
Abstract
Dural arteriovenous fistulas can lead to catastrophic intracranial hemorrhage if left untreated. Transvenous embolization can cure arteriovenous fistulas, but preserving normal venous structures can be challenging. Inadvertent embolization of a functioning vein can result in catastrophic venous infarction or hemorrhage. Here, we report a case using balloon-assistance to facilitate preservation of the superior petrosal sinus during transvenous embolization of a sigmoid sinus dural arteriovenous fistula.
Introduction
Dural arteriovenous fistulas (dAVFs) can lead to catastrophic intracranial hemorrhage if left untreated. Transvenous embolization can cure arteriovenous fistulas (AVFs), but preserving normal venous structures can be challenging. Inadvertent embolization of a functioning vein can result in catastrophic venous infarction or hemorrhage. Here, we report a case using balloon-assistance to facilitate preservation of the superior petrosal sinus (SPS) during transvenous embolization of a sigmoid sinus dAVF.
Case report
An 88-year-old woman developed new, continuously present, left pulsatile tinnitus. Her neurologist, to whom the patient was well-known because she was treating her cervical dystonia with botulinum toxin injections, ordered an Magnetic Resonance Imaging (MRI) and Magnetic Resonance Angiogram (MRA) for further evaluation. Her past medical history included systemic hypertension, pulmonary hypertension, and a transient ischemic attack 5 years earlier characterized by double vision and facial weakness. She also had a history of continuous-tone, non-pulsatile tinnitus, which resolved with hearing aid use. She had no antecedent trauma or known hypercoagulability. Her medications included oxycodone, diltiazem and tadafanil. The MRI and MRA showed asymmetric enlargement of the left external carotid artery branches with abnormal trans-osseous arteries adjacent to the left transverse sinus (Figure 1). There was abnormal flow-related enhancement on MRA in the left transverse sinus, with abnormally elevated arterial spin labelling (ASL) signal in the left transverse, sigmoid sinus and inferior petrosal sinus as well as the vein of Labbe. She was referred to the neurointerventional service for evaluation and management. Her neurological examination was normal. The presence of an abnormal ASL signal in the vein of Labbe was felt to likely represent a Cognard IIa+b shunt, conveying an estimated annualized hemorrhage risk of 10%. 1 After a discussion of the risks, benefits, and alternatives to treating this dural arteriovenous fistula, the patient made the decision to proceed with diagnostic angiography and possible embolization.
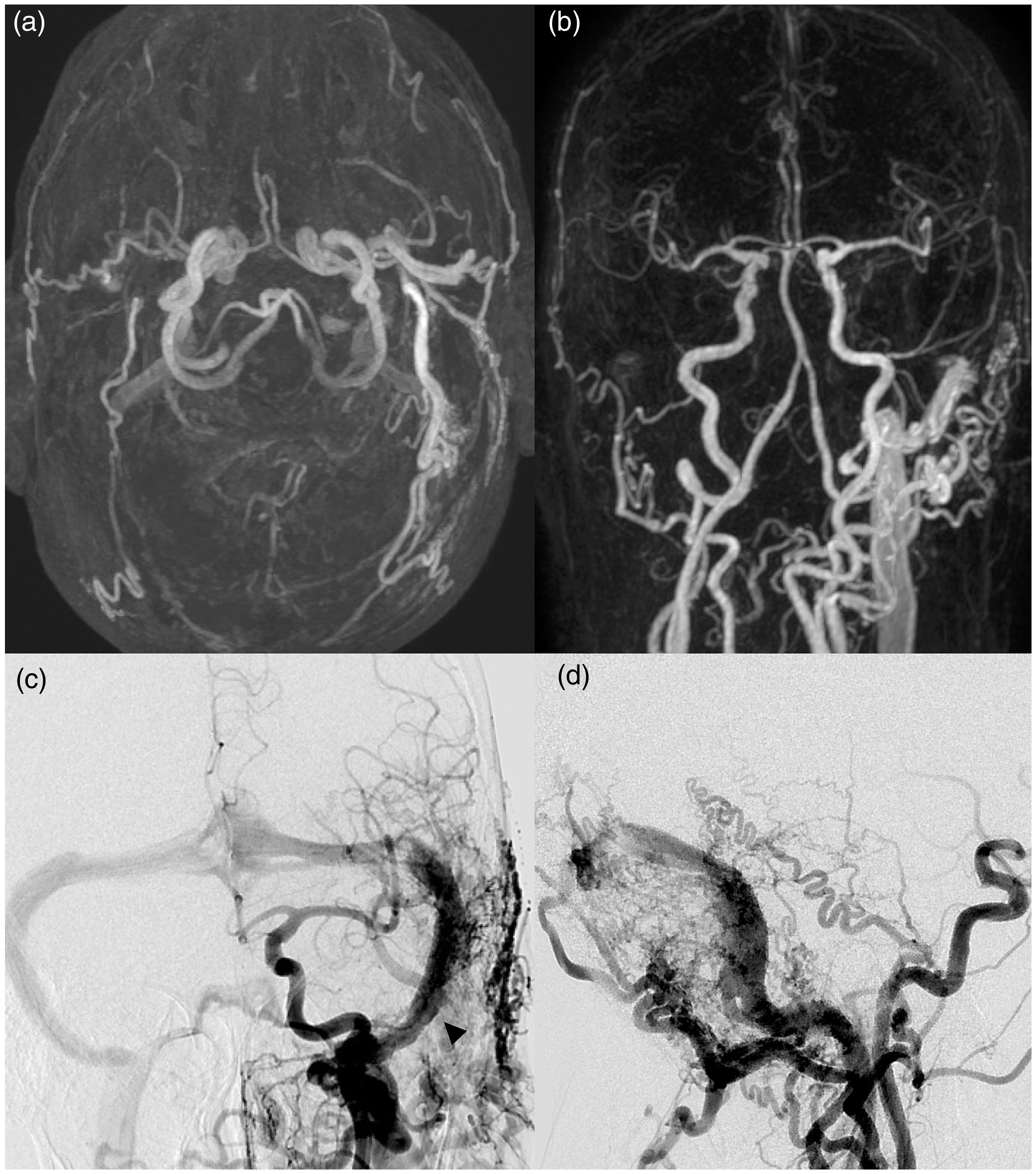
Brain maximum intensity projection (a) and coronal Maximum Intensity Projection (MIP) (b) of gadolinium-enhanced Magnetic Resonance Angiogram (MRA) demonstrate asymmetric enlargement of the left external carotid artery branches with abnormal transosseous arteries adjacent to the left transverse sinus. Subsequent angiography of the left common carotid artery shows extensive arteriovenous shunting into the left sigmoid sinus (arrowhead) by numerous branches of the left external carotid artery as well as meningeal branches of the left internal carotid artery in (c) Towne’s projection and (d) lateral projection.
The intervention was completed under general anesthesia. Selective injection of the left common carotid artery showed extensive arteriovenous shunting into the left sigmoid sinus by enlarged branches of the left external carotid artery (middle meningeal artery, anterior and posterior auricular arteries, ascending pharyngeal artery, and transmastoid branches of the occipital artery), pial branches of the left internal carotid artery (temporal branches of middle cerebral artery), the vertebrobasilar system (left posterior cerebral artery, left superior cerebellar artery, and direct feeders from left vertebral artery and its posterior meningeal branch), and branches of the meningohypophyseal trunk of the left internal carotid artery (Figure 1). The principal outflow of the shunt was unrestricted, via the left sigmoid and jugular vein, with some reflux via the inferior petrosal sinus to the cavernous sinus and circular sinus. Although no direct cortical venous reflux was observed, antegrade drainage of the vein of Labbe was sluggish, suggesting impending stagnation and/or reversal of flow, which guided the decision to pursue endovascular treatment. The SPS inserted into the sigmoid sinus immediately adjacent to the most cranial aspect of the fistula. No cortical veins were draining into the sigmoid sinus at the site of the fistula. Selective injection of the left subclavian and vertebral artery showed the supply to the fistula from the temporal branches of a posterior cerebral artery and left superior cerebellar artery. Supply from the right posterior meningeal artery (PMA) branch was also confirmed.
Given the large number of pial arterial feeders, transarterial treatment with liquid embolic agents was deemed to have a significant risk of nontarget embolization, which could result in stroke. 2 The presence of pial arterial supply and lack of cortical venous drainage into the sigmoid sinus at the site of fistula favored transvenous coil embolization. 3 First, a triaxial catheter system comprised of a 071 6 Fr Benchmark (Penumbra, Alameda, California, USA), a 038 Distal Access Catheter (Stryker Neurovascular, Kalamazoo, Missouri, USA) and a Prowler Plus microcatheter (Cerenovus/Codman, Alameda, California, USA) prepared over a Synchro 2 microwire (Stryker Neurovascular, Kalamazoo, Missouri, USA) was advanced into the left jugular vein. A 5 Fr University of California San Francisco (UCSF) 2 diagnostic catheter (Cordis, Miami Lakes, Florida, USA) was advanced into the right vertebral artery and attached to a heparinized saline drip; this catheter was used to visualize the most distal arterial feeders (relative to the heart) to the fistula which arose from the PMA and were used as a landmark to determine the distal extent of coiling necessary to obliterate the shunt. However, the left SPS insertion was noted to be very close the shunt site (less than 7 mm). To confirm physiologic drainage pattern of the SPS, a balloon (TransForm 7 × 7 mm Stryker Neurovascular, Kalamazoo, Missouri, USA) was inflated in the left sigmoid sinus at the origin of the left SPS, and angiography showed stagnation of flow in the left SPS (Figure 2(a) and (b)). This provided supporting evidence that inadvertent occlusion of the SPS-sigmoid connection could result in catastrophic venous infarction of the SPS watershed. To avoid this complication and still achieve angiographic cure with high-precision placement of coils to treat the most distal extent of the fistula, the balloon was again inflated in the sigmoid sinus, temporarily occluding the origin of the left SPS but not covering the fistula site. Using this balloon as a “backstop,” coil embolization of the diseased sigmoid sinus was performed in a distal to proximal fashion (Figure 3). The balloon was only used during initial placement of the “framing coils” (Figure 2(c)), and then pulled through the coil construct under a blank roadmap to ensure that the coils did not migrate after accurate positioning of the coils was confirmed (Figure 2(d)). The fistula was coiled to angiographic cure, and flow within the SPS was unimpeded on control angiography (Figure 4).
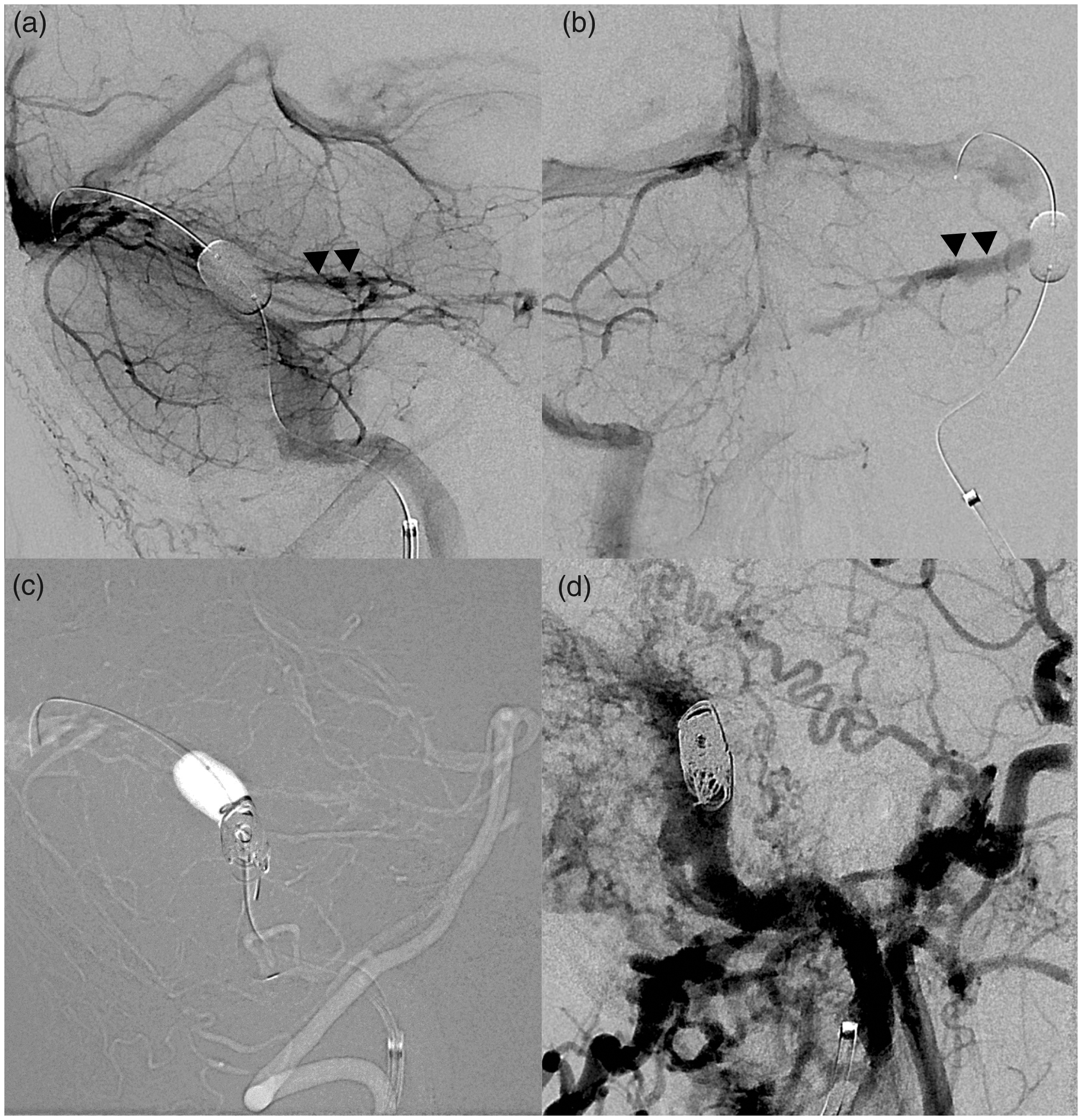
Injection of the left vertebral artery, with Transcend balloon inflated in the sigmoid sinus, temporarily occluding the insertion of the superior petrosal sinus (SPS: double arrowhead) in lateral (a) and anterioposterior Towne’s (b) projections showed stagnation of flow in the SPS. Lateral projection blank roadmap (c) was used during placement of initial framing coils at the distalmost fistula site, using the balloon as a ‘backstop’ to shape the initial framing coils (note the “flat” or “concave” appearance of the superior aspect of the coil mass). Post-deflation from the same vessel (d) shows stable position of the framing coils within the sinus, facilitating dense coiling of the shunt with softer, filling coils.
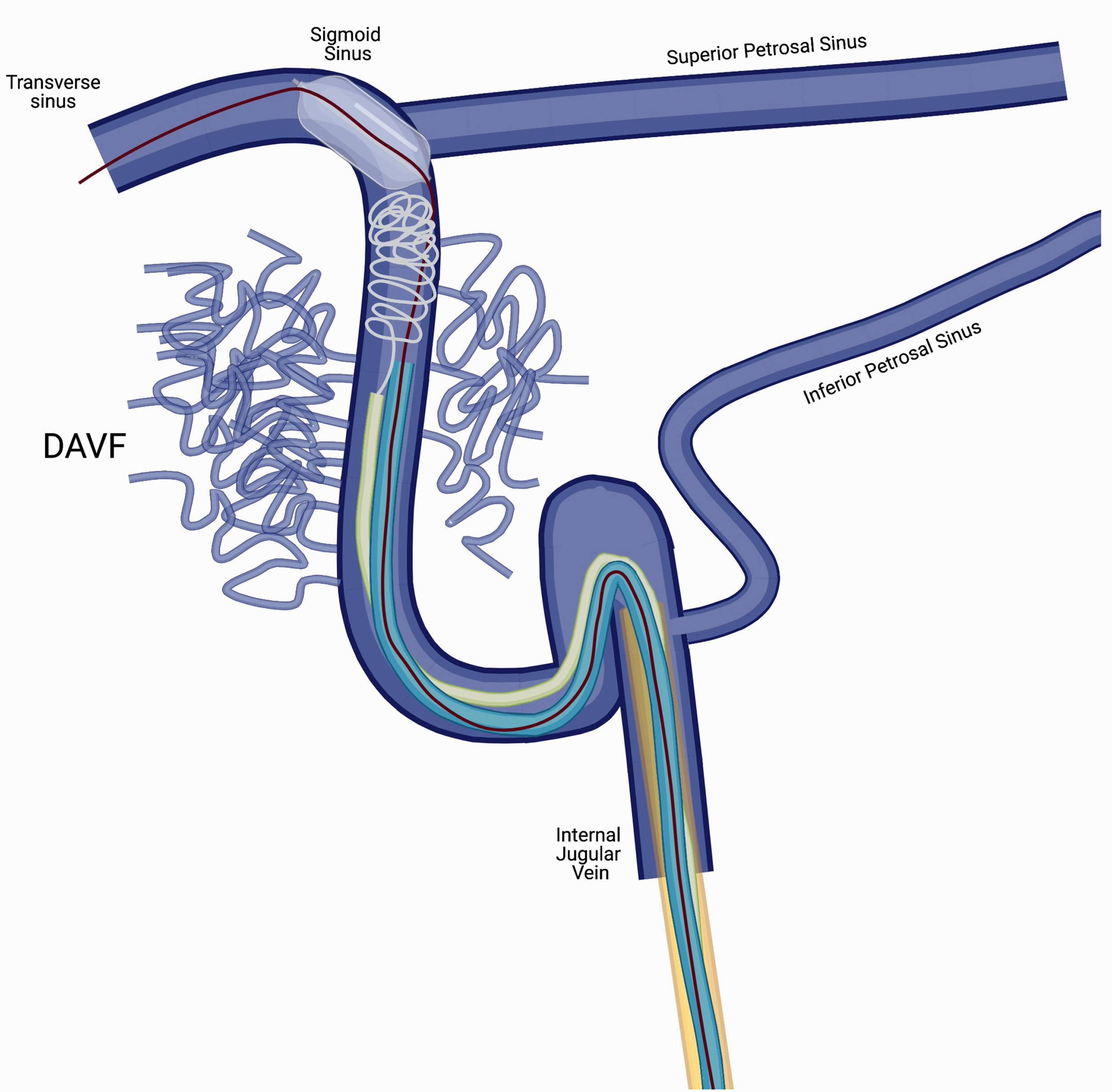
Technical diagram of balloon-assisted backstop coiling. A triaxial catheter system comprised of a 071 6 Fr Benchmark, 038 a Distal Access Catheter, a Prowler Plus microcatheter prepared over a Synchro 2 microwire, placed within the left jugular vein. The balloon is inflated in the left sigmoid sinus, at the origin of the left superior petrosal sinus. Coils were then placed to treat the distal extent of the fistula, to place “framing coils,” after which the balloon was deflated to place rest of coils. Created with BioRender.com. DAVF: dural arteriovenous fistula.
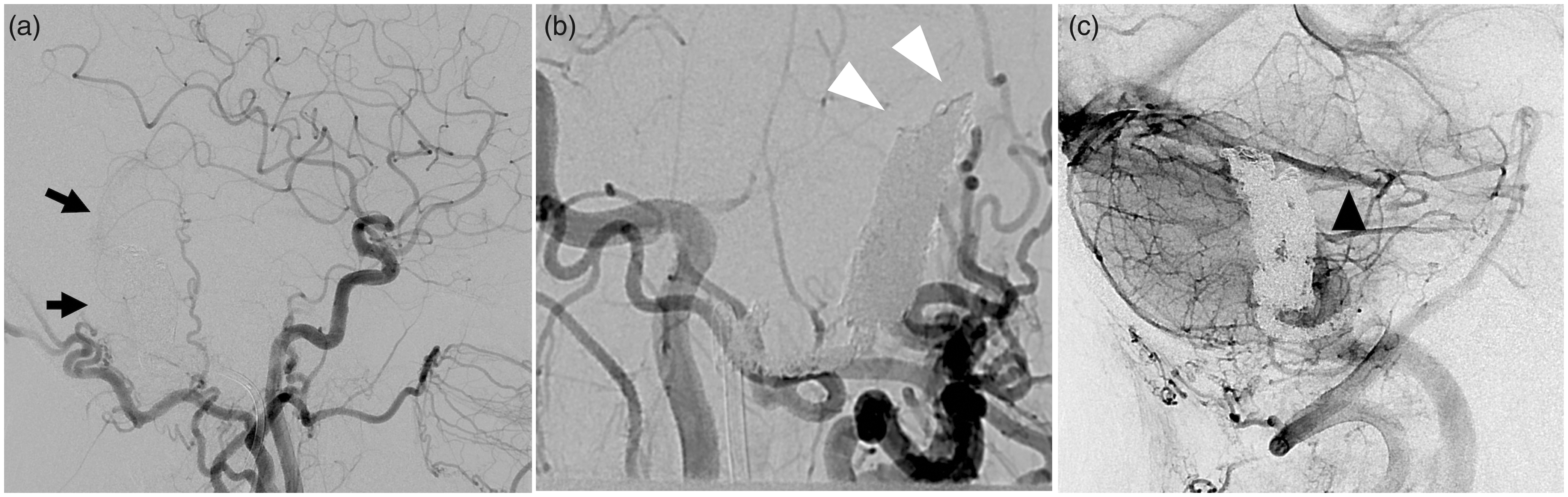
(a) Post-embolization left common carotid artery (CCA) injection in the lateral projection show final position of coils (arrows) with no residual shunting. (b) A magnified oblique injection of the left CCA highlights the “flattened” appearance of coils due to balloon-backstop remodeling (white arrowheads). (c) Venous phase left CCA injection in lateral projection shows normal filling of the superior petrosal sinus, inserting just cranial to the coil mass.
Discussion
In this case we report the use of an endovenous balloon as a “backstop” to prevent inadvertent occlusion of a physiologically healthy vein during transvenous coil embolization of sigmoid dural AVFs.
dAVF of the sigmoid sinus may be amenable to transarterial or transvenous endovascular treatment strategies, but in certain circumstances, transvenous coiling can be the safest and most durable option.3–5 Transvenous embolization may be particularly preferable in patients with large amount of pial arterial supply. 2 Despite the favorable safety profile relative to liquid embolic approaches, transvenous coiling can result in complications when cortical veins draining into the recipient pouch are occluded. Neurointerventionalists must recognize the risk of unintentional occlusion of normal cortical veins when sacrificing the fistulous sinus. In this case, angiographic cure of the AVF required occlusion of the sinus at the insertion site of the most distal arterial feeders. Failure to do so would not have cured the fistula and would have also made subsequent treatment options more difficult – requiring either a trans-arterial approach or a contralateral venous approach with crossing of the torcula. The proximity of the superior petrosal insertion site to the fistula presented a considerable challenge, which was successfully addressed using a balloon as a backstop when placing the coils into the sigmoid sinus allowed for preventing the coils from blocking the insertion of the left SPS. Inadvertent injury of the SPS is increasingly recognized as a hazard of skull-base surgery, which carries morbidity of up to 30%. 6 The risk of endovascular occlusion is less well understood but poses a similar theoretical risk. Although normal venous drainage in the brain could occur via the right sigmoid sinus system, the preservation of the left petrosal sinus reduces risks of venous congestion, venous infarction or hemorrhage.
Since the 1970s, dural AVFs were treated with several different types of therapeutic embolization, using polyvinyl alcohol (PVA) particles, ethyl alcohol, cyanocryalates, coils as well as more recently Onyx. 7 DAVFs with direct cortical drainage veins are often treated with Onyx due to its predictable polymerization and controllability in release, precluding non-target embolization or occlusion of healthy vessels. However, as all experienced operators know, when a large volume of Onyx is deposited around the fistula, it can be difficult to accurately visualize and identify retrograde filling of the pial arteries with Onyx. Retrograde filling of the pial arteries with Onyx can lead to stroke. In such cases, the transvenous approach is an elegant and less risky alternative. In addition, in cases where the cortical veins are no longer draining via the sinus, transvenous treatment can be used to completely occlude the diseased sinus.8–10 However, in some complex dAVF cases, normal cortical veins insert near the fistula site and it may be difficult, particularly while using soft coils, to avoid inadvertently covering the insertion of the cortical veins.
The use of detachable endovascular balloons for treatment of fistulas was one of the first successful endovascular approaches described in the literature. 3 , 11 The evolution of this original technique is evident in more recent applications, such as the use of endovascular balloon-remodeling for transarterial aneurysm treatment with the intent of avoiding coil prolapse. 12 The use of dural sinus balloons as adjuvant tools is relatively new, with several recent studies reporting their use to block transarterial liquid embolic agents from filling the sinus, and potentially refluxing into cortical veins. 8 , 13 , 14 This technique requires specialized balloons that are compatible with dimethyl sulfoxide (DMSO), the solvent for Onyx. Building from this technique, we define a new role for dural sinus balloons as temporary scaffolding for transvenous (TV) coil embolization. After identifying essential drainage veins near the target embolization site, a balloon can be inflated across the insertion sites of healthy veins and coils can then be deployed into the large, diseased sigmoid sinus, without risk of migration or herniation of coils into the healthy vein. This serves both to protect an at-risk vein and enables dense coiling of the diseased sinus, increasing the chances of immediate and durable cure. The “backstop” feature of the balloon is another benefit of this technique, preventing premature “upstream” displacement of coils before they are fully deployed and detached. In addition, the balloon used for this technique does not need to be DMSO-compatible, any appropriately-sized neurovascular balloon will suffice. The additive risks of balloon-protected TV coiling are relatively small but include theoretical risk of sinus rupture and subdural hemorrhage. This risk is minimized by use of a super compliant balloon and intermittent deflation. 9 Another approach to consider would be to use a separate venous access to position the balloon via a contralateral approach by crossing the torcula. This would have obviated the need to pull the balloon through the coil mass and may have limited the chances of coil migration.
In summary, the authors describe a novel method of cortical venous protection during TV embolization of cranial AVFs. This technique mitigates the risk of venous complications without substantial added risk, and further expands the scope of fistulas amenable to cure by the TV approach.
Footnotes
Acknowledgements
MD wrote the manuscript with the help of MC, KN, and MA. All authors discussed the case and contributed to the final manuscript. The patient provided written informed consent for the publication of patient information and images.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by National Institutes of Health (NIH) National Heart, Lung, and Blood Institute (NHLBI) of the NIH under the award number R56HL149124-01.