
Abstract
Background
Though flow diverter is a safe and efficient modality, some patients can experience delayed aneurysmal rupture. The mechanism of delayed rupture is still obscure to us.
Methods
We performed a systematic search in the PubMed database for patients with delayed rupture of intracranial aneurysms after flow diverter placement.
Results
A total of 36 articles reporting on 60 patients were included in the final analysis. Of the 49 patients with description of presenting symptoms, six (12.2%) patients were incidentally diagnosed, 39 (87.8%) patients were admitted for aneurysmal rupture or mass effect. Multiple flow diverters were used in 38.3% (18/47) of the patients. Coil assistance was applied in 13.0% (7/54) of the patients. Delayed aneurysmal rupture led to intracranial hemorrhage or carotid–cavernous sinus fistula (CCF) in 76.8% (43/56) and 23.2% (13/56) of the patients, respectively. Of the 55 patients with description of outcome, 14 (25.5%) patients achieved good recovery, one (1.8%) patient was severely disabled, 40 (72.7%) patients died. All of the patients in the CCF group survived and experienced good recovery.
Conclusion
Increased intra-aneurysmal pressure, destabilization of the aneurysm wall by intra-aneurysmal thrombus, persistent residual intra-aneurysmal flow, characteristics of the specific aneurysm, and mechanical injury by the flow diverter might conjointly contribute to the final delayed rupture. There has been no established preventive measure to decrease the incidence of delayed rupture yet. The treatment and outcome depend on the presentation of delayed rupture. Patients presenting with aneurysm-related intracranial hemorrhage have a dismal outcome. Those presenting with CCFs usually have a satisfactory recovery.
Introduction
Intra-luminal flow diverter has been demonstrated to be a groundbreaking innovation in the treatment of intracranial aneurysms. It has shifted the treatment concept in endovascular management of intracranial aneurysms from direct coiling to blood flow diverting. 1 , 2 The indications and off-label use of flow diverter have been continuously expanding, which range from giant to small, proximal to peripheral, anterior circulation to posterior circulation, unruptured to ruptured and saccular to non-saccular (fusiform/dissecting, pseudo and blood blister) aneurysms.3–8 Though flow diverter is a considerably safe and efficient modality, in rare circumstances, some patients can experience delayed aneurysmal rupture. 9 , 10 However, the mechanism of delayed rupture is still obscure to us. To our knowledge, systematic review of delayed aneurysmal rupture after flow diverter placement is lacking. In this study, we perform a systematic literature review on this specific entity.
Methods
On 21 August 2019, we performed a systematic search in the PubMed database for patients with delayed rupture of intracranial aneurysms after flow diverter placement. The searching strategy was as follows: (flow diverter[Title/Abstract]) OR flow diversion[Title/Abstract]) OR flow diverting device[Title/Abstract]) OR pipeline[Title/Abstract]) OR pipeline flex[Title/Abstract]) OR surpass[Title/Abstract]) OR surpass streamline[Title/Abstract]) OR fred[Title/Abstract]) OR silk[Title/Abstract]) OR leo[Title/Abstract]) OR pipeline shield[Title/Abstract]) OR tubridge[Title/Abstract]) OR p64[Title/Abstract]) AND aneurysm[Title/Abstract]. The inclusion criteria for the identified articles were: 1) full text could be obtained or 2) sufficient data could be obtained from the abstract if the full text is inaccessible. Studies without sufficient description of the demographic, clinical and radiological data of the individual patient were excluded from the final analysis. In order to identify potentially missed articles, manual searching of the reference lists of the included articles was also performed. Modified Rankin Scale (mRS) was used for outcome assessment. A mRS score ≤ 3 was defined as good recovery. With respect to the criteria of delayed aneurysmal rupture, the following two points must be fulfilled: 1) rupture of the treated aneurysm after placement of the flow diverter, 2) demonstration of no contrast extravasation on the last angiogram before termination of the procedure.
Results
General information
The PubMed search identified 1334 records, of which 1257 were excluded based on title and abstract screening. Forty-three records were further excluded after reading the full text. We manually searched the reference lists of the remaining 34 articles and two additional articles were further identified. Finally, 36 articles reporting on 60 patients were included in the final analysis (Table 1). 8 ,11–45 The flowchart of searching strategy is illustrated in Figure 1. The patients were aged from 29 to 86 (55.31 ± 13.98) (n = 42) years, with a male to female ratio of 1:3 (11:33).
Clinical data of the patients with delayed aneurysmal rupture after flow diverter treatment.
BBA: blood blister aneurysm; CCF: carotid-cavernous fistula; CN: cranial nerve; CS: cavernous sinus; F: female; FD: flow diverter; ICA: internal carotid artery; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage; M: male; MCA: middle cerebral artery; mRS: modified Rankin Scale; NA/NM: not applicable/not mentioned; PAO: parent artery occlusion; PcomA: posterior communicating artery; SAH: subarachnoid hemorrhage; TVE: transvenous embolization; VA: vertebral artery
Flow chart of the searching strategy.
Before flow diverter placement
Of the 49 patients with description of presenting symptoms, six (12.2%) patients were incidentally diagnosed, five (10.2%) patients were admitted for aneurysmal rupture, two (4.1%) patients presented with non-subarachnoid hemorrhage-related headache and 36 (73.5%) patients presented with symptoms of mass effect by the responsible aneurysm. The treated aneurysms were unruptured in 91.7% (55/60) of the patients. The intracranial locations of the aneurysms were at middle cerebral artery, internal carotid artery (ICA) terminus, ICA-posterior communicating artery, ICA-supraclinoid segment, ICA-paraclinoid segment, ICA-superior hypophyseal segment, ICA-ophthalmic segment, ICA-cavernous sinus segment, basilar artery, vertebral artery in two (3.3%), two (3.3%), one (1.7%), 12 (20%), two (3.3%), one (1.7%), 13 (21.7%), 14 (23.3%), 10 (16.7%) and three (5%) patients, respectively (Figure 2(a)). The morphologies were blood blister aneurysm, pseudoaneurysm, fusiform/dissecting aneurysm, saccular aneurysm in two (3.3%), one (1.7%), 13 (21.7%) and 44 (73.3%) patients, respectively (Figure 2(b)). Three (6.8%, 3/44) aneurysms were demonstrated to be partially thrombosed before flow diverter placement. The sizes of the aneurysms were <5 mm, 5–10 mm, >10–≤25 mm, and >25 mm in two (3.3%), five (8.3%), 29 (48.3%) and 24 (40%) patients, respectively (Figure 2(c)).
Statistical diagrams of the ruptured aneurysms after flow diversion.
Peri-flow diverter placement
As for the type of flow diverters used, FRED, Silk, p64 and Pipeline were solely used in one (1.7%, 1/58), 17 (29.3%, 17/58), one (1.7%, 1/58) and 32 (55.2%, 32/58) patients, respectively. Different flow diverters were conjointly used in 12.1% (7/58) of the patients. Multiple flow diverters were used in 38.3% (18/47) of the patients. Coil assistance was applied in 13.0% (7/54) of the patients. Immediate intra-aneurysmal contrast stagnation was demonstrated in 92.6% (50/54) of the patients. Other procedure-related complications occurred in 21.6% (11/51) of the patients immediately after flow diverter placement.
Outcome of flow diverter placement
Before post-procedural rupture, formation of intra-aneurysmal thrombus was demonstrated in 97.3% (36/37) of the patients after flow diverter placement. With respect to the timeline of delayed rupture, 11.7% (7/60) of the patients experienced aneurysmal rupture in 1 day post flow diverter placement, 38.3% (23/60) of the patients between the second day and first week, 30% (18/60) of the patients between the second week and first month, 10% (6/60) of the patients between the second and third month, 8.3% (5/60) of the patients between the third and sixth month and 1.7% (1/60) of the patients beyond the sixth month, respectively (Figure 2(d)). Delayed aneurysmal rupture led to intracranial hemorrhage and carotid–cavernous sinus fistula (CCF) in 76.8% (43/56) and 23.2% (13/56) of the patients, respectively. In the patients with intracranial hemorrhage after delayed aneurysmal rupture, only four (9.5%, 4/42) survived following further treatment. However, all of the patients with CCF survived and experienced good recovery. The definite cause of delayed rupture was identified in two (3.3%, 2/60) patients as flow diverter migration. Of the 55 patients with description of outcome, 14 (25.5%) patients achieved good recovery, one (1.8%) patient was severely disabled, 40 (72.7%) patients died.
Antithrombotic regimen
Preoperative antiplatelet regimen could be identified in 54 patients, of whom two (3.7%) received single antiplatelet agent (including one receiving abciximab), 51 (94.4%) received dual antiplatelet agents and one (1.9%) received triple antiplatelet agents. No patient received preoperative anticoagulation agent. Postoperatively, antithrombotic regimen could be identified in 46 patients, of whom six experienced aneurysmal rupture during receiving single antiplatelet agents (13.0%, including one receiving additional anticoagulation agent), 39 during receiving dual antiplatelet agents (84.8%, including two receiving additional anticoagulation agent), one (2.2%) during receiving triple antiplatelet agents.
Discussion
Mechanism of delayed rupture
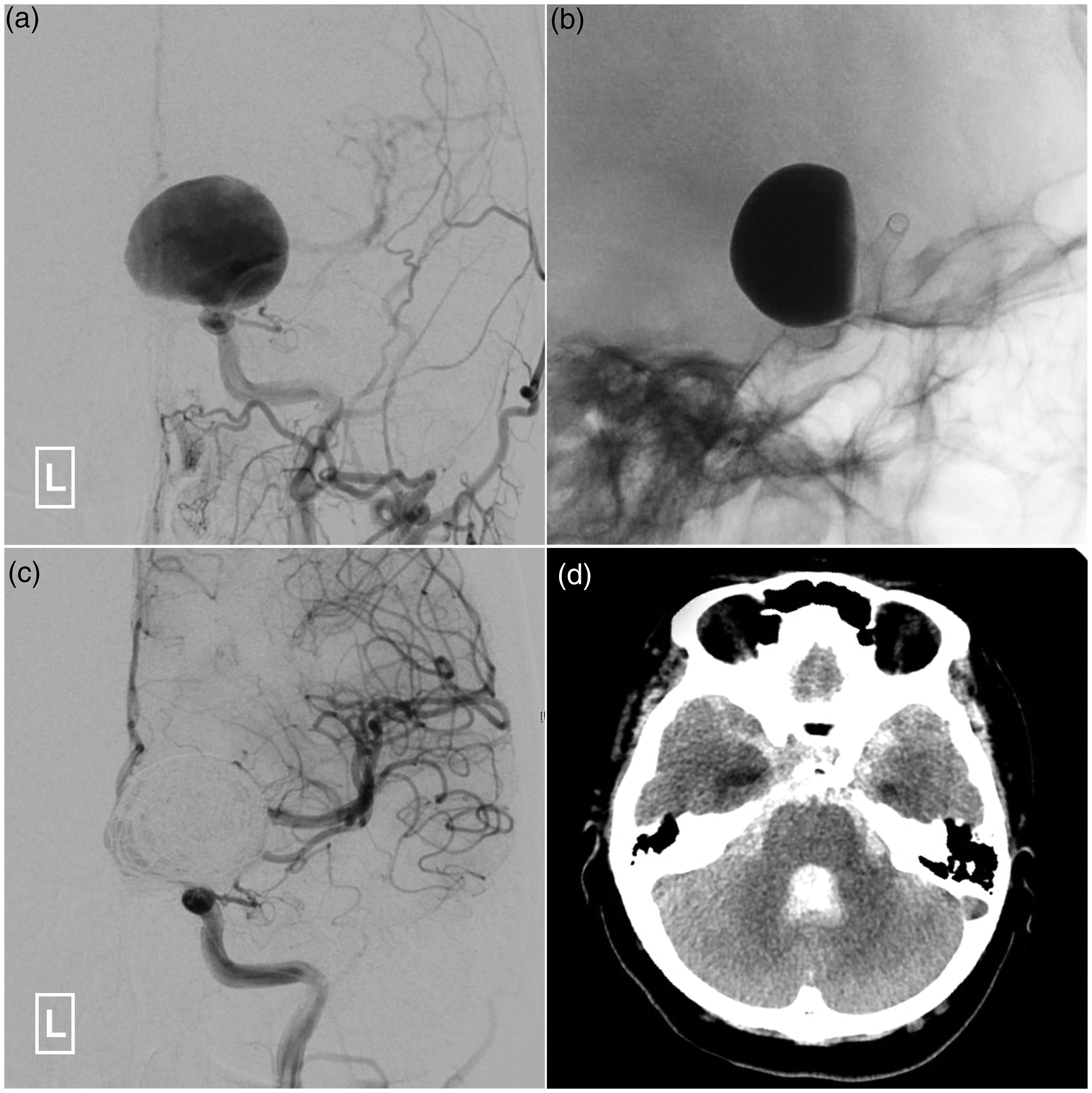
Flow diverter has become a more and more popular option, especially for the treatment of complex intracranial aneurysms. Some illustrative cases suited for flow diverter placement are presented in Figure 3. Delayed aneurysmal rupture is a severe complication after flow diverter placement, which could lead to a catastrophic consequence (Figure 4). The reported incidence varies greatly between different centers. In a single-center study of the 44 patients with cavernous carotid aneurysms treated with Pipeline, 11.4% (5/44) of the patients developed delayed CCF. 38 However, in another international multi-center retrospective study of intracranial aneurysms treated with Pipeline, the reported incidence of delayed rupture was 0.6% (5/793). 9 The mechanism is still unknown. According to the past studies, several factors might conjointly contribute to this severe consequence.
Illustrative cases suitable for flow diverter placement.
Illustrative case of delayed aneurysmal rupture after flow diverter placement.
First, flow diverter placement leads to increased intra-aneurysmal pressure. Compared with the successfully occluded aneurysms, delayed ruptured aneurysms endure more intra-saccular pressure after flow diverter placement by computational hemodynamic analysis. 16 This phenomenon can be explained in two possible ways. On one hand, successful deployment of the flow diverter stent could eliminate the pre-existing proximal stenosis of the parent artery. Though it is not the aim, reduction in proximal stenosis leads to reduced proximal resistance and subsequent increased pressure in the aneurysm segment. On the other hand, placement of flow diverter results in an increased resistance in the aneurysm segment of the parent artery, which would cause reduction in distal vascular resistance and increase in systemic blood pressure by complex autoregulation to maintain blood flow. The intra-aneurysmal pressure would increase with the increase in flow rate.
Second, though a key step in permanent aneurysm repair, intra-aneurysmal thrombus formation following flow diverter placement could also provoke a cascade of local inflammation and autolysis, leading to delayed aneurysm rupture. 15 , 17 , 32 This process is a known source of protease secretion that can weaken the aneurysmal wall. 35 Due to the destabilization of the aneurysm wall by intra-aneurysmal thrombus, any residual filling of the aneurysm sac after flow diverter deployment may have the potential for causing subsequent rupture. 32 , 46 This deduction is based on clinical observation and postmortem histopathological investigations of the ruptured cases and previous study of abdominal aortic aneurysms with intra-luminal thrombus. 17 In this study, before post-procedural rupture, partial formation of intra-aneurysmal thrombus was demonstrated in 97.3% (36/37) of the patients after flow diverter placement. However, it is still a mystery why intra-aneurysmal thrombosis may result in permanent cure in some patients but trigger autolysis and future rupture in other patients.
Other risk factors of delayed rupture include: 1) large and giant aneurysm; 2) symptomatic aneurysms; 3) saccular aneurysm with an aspect ratio of > 1.6; 4) delayed flow diverter migration into the aneurysm sac; 5) mechanical injury by flow diverter. 13 , 15 , 25 , 35 In this study, we found that 88.8% and 97.8% of the aneurysms experiencing delayed rupture were large/giant and symptomatic aneurysms, respectively. In addition, delayed flow diverter migration into the aneurysm sac was also identified in two patients, which accounts for a rare cause of delayed aneurysm rupture. 13 , 25 Linear tear of the aneurysm wall was identified in one patient during autopsy. 35 Histopathological examination showed that the aneurysmal wall was extremely thin and microfissures were also noted. No inflammatory cells were detected within the wall and thrombus. Hence, in view of the aforementioned reasons, mechanical stretch was considered the cause of delayed rupture in this patient. Besides, due to the disruption in all layers of aneurysm wall, blood blister aneurysm or pseudoaneurysm is at higher risk of delayed rupture. 33 , 36 Antithrombotic regimen might present another factor in delayed aneurysmal rupture. However, on one hand, the antithrombotic regimen varies greatly among different institutions with regard to the dosage, duration and agent selection. On the other hand, no study with large sample size focusing on antithrombotic regimen on delayed aneurysmal rupture has been published. Statistical analysis with regard to the antithrombotic regimen on delayed aneurysmal rupture could not be conducted at present. Of note, there were three patients who experienced delayed aneurysmal rupture during receiving single antiplatelet after ceasing the previous dual antiplatelet regimen. 15 Hence, the effect of antiplatelet regimen on aneurysmal rupture is a complicated issue to be investigated. Flow diverter coated with antithrombotic shield presented to be a new technology in the treatment of intracranial aneurysms. 47 , 48 As patients using flow diverter with shield technology adopt only single antiplatelet regimen, the risk of delayed aneurysmal rupture might be lower in theory. However, its effectiveness and safety need to be verified by further study.
Preventive measures
As was demonstrated by our study, delayed rupture meant a catastrophic event to most of the afflicted patients. Preventive measures to avoid this fatal complication are of great importance. Regrettably, to our knowledge, there has been no well-established suggestion to prevent delayed aneurysm rupture after flow diverter placement. All of the available measures are based on the speculated mechanism of delayed rupture. As hemodynamic study has demonstrated increased intra-aneurysmal pressure after flow diverter placement, some authors advocated careful post-procedural blood pressure control. 16 , 32 However, no comparative study on blood control in reducing delayed aneurysm rupture has ever been published until now. The effectiveness is to be verified. To achieve complete and stabilized aneurysm thrombosis and early isolation from the blood flow, coil assistance or multiple stent-in-stent flow diverters were also suggested. 15 , 16 , 32 , 49 But, according to our study, multiple flow diverters were used in 38.3% (18/47) of the patients who experienced delayed rupture. Coil assistance was applied in 13.0% (7/54) of the patients. Of note, multiple stent-in-stent flow diverters carry the risk of branch artery occlusion. To stabilize the already thrombosed aneurysm after flow diverter placement, some authors proposed reducing the post-procedural dose of antiplatelet agent. 32 However, the dose and duration of antiplatelet agent post flow diverter placement has always been a question of debate. With respect to the different brands of flow diverters on the occurrence of delayed aneurysm rupture, no comparative study has ever been reported. In this review, FRED, Silk, p64 and Pipeline were solely used in one (1.7%, 1/58), 17 (29.3%, 17/58), one (1.7%, 1/58) and 32 (55.2%, 32/58) patients, respectively. Different generation of flow diverters might also affect the incidence of post-procedural aneurysm rupture. According to the preliminary reports, the second-generation flow diverters seem safer with regard to the issue of delayed rupture. 44 ,50–52 But, as the second-generation flow diverters were just used in a relatively short period time and a limited population, prospective and comparative study with their first-generation counterparts is needed. Besides, as a majority of the delayed ruptured aneurysms were large/giant and symptomatic ones, the decision of flow diverter treatment should be prudent and under sufficient pre-procedural evaluation.
Treatment and outcome
In general, delayed aneurysm rupture after flow diverter placement can present with acute intracranial bleeding (subarachnoid hemorrhage and/or intracerebral hemorrhage) or CCF. Acute intracranial bleeding always means a fatal event. In our review, only four (9.5%, 4/42) patients survived following further treatment. Because of the rapidity of deterioration in general state, most of the patients in this subgroup have no opportunity for further treatment. Even with aggressive management, most of the cases would also experience inevitable deterioration and death. 11 , 22 , 25 , 30 , 36 Of note, there was one patient who survived and experienced complete thrombosis of the aneurysm with just conservative management. 45
Patients presented with CCF after flow diverter placement would experience a relatively more favorable outcome. According to this review, all of the patients with CCF survived and experienced good recovery. The treatment for this subgroup of patients was diverse and included transvenous embolization with coils, placement of an additional flow diverter, and ICA occlusion. 8 , 12 , 15 Due to the higher metal coverage of flow diverter, it is difficult to advance the microcatheter through the flow diverter to the carvernous sinus. And embolization of the cavernous sinus via transarterial approach is always impossible. 38 , 39 Hence, transvenous approach is the preferred route. But attention should be paid to the possibility of cranial nerve palsy by mass effect of coils. If transvenous approach is inaccessible, ICA sacrifice could be considered under prudent evaluation with balloon occlusion test. There was one report that the CCF was successfully treated with an additional flow diverter, 8 but this case presented with a low-flow CCF. The CCF was gradually occluded in a delayed manner. Hence, the efficacy and safety of placing additional flow diverters warrants further investigation.
Conclusion
Delayed rupture of intracranial aneurysm after flow diverter treatment is a rare but usually fatal complication, the mechanism of which is still obscure to us. Increased intra-aneurysmal pressure, destabilization of the aneurysm wall by intra-aneurysmal thrombus, persistent residual intra-aneurysmal flow, characteristics of the specific aneurysm and mechanical injury by the flow diverter might conjointly contribute to the final delayed rupture. There has been no established preventive measure to decrease the incidence of delayed rupture yet. The proposed existing measures need to be verified by future study. The treatment and outcome depend on the presentation of delayed rupture. Patients presenting with aneurysm-related intracranial hemorrhage have a dismal outcome. Those presenting with CCFs usually have a satisfactory recovery. Flow diverter represents groundbreaking progress in the treatment of intracranial aneurysms, but is not an infallible method. Patients receiving flow diverter treatment should be evaluated individually.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.