
Abstract
Background
Cavernous carotid artery aneurysms can be treated by several endovascular techniques including flow diversion (FD) and parent vessel occlusion (PVO). We reviewed our institution’s consecutive series of endovascularly treated cavernous carotid artery aneurysms to compare these two modalities and their associated clinical and radiographic outcomes.
Methods
All patients harboring a cavernous carotid artery aneurysm treated by FD or PVO from January 2008 to December 2018 were enrolled. Data were collected retrospectively and analyzed on patient presentation, aneurysm dimensions, treatments and related complications, rate of aneurysm occlusion, sac regression, and outcomes.
Results
Fourteen patients were treated with FD and 12 underwent PVO subsequent to passing a balloon test occlusion. There was no significant difference between treatment modalities in aneurysmal occlusion (97.0 ± 8.4% (FD) vs. 100% (PVO), p = 0.23), degree of sac regression (62.5 ± 16.7% (FD) vs. 56.8 ± 24.3% (PVO), p = 0.49), or near-complete to complete symptom improvement (66.7% (FD) vs. 81.8% (PVO), p = 0.62). Major complications included subarachnoid hemorrhage from aneurysmal rupture in 1 (7.1%) patient post-FD and 2 (16.7%) ischemic strokes following PVO.
Conclusions
Endovascular treatment of cavernous carotid artery aneurysms by FD or PVO are both effective and safe. There is insufficient evidence to recommend one technique over the other and decision making should be individualized to the patient, their aneurysm morphology, and operator experience.
Introduction
Cavernous carotid artery aneurysms (CCAAs) account for approximately 4% of cranial aneurysms occurring more commonly in females.1,2 While the risk of subarachnoid hemorrhage from these aneurysms is low, intervention is often considered when these become large or giant, grow, or cause symptoms due to mass effect, mostly cranial neuropathy. Rarely carotid cavernous fistula formation or rupture into the paranasal sinuses with epistaxis may also warrant treatment. 3 , 4 Traditionally, aneurysms of this location have proven technically challenging for microsurgery owing to the anatomical relationships and morphology, which often include partially thrombosed components and frequently incorporation of the parent internal carotid artery (ICA) in a fusiform or fusisaccular morphology. The advent of endovascular therapies has presented alternative strategies in the form of parent vessel occlusion (PVO), coiling with or without stent-assistance, and more recently, flow diversion (FD). PVO is associated with a high rate of aneurysmal occlusion but with risks of ischemic complications and theoretical risks of altered hemodynamics that may promote growth of mirror internal carotid artery aneurysms or de novo aneurysm formation. 5 , 6 FD is a reconstructive technique that has increasingly shown to be effective and safe, particularly for large, wide-necked aneurysms which are less readily addressed by traditional endovascular means. FD permits preservation of the parent artery.7–10
Symptom resolution post-operatively is thought to be due to elimination of fundus pulsations and reduced mass effect on neighboring structures. This has primarily been evaluated based on occlusion rate; however, regression of the aneurysmal sac may also serve as a useful measure of reduced mass effect. Our study aims to compare the efficacy, based on degree of aneurysmal occlusion, sac regression, and symptom resolution, in addition to safety of CCAA treatment by FD to PVO.
Methods
Patient cohort and imaging characteristics
Consecutive patients from January 2008 to December 2018 undergoing endovascular treatment of a CCAA at our tertiary care hospital were reviewed retrospectively. Patients were included if they harbored any aneurysm arising from the cavernous segment of the internal carotid artery, underwent pre-operative computed tomography angiography (CTA) or magnetic resonance angiography (MRA), and returned for at least one clinical and radiological follow-up. Information was collected from medical records on patient age, sex, comorbidities (hypertension, smoking status), presenting symptoms, balloon test occlusion (BTO) results, and treatment modality. Aneurysm size was assessed according to maximal sac dimension (anterior–posterior (AP) or transverse (TR)), sac cross-sectional area at its maximal dimension

and greatest luminal dimension. Sac dimensions were measured from T2-weighted sequences on MRI or non-enhanced CT. Luminal dimensions were measured from contrast-enhanced MRA or CTA. These sequences were standardized by orienting the axial images parallel to the subcallosal plane. Aneurysm location, rupture status, and presence of a contralateral mirror aneurysm in addition to adjacent parenchymal edema was also recorded.
Choice of treatment modality was based on the clinical discretion of the treating interventional neuroradiologist. FD was achieved by implantation of the Pipeline embolization device (Medtronic, Minneapolis, USA) with no additional coils placed within the aneurysm sac. Prior to FD stent placement, patients were administered 325 mg aspirin and 75 mg clopidogrel orally for 5 days and remained on this regimen for 6 months. The clopidogrel was then discontinued followed by a reduction in aspirin to 81 mg, which was continued indefinitely. More recently, ticagrelor has replaced the use of clopidogrel (due to a more reliable response) loaded the day prior to treatment at a dose of 180 mg and continued for a similar duration to clopidogrel at 90 mg twice daily. When used with ticagrelor, the dose of aspirin was reduced to 81 mg. PVO was accomplished with detachable balloons or coils after successfully passing a BTO. This was performed awake with the balloon catheter inflated within the ipsilateral petrous internal carotid artery for 30 minutes under systemic heparinization. A pass was defined as absence of new neurological deficits, symmetric vessel opacification (up to one frame venous delay accepted) on injections of the contralateral internal carotid artery and or vertebral artery, as well as no significant asymmetry (10% or less) on single-photon emission computed tomography (SPECT) when compared with the contralateral hemisphere or a baseline exam if available (single pass agent radiotracer injected at 20 minutes of balloon inflation). Asymptomatic aneurysms demonstrating interval radiographic growth were considered for treatment. Data collection and analysis occurred following approval by the local institutional research ethics board.
Outcome
The primary outcome of interest was the resolution of symptoms, principally cranial neuropathy, graded as complete, near complete, partial, or none. Time from treatment to complete or near complete resolution as assessed at clinical follow-up was recorded. Efficacy of aneurysm treatment and subsequent relief of mass effect was gauged by degree of occlusion and sac regression on the latest follow-up CT or MR angiogram. Aneurysm occlusion was defined as the percentage reduction in luminal filling and sac regression as the percentage reduction in cross-sectional area of the aneurysm fundus (including the thrombosed component) at its widest dimension. Periprocedural complications and need for retreatment were assessed.
Statistical analysis
Patients were divided into two groups based on treatment with FD or parent vessel occlusion. The data for each group were described using means ± standard deviation for continuous variables and frequencies with their associated percentages for categorical variables. Bivariate analysis was employed to identify differences in patient or aneurysm characteristics as well as outcomes between patients who underwent FD compared with PVO. This analysis was performed using the Student’s t-test, chi-squared test, or Fisher exact test depending on the data type and distribution. All tests were 2-sided and significance was pre-established at a p-value less than 0.05.
Results
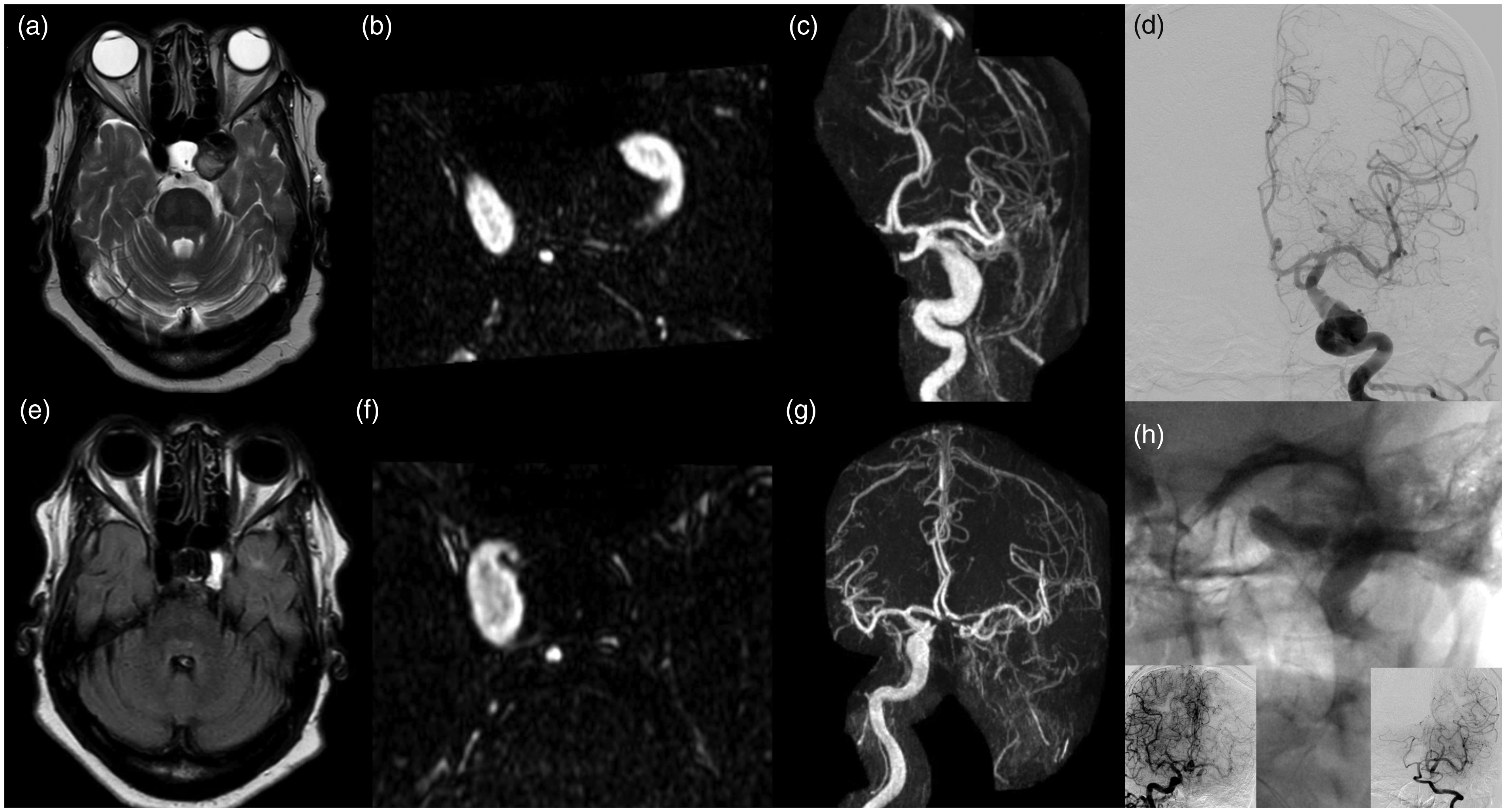
Over a 10-year period, a total of 30 patients with a CCAA were treated with endovascular therapy. Four patients were excluded due to treatment by partial coiling of the aneurysm fundus only (1), loss to clinical follow-up (2), and death within days after intervention in a patient who initially presented with rupture and subarachnoid hemorrhage. The mean patient age was 60.2 ±13.1 years with a majority female (80.8%) and hypertensive (53.9%). The most common presenting sequalae of aneurysmal mass effect was ophthalmoplegia (65%), although six (23%) were asymptomatic. FD was the treatment of choice for 14 patients, of which 1 failed their BTO. Twelve patients underwent PVO after clinically and radiographically tolerating a BTO. Those treated with PVO were significantly older (66.8 ± 7.6 years vs. 54.6 ± 14.4, p = 0.01) than those treated by FD. A higher frequency of FD-treated patients had incidental aneurysms; however, this difference was not statistically significant. There was no between-group difference in aneurysm size as measured by luminal and sac dimensions (see Table 1).
Baseline characteristics between flow diversion and parent vessel occlusion: values presented as mean ± standard deviation or frequency (%). p-values calculated by two-sided t-tests, chi-squared test, or Fisher exact test.
aLargest AP or transverse dimension measured in the subcallosal plane.
bSac cross-sectional area calculated using area of ellipse =
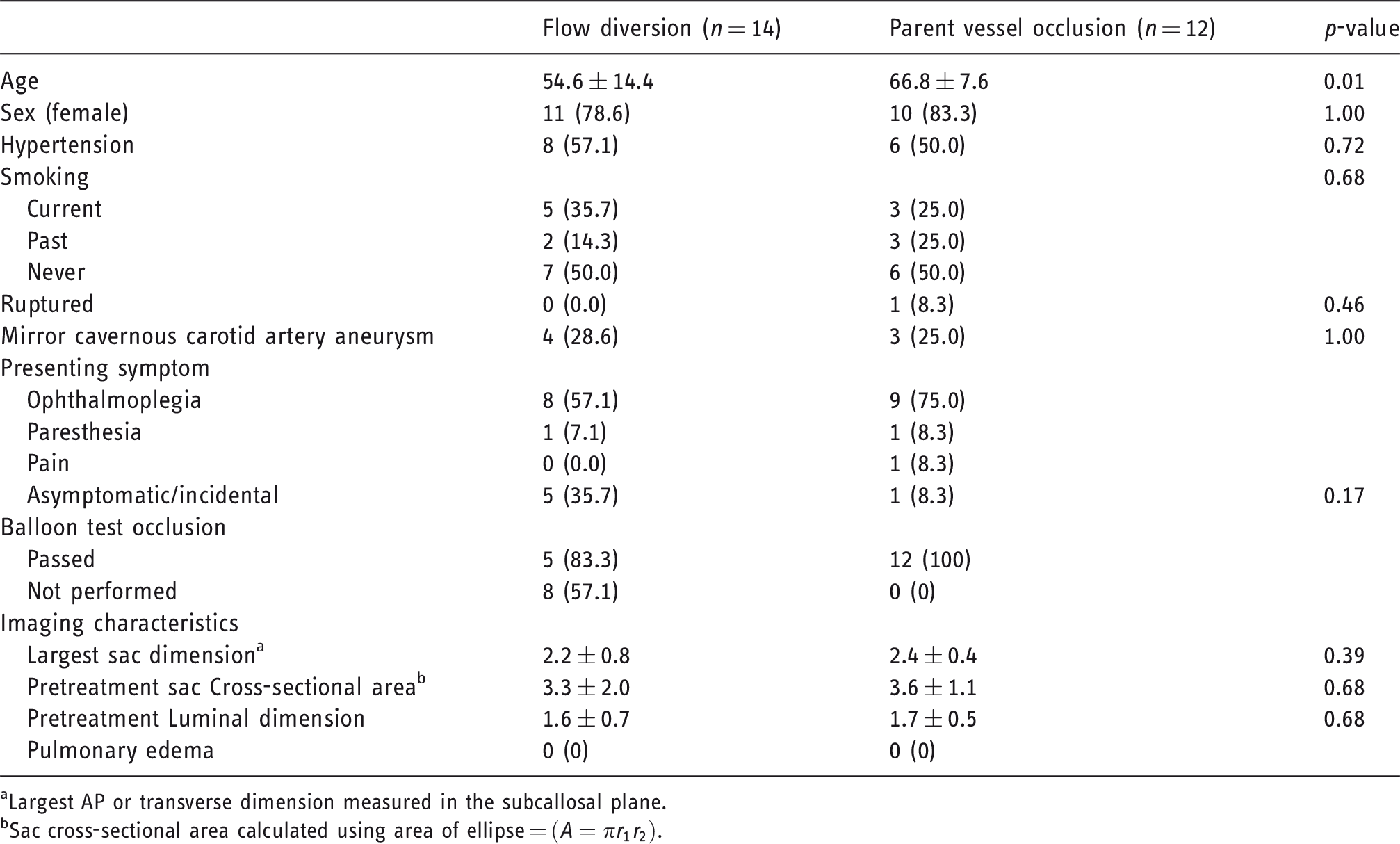
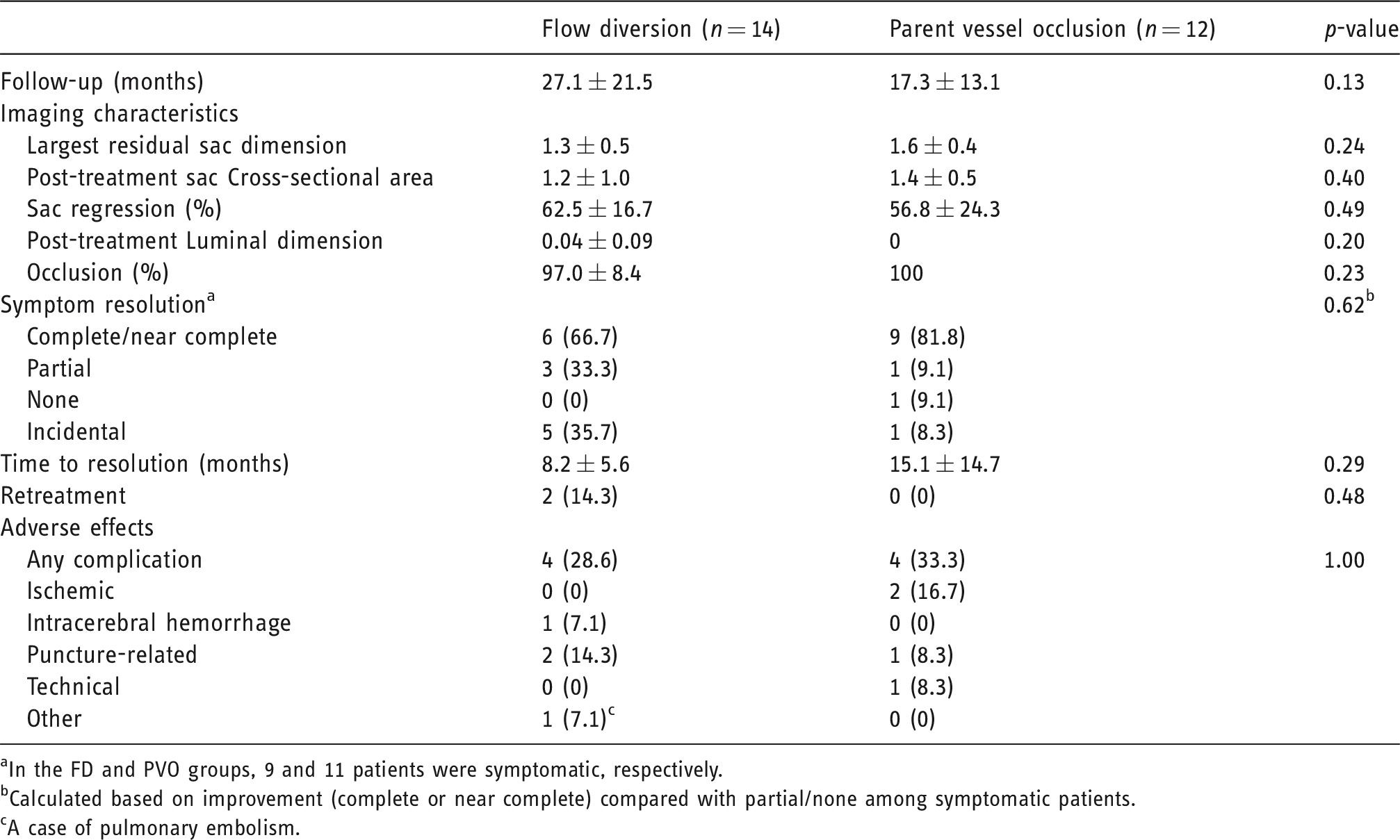
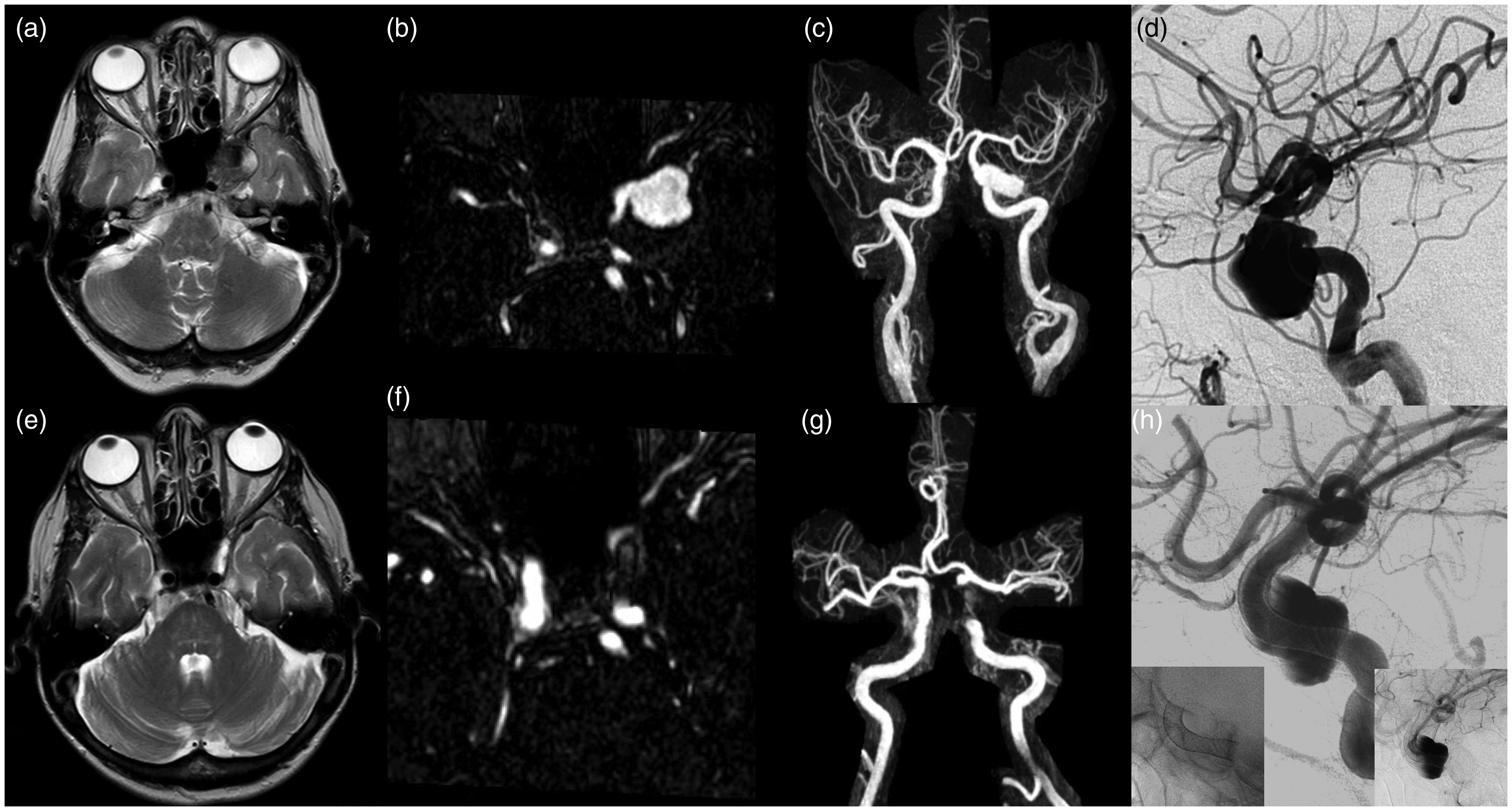
FD in nine symptomatic patients resulted in complete resolution of symptoms in 44.4%, near complete in 22.2%, and partial resolution in the remainder of patients (33.3%) (see Table 2). The 11 symptomatic patients treated with PVO experienced complete symptom improvement in 54.5%, near complete improvement in 27.3%, partial improvement in 9.1%, and no improvement in 9.1%. The mean rate for symptoms to resolve to complete or near complete was shorter following FD (8.2 ± 5.6 months vs. 15.1 ± 14.7 months, p = 0.29); however, this did not reach statistical significance. After a mean follow-up of 27.1 ± 21.5 months, all but 2 (14.3%) aneurysms treated by FD demonstrated 100% occlusion. All aneurysms treated by PVO were completely occluded following a mean of 17.3 ± 13.1 months. The degree of aneurysmal sac regression was similar between the two treatment groups (62.5 ± 16.7% − FD vs. 56.8 ± 24.3% − PVO) as well as among those who had near complete to complete resolution of symptoms (59.0 ± 22.4%) and those who had partial or no resolution of symptoms (63.5 ± 12.1%). Representative cases of treatment by PVO and FD are illustrated in Figure 1 and Figure 2, respectively. Retreatment was required for two patients (7.7%), both of whom were treated with FD. One was due to persistent filling after 6 months and the other following short-term, interval recanalization.
Outcomes following flow diversion and parent vessel occlusion: values presented as mean ± standard deviation or frequency (%). p-values calculated by two-sided t-tests, chi-squared test, or Fisher exact test.
aIn the FD and PVO groups, 9 and 11 patients were symptomatic, respectively.
bCalculated based on improvement (complete or near complete) compared with partial/none among symptomatic patients.
cA case of pulmonary embolism.
A patient in their 80s presenting with retro-orbital pain and cranial nerve III palsy. (a to c) Large, partially thrombosed left cavernous carotid artery aneurysm on MRI axial T2-weighted image (a) and gadolinium-enhanced magnetic resonance angiography (MRA) in axial (b) and coronal MIP (c). (d) AP DSA pretreatment. (e to g) Corresponding MR images 12 months post-internal carotid artery occlusion with detachable balloons. (h) Intraprocedural AP view showing two detachable balloons occluding the petrous internal carotid artery (inset images show perfusion of the left middle cerebral artery territory via the anterior and posterior communicating arteries from prior balloon test occlusion). The patient had near complete resolution of their symptoms at latest follow-up. MIP: maximum intensity projection; DSA: digital subtraction angiography.
A patient in their 70s presenting with cranial nerve III palsy. (a to c) Large left cavernous carotid artery aneurysm on MRI axial T2-weighted image (a) and gadolinium-enhanced magnetic resonance angiography (MRA) in axial (b) and coronal MIP (c). (d) Lateral DSA pretreatment. (e to g) Corresponding MR images 30 months post-flow diversion demonstrating interval sac regression (signal dropout from the Pipeline Embolization Devices (PED) obscures the patent internal carotid artery lumen). (h) Intraprocedural lateral DSA confirms the PEDs across the aneurysm neck (inset images show unsubtracted view of the devices’ positions and delayed view showing stasis). The patient’s ophthalmoplegia resolved completely.
The overall rate of major complication in this cohort of endovascularly treated CCAA was 11.5%. This included two patients who underwent PVO with post-operative symptomatic infarction and one patient (known history of polyarteritis nodosa) having an intraoperative rupture with subsequent subarachnoid hemorrhage following FD. The latter involved a large, multilobulated aneurysm requiring telescoping devices. Significant puncture-related hematomas were the most common of minor complications present in two patients after flow diversion and one following PVO, one of which precipitated hypotension and ensuing cerebral ischemia. One patient was treated with both detachable balloons and coils, later found to have coil migration without hemodynamic sequelae on follow-up imaging. There was also a single incident of post-operative pulmonary embolism after FD.
Discussion
The optimal endovascular treatment for CCAA remains to be determined. PVO following clinical and radiological pass of a BTO has been shown to achieve complete thrombosis in a large percentage of patients. 11 , 12 A meta-analysis of 247 patients with CCAA treated with balloon occlusion revealed a 99% rate of complete aneurysmal thrombosis and improvement in diplopia in 81.5%. 5 Similarly, Van Rooij’s series of 50 patients showed total thrombosis in all aneurysms managed with internal carotid artery occlusion resulting in partial to full cranial nerve palsy resolution in 92% (42% complete). 1 The PVO cohort in this study demonstrated a comparable high rate of complete occlusion totaling 100% with resolution of presenting symptoms in 81.8%. FD offers an arterial reconstructive alternative that not only effectively promotes aneurysmal thrombosis, particularly in wide-necked aneurysms, but also exhibits a low complication rate.8–10, 13 , 14 Tanweer et al.’s series of 43 CCAAs treated with FD showed complete or near complete occlusion in 88.4%, visual deficit improvement in 84.2%, and only a 3.5% major complication rate. 9 Another series of 44 CCAAs, a majority of which were giant aneurysms, demonstrated 71% complete occlusion on final follow-up angiography after a mean of 10.9 months and 90% significant symptom improvement. 8 This current series shows similar rates of angiographic complete occlusion with FD at 85.7% although slightly reduced symptomatic resolution at 66.7%.
Few studies have examined the relationship between aneurysmal sac regression and relief of mass effect-related cranial neuropathy. In PVO, aneurysmal occlusion occurs rapidly; however, symptom resolution often takes days to weeks presumably as the aneurysm thromboses and regresses. Szikora et al. found in their cohort of CCAAs treated by FD that regression of the aneurysmal sac coincided with cessation of angiographic filling, the former being necessary for initiation of improvement in cranial neuropathy. 14 This change in the aneurysm sac occurred between 3 to 8 months post-treatment. To the authors’ best knowledge, our study is the first to quantify the degree of aneurysmal sac regression. We demonstrated that the amount of post-operative sac regression was similar between CCAAs treated by FD and PVO suggesting equivalent efficacy. This is further supported by no difference seen between treatment groups in symptom resolution. While a majority of patients experienced near complete to complete symptom improvement following treatment, no significant relationship to aneurysmal sac regression was found between this group and those who had partial or no improvement.
The primary risks of endovascular therapy for CCAAs are ipsilateral ischemia for both FD and PVO in addition to aneurysmal rupture or intracerebral hemorrhage either related to the aneurysm or iatrogenic in relation to maneuvers pertaining to the endovascular procedure. With respect to the latter, PVO has the advantage that devices can remain extradural. In our study, there was one patient (7.1%) who suffered a periprocedural subarachnoid hemorrhage in the FD group, which is slightly higher than other reported hemorrhagic rates in the literature for aneurysms of this segment of the internal carotid artery. In the treatment of 97 unruptured intracranial aneurysms with Pipeline embolization device in a Canadian cohort, the rate of hemorrhage was 7.5% as a result of periprocedural aneurysmal rupture and ipsilateral distal territory hemorrhage. 13 When focusing on aneurysms isolated to the cavernous segment though, there were no reported hemorrhages, either subarachnoid or intraparenchymal. Puffer et al. identified only 1 (2%) small volume hemorrhage from which the patient was asymptomatic. 8 A systematic review which identified 227 CCAAs treated with FD concluded that the overall morbidity and mortality rate was 3.5%. 9 The discrepancy is likely related to our small sample size; however, another possibility is an underlying vascular fragility in the context of our patient having polyarteritis nodosa. Periprocedural ischemia following PVO appears to be more common with an incidence of 13.3% in a recent comparison study of various endovascular modalities for CCAAs. 10 Starke et al. reported a risk as high as 20% of any central nervous system complication post-PVO of which 66.6% (or 13.3% overall) were permanent. 11 A lower rate of periprocedural ischemia, 4%, was observed in van Rooij’s series, one of which was secondary to an extensive retroperitoneal hematoma with subsequent hypoperfusion. 1 The rate of ischemic stroke following treatment with PVO in our cohort, 16.7%, falls within the higher range observed in other studies despite the fact that all patients passed a BTO (clinically and angiographically).
The major limitation of this study is its retrospective, observational design predisposing it to selection bias. This is evidenced by the significantly older cohort that underwent PVO as compared with FD. Age may influence the outcomes associated with a particular treatment as younger patients harbor less vessel tortuosity and atheromatous changes increasing the chances of successful deployment of a flow-diverting stent. It also highlights the importance of patient selection, as we were able to achieve high occlusion rates and reasonable clinical improvement for both modalities. In addition, no standardized angiographic or clinical outcome grading scales were used introducing the possibility of measurement bias. A prospective, controlled trial with randomization to each treatment modality is needed. However, given the wide adoption of FD owing to its success in treating other intracranial aneurysms, a more practical approach may be establishing a prospectively collected national or international database of all endovascularly treated CCAAs to improve the power in analysis.
Conclusion
FD and PVO represent effective and safe treatments for CCAAs. These modalities are each associated with high aneurysmal occlusion rates, similar degree of sac regression, and comparable rates of symptomatic resolution. FD achieves aneurysm occlusion without compromising the parent vessel, while PVO has the advantage of being less technically demanding with high durability. The choice of treatment should be individualized and based upon patient characteristics, aneurysm anatomy, and operator expertise.