
Abstract
Susac’s syndrome is an uncommon autoimmune microangiopathy characterised mainly by encephalopathy, hearing loss and branch retinal artery occlusions. We present here a case of Susac’s syndrome with initial isolated arterial stroke symptoms which are not an uncommon feature of the disease.
Case report
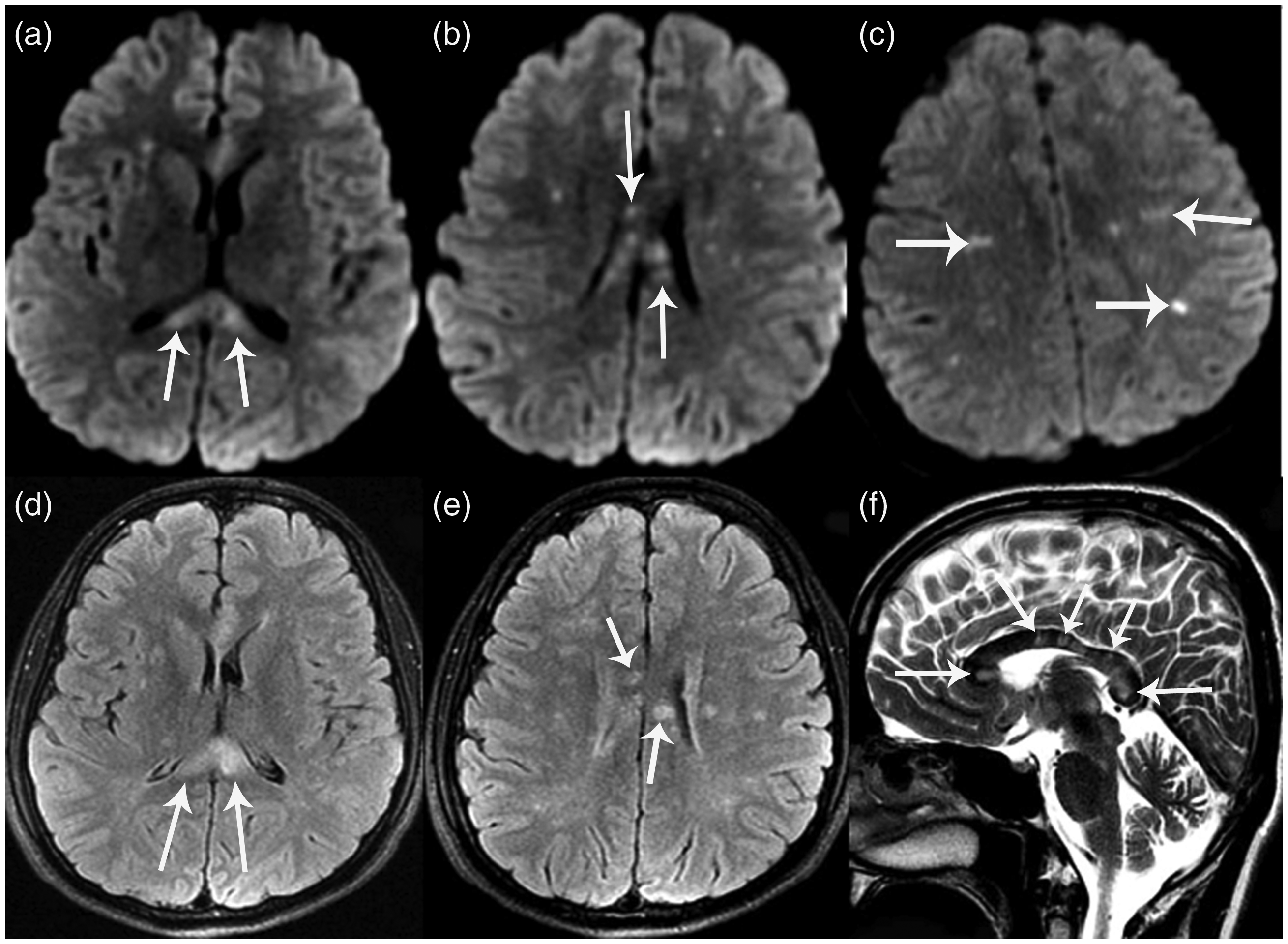
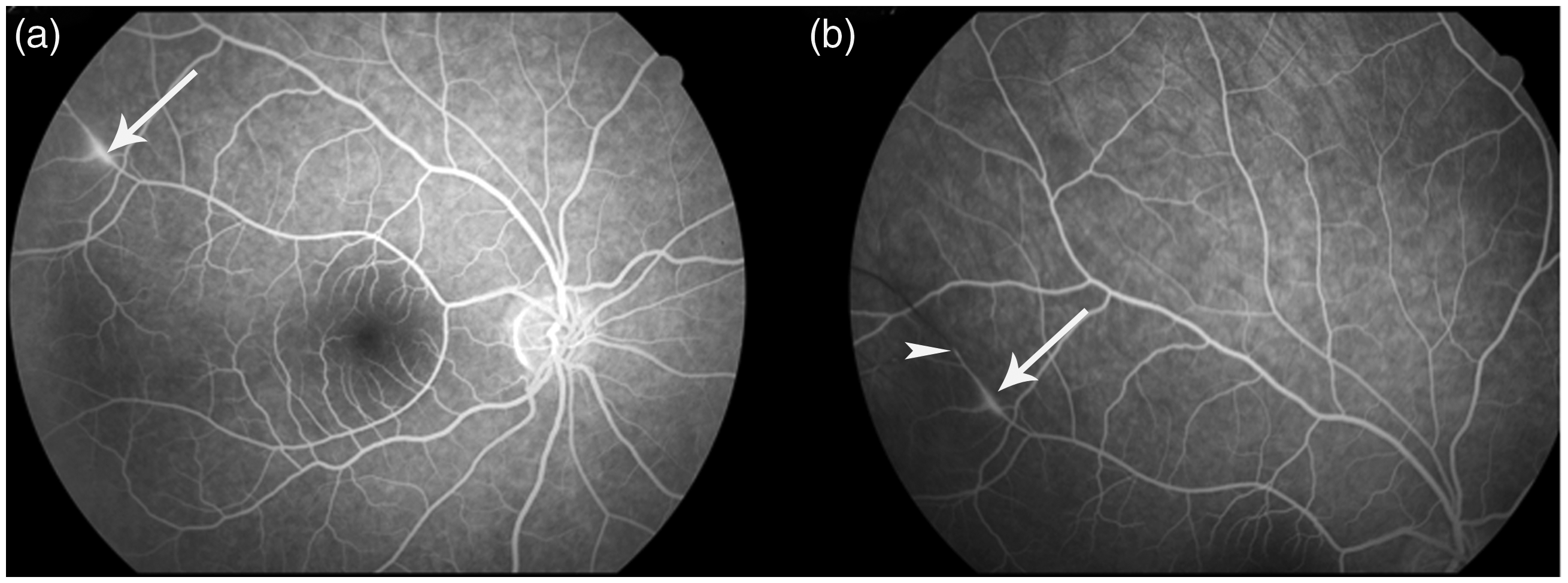
A 32-year-old male patient presented to the outpatient clinic with paresthesia in the right hand, progressive headache and nausea. His medical history was uneventful, and physical examination did not show any pathologies. On magnetic resonance imaging (MRI) of the brain, multiple small foci of diffusion restrictions were seen in the periventricular white matter and splenium of the corpus callosum. A left corona radiata hyperintense signal was also seen on fluid-attenuated inversion recovery (FLAIR) sequence without restricted diffusion (Figure 1). The patient was internalised to our neurology inpatient clinic with a diagnosis of arterial stroke. The results of non-invasive vascular and cardiac imaging studies and laboratory studies, including autoimmune and thrombosis panels, were normal. Lumbar puncture revealed increased opening pressure, a few mononuclear cells, an elevated protein level of 186.4 mg/dL and an elevated IgG index (0,71). On the third day of hospitalisation, the patient’s cognitive state had deteriorated, with memory loss and confusion. Repeated MRI of the brain showed multiple expanded restricted diffusions, with new ones in the periventricular white matter and corpus callosum. Recognition of the callosal involvement pattern suggested the diagnosis of Susac’s syndrome (SS) (Figure 2). Thus, a retinal fluorescein angiography was recommended. Superior temporal arteriolar occlusion and arteriolar wall hyperfluorescences on the right eye were found, confirming the diagnosis (Figure 3). The patient was unable to cooperate with a hearing test due to encephalopathy. He was treated with intravenous methylprednisolone and intravenous immunoglobulin, and was in full recovery on the day of discharge.
Initial magnetic resonance imaging of the brain. (a–c) Axial diffusion-weighted images show multiple small foci of diffusion restrictions in the splenium of the corpus callosum (arrows in (a)) and in the periventricular white matter (arrows in (b) and (c)). (d) A left corona radiata hyperintense signal (arrowhead) and hyperintense lesions in the splenium of the corpus callosum (arrow) are seen on an axial fluid-attenuated inversion recovery (FLAIR) sequence. (e) There is no lesion on the axial FLAIR image through the level of the corpus callosum. (f) There is normal-appearing corpus callosum parenchyma except the splenial lesions (arrow) on the sagittal T2-weighted image obtained through the midline. Repeat magnetic resonance imaging of the brain. (a–c) Axial diffusion-weighted images show multiple expanded restricted diffusions with new ones in the periventricular white matter and corpus callosum. Axial fluid-attenuated inversion recovery images through the level of the corpus callosum (d, e) and sagittal T2-weighted image through the midline (f) show snowball lesions (arrows) whose central location in the callosum makes them pathognomonic of Susac’s syndrome. Retinal fluorescein angiogram of the right eye (a, b) shows inflamed retinal arterioles with arteriolar wall hyperfluorescences (arrows) and superior temporal arteriolar occlusion (arrowhead), confirming the diagnosis of Susac’s syndrome.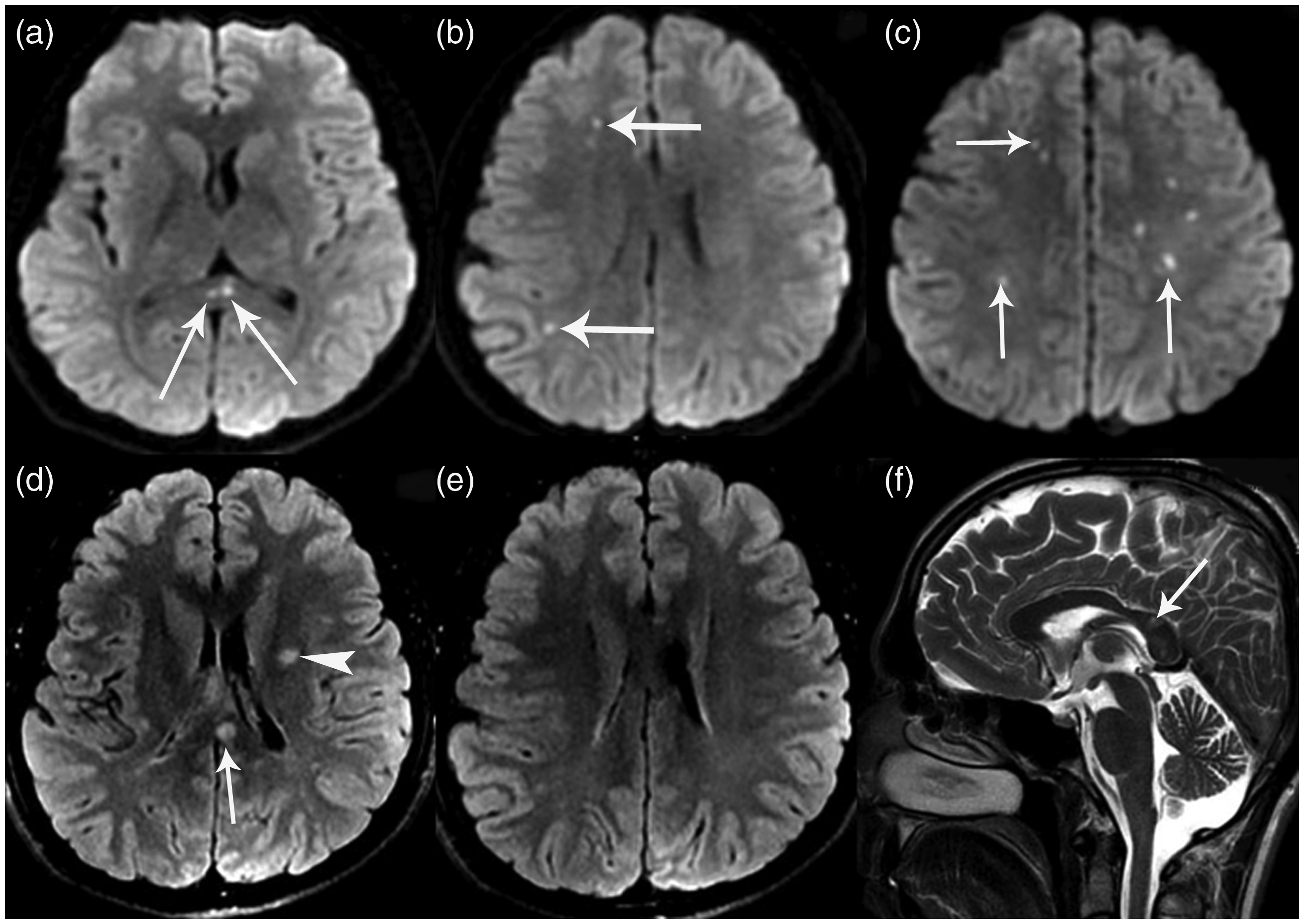
Discussion
SS is a rare autoimmune microangiopathy of the brain, eye and ear. It most commonly affects women in the second to the fourth decades of life. No familial cases have been reported. Patients may present with a pathognomonic clinical triad of acute or subacute encephalopathy, sensorineural hearing loss and vision distortion.1,2 The presentation with the full clinical triad of symptoms is approximately 13%. At clinical onset, the most common manifestation was central nervous system symptoms (67%), followed by visual symptoms (40%) and hearing disturbances (37%). Headaches were present in about 80% of patients at the beginning. During the course of the disease, the complete triad was documented in 85% of cases. 3 There is also a neuroimaging triad of white matter lesions, deep grey matter lesions and leptomeningeal disease. The frequency of supratentorial white matter lesions, supratentorial grey matter lesions and leptomeningeal enhancement was reported as 98%, 42% and 51%, respectively. 3 SS is definitely diagnosed when the clinical triad or the neuroimaging triad is present. 4 However, this disease may pose a diagnostic challenge when the clinical triad is incomplete. MRI then plays an important role in making a correct diagnosis, because callosal lesions are considered almost pathognomonic. The most common characteristic callosal finding is the presence of microinfarcts in its central portions of the body and splenium as snowballs with relative sparing of the periphery when acute, and as ‘punched out’ holes when chronic. The callosal roof may also be involved by microinfarcts in ‘icicle’ and ‘spoke’ configurations. A ‘string of pearls’ appearance due to punctate microinfarcts involving the internal capsule is another MRI finding of the disease.1–4 These imaging findings together with arteriolar wall hyperfluorescences on fluorescein angiography in retinal arterioles are also diagnostic of SS.4,5 The main differential diagnoses include central nervous system vasculitic disorders, multiple sclerosis, acute disseminated encephalitis and connective tissue disorders. 6 Optimal treatment still remains unknown. It involves the use of immunomodulation and/or anticoagulation or antiaggregation. Prompt and aggressive treatment with corticosteroids and immunoglobulin are the mainstay of initial therapy, as in the presented case.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
All procedures in this study were in accordance with national and international ethical standards. Informed consent was obtained from the patient.