Anterior cranial fossa bony defects were extensive. CT imaging demonstrated marked supratentorial ventriculomegaly, loculated extra-axial fluid scalloping the right temporal bone, and multifocal periventricular and cortical calcifications. Evidence of hydrocephalus and a defect in the cribriform plate was also apparent on CT and magnetic resonance imaging (MRI) of the brain (Figure 3). Bilateral defects in the cribriform plate, as well as meningoencephalocele herniation into the nasal cavity, were evident (Figure 4). Innumerable areas of arachnoid pitting in the anterior cranial fossa developed meningoencephaloceles, with herniation of the frontal horn into the extraconal space of the right orbit (Figure 5).
Lateral and oblique radiographs of the skull show the “copper beaten” appearance (a). Coronal computed tomography of the head in the bone window shows the “copper beaten” appearance of the skull (b). Axial computed tomography of the head through the anterior skull base shows bilateral defects noted at the level of the cribriform plate (arrows) extending into the nasal cavity (a). A defect in the cribriform plate (arrow) is demonstrated in sagittal T1-weighted imaging (WI) (b) and T2WI ((c) and (d)) of the brain. Hydrocephalus is also exhibited as enlargement of the third and lateral ventricles with cerebral aqueduct stenosis and cerebellar tonsil herniation ((b)–(d)). Magnetic resonance imaging of the brain shows bilateral defects noted at the level of the cribriform plate (arrows) extending into the nasal cavity. Axial T2-weighted imaging (WI) ((a) and (b)) and fluid-attenuated inversion recovery (c) images are provided, as well as coronal T2WI (d). Coronal T2-weighted imaging (WI) shows herniation of the frontal horn into the extraconal space of the right orbit ((a) and (b)). Axial T2WI shows extensive meningoencephalocele involvement within the right orbit (c).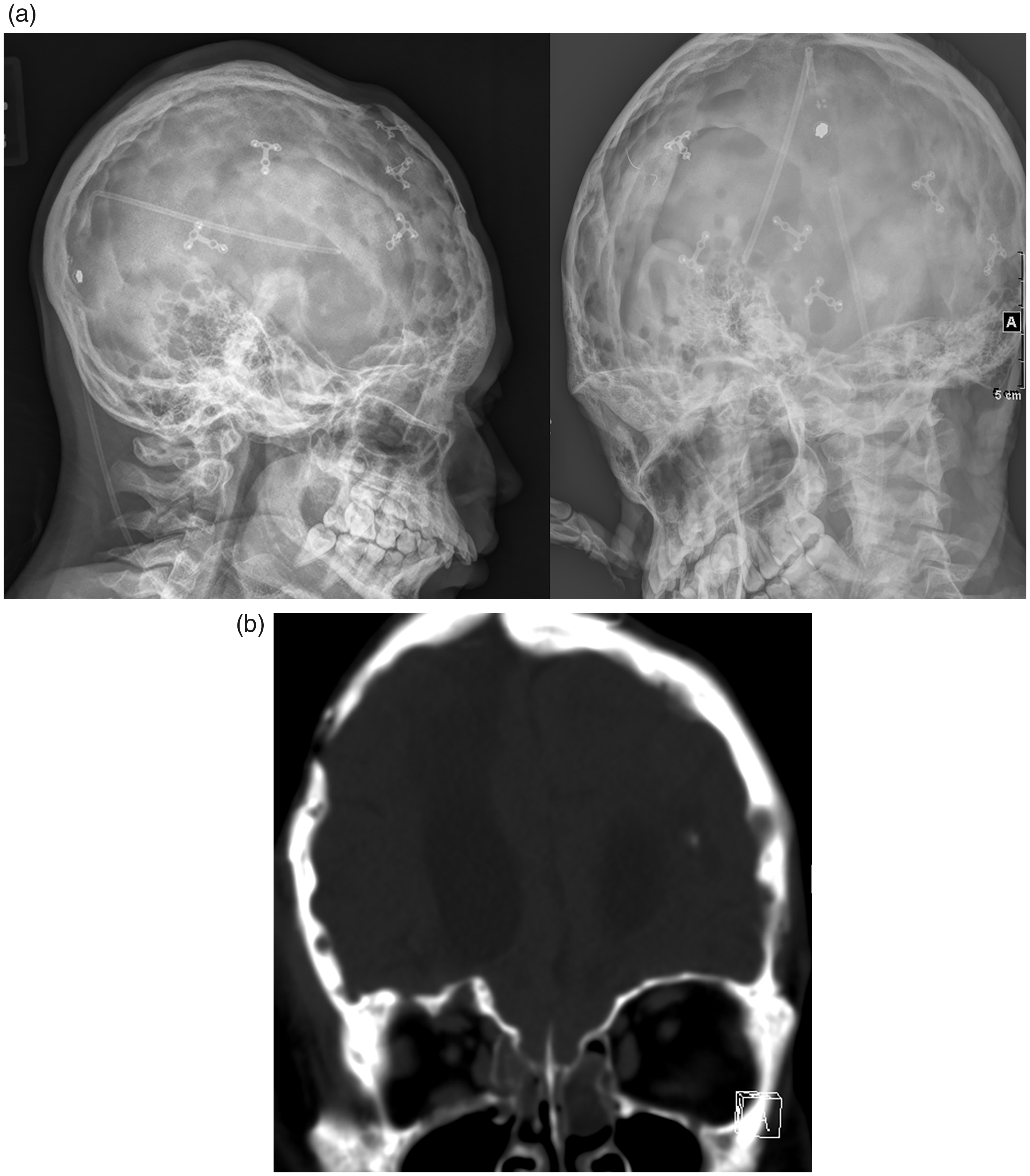
Surgical intervention
The patient was taken to the operating room. A left occipital ventriculoperitoneal (VP) shunt was placed, as the patient was not a candidate for endoscopic third ventriculostomy (ETV) because of the anatomy and configuration of the third ventricle, as well as the anterior brainstem translation. On postoperative day one, the seizures and emesis resolved, and there was remarkable improvement of the proptosis. He was discharged on postoperative day one with no interval seizures.
Post-hospitalization course
After discharge, the patient was followed in the tuberous sclerosis clinic one month later. A repeat MRI brain noted resolution of cerebellar tonsil herniation and prepontine cistern effacement, as well as the arachnoid pitting (Figure 6). Protrusion of the meningoencephalocele into the right orbital roof was markedly decreased in size, and the left orbit abnormality was no longer appreciable. On physical exam the pupils were reactive to light, and extraocular muscles were intact with no noticeable proptosis or exotropia (Figure 1).
One-month postoperative sagittal T1-weighted imaging shows resolution of cerebral aqueduct stenosis and cerebellar tonsil herniation with reduction in third and lateral ventricle size (a). Coronal T2-fluid-attenuated inversion recovery shows significant improvement of the orbital meningoencephalocele (b).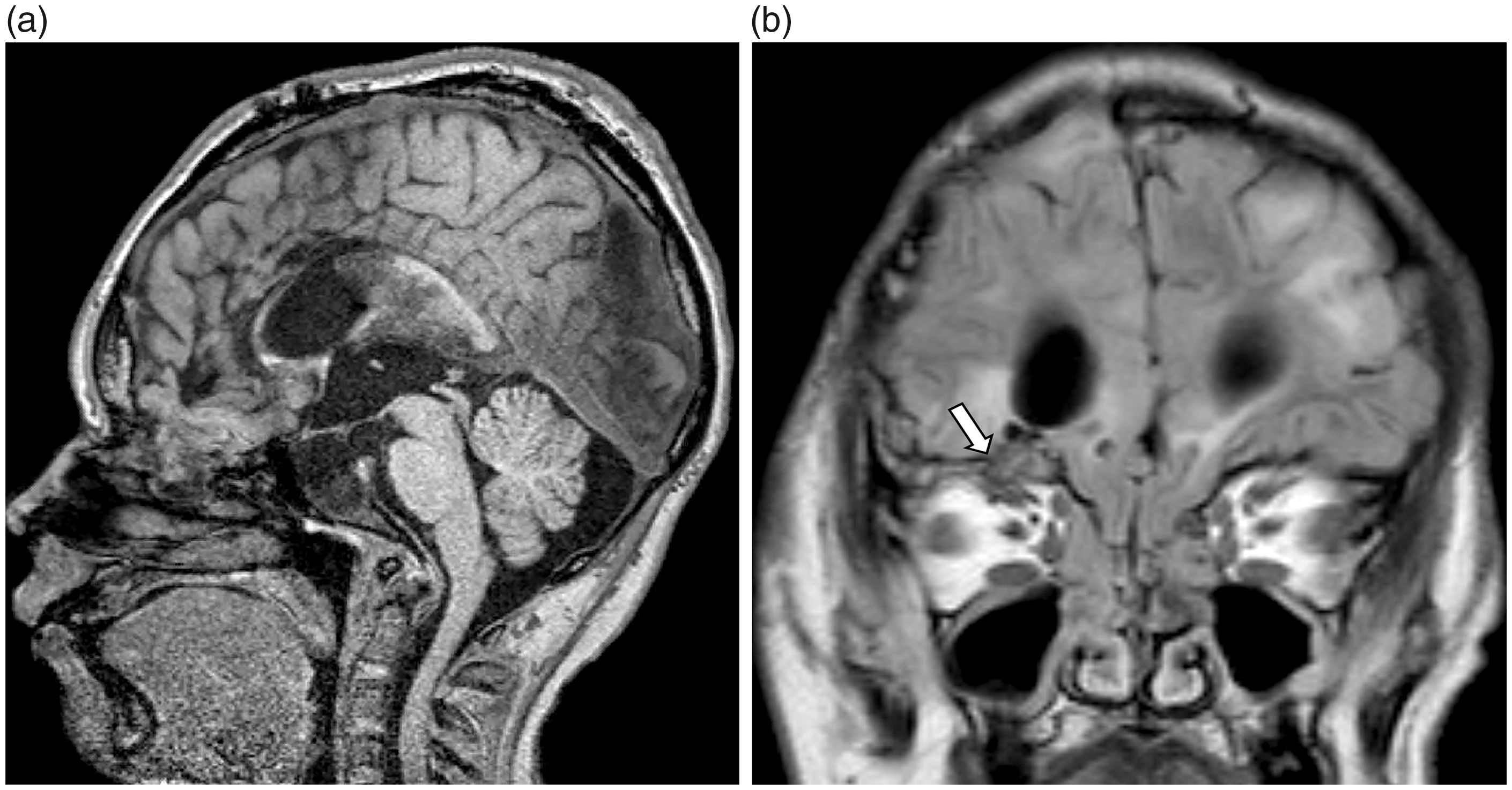
Discussion
To the best of our knowledge, no case has reported chronic hydrocephalus as the driving force for nasal and orbital meningoencephalocele formation in the absence of trauma causing bilateral proptosis. Chronic hydrocephalus as a cause of proptosis was initially reported in 1935 by van der Hoeve, and was presented as the causative factor in a recent report of unilateral blepharoencephaloventriculocele in a patient with cerebral aqueduct stenosis following a decade without medical care.15,16 Additionally, a case series describing anterior encephaloceles noted hydrocephalus as a potential cause of some anterior encephaloceles, but does not establish a clear temporal or causal description to identify hydrocephalus as the primary factor behind proptosis development. 17 However, the “copper beaten” appearance of the skull on initial radiography in this report supports a history of chronically elevated intracranial pressure, leading to increased inner table convolutional markings throughout the skull vault. The cause of chronic hydrocephalus in this patient is likely secondary to cerebral aqueduct stenosis given the patient’s baseline triventricular dilatation with a comparatively small fourth ventricle and narrowing of the cerebral aqueduct on T2-weighted images.
In patients with a history of SEGA, elevated levels of protein in the CSF are common and may contribute to hydrocephalus.18,19 Some have argued that earlier surgical intervention may avoid the sequelae of hydrocephalus. 20 However, everolimus decreases protein levels, and has been shown to help maintain proper shunt functioning.21–23 Thus, VP shunting in tandem with everolimus therapy may prolong shunt durability and is a worthwhile option in patients who are not candidates for ETV.
Regardless of the etiology of hydrocephalus, it is important to obtain both CT and MRI of the brain and orbit prior to surgery to evaluate the brain parenchyma and bony defects along the skull base or orbits. Early diagnosis and repair should be performed to relieve pressure on the optic nerve and preserve vision. Previous cases that noted hydrocephalus as a causative factor of proptosis showed adequate resolution of symptoms following CSF diversion.10,13,14,16 Similarly, we chose to clinically observe the patient’s improvement with a VP shunt. An alternative approach to VP shunt placement in cases of cerebral aqueduct stenosis is ETV, which was not an option in the current case because of the abnormal translation of the brainstem and effacement of the prepontine cistern. Some patients may benefit from additional reconstructive surgery to expose the bony defect, excise herniated tissue, and perform cranioplasty with titanium mesh or bone graft to abate recurrence.8,24 Potential sequelae of meningoencephalocele excision are scarring of adjacent brain parenchyma, which may result in seizures. Given the patient’s marked improvement with CSF diversion alone and a history of seizures, we chose not to perform reconstructive surgery. The MRI findings one month postoperatively showed significant reduction of ventriculomegaly and cerebellar herniation, and clinically the proptosis resolved. At the time of writing this report, one year after initial presentation, the patient has remained stable in regard to intracranial pressure and proptosis recurrence, and the shunt has not malfunctioned.
Conclusion
We describe a case of bilateral proptosis as the result of nasal and orbital meningoencephaloceles in the setting of chronic hydrocephalus in the absence of trauma. VP shunting without cranial reconstruction successfully provided relief within the first postoperative day, and has provided the patient with an improved quality of life and resolution of symptoms at the time of writing this report almost one year post-procedure.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication on this article.