
Abstract
Introduction
The Flow Redirection Intraluminal Device (FRED) flow diverter has a unique bilayer design, with the outer scaffolding stent extending beyond the inner flow diverting component by about 3 mm at each end. Here, we describe a technique to utilize these unrestrained flared ends for precise flow diverter placement in cases where the aneurysm and an adjacent branch are in close proximity and branch jailing is not desired, such as in posterior communicating artery aneurysms.
Conclusions
The non-flow diverting unrestrained flared ends of the FRED stabilize the distal end of the device when deployed directly into the branches at the arterial bifurcation. The technique is useful to provide adequate neck coverage of cerebral aneurysm located directly adjacent to the bifurcation as is frequently the case with posterior communicating artery aneurysms.
Introduction
Flow diversion is an established endovascular treatment modality for cerebral aneurysms. 1 The Flow Redirection Intraluminal Device (FRED) is a flow diverter approved by the Food and Drug Administration in 2020 for wide-necked saccular or fusiform internal carotid artery cerebral aneurysms from the petrous segment to the carotid terminus. The design differs from other flow diverters in that it is made up of two layers: an outer layer with 16 wires that serves as a scaffold and an inner low porosity flow diverting layer with 48 wires providing 33–44% metal coverage. 2 The outer layer has unrestrained flared ends that exceed the inner layer on each side by approximately 3 mm. Those ends have minimal to no flow-diverting properties. 3 These flared ends can serve as an anchor for precise device placement in cases where the aneurysm neck and an important branch not desirable for jailing are in close proximity. This technical nuance has not been reported in the literature thus far. Here, we describe our early experience using this technique in the treatment of supraclinoid internal carotid artery aneurysms, particularly those related to the posterior communicating artery.
Technical note
On each end of the FRED, the outer stent ends in four triangular-shaped wires, with a radiopaque marker at each triangle extending beyond the flow diverting mesh. The distal end of the FRED device is pushed out of the microcatheter at the carotid terminus to allow the distal ends to flare. Once fully open, the ends are situated in the terminus, ideally with at least one of the limbs in the A1 segment of the anterior cerebral artery. The device is subsequently unsheathed under gentle forward pressure. This technique stabilizes the device at the distal landing zone and prevents unintended foreshortening at the distal end. This is particularly important for aneurysms located adjacent to the carotid terminus to assure adequate neck coverage (Figure 1).
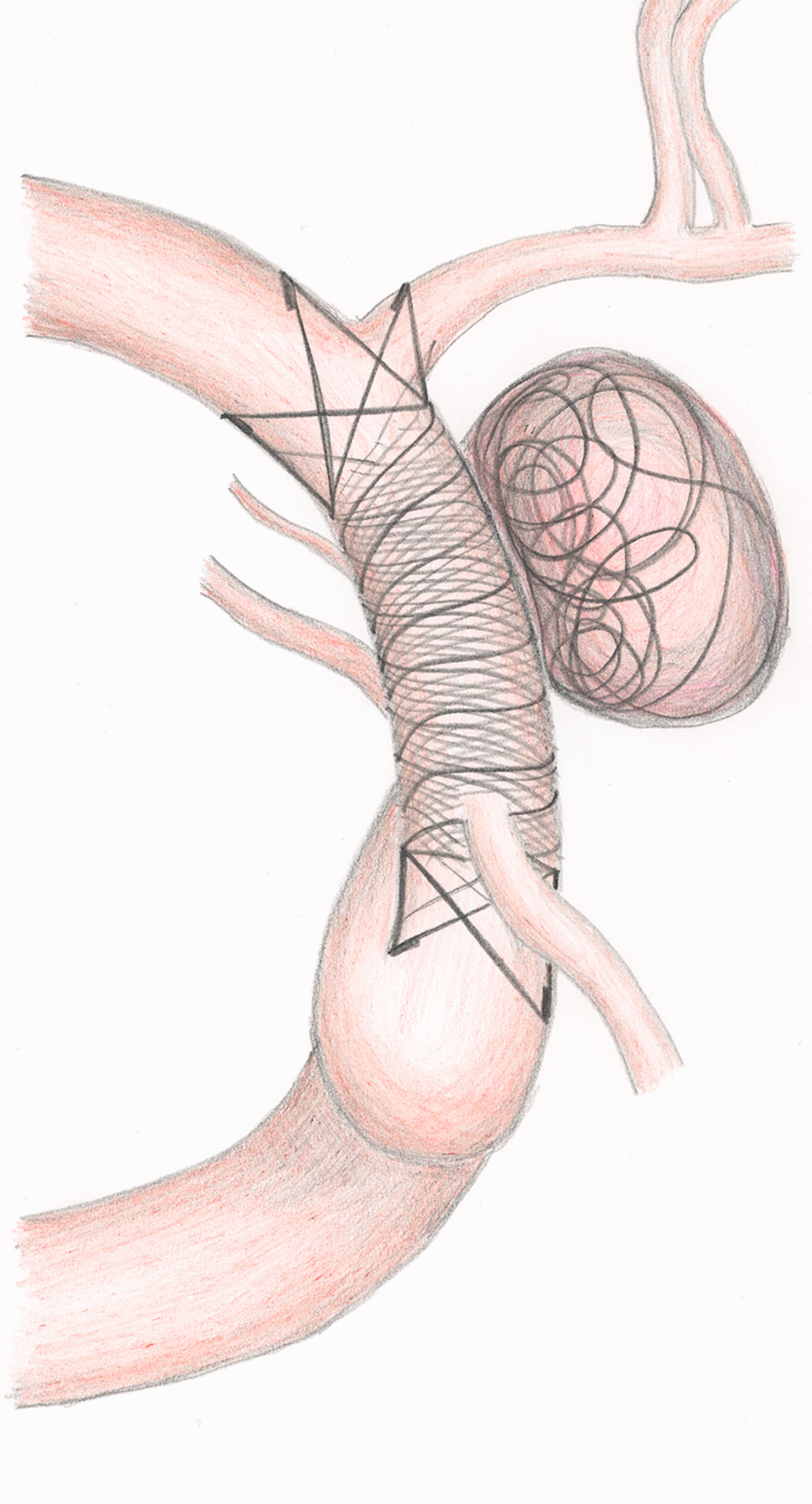
Concept of landing the non-flow diverting stent portions of the Flow Redirection Intraluminal Device (FRED) within the internal carotid artery (ICA) terminus without jailing A1 or M1 vessel segments.
Case presentation
A 85-year-old female patient was treated with coil embolization for a ruptured superior hypophysial artery aneurysm and was lost to follow-up. She presented again one year later to our emergency room with headaches and dizziness, and imaging showed an early large aneurysm recurrence without aneurysm re-rupture. The decision was made for flow diversion due to the wide neck and early recurrence after coiling. Due to the short distal landing zone and the long diseased segment with mismatching vessel diameter and additional paraclinoid fusiform aneurysmal component, a FRED was chosen as flow diversion treatment (Figure 2). After loading with ticagrelor 90 mg b.i.d. and aspirin 325 mg and with P2Y12 Reaction Units in the therapeutic range, a long sheath and intermediate catheter was placed in the right internal carotid artery through a femoral access. Weight-based therapeutic heparin was given, and the FRED delivery catheter was placed in the right middle cerebral artery using a microwire. Next, the 4 mm × 28 mm/34 mm FRED was carefully deployed, starting with the stent (non-flow diverting) portion in the internal carotid artery terminus covering then the aneurysm neck, as well as the proximal paraclinoid fusiform aneurysm portion (Figures 1 and 2). Post-deployment two- and three-dimensional angiography confirmed favorable FRED wall apposition and coverage of the aneurysm neck, with significant stasis within the aneurysm without jailing the A1 or M1 segment. The patient woke without neurological deficits and was discharged the next day.
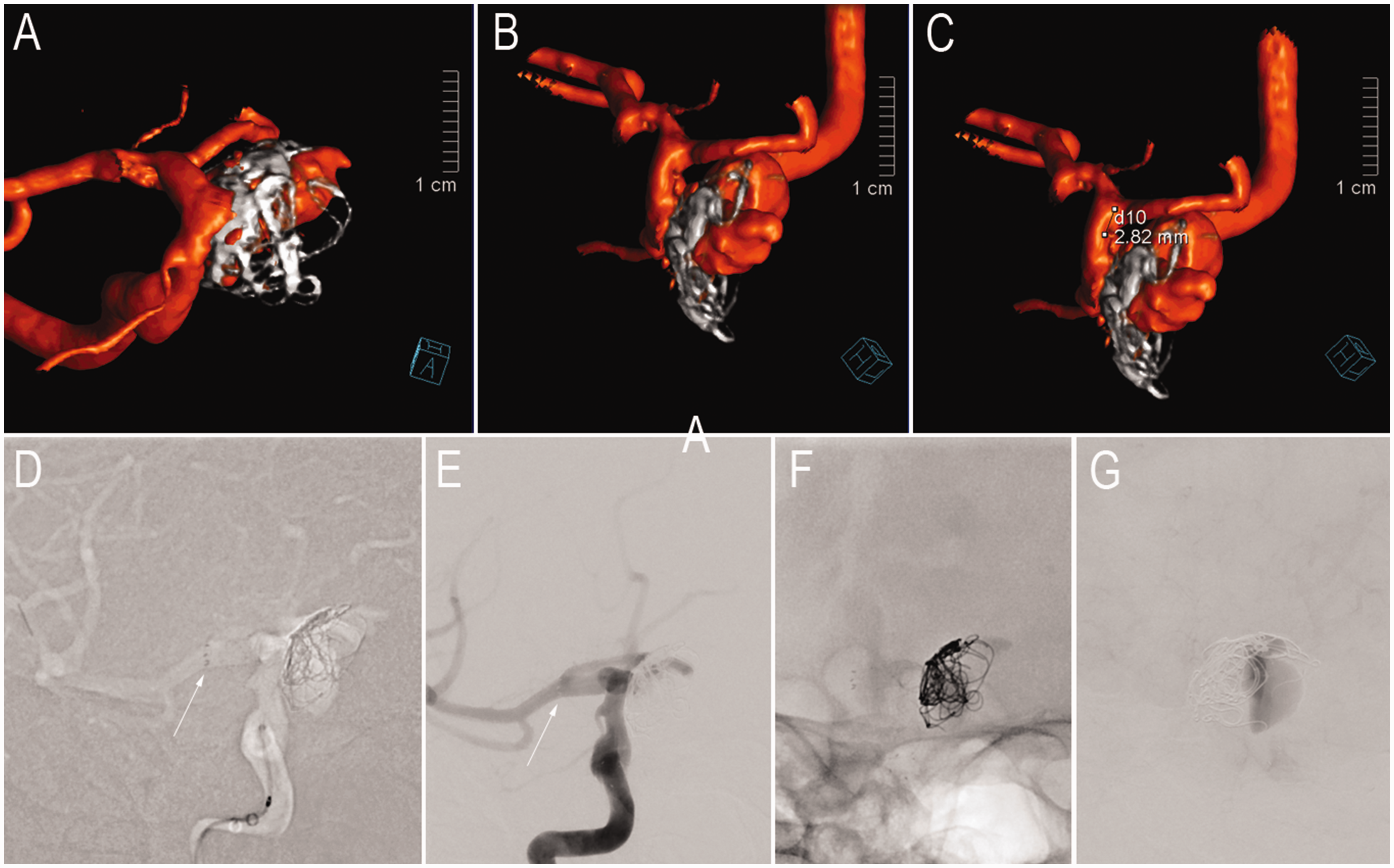
An 85-year-old female patient with early recurrent right superior hypophysial artery aneurysm after coiling. A three-dimensional rotational angiogram shows the early recurrent superior hypophysial artery aneurysm with the coil mass ((a) and (b)) and the short distance between the ICA terminus and distal aneurysm neck of approximately 3 mm (c). Anteroposterior projection showing during FRED deployment (d) and patent FRED after deployment (e), as well as a native image with the final construct (f) and significant stasis in the late angiography phase (g). Note the distal placement of the FRED within the ICA terminus without jailing the A1 or M1 segment and without compromising flow (white arrows in (d) and (e)).
Discussion
The FRED differs from other flow diverters in its unique bilayer design that incorporates a portion of the device at each end that is non-flow diverting. These ends consist of four triangular-shaped wires that are unrestrained and open beyond the nominal diameter of the flow diverter. When properly placed, they anchor the device distally in the arterial bifurcation where the luminal area is wider than the vessel proximal to the bifurcation. To our knowledge, application of this unique device feature for precise flow diverter placement and anchoring has not been previously reported.
The aneurysm location most suitable for treatment using this technique is the posterior communicating artery. In the International Subarachnoid Aneurysm Trial, aneurysms of the posterior communicating region made up 25% of all enrolled aneurysms, second only to anterior communicating artery aneurysms. 4 It was the same trial that paved the way for increased utilization of endovascular treatment modalities. Coiling of ruptured aneurysms, however, has been associated with particularly high rates of aneurysm recurrence. 5 Flow diversion has become a popular option for retreatment of recurring aneurysms, after both failed coiling and microsurgical clipping. 6 In posterior communicating artery aneurysms, flow diversion has shown acceptable occlusion rates. 7 , 8 While the presence of a fetal posterior communicating artery or origin of the posterior communicating artery from the aneurysm has not proven to affect occlusion rates, 7 those situations remain a concern in clinical practice. Similarly, coverage of the anterior cerebral artery origin with a flow diverter is not desired. Although usually asymptomatic, delayed occlusion rates of the anterior cerebral artery are highest among flow diverter-covered branches, which can be attributed to competitive flow from the rich collateral network from the contralateral anterior cerebral artery. 9 The long-term consequences of occlusions of such important cerebral blood vessels remain unknown. For those reasons, precise landing of the distal end of the flow diverter proximal to the anterior cerebral artery take off but distal to the posterior communicating artery aneurysm neck is required. This, however, is not feasible in most instances with flow diverters that do not possess non-flow diverting ends. Combined with the acute turn in the terminal carotid artery superiorly at the posterior communicating artery take off, there is often no option other than to deploy and stabilize the flow diverter in the proximal middle cerebral artery and to jail the anterior cerebral artery. 10 The FRED, however, has the unique design feature that allows for the distal non-flow diverting end to be positioned in the carotid terminus without jailing the anterior cerebral artery. Once the flared ends are positioned correctly, the distal end of the device is anchored with a lower risk of distal foreshortening. The device also has the advantage that the delivery system does not have to be recaptured—a process that can also lead to unintended foreshortening at the distal end. Whether this distal anchoring technique in the bifurcation proves beneficial, even in locations other than the carotid terminus, remains to be determined.
Conclusions
The FRED non-flow diverting unrestrained flared ends stabilize the distal end of the device when deployed directly into the branches at the arterial bifurcation. The technique is useful to provide adequate neck coverage of cerebral aneurysm located directly adjacent to the bifurcation, such as in posterior communicating artery aneurysms.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CJG receives research support from Medtronic and consulting honoraria from Stryker and Microvention. None are related to the current work.