
Abstract
Purpose
Spinal sarcoidosis, referring to involvement of the spine in sarcoidosis, is relatively rare and may mimic other neurological disease affecting the spine. The authors present a clinic radiological review of 18 spinal sarcoidosis patients who presented to a tertiary hospital, with emphasis on initial imaging and radiological response to treatment.
Materials and methods
We retrospectively reviewed our departmental imaging archives over a 15-year period and found 49 cases of neurosarcoidosis out of which 18 patients had spinal magnetic resonance imaging.
Results
Approximately 72% (13/18) of the neurosarcoidosis patients showed some form of spinal involvement. The clinical, epidemiological and imaging data were reviewed for these 13 patients at presentation and follow-up. The findings on magnetic resonance imaging included leptomeningeal enhancement (61%), pachymeningeal (23%), intramedullary enhancing lesions (38%) and bony involvement (15%). The cervical segment was most frequently involved followed by the thoracic segment. Involvement was often long segment (4.2 spinal segments) with proclivity for the dorsal cord. Mean follow-up was 23.2 months. A complete or near-complete radiological response occurred in 66% while partial response was seen in 25% patients. Four patients had isolated central nervous system involvement including one with isolated spinal cord involvement. On diffusion-weighted imaging, the apparent diffusion coefficient of intramedullary lesions was increased compared to normal-appearing cord on baseline and subsequent follow-up scans.
Conclusions
Spinal sarcoidosis was previously considered uncommon but is being increasingly recognized with widespread use of magnetic resonance imaging. Proclivity for dorsal surface involvement is characteristic, although not necessarily pathognomonic. Also, quantitative diffusion studies may serve as a biomarker for the disease activity and parenchymal injury.
Introduction
Sarcoidosis is a chronic idiopathic, multisystem inflammatory disorder with a global annual incidence of approximately 10–20 per 100,000 persons. 1 Sarcoidosis most frequently involves the lungs, skin and lymph nodes. Central nervous system (CNS) involvement is uncommon, occurring symptomatically in 5–15% of sarcoidosis patients and in about 25% of patients with systemic sarcoidosis on autopsy studies. 2 Spinal cord involvement occurring together with CNS involvement has traditionally been considered uncommon, while isolated spinal sarcoidosis (SS) is much rarer. Spinal cord involvement is non-specific, and the diagnosis is often difficult when the spinal involvement is the first clinical presentation especially in the absence of systemic sarcoidosis. The true prevalence of SS is unknown, although it has traditionally been reported in less than 1% of all sarcoidosis patients. Scattered case reports and small retrospective studies have previously described imaging findings in SS which include intramedullary lesions, cord edema, arachnoiditis and pachymeningitis.3–14 These studies have reviewed the follow-up spinal imaging for any intramedullary T2 signal changes and contrast enhancement with no other well-defined imaging biomarkers which may reflect clinical severity, response to therapy or residual neurological deficits. However, most of these studies only have a smaller number of patients and are retrospective in nature.3–14 In addition to T2 signal changes and contrast enhancement we have also evaluated the diffusion properties of intramedullary lesions which has not been attempted by previously reported studies to our knowledge.
The goal of the present study was to determine the prevalence of spinal involvement in patients with neurosarcoidosis at the time of initial diagnosis, to describe the imaging findings at presentation and on follow-up and to evaluate the apparent diffusion coefficient (ADC) values of intramedullary lesions compared to normal-appearing cord on initial and subsequent follow-up scans. We hypothesized that the spinal involvement in neurosarcoidosis patients is likely to be significantly higher than previously reported in the literature. We also assumed that despite the resolution of imaging findings with therapy, patients may show persistent neurological deficits which could reflect either ongoing inflammation at the microscopic level versus permanent injury.
Materials and methods
Demographic, clinical and imaging features of reported 13 patients with spinal sarcoidosis.
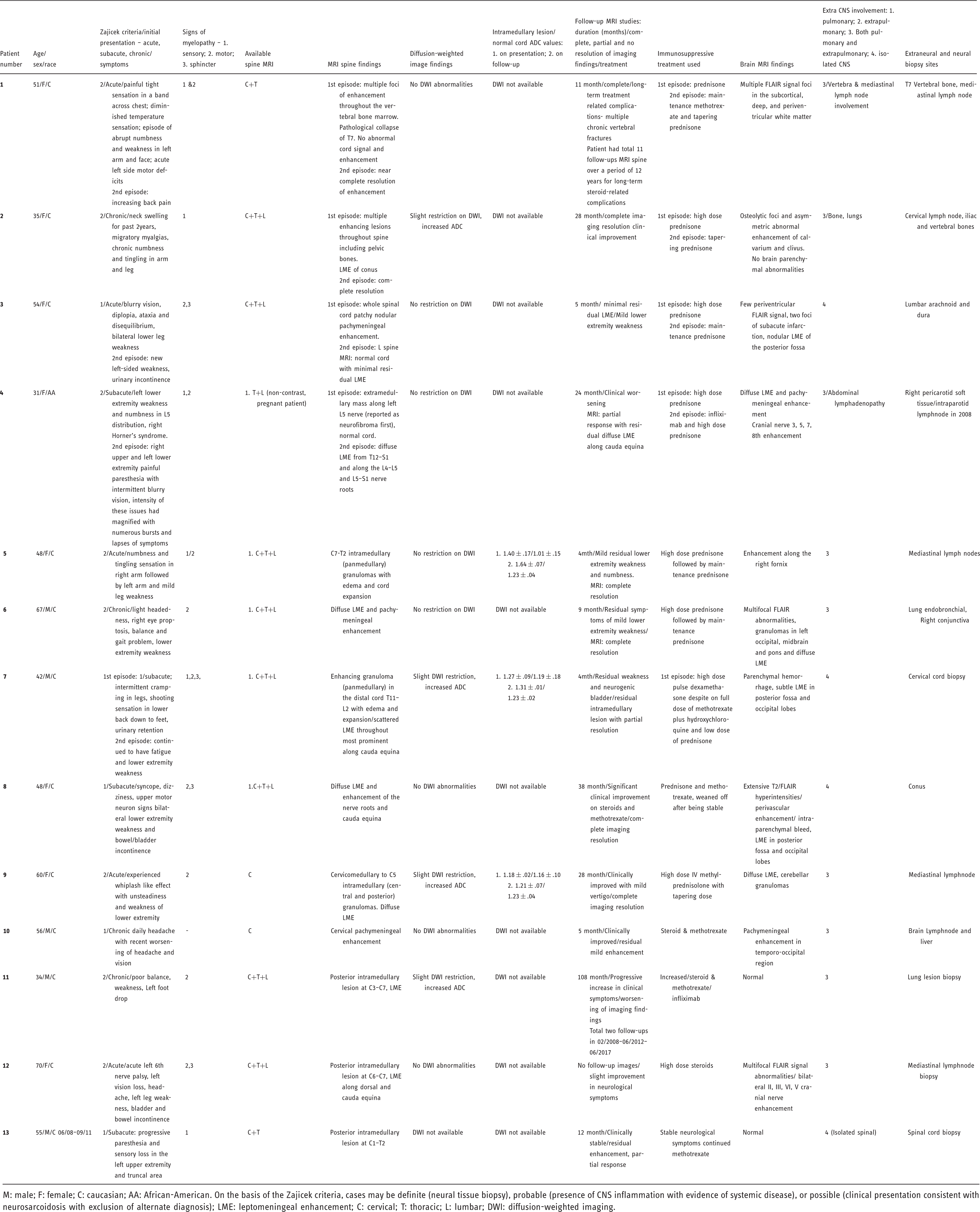
M: male; F: female; C: caucasian; AA: African-American. On the basis of the Zajicek criteria, cases may be definite (neural tissue biopsy), probable (presence of CNS inflammation with evidence of systemic disease), or possible (clinical presentation consistent with neurosarcoidosis with exclusion of alternate diagnosis); LME: leptomeningeal enhancement; C: cervical; T: thoracic; L: lumbar; DWI: diffusion-weighted imaging.
Images were acquired on either a 1.5 or 3T system. Spine MRI included standard T1-weighted imaging, T2-weighted imaging, short tau inversion recovery, and post-contrast sequences in at least one axial or sagittal plane. At the time of initial presentation all the spinal MRIs were done with contrast except for one patient who was pregnant at the time of diagnosis. Available diffusion-weighted imaging (DWI) sequences were also evaluated to assess the diffusivity of the intramedullary lesions compared with normal-appearing cord. We measured the ADC values of intramedullary lesions and normal-appearing spinal cord at initial and follow-up scans. DWI images were acquired in the axial plane with 6 mm of slice thickness and a b value of 0 and 1000 except in one patient in whom DWI was acquired in the sagittal plane. Both qualitative and quantitative evaluation of the intramedullary enhancing lesions and normal spinal cord were done on DWI. Regions of interest (ROI) were defined in areas of increased intramedullary enhancement on post-contrast axial T1-weighted sequence and copied to the DWI and ADC map. The same ROI was placed in the portion of the normal-appearing spinal cord without signal abnormality and the ADC value was measured to serve as an internal reference standard. Follow-up MRIs were evaluated for radiological response after treatment. Duration of follow-up included the time between first and last available spine MRIs. Data were expressed as mean, standard deviation and range. Percentages of positive and negative findings were calculated. We also examined the available brain MRIs of these patients for the presence or absence of associated brain lesions.
Results
Of the 18 patients with available spine MRIs, only eight patients had whole-spine MRI studies, while the remaining 10 patients had limited spine MRI at presentation (cervical and thoracic in four, thoracic and lumbar in three, only cervical in two and only thoracic spine imaging in one patient). Abnormal imaging findings on spinal MRIs were noted in 72% (13/18) of the patients. The clinical summary with imaging findings for all 13 patients is outlined in Table 1. The mean age at presentation was 50 years; age range 31–70 and a male to female ratio of 5:8. Most of the patients were white 92% (12/13) and one was African-American. According to the Zajicek criteria, five patients met ‘definite’ criteria (neural tissue biopsy) and eight patients met ‘probable’ criteria. 16 Approximately 69% (9/13) of the patients had co-existing systemic disease, often with either pulmonary or lymph nodal involvement. All patients had neurological signs at presentation and these were acute in 38% (5/13), subacute in 31% (4/13), and chronic in 31% (4/13) patients, defined as neurological clinical presentation within 1 month, 1–3 months and 3 months or more, respectively. Almost all the patients 92% (11/13) except one presented with myelopathic symptoms of motor (77%), sensory (46%) and sphincter (30%) dysfunction. The myelopathy presentation was acute in 42%, subacute in 25% and 33% in chronic. In most of our patients, the histological diagnosis of sarcoidosis was established from extra-neural organ biopsies (69%) including two vertebral bone biopsies. Neurosurgical biopsies were obtained in 38% (5/13) patients including four spinal cord and one brain biopsy. One patient had both neural and extra-neural biopsy. Biopsy revealed non-caseating granulomas in all 13 patients.
Spine and brain MRI characteristics of 13 spinal sarcoidosis patients.
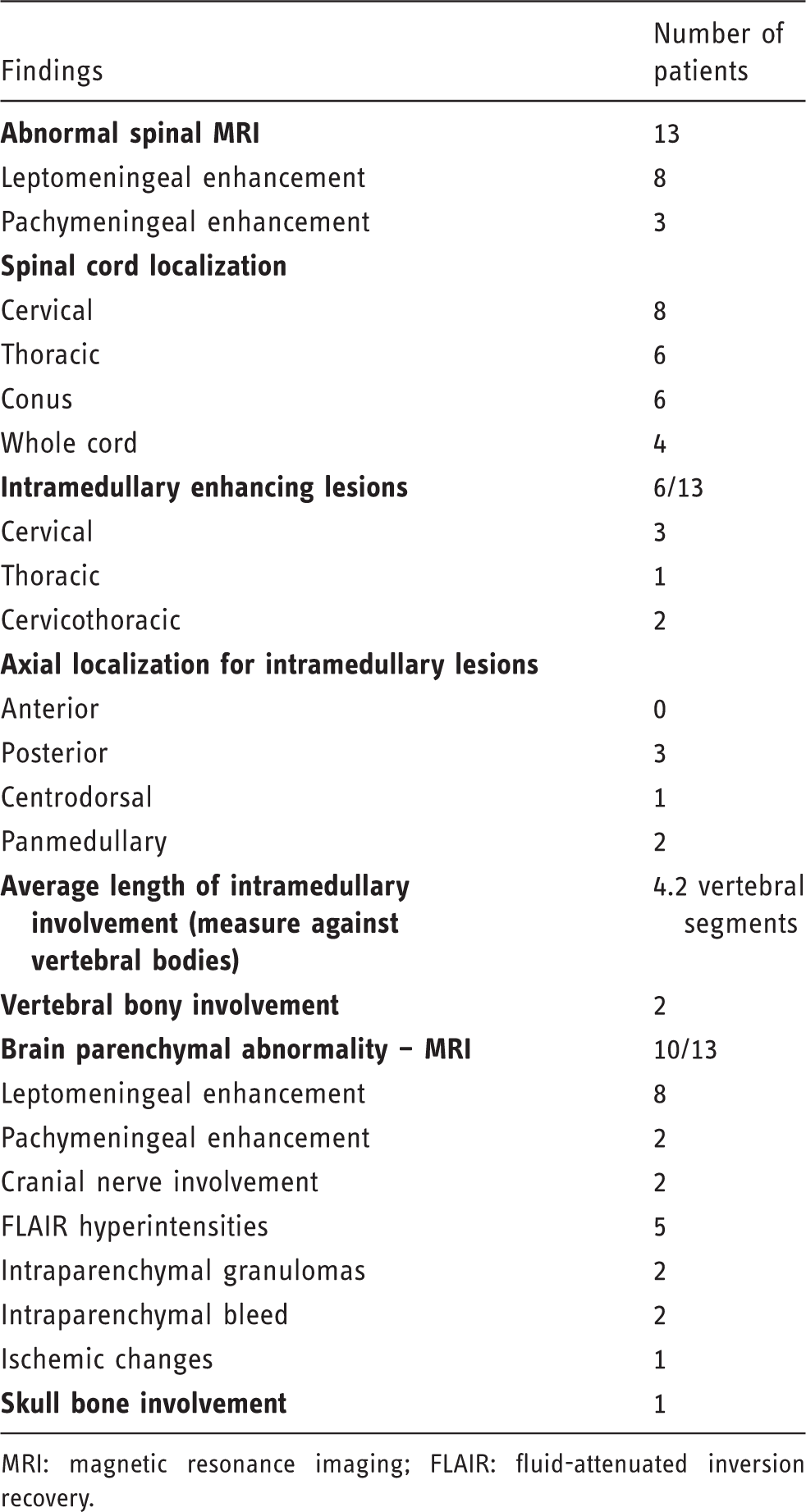
MRI: magnetic resonance imaging; FLAIR: fluid-attenuated inversion recovery.
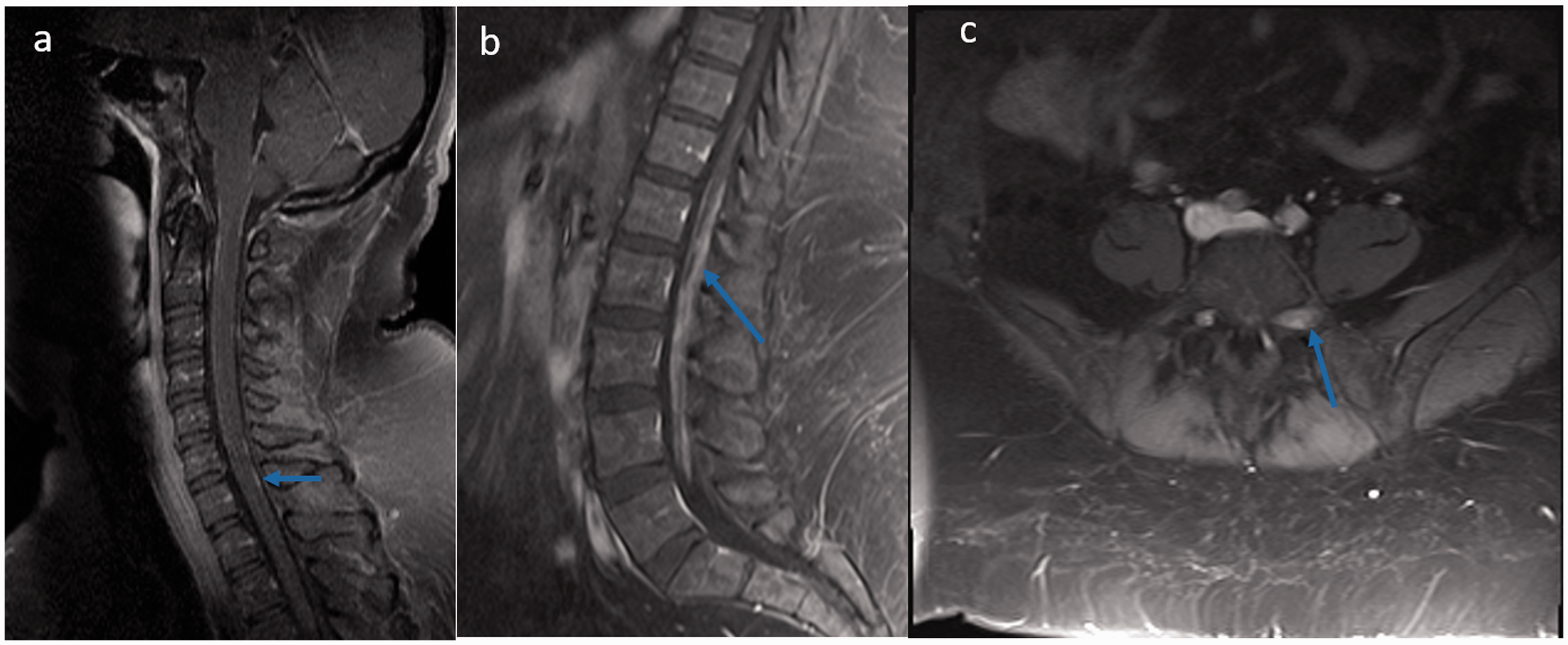
(a, b) Sagittal T1-weighted post-contrast images reveal linear leptomeningeal enhancement of cervical and nodular pachymeningeal enhancement in the conus region (blue arrows). (c) Axial T1-weighted post-contrast image reveals dorsal, extramedullary mass along left L5 nerve (blue arrow).
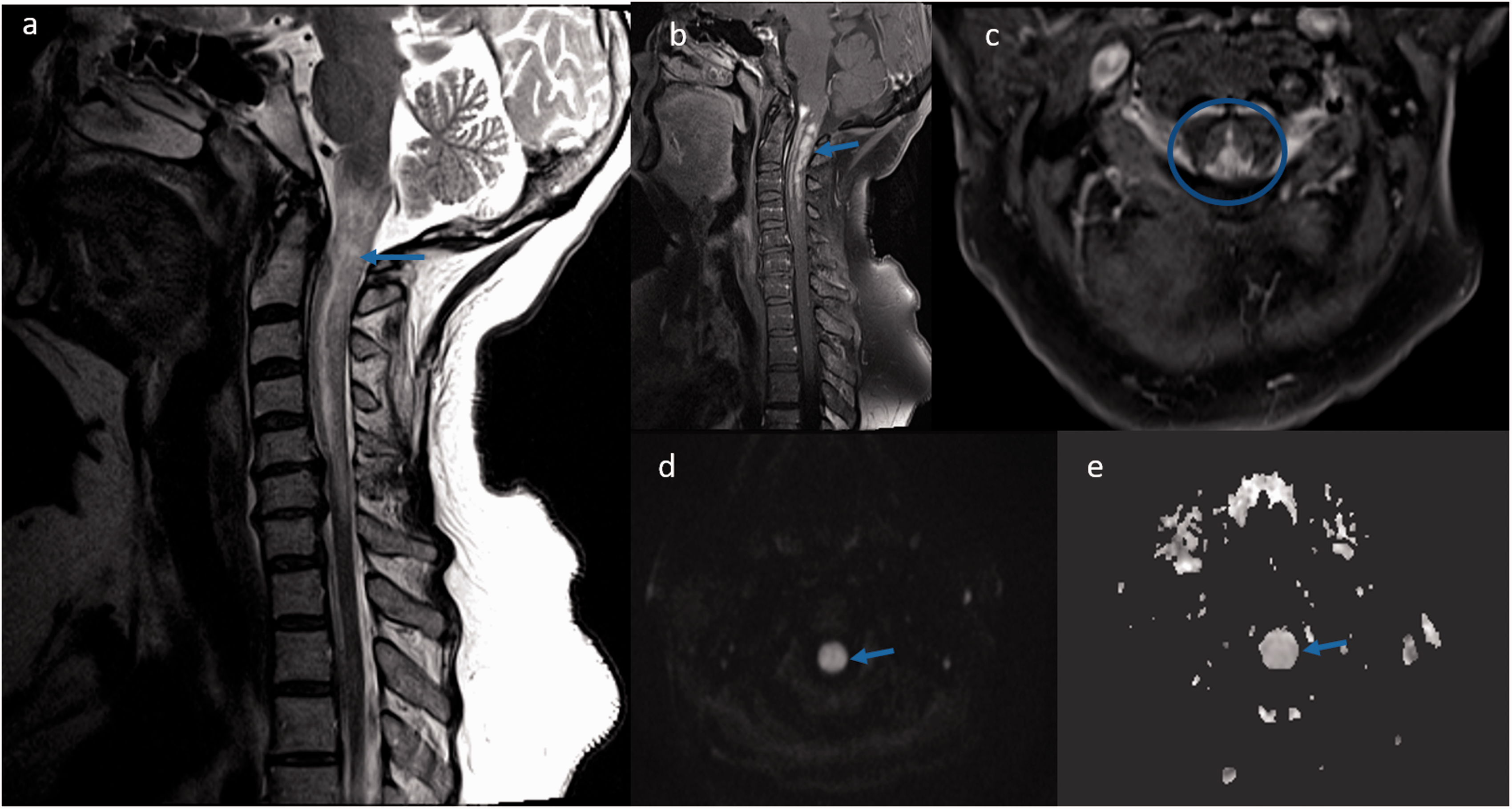
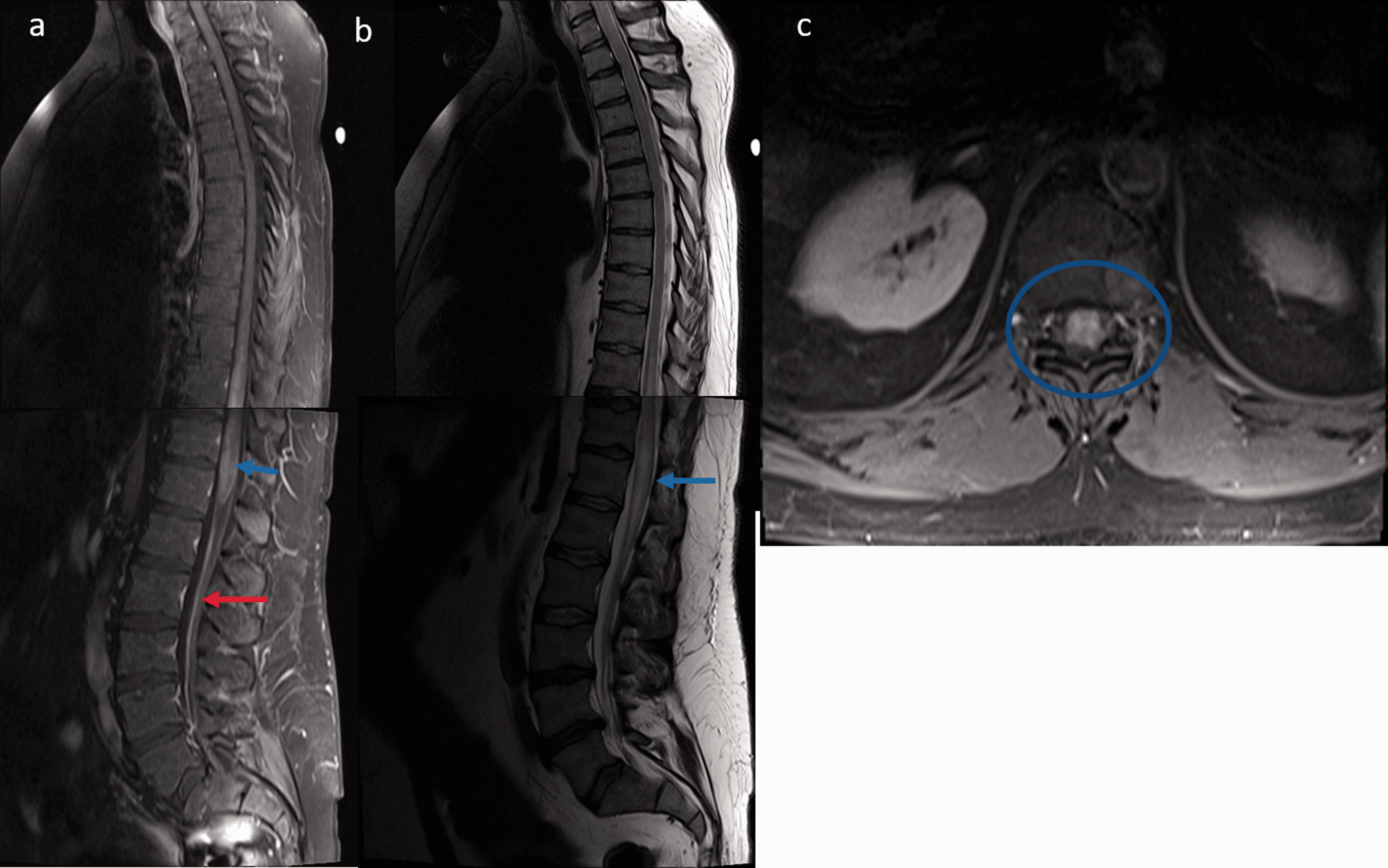
Spinal cord magnetic resonance imaging displaying lesions in cervical cord sarcoidosis: (a) Sagittal T2-weighted image displaying heterogeneous cord hyperintensities and edema in the cervical area (blue arrow); (b) T1-weighted post-contrast image showed intramedullary gadolinium enhancement in the cervico-medullary region (blue arrow); (c) Axial T1-weighted post-contrast image showed predominant posterior cord involvement (blue circle). The corresponding lesions exhibited normal to slightly increased diffusion on axial diffusion-weighted image (d, arrow) and axial apparent diffusion coefficient map image (e, arrow), reflecting vasogenic edema and inflammation.
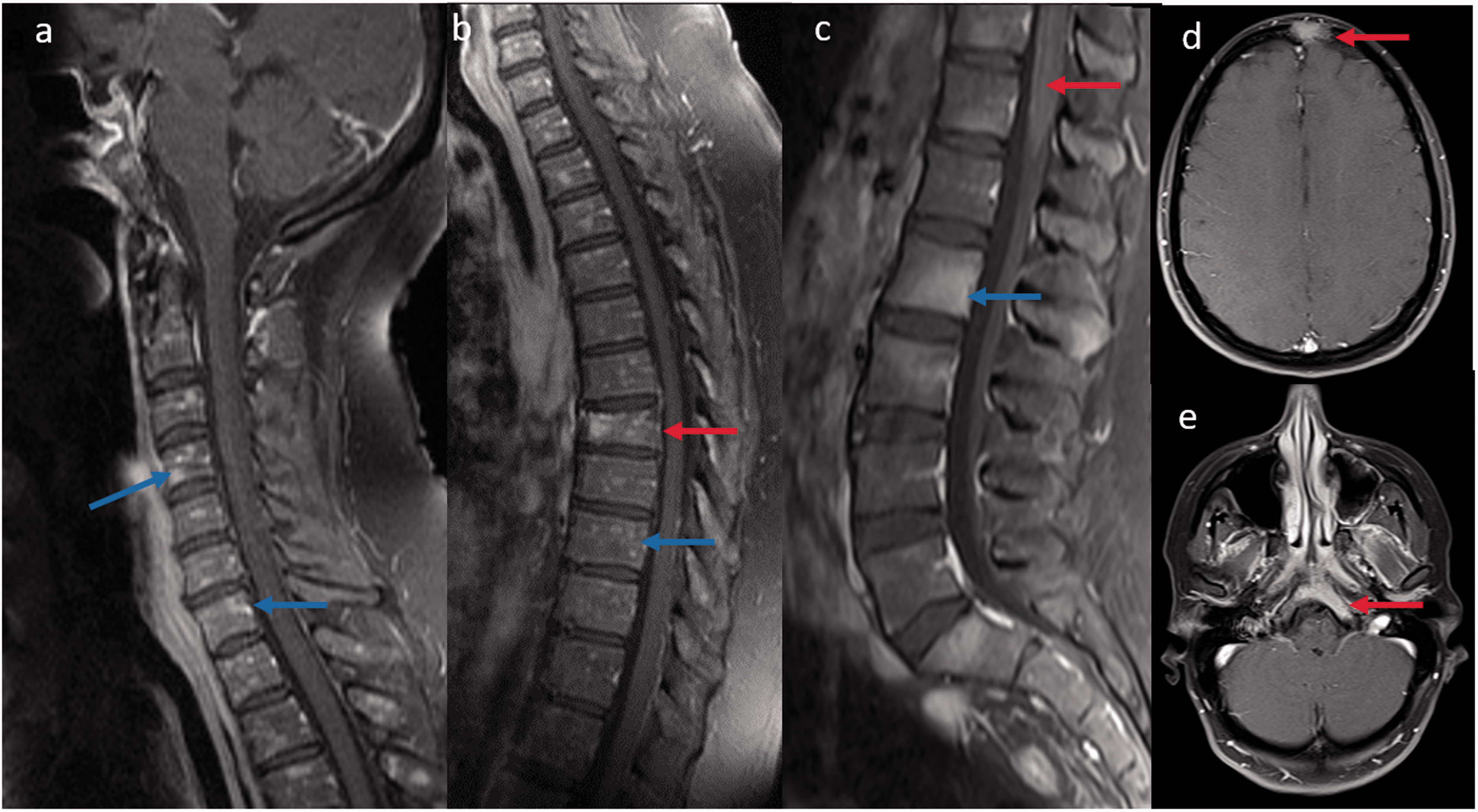
Spinal cord magnetic resonance imaging displaying lesions in spinal cord sarcoidosis: (a) Sagittal T1-weighted post-contrast imaging of whole spine revealed intramedullary gadolinium enhancement in the dorsal (T10–T12) and conus region (blue arrow) with diffuse leptomeningeal enhancement along the cauda equina (red arrow); (b) Sagittal T2-weighted image displaying heterogeneous cord hyperintensities with edema (blue arrow); (c) Axial T1-weighted post-contrast image shows panmedullary cord involvement (blue circle).
(a, b) Sagittal T1-weighted post-contrast images reveal diffuse peppered enhancement of the cervical and thoracic vertebrae bone marrow (blue arrow) without any leptomeningeal and cord involvement. Associated T7 vertebral pathological collapse (red arrow). Biopsy revealed non-caseating granuloma. (c) Sagittal T1-weighted post-contrast image in another patient reveals multifocal areas of bone marrow enhancement (blue arrow) along with leptomeningeal enhancement (red arrow). Axial T1-weighted post-contrast brain images of the same patient also showed bony enhancement of frontal and clivus (red arrow) regions.
Diffusion-weighted imaging – ADC values from intramedullary lesions and normal appearing cord on initial presentation and subsequent follow-ups in three patients.
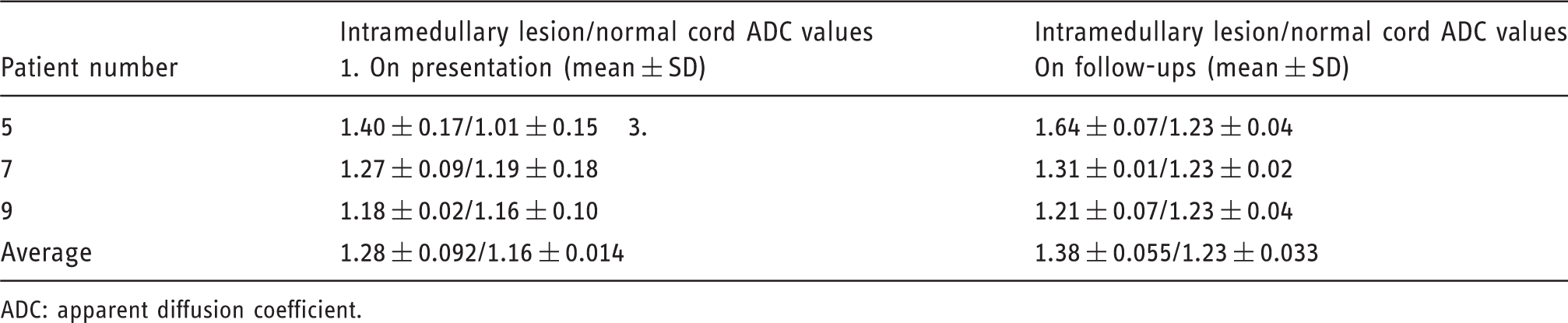
ADC: apparent diffusion coefficient.
All the patients received corticosteroids as initial treatments with the addition of immunosuppressive agents when required. Follow-up imaging was available in 93% (12/13) of patients with a total 27 follow-up scans of which one patient had 11 follow-ups for treatment-related complications. The mean follow-up period was 23.2 months with range of 4–108 months. The clinical summary for all patients is outlined in Table 1. Corticosteroids (methylprednisolone, prednisone or dexamethasone) were given to all patients as the initial treatment followed by other immunotherapeutic agents such as methotrexate (n = 5) and infliximab (n = 2) in non-responsive cases or corticosteroid-induced complications. Complete or near-complete imaging resolution with minimal residual leptomeningeal/pachymeningeal/cord enhancement was seen in eight patients (Table 1), with mean onset of imaging improvement occurring at 16 months (range 4–38 months). At the study conclusion, residual neurological deficits were present in all patients, being relatively mild in six patients. Partial response with moderate resolution of imaging findings was seen in three patients over a period of 14 months (range 4–24 months) with persistent sphincter dysfunction and significant lower extremity weakness. One patient who is currently clinically stable had numerous bursts and lapses of clinical symptoms in between and showed progressive worsening of clinical and imaging findings despite being on a full dose of methotrexate and infliximab over a follow-up duration of 108 months.
Concurrent brain MRIs showed parenchymal abnormalities in 77% (10/13) of patients. These abnormal MRI findings (Figure 5) were most commonly leptomeningeal enhancement (80%), abnormal periventricular white matter fluid-attenuated inversion recovery (FLAIR) hyperintensities (50%), cranial nerve involvement (20%), enhancing intraparenchymal granulomas, bleed (20% each), and subacute infarct (10%). MRI brain findings are summarized in Table 2.
(a–f) Axial brain magnetic resonance imaging showing associated abnormal brain findings.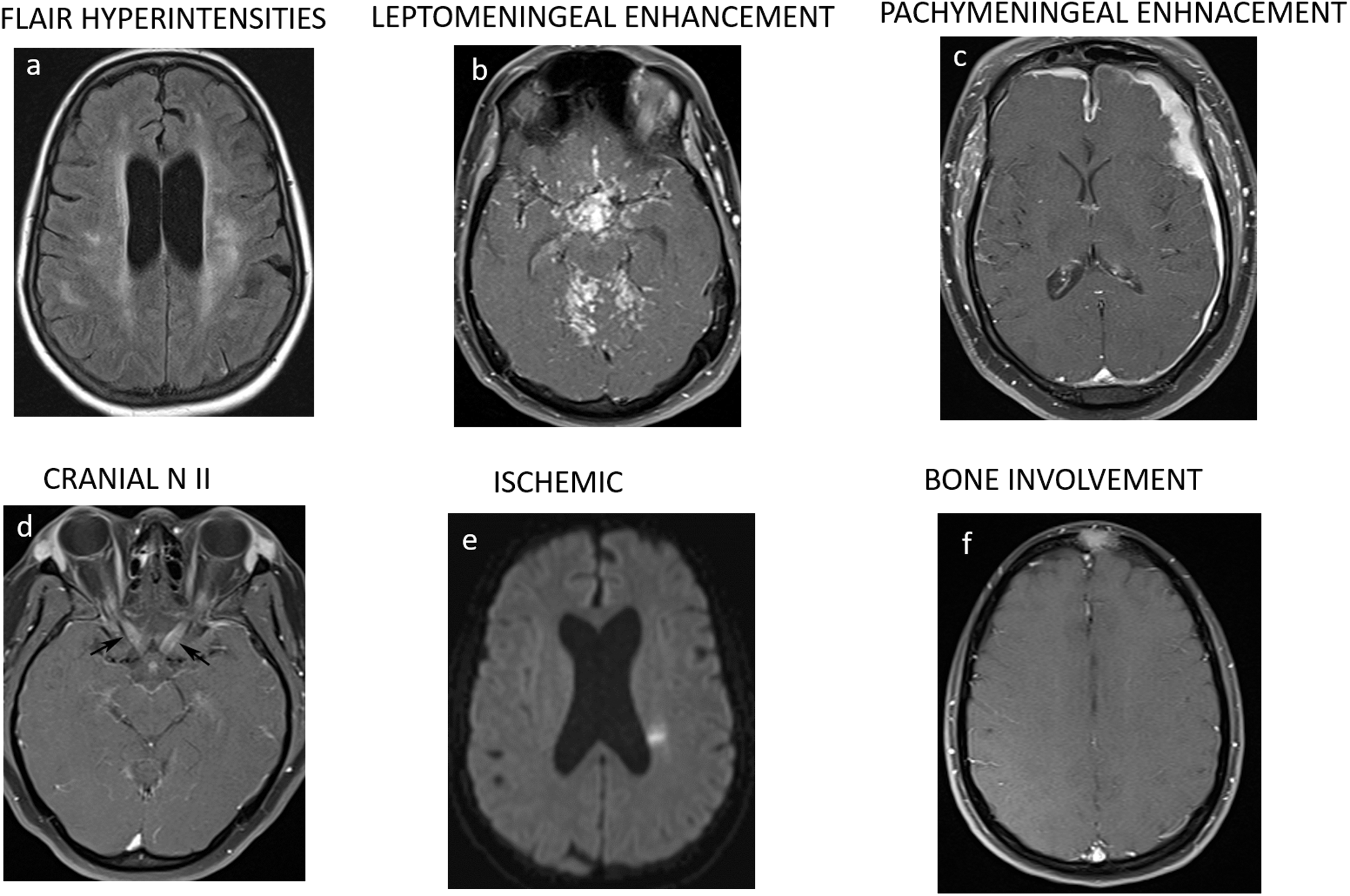
Discussion
Spinal involvement was traditionally considered rare in sarcoidosis patients but can encompass a large spectrum of manifestations such as leptomeningeal, pachymeningeal, intramedullary and rarely vertebral bodies. The clinical presentation of SS mimics other myelopathies and manifests with sensory, motor, bladder and bowel dysfunction. MRI is very sensitive to localize the lesions; however, imaging appearances are less specific and highly variable. The diagnosis of SS is challenging especially in the absence of systemic sarcoidosis; therefore, the evaluation of extra-neural sarcoidosis is usually performed to avoid invasive neural tissue biopsy.7,9,10 In the present study, we retrospectively analyzed the clinical and imaging manifestations of 13 SS patients including subsequent follow-ups to evaluate the long-term imaging response to treatment. The clinical presentation of the 13 SS cases was in concordance with the previously reported studies in the literature.3–14 As reported earlier, there was a female dominance and most patients were in the 35–45 year age group. All the patients in the current study experienced neurological symptoms at the time of the initial sarcoidosis diagnosis, and 92% of patients presented with myelopathic symptoms of sensory, motor and sphincter dysfunction including two patients with characteristic ‘corset-like’ neuropathy presentation. 17
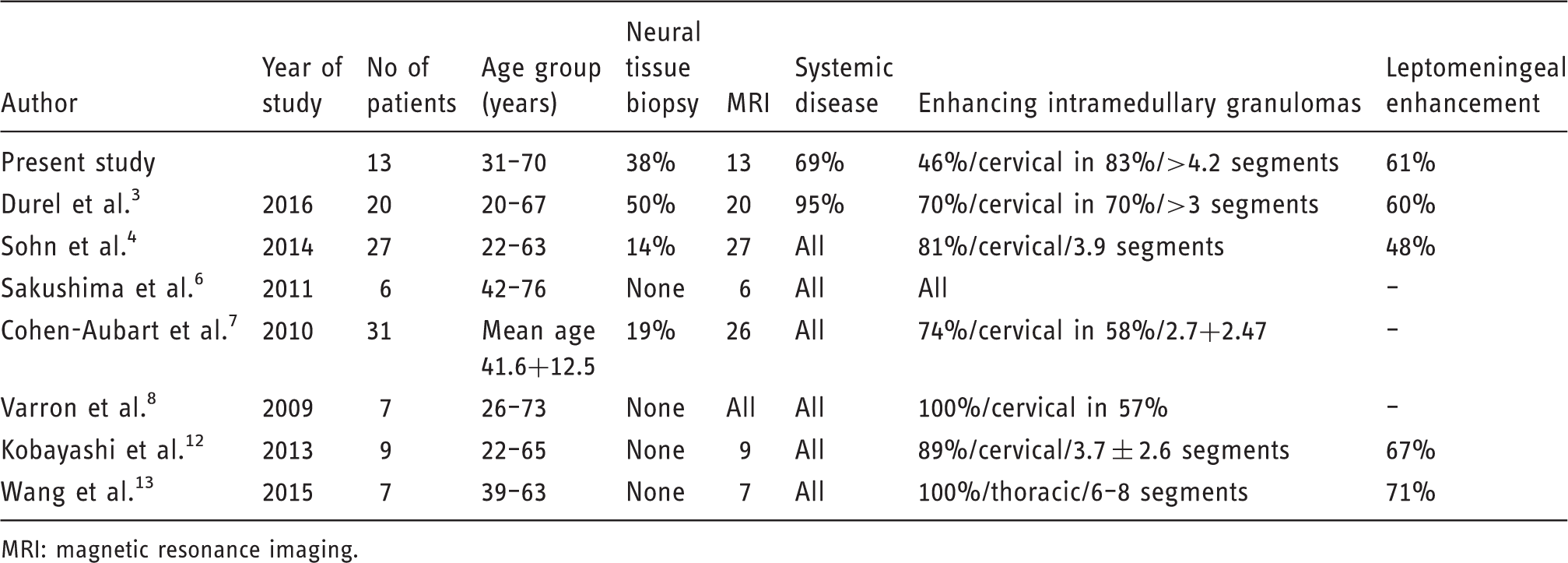
Cases of spinal sarcoidosis in the reported English language literature.
MRI: magnetic resonance imaging.
Spinal cord sarcoidosis can occur at any spinal level, although cervical (56%) and thoracic segment (37%) involvement was found to be more common compared to lumbosacral involvement, as reported by previous studies.3–14 The average length of the spinal cord involvement by enhancing intramedullary granulomas was found to be long and spanned for 4.2 vertebral segments, which may be an important clue in differentiating SS from other neurological disease mimics.3,4,6 Furthermore, axial images may be of importance in localizing the intramedullary granulomas and a propensity for the dorsal cord.3,4,12,13
All the intramedullary lesions exhibited normal to slightly increased diffusivity with correspondingly increased values at the ADC map image, reflecting vasogenic edema and inflammation. Kobayashi et al. also reported iso to high signal intensity with normal to slightly increased diffusion on DWI in two patients with intramedullary lesions, reflecting vasogenic edema and inflammation. 12 We also evaluated quantitative diffusion in a small subset of patients with intramedullary lesions on first and subsequent follow-up scans. We noticed increased ADC in the intramedullary lesions compared to the normal cord on baseline and subsequent follow-up scans despite being imaging resolution of enhancement and edema. This suggests either continued ongoing neural inflammation versus underlying tract injury, and probably requires further assessment with high resolution MRI and quantitative diffusion tensor imaging (DTI) studies of the spinal cord. Despite the presence of DWI in most of the MRI studies in the current series, we did not find any acute cord infarcts, even though spinal infarcts have previously been documented on autopsy studies. This may be because of the high slice thickness on our diffusion-weighted images (6 mm). It is possible that higher resolution imaging may show such infarcts which likely to be are currently underdiagnosed on imaging.
A few studies have also reported sarcoid vasculitis-related rare cerebrovascular complications of infarct and bleeding in neurosardoidosis patients.15,18–20 Nagai et al. reported an autopsy finding of an intramedullary sarcoidosis with marked atrophy in the cervicothoracic segments and loss of normal grey and white matter structures. 21 Microscopically, the parenchyma of the spinal cord was necrotic and studded by numerous granulomatous nodules in a perivascular distribution, with intense perivascular infiltration of lymphocytes which contributes to spinal cord necrosis due to ischemia from arterial obliteration. 21 A rare published case report of spinal cord hemorrhage in a neurosardoidosis patient who had been on long-term corticosteroid treatment, recently highlighted the possibilities of spinal cord hemorrhage secondary to sarcoid vasculitis. In our study, we have not encountered any similar case of intramedullary hemorrhage, although susceptibility sequences sensitive for hemorrhage detection was not available in any of the patients. 22
Isolated involvement of the spinal cord by sarcoidosis in the absence of brain and systemic involvement is extremely rare. This needs to be neurologically and radiologically differentiated from other mimickers such as neuromyelitis optica spectrum disorders to prevent delayed diagnosis and treatment. Neuroimaging findings suggestive of SS are subpial gadolinium enhancement extending two or more vertebral segments and persistent enhancement for over 2 months after corticosteroid treatment, whereas ring-like enhancement is more common in neuromyelitis optica spectrum disorders. 23
In our series, we encountered one case of isolated intramedullary sarcoidosis in which the patient presented with cervical myelopathy. The diagnosis was established after spinal cord biopsy and treated with high-dose steroids followed by methotrexate. After 12 months of adequate treatment, the patient was clinically stable with persistent sensorimotor paraparesis and the neuroradiological findings partially remitted.7,24 Another study by Saleh et al. found only one biopsy-confirmed case of true isolated spinal cord sarcoidosis, further highlighting the rarity of the disease. 25
Brain MRIs were more frequently reported to be abnormal in SS, and we found brain parenchymal abnormalities in 70% and bony calvarium involvement in 10% of our cohort of patients.3,7,12 Such findings are important in narrowing the differential diagnosis and guiding the diagnostic algorithm. In our study, leptomeningeal enhancement and FLAIR signal abnormalities were predominantly reported, and our results were concurrent with the previously reported literature.3–7,12,13 CNS bleeding and ischemia are rare complications of neurosarcoidosis and we found two such cases of subacute infarct and parenchymal bleed in this cohort.15,21
In general, osseous involvement in sarcoidosis ranges from 1% to 13% and is felt to be underestimated as most of the lesions are clinically asymptomatic. It most commonly involves the tubular bones of the hands and feet, with less frequent involvement of the skull and vertebral column, located mainly in the thoracolumbar region. 26 The radiographic pattern of involvement varies between purely lytic to mixed lytic sclerotic lesions on computed tomography. MRI is sensitive for bone lesion detection but is not specific for the diagnosis of sarcoidosis. Lesions are usually T1 hypointense with variable T2 signal intensity and enhance on contrast administration. Histological proof is required to exclude the numerous other possibilities such as metastasis, lymphoma and infections.27,28 In our case series, we have found two biopsy-confirmed cases of vertebral bone involvement, with exclusive bone involvement in one patient (Figure 4) including the skull and pelvic bones. One patient had peppered lesions (Figure 4(a,b)), while the other had more ill-defined lesions (Figure 4(c)) on MRI which were both lytic and sclerotic on computed tomography.
SS may be refractory to treatment and frequently requires immunosuppressants in addition to corticosteroids in non-responsive refractory cases. In our study, additional immunosuppressants were given to seven patients who were resistant to steroids. We reported complete or near-complete imaging resolution in eight patients, with residual mild neurological deficits in six patients. Partial imaging response with persistent sphincter dysfunction and significant lower extremity weakness was reported in three patients. One patient had progressive worsening of clinical and imaging findings despite being on a full dose of methotrexate and infliximab. Clinical findings do not always parallel MRI findings and despite improvements in MRI findings over the follow-up period, a sufficient number of the patients displayed functional disabilities.4,7,29 The question as to how disease activity in neurosardoidosis should be monitored is not clear and no reliable imaging biomarkers have yet been identified. Our observations of alterations in ADC values which persist despite resolution of contrast enhancement, although noted in a small subset of patients, raise the possibility that ADC values and DTI may be helpful as an imaging biomarker. We proposed a larger, prospective quantitative diffusion study to explore further the possibility of DTI as an imaging biomarker.
The limitations of our study include its retrospective nature and a small sample size, which are not uncommon given the rarity of this disease. Due to the small sample size and absence of any comparison group we were not able to conclude any statistical significance. Other limitations include referral bias as the study was performed at a tertiary care center, and also a geographical bias of a mid-west population base which was reflected in the composition of our cohort. Similarly, whole-spine MRIs were not available in all the patients which might have biased the distribution of findings. Finally, DWI sequences were acquired with slice thickness of 6 mm which probably precluded the detection of ischemic lesions.
Despite these limitations, our study observations support the previously reported findings and strengthen the existing literature on this rare disease. Given the positive imaging findings in a large number of patients with SS, these also argue for routine spinal imaging in patients with neurosarcoidosis. The strengths of our study include the presence of a tissue diagnosis in all patients and evaluation of ADC values in intramedullary lesions. The observation that the ADC values did not return to baseline despite the resolution of contrast enhancement raises interesting questions which need to be addressed in future studies.
Conclusions
SS was previously considered uncommon but now is being increasingly recognized with the widespread use of MRI. The predominance of dorsal cord involvement is characteristic, although not necessarily pathognomonic. Other imaging findings include diffuse leptomeningeal and nerve root enhancement, with concomitant intramedullary enhancing granulomas spanning more than three vertebral segments with predilection for cervicothoracic segments. In line with previous studies, these findings are helpful to distinguish SS from other neurological disease primarily affecting the spinal cord. Also, evaluation of ADC values may serve as an important imaging biomarker and its role needs to be explored further.
Footnotes
Acknowledgment
This paper was presented at the American Society of Neuroradiology Annual Meeting 2017.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.