
Abstract
Hereditary spastic paraplegias are an uncommon group of monogenic diseases that include 79 types of genetic disorders. The most frequent cause of recessive hereditary spastic paraplegia is a mutation in the spastic paraplegia gene type 11 followed by type 15. This group is usually associated with non-specific clinical features like cognitive decline and may precede the progressive weakness and spasticity of lower limbs. The magnetic resonance imaging hallmark of hereditary spastic paraplegia is thinning of the spinal cord. However, brain magnetic resonance imaging may provide relevant clues for specific hereditary spastic paraplegia subtypes, and thinning of the corpus callosum has been described as the most frequent abnormality in almost one-third of recessive hereditary spastic paraplegias. Moreover, a characteristic abnormality affecting the forceps minor of the corpus callosum has been recently reported as the “ears of the lynx” sign and is highly suggestive of type 11 and 15 hereditary spastic paraplegias. We report a patient who was diagnosed with hereditary spastic paraplegia type 11 by exome genetic testing, presenting the ears of the lynx sign in the first magnetic resonance imaging assessment.
Introduction
Hereditary spastic paraplegias (HSPs) are an uncommon group of monogenic diseases that include over 79 types of genetic disorders. They may segregate as an autosomal dominant, autosomal recessive, X-linked, or mitochondrial trait. 1 Based on the clinical phenotype, Harding criteria have classified HSP as pure (pHSP) and complicated (cHSP). 2 In pHSP, symptoms are restricted to the pyramidal motor system while in cHSP other neurological domains can be involved; such as cognitive, cerebellar, extrapyramidal, or peripheral systems. The most frequent cHSP is type 11, and is caused by mutations in the gene associated with spatacsin vesicle trafficking, clinically manifesting around the first or second decades with cognitive deterioration followed by gait disturbances. If patients also develop peripheral neuropathy, pigmented maculopathy, and movement disorders like dopa-responsive parkinsonism, 3 the clinical suspicion could be HSP type 15. This broad clinical spectrum and the absence of positive background history make the recessive forms of HSP a difficult group to diagnose. Therefore, recently described specific magnetic resonance imaging (MRI) signs may assist diagnostic suspicion. The MRI hallmark in HSP is the thinning of the spinal cord, but it lacks specificity. Other brain MRI abnormalities more frequently associated with cHSP 3 , 4 are widespread white matter damage and volume reduction in cortical and deep gray matter. Thinning of corpus callosum (TCC) has been used to characterize a certain group of HSP patients (HSP-TCC) and has been reported in at least 15 different HSP subtypes. However, focal thinning in the genu fibers of the corpus callosum described as the “ears of the lynx” sign has been related to only two recessive forms of HSP, type 11 and type 15.3–6
We describe a case of a patient to emphasize the importance of specific signs on brain MRI related to recessive types of HSP.
Case report
A 14-year-old patient with no background family history for HSP developed muscle pain and cramps, dysarthria, and tendency to falls. Previously, the patient had attention deficit disorder at primary school. Three years later the patient started with bilateral brachial weakness. Despite this, cognitive impairment, dysarthria, and paraplegia were the predominant symptoms. Physical examination revealed spastic paraplegia, bilateral clonus, and hyperreflexia. Also, the patient had spastic gait requiring unilateral support. Serological studies like arilsulfatase A/sulfatides, beta galactocerebrosidase, hexosaminidase, biliary acids, and plasmatic amino acids were normal. Four years after the first evaluation, HSP type 11 was diagnosed by genetic exome test. Interestingly prior to genetic diagnosis, MRI showed a thin corpus callosum, particularly in the genu and anterior portion of the body as shown sagittal T1
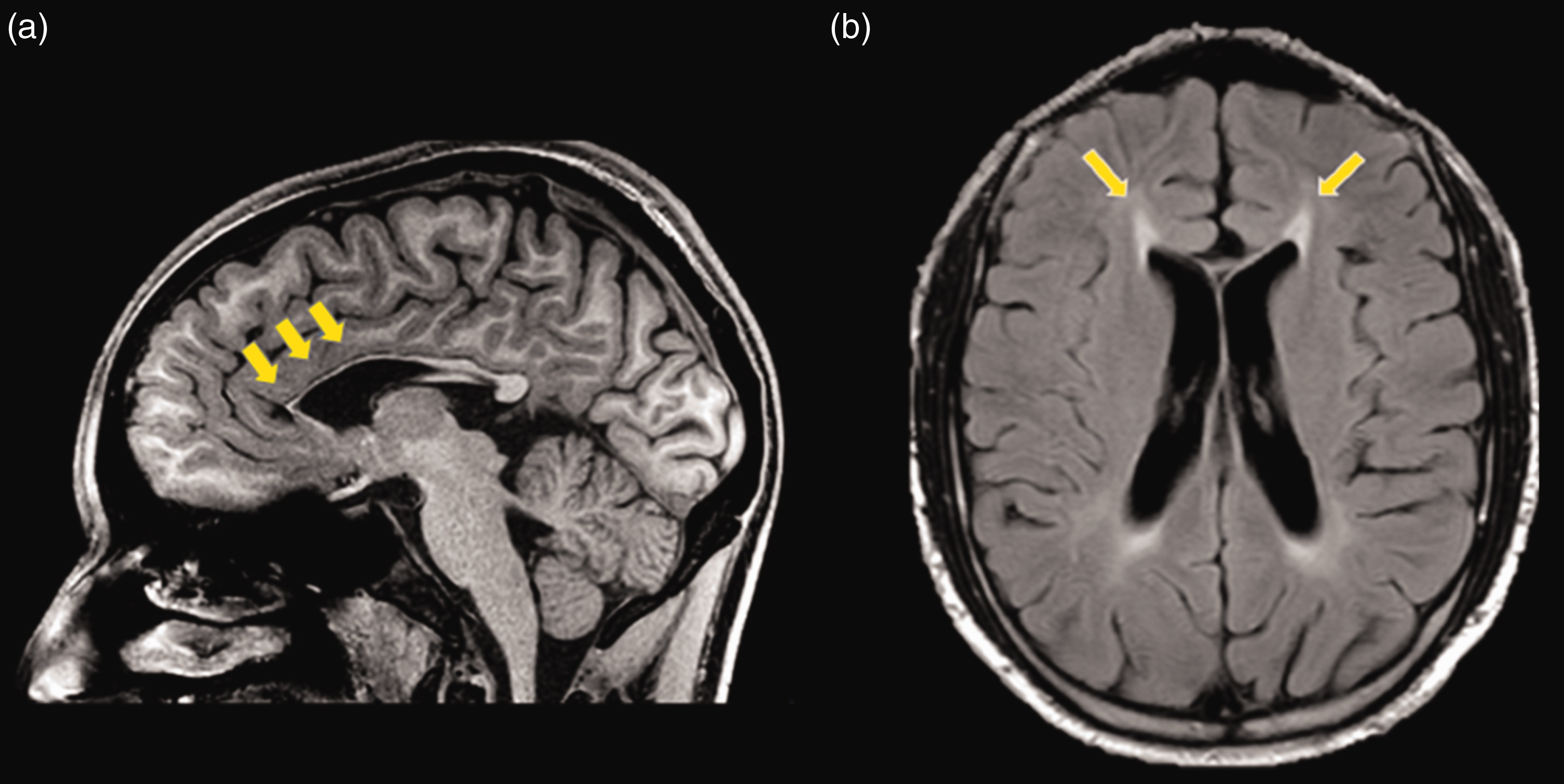
(a) Sagittal T1 shows atrophy of the anterior portion of the corpus callosum; (b) brightness on axial Fluid-attenuated inversion recovery (FLAIR) represent the damage in genu fibers of forceps minor.
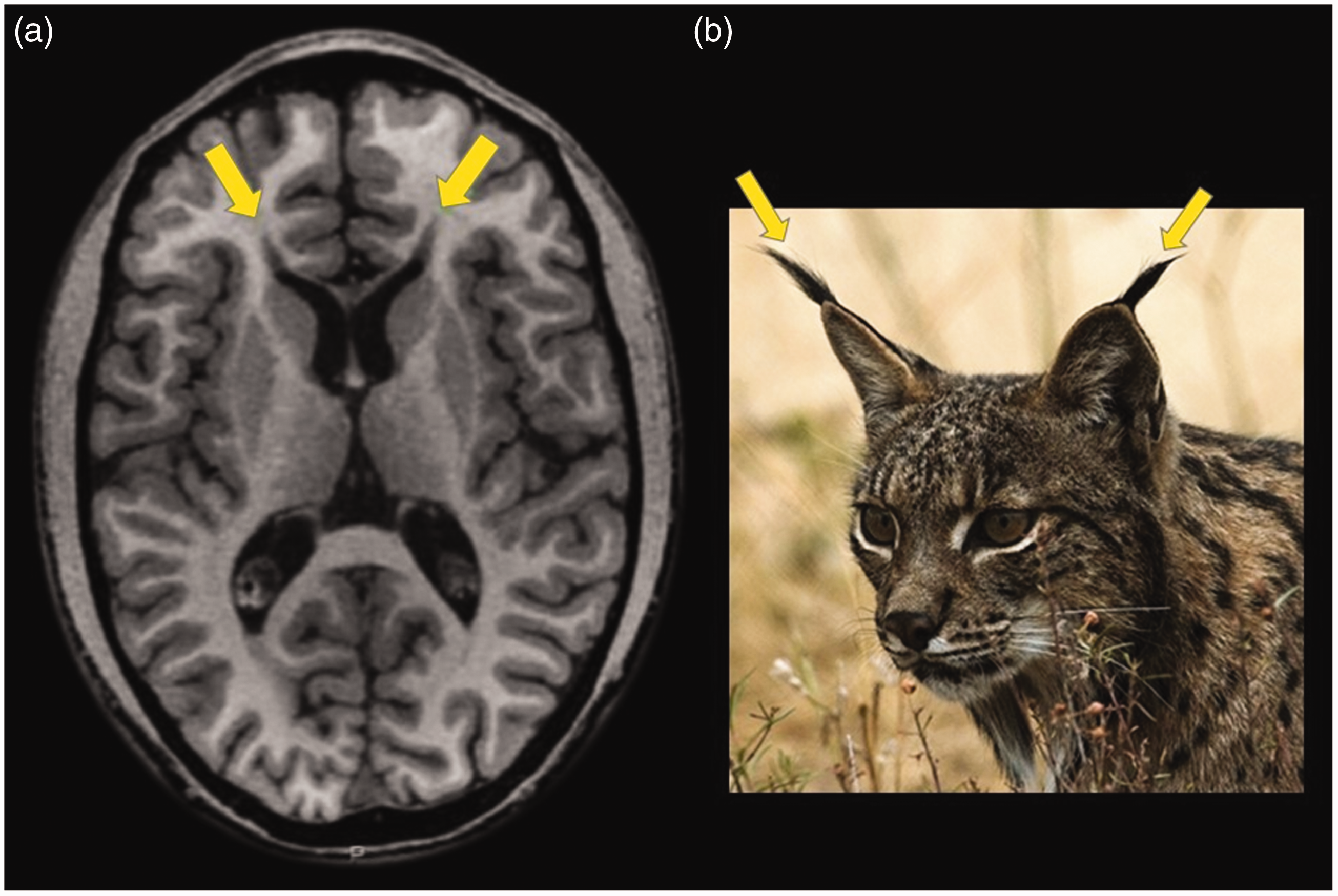
(a) In the T1 axial plane, the atrophy in forceps minor appears dark and is known as the ears of the lynx sign because it resembles the tip of the ears of the lynx (b). This sign is highly suggestive of type 11 and 15 hereditary spastic paraplegia.
Presently the patient has cognitive decline including memory, attention-executive, language and visuospatial functions, uses Botox for spasticity and occasionally has urinary incontinence.
The MRI imaging study was performed using a 1.5-Tesla scanner with sequence that includes T1: turbo field echo 3D, acquisition matrix: 300 × 300, plane of acquisition: sagittal, slice thickness: 1 mm, repetition time: 7.5 ms, echo time: 3.6 ms, flip angle: 8°, and FLAIR: turbo inversion recovery 3D, acquisition matrix: 224 × 224, plane of acquisition: sagittal, slice thickness: 1.12 mm, repetition time: 4800 ms, echo time: 296.16 ms, flip angle: 90°.
Discussion
Autosomal recessive HSP
Less specific findings on MRI are widespread white matter hyperintensities and cortical and deep grey matter volume reduction. To understand the broad spectrum of MRI features, Agosta et al. found a direct correlation between disease severity and white matter involvement. Furthermore, damage in the interhemispheric, limbic, corticocortical, and cerebellar white matter tracts was associated with cognitive impairment. 2
Selective damage to the corpus callosum is interesting. Currently, the evolutionary moment in which it is affected is unknown. Even in our case, the patient already had atrophy of the corpus callosum on MRI assessment 1 year after the clinical onset, but definitive diagnosis was made after 4 years of queries and multiple complementary studies. Therefore, in order to reduce the diagnosis time, the radiologist must be aware of and detect the ears of the lynx sign. This information could help neurologists, since it would limit genetic tests by reducing the spectrum of the disease 6 and redirecting symptomatic treatment.
Conclusion
In the diverse clinical context and without specific MRI findings, the ears of the lynx sign is an important feature, suggesting a narrower spectrum in the broad causality of HSP. Radiologists should take care and note the relevance of this sign, reducing the possibilities to two specific causes such as HSP type 11 or 15.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.