
Abstract
Superficial siderosis refers to hemosiderin deposition along the pial surface of the brain and spinal cord. It results from chronic and repetitive low-grade bleeding into the subarachnoid space. Dural tears are a common cause of superficial siderosis. Although such tears typically occur in the spine, dural tears can also occur in the posterior fossa. In many cases, posterior fossa dural tears are iatrogenic, and patients may present with neuroimaging evidence of postoperative pseudomeningoceles. We present a case of superficial siderosis caused by a persistent posterior fossa dural leak. The patient presented with superficial siderosis 30 years after a Chiari I malformation repair. A pinhole-sized dural tear was identified preoperatively using computed tomography cisternography. The dural defect was successfully repaired. An additional small tear that was not seen on imaging was also identified at surgery and successfully repaired.
Introduction
Superficial siderosis (SS) is a disorder characterized by hemosiderin deposition along the pial surface of the neuroaxis. It results from chronic and repetitive low-grade bleeding into the subarachnoid space. 1 SS may be idiopathic or seen secondary to conditions such as brain tumors or trauma. The most common potentially treatable etiology for SS is a dural tear. 2 One recent report described three patients developing SS after posterior fossa surgery complicated by pseudomeningoceles. 3 All patients were found to have incomplete dural closure at surgery. In two previous cases, computed tomography (CT) cisternography was used to demonstrate extra-arachnoid contrast accumulation suggesting a dural leak, although the exact location of the leak was not identified on imaging.3,4 Prior cases have also demonstrated SS in patients with diskogenic spinal cerebrospinal fluid (CSF) leaks. 5 Here, we present a case of SS in a patient with remote repair of a Chiari I malformation. Preoperative CT cisternography successfully identified a discrete site of CSF egress into a pseudomeningocele. This finding was confirmed intraoperatively.
Patient presentation and work-up
A 48-year-old man presented with 2 years of progressive orthostatic headaches and gait ataxia. He had undergone repair of a Chiari I malformation 30 years prior to presentation. Initial brain magnetic resonance imaging (MRI) and subsequent head CT revealed a posterior fossa pseudomeningocele with peripheral calcification (Figure 1). MRI of the brain and spine demonstrated extensive SS overlying the brain and extending over the spinal cord (Figure 2). Lumbar puncture showed an elevated red blood cell count (1000 per μl), elevated protein (162 mg/dl), and xanthochromia, suggestive of ongoing subarachnoid hemorrhage. CT cisternography showed contrast opacification of the patient’s pseudomeningocele and identified a clear site of dural leak (Figure 3). Based on this finding, the patient underwent surgical exploration, confirming two discrete sites of CSF egress, the larger of which corresponded to the CT cisternographic finding, and the smaller of which was occult on imaging; both leak sites were successfully repaired (Figure 4). Postoperative CT cisternography confirmed that the leak into the pseudomeningocele had resolved (Figure 5). No persistent dural defect was present. The patient had an uneventful postoperative course.
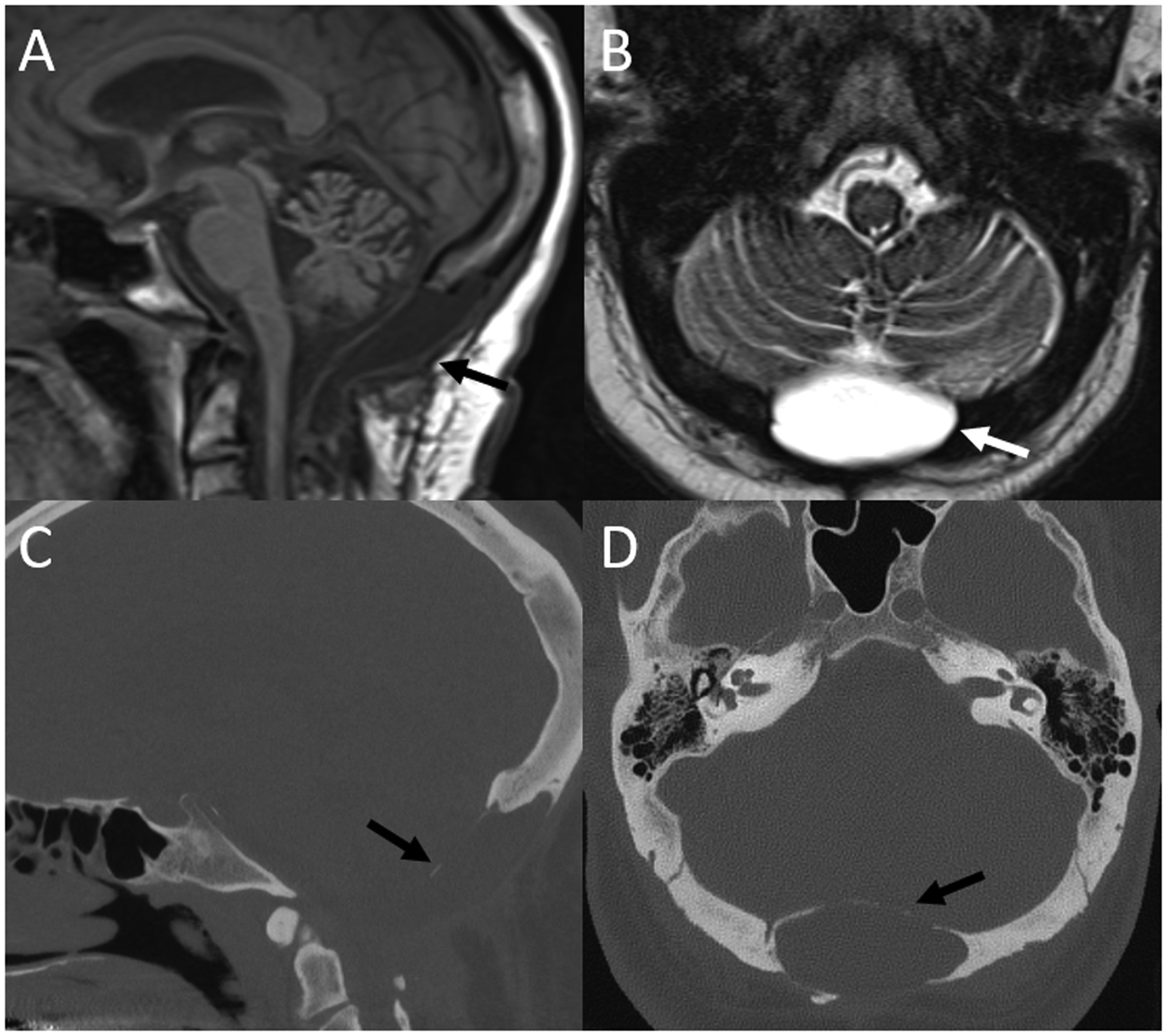
Sagittal T1-weighted (a) and axial T2-weighted (b) images from the patient’s brain magnetic resonance imaging (MRI) demonstrate a T1 hypointense, T2 hyperintense fluid collection in the posterior fossa (a and b, arrows), consistent with a pseudomeningocele in the setting of the patient’s history of Chiari I decompression. On the patient’s subsequent computed tomography scan, this pseudomeningocele was noted to have a thin rim of calcification (c and d, arrows).
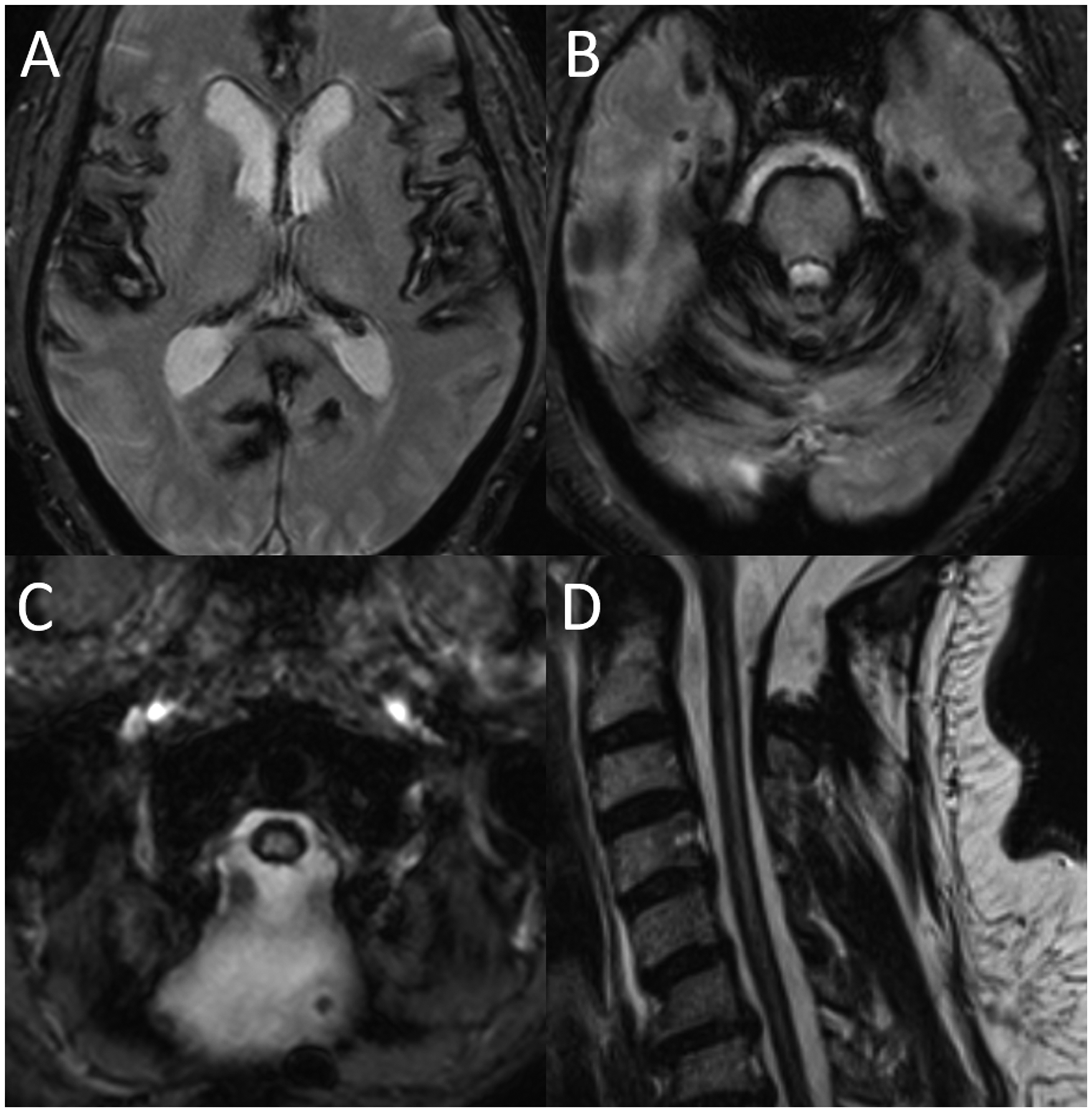
Axial susceptibility weighted images from the patient’s brain magnetic resonance imaging (MRI) (a–c) and sagittal T2-weighted image from the patient’s cervical spine MRI (d) demonstrate extensive hypointense signal along the pial surface of the brain and spinal cord, compatible with superficial siderosis.
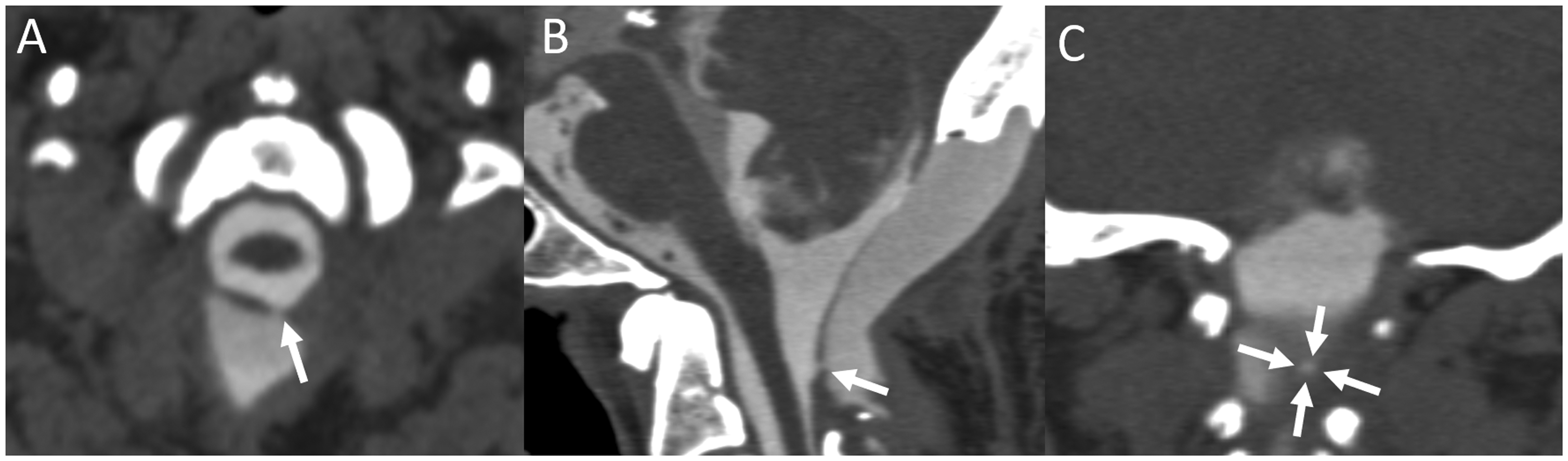
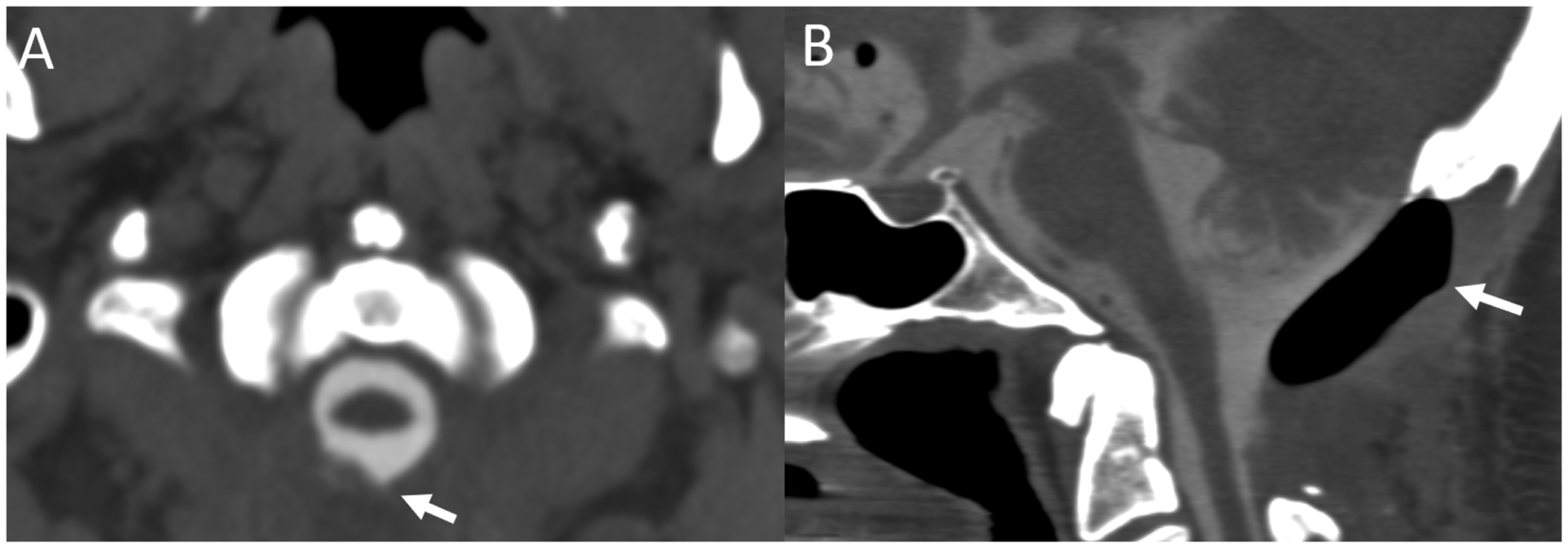
Axial (a), sagittal (b), and coronal (c) images from the patient’s preoperative computed tomography (CT) cisternogram demonstrate a discrete pinhole-sized dural defect (a–c, arrows). There is also complete contrast opacification of the patient’s posterior fossa pseudomeningocele.
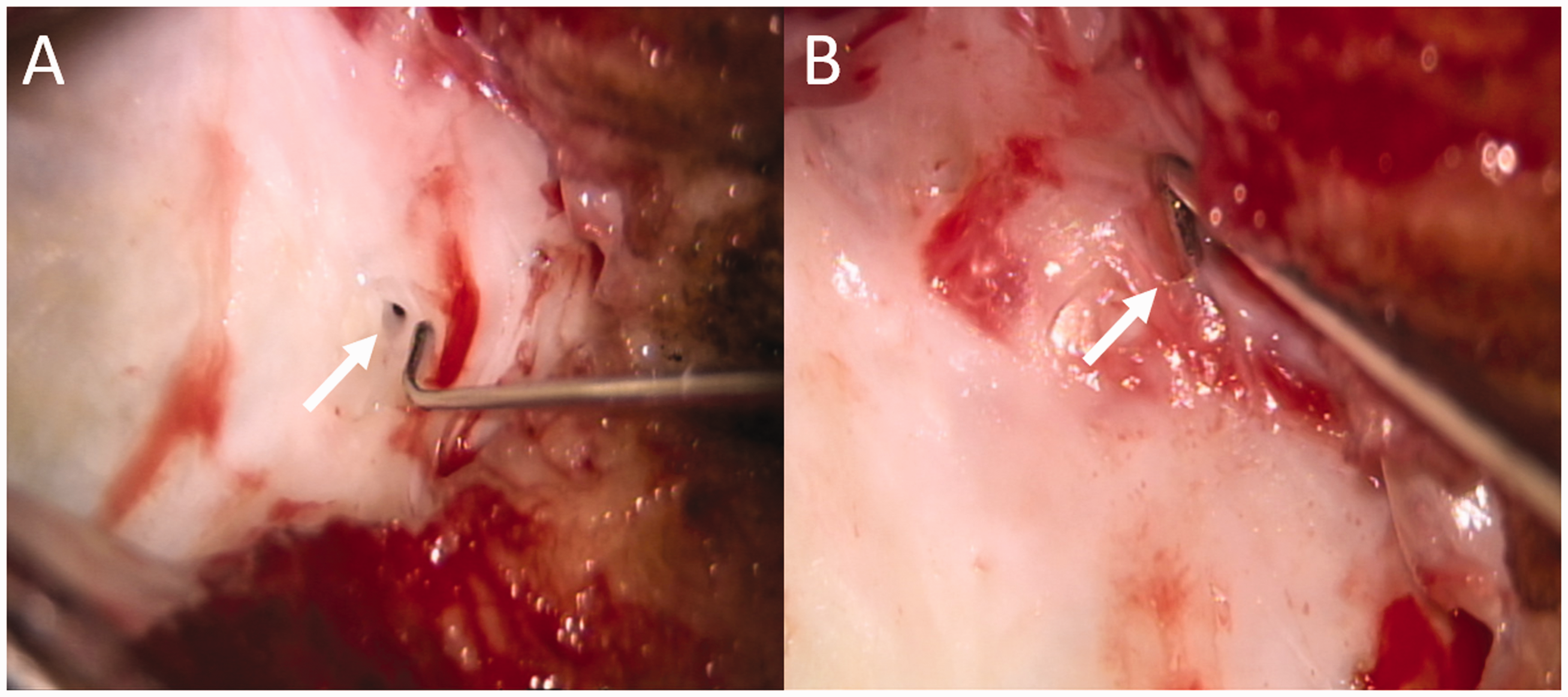
Intraoperative photographs obtained during repair of the patient’s dural leak show a prominent left-sided hole in the dura at the level of the cervicomedullary junction (a, arrow), which was felt to correspond to the abnormality seen on computed tomography (CT) cisternography. In addition, an adjacent more subtle hole on the right side of the dura (b, arrow) was identified intraoperatively. Although less conspicuous, clear cerebrospinal fluid (CSF) egress was noted from this hole during Valsalva. This second leak was occult on CT cisternography.
Axial (a) and sagittal (b) images from the patient’s postoperative computed tomography (CT) cisternogram show that the left-sided dural defect has resolved (a, arrow), with expected postoperative air within the sealed off pseudomeningocele (b, arrow) and no extra-arachnoid contrast leak.
Discussion
We have described a case of SS associated with posterior fossa surgery complicated by a dural leak. Although this association has been demonstrated before, this is the first reported case illustrating a discrete, pinhole-sized dural defect on CT cisternography with resolution on postoperative CT cisternogram. Thus, in the case, CT cisternography was beneficial for both diagnosis and preoperative planning.
SS most commonly presents with sensorineural hearing loss and ataxia. SS can also be asymptomatic and can be seen incidentally in patients being imaged for unrelated reasons. MRI in patients with SS shows a T2 hypointense signal along the pial surface of the brain, brainstem, and spinal cord, with characteristic blooming on susceptibility weighted imaging. 6 These findings most commonly involve posterior fossa structures such as the brainstem and cerebellum. Hemosiderin deposition can also occur along other pial surfaces and along the eighth cranial nerve. Although the clinical consequences of SS are often irreversible, we believe identification and repair of the source of bleeding is important to halt the progression of ataxia, hearing loss, and other symptoms.
Dural defects are a common and treatable cause of SS. Such defects are most frequently seen in the spine; they may be related to spontaneous ventral dural tears adjacent to spiculated osteophytes but can also be caused by trauma, surgery, and a variety of other etiologies.2,5,7 Dynamic CT myelography and digital subtraction myelography can be used to localize such defects.8,9 Dural defects can also occur in the posterior fossa, sometimes after surgery for tumors, Chiari malformation repair, or other procedures requiring incision of the dura. As posterior fossa leaks are less common than spinal CSF leaks, there is a paucity of data in the literature regarding the use of advanced imaging for their identification. 3
Our case demonstrates that in patients with a history of posterior fossa surgery presenting with new symptoms such as hearing loss, ataxia, or orthostatic headaches, a CSF leak associated with SS should be considered, particularly if a pseudomeningocele is seen on initial head CT imaging. MRI should be performed in such patients to confirm the presence of SS. If present, it is important to identify any persistent dural leak that may be causing progressive SS. CT cisternography may be useful to identify a dural defect and aid in preoperative planning. It is important to include high resolution thin section imaging in order to aid in the identification of a discrete dural tear. In addition, we show that postoperative CT cisternography is effective in confirming complete dural closure. In our case, conventional CT cisternography without any dynamic or delayed imaging was sufficient to identify one of the patient’s dural tears. Importantly, preoperative imaging may still miss very subtle dural defects; in our case, a second defect was identified intraoperatively that was not apparent on CT cisternography, even in retrospect. Therefore, it is important for surgeons to use preoperative imaging for guidance but also scrutinize the dura for additional sites of occult leak.
The mechanism of SS in patients with posterior fossa CSF leaks remains uncertain. In a prior series of patients, it was speculated that ventriculoperitoneal (VP) shunt placement and/or friable vessels along open dural edges may have contributed to the development of SS. 3 Our case would support the latter hypothesis. Future study of a larger cohort of patients with SS and prior posterior fossa surgery would be helpful to elucidate further the mechanism of this disorder and clarify appropriate diagnostic steps.
Conclusion
We have presented a case of SS in a patient with remote posterior fossa surgery for a Chiari I malformation. CT cisternography was effective in identifying a discrete dural defect preoperatively, as well as demonstrating watertight closure of the defect postoperatively. Surgery confirmed this finding and showed a second dural tear that was occult on imaging. Our case illustrates three main teaching points. First, incomplete dural closure after posterior fossa surgery may result in SS, particularly in patients presenting with postoperative pseudomeningoceles. Second, CT cisternography can identify the site of dural leak and aid in preoperative planning, as well as confirm complete dural closure after surgery. Finally, our case emphasizes the importance of careful evaluation of the dura during surgery to identify tears that may be occult on imaging.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Informed consent was obtained from the patient for medical images and records to be used for research purposes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.