
Abstract
The sellar, suprasellar, and parasellar space contain a vast array of pathologies, including neoplastic, congenital, vascular, inflammatory, and infectious etiologies. Symptoms, if present, include a combination of headache, eye pain, ophthalmoplegia, visual field deficits, cranial neuropathy, and endocrine manifestations. A special focus is paid to key features on CT and MRI that can help in differentiating different pathologies. While most lesions ultimately require histopathologic evaluation, expert knowledge of skull base anatomy in combination with awareness of key imaging features can be useful in limiting the differential diagnosis and guiding management. Surgical techniques, including endoscopic endonasal and transcranial neurosurgical approaches are described in detail.
Introduction
This review article will address the spectrum of pathologies occurring in the sellar, suprasellar, and parasellar space, including neoplastic, congenital, vascular, inflammatory, and infectious etiologies. We will address treatment options, including neurosurgical approaches for surgical biopsy or resection.
Sellar space and masses
Neoplasms
Pituitary Microadenoma and Macroadenoma. Pituitary adenoma is the most common sellar mass, arising from the anterior pituitary hormone secreting cells.1-4 Microadenomas are defined as less than 10 mm in size, while macroadenomas are larger than 10 mm. Pituitary adenomas show variable T2 signal, have mild to moderate contrast enhancement, but can be heterogenous due to hemorrhage, cystic change, or necrosis.
2
Dynamic contrast-enhanced MRI images add value to conventional post-contrast images in detecting microadenoma, which are typically visualized as a round area of decreased enhancement compared to surrounding pituitary gland (Figure 1(a)).
5
Larger tumors have lobulated tumor margins, displace the infundibulum to the contralateral side, enlarge and remodel the sella, and can invade the clivus or cavernous sinuses.2,6 Sellar expansion, absence of intra-tumoral calcification, and inability to separate tumor from the pituitary gland are the most helpful features in establishing the diagnosis on imaging.
2
On coronal plane, macroadenoma can have a figure of eight, or snowman appearance, narrowed in the mid-portion by the diaphragm sella.
2
Up to 10% of macroadenomas demonstrate cavernous sinus invasion, and there is potential for encasement of the internal carotid artery (ICA).
7
Greater than 67% encasement of ICA on imaging had 100% positive predictive value for invasion as confirmed by surgery.
7
Tumors that invade cavernous sinus are more biologically aggressive with increased surgical morbidity and mortality, and cavernous sinus invasion is the limiting factor for complete resection.
2
Sellar lesions. (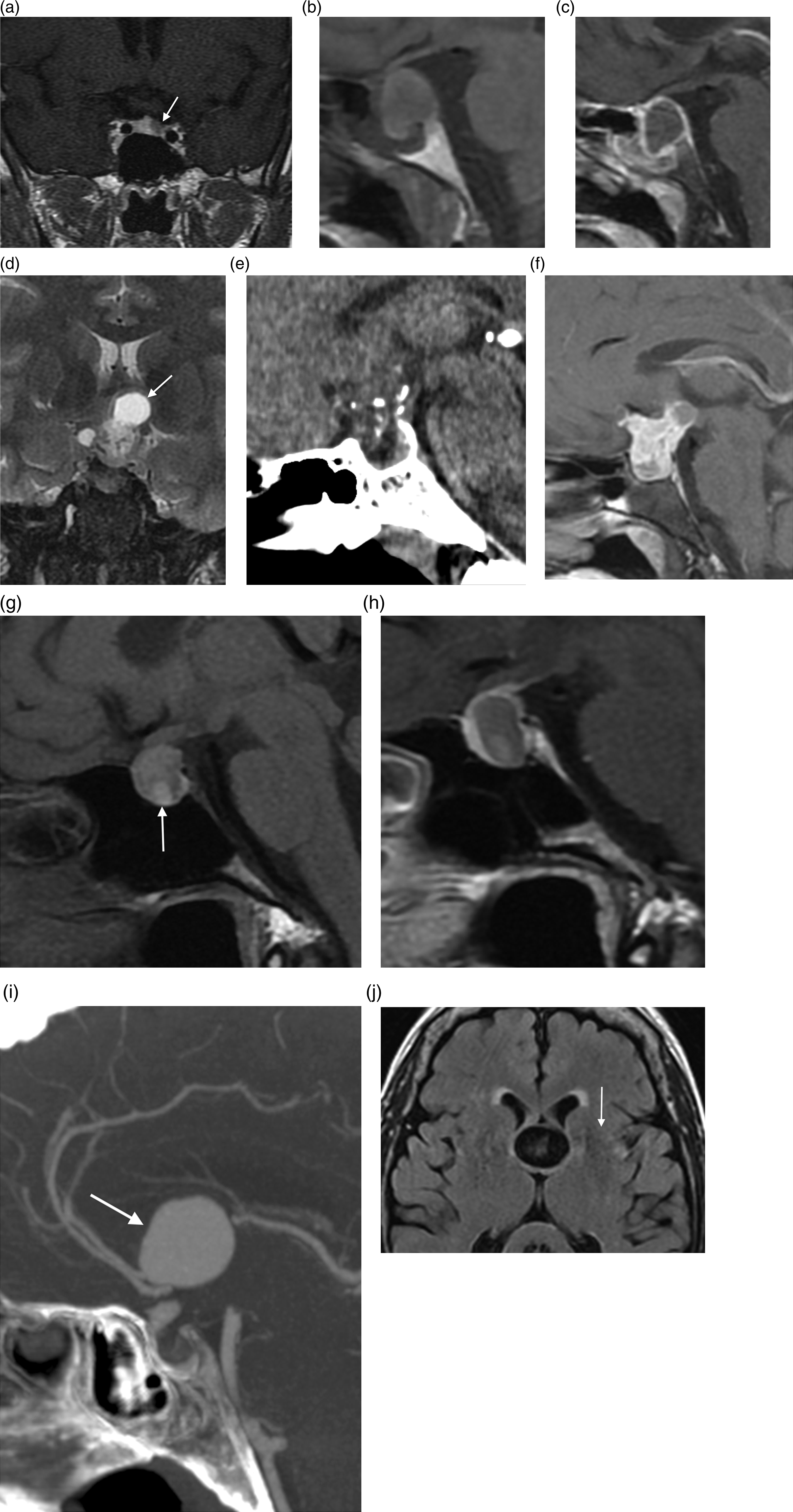
Pituitary apoplexy and hemorrhage. Pituitary apoplexy is the acute ischemic or hemorrhagic infarction of a pituitary gland, typically within a pre-existing adenoma. 7 Patients present with a headache, nausea, visual deficits, altered mental status, ophthalmoplegia, or endocrine dysfunction. 8 Acute presentation differentiates apoplexy from hemorrhage within adenoma (typically stable patient). Apoplexy should be considered in sellar masses in the setting of acute presentation, heterogenous pituitary gland signal, fluid-fluid level, T1 shortening (bright T1 signal), lack of central enhancement, and thin peripheral linear enhancement (Figure 1(b) and (c)). 2 Treatment includes medical and surgical options depending on the clinical status.
Meningioma. Meningioma is the second most common sellar and parasellar tumor, and the most common primary central nervous system (CNS) neoplasm. 2 They are three times more common in women and most occur after age 55. 7 In the sella and central skull base, meningiomas can arise from the tuberculum sella, dorsum sella, diaphragm sella, clivus, sphenoid wing, cavernous sinus dura, and planum sphenoidale. On CT, they tend to be isointense to hyperdense to brain parenchyma and may be calcified. On MRI, they are well defined, isointense to hypointense on T1 and T2. They demonstrate characteristic intense homogenous enhancement on CT or MRI.2,6,9 Meningiomas form obtuse margins with their broad-based dural attachments. Dural tail is a characteristic finding. A cerebrospinal fluid (CSF) cleft between the mass and the normal appearing pituitary gland points to the diagnosis of meningioma, and not pituitary adenoma. Hyperostosis of adjacent bone is another frequent feature of meningiomas.2,9 Pneumosinus dilitans, or abnormal dilatation of an adjacent paranasal sinus, has been described in meningioma.2,7 Identification of ICA encasement, involvement of the optic chiasm, olfactory grooves, and optic canals is important in pre-surgical planning. Treatment options include surgery and radiation therapy. 2
Craniopharyngioma. Craniopharyngioma and Rathke cleft cysts (RCC) arise from Rathke pouch remnants and can occur anywhere from the nasopharynx to the third ventricle. In children, these are the two most common intrasellar pathologies. 10 Craniopharyngioma is neoplastic, while RCC is congenital. Craniopharyngiomas are the most common non-glial tumor in children, and second most common suprasellar mass, after macroadenoma.2,4 Craniopharyngioma has a bimodal age distribution of 5–14 years old and 50–75 years old. 7 There is no gender predilection. 4 In children, the adamantinomatous subtype is most common. Calcifications and solid/cystic components are typically the pathognomonic features.2,7,8 CT and MRI demonstrate the solid/cystic lobulated mass with enhancing components. Intratumoral cysts may be T1 hyperintense (internal cholesterol contents) (Figure 1(D)-(F)). In adults, the papillary subtype is seen more commonly, has predominantly solid and rounded appearance; calcifications and cysts are less common. 10 Craniopharyngiomas originate from infundibulum, are more commonly suprasellar (75%), combined intra and suprasellar (21%), and rarely purely intrasellar (4%). 6 Extension into the anterior/middle cranial fosse occurs up to 30% of the time, and can also extend into the prepontine space; occasional vessel encasement.7,10 Pituitary adenoma can be excluded from the differential diagnosis if normal pituitary gland is seen separate from the mass.
Metastasis. Other tumors can involve the sella via direct invasion from nearby structures or hematogenous/perineural spread. Metastasis to the pituitary gland is much rarer than the nearby osseous skull base metastasis. 7 The most common tumors to metastasize to the sella are breast, lung, renal, colorectal, and prostate cancer.3,7 Primary brain tumors such as ependymoma, medulloblastoma, germinoma, and pineoblastoma can seed the suprasellar area and the anterior third ventricular recesses. Infundibulum thickness measuring more than 3 mm on post-contrast images could be pathologic. 11
Posterior Pituitary Tumors. World Health Organization (WHO) Grade 1 posterior pituitary tumors are rare sellar pathologies and include pituicytoma, granular cell tumor, spindle cell oncocytoma, and sellar ependymoma.1,12 A frequent imaging pitfall includes misdiagnosis as non-functioning pituitary macroadenoma.
Congenital
Rathke Cleft Cyst. RCCs are benign cystic remnants of Rathke’s pouch.10,11 They are more common in females, with symptomatic patients presenting at age 30–60.4,7 MRI shows a midline cystic lesion with homogenous T1 and T2 signal, though the signal may vary based on protein concentration, mucopolysaccharides, and rarely hemorrhage.2,7,10 The presence of a T1 hyperintense and T2 hypointense intracystic nodule is suggestive of the diagnosis (Figure 1(g)). The presence of a fluid–fluid level, a hypointense rim on T2-weighted images, septation, and an off-midline location are more commonly seen with pituitary adenomas, whereas the presence of this intracystic nodule is more common with RCCs. 5 RCCs do not have solid components, and do not enhance with contrast, separating them from adenomas and craniopharyngiomas (Figure 1(h)). The high T1 signal may mimic apoplexy, but the clinical presentation of RCC is either asymptomatic or a chronic presentation, whereas apoplexy presents with acute symptoms. 2 RCC are more frequently sellar and suprasellar (87%), rather than isolated in either compartment.2,10 RCC characteristically causes midline anterior infundibular displacement. 9 A cyst less than 3 mm in the sella may represent an incidental pars intermedia cyst, which cannot be differentiated on imaging from RCC, and requires no follow up if asymptomatic. 10 Because RCC is a benign cyst, drainage of the cyst to improve mass effect, or partial excision can be considered, and weighed against the risk of recurrence; 10–14% of them can “reaccumulate.” 2
Vascular
Aneurysms. Aneurysm may arise from the cavernous or supra-clinoid ICA, ophthalmic artery, or anterior communicating artery; giant aneurysms are those over 2.5 cm. 7 Aneurysms are important to consider as a potential diagnosis of the sellar/suprasellar mass in order to avoid potential biopsy and prevent catastrophic outcome. They can enhance homogeneously after contrast administration on CT angiography (CTA) or MR angiography (MRA) (Figure 1(i)). Rim calcification is a supportive feature for aneurysm. 2 On CT, aneurysms can remodel the skull base and extend into the parasellar spaces, infratemporal fossa, or parapharyngeal space. 7 The sella should not be expanded, pointing away from macroadenoma as a diagnosis. Aneurysms have T2 dark signal void in the un-thrombosed areas. The thrombosed portion may be T1 bright and can have lamellated appearance on T1 and T2 images along the periphery. The MRI feature that can be a clue is phase misregistration artifact from disordered turbulent intranidal flow. This artifact is linear, left to right, representing a pulsation artifact in the phase encoding direction (Figure 1(j)). 8
Infectious and Inflammatory Lesions
Infection. Pituitary abscess is a rare but potentially life-threatening condition. 13 Infection typically spreads hematogenously or contiguously from sphenoid sinus, and rarely from a thrombosed cavernous sinus. Infection is most often seen in the immunocompromised patients, with fungal disease a common etiology. 3
Inflammatory. Wegener’s disease is a systemic granulomatous disorder with necrosis and small vessel vasculitis, closely associated with anti-neutrophil cytoplasmic antibodies. The disease classically affects the ear, nose, throat, lung, and kidneys. There can additionally be either vasculitis of the pituitary vessels, granulomatous lesions in the sella, or extension of disease from the paranasal region. Erdheim-Chester disease is exceedingly rare, more frequently found in adults. 13 Other diseases including giant-cell granulomatous hypophysitis, Takayasu disease, Cogan syndrome, and Crohn’s disease can affect the pituitary gland. Lymphocytic hypophysitis and sarcoidosis will be discussed in the suprasellar section.
Tumor mimics
Physiologic Enlargement. Pituitary enlargement, up to 12 mm in pubertal females or during pregnancy, should not be mistaken for an adenoma, especially if there are no clinical or laboratory signs pointing toward adenoma.2,10,14 Pituitary hyperplasia can also mimic a mass. 10
Suprasellar space and masses
Neoplastic
Optic Pathway Glioma. Gliomas of the hypothalamus, optic nerves, optic chiasm, and along the visual pathways are common cause of suprasellar masses. One third of suprasellar gliomas are related to neurofibromatosis type 1 (NF1), and is the most common CNS neoplasm in NF1.
7
The great majority are diagnosed before age 20, syndromic cases usually before age 4, and can less commonly occur in older adults. NF1 related gliomas are typically low-grade histologically and slow growing, typically pilocytic astrocytoma (Figure 2(a) and (b)).
10
Sporadic gliomas tend to have worse outcomes. While syndromic cases favor the optic nerve location, sporadic cases more frequently involve optic chiasm or post-chiasmatic location. Optic pathway gliomas infiltrate and expand the optic nerve, optic chiasm, or optic tracts. On MRI, the masses are circumscribed, T1 hypointense to isointense and T2 hyperintense.7,10 They show variable enhancement patterns, and can present as non-enhancing, peripherally enhancing, or diffusely enhancing.4,6,7 The enhancement pattern does not correlate with tumor grade. Cysts are more common in sporadic cases. If NF1 is present, pre-treatment biopsy is typically not performed. However, if no NF1 is present, usually biopsy is indicated to identify the pathology and differentiate glioma from germ cell tumor.
10
Gliomas can be treated with chemotherapy, although surgery may be needed for obstructive physiology. Rarely, ganglioglioma or primitive neuro-ectodermal tumors (PNET) may involve optic pathways.
2
Suprasellar lesions. (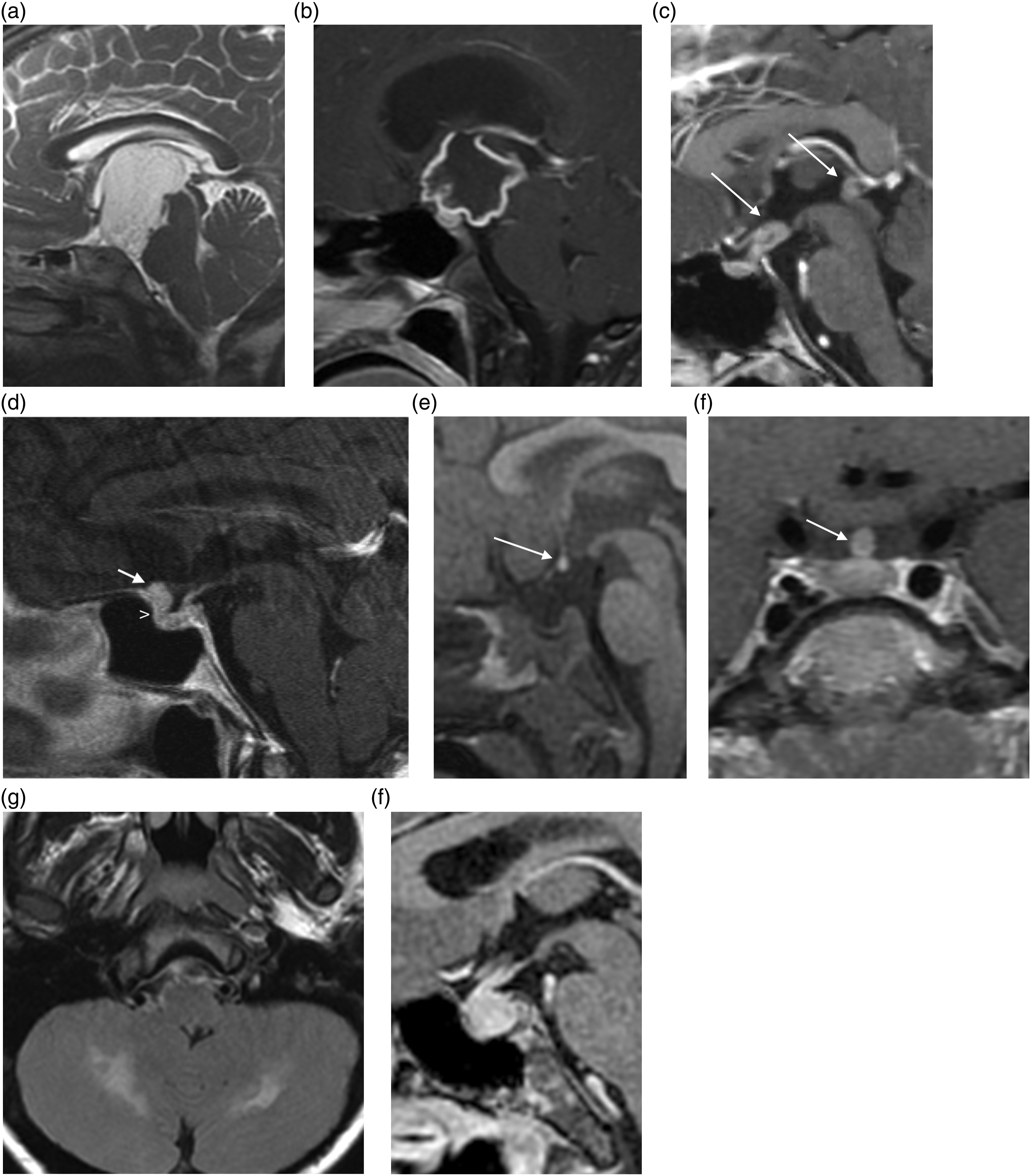
Suprasellar Germinoma. These tumors are more common in females, and frequently encountered in the first or second decade of life. 7 Germinomas present with hormonal dysfunction more often than suprasellar gliomas. Small germinomas are typically centered in the pituitary stalk and can extend to the hypothalamus and pituitary gland. Larger lesions can extend to the basal ganglia, highly suggestive of germinoma. Suprasellar germinomas may occur concurrently to those in the pineal region and can help narrow the diagnosis if masses are found in both locations (Figure 2(c)). Suprasellar germinomas are faster growing, more often non-cystic, non-calcified, and non-hemorrhagic when compared to gliomas. They demonstrate avid enhancement. 2 MRI may show restricted diffusion, low ADC values, and CT shows hyperdense tumor, due to high cellularity. Homogenous enhancement and low ADC values helps distinguish these tumors from craniopharyngioma in the pediatric population. There is greater propensity to disseminate into the subarachnoid space and the ventricular system as compared to optic/hypothalamic gliomas, and imaging of the entire neural axis is therefore recommended. These tumors are highly sensitive to radiation therapy. 6 Survival rates are greater than 90% at 5 years with radiotherapy alone for pure germinomas. 7
Other Neoplasms. Masses arising from the third ventricle, such as choroid plexus papilloma, ependymoma, parenchymal gliomas, metastases, meningioma (Figure 2(d)), and cavernoma can extend into the suprasellar cistern. 10
Developmental
Epidermoid Cyst. Epidermoids are rare developmental inclusion cysts containing ectodermal components. Despite being congenital, these lesions usually manifest later in life, the fourth to fifth decades.4,7 Epidermoid tumors are most commonly seen at the cerebellopontine angle, and less commonly in the parasellar, intraosseous location, chiasmatic cistern, prepontine cistern, or the sylvian fissure; they tend to occur off midline. 7 CT imaging shows a lesion with density similar to the CSF. Rarely, the CT density will be higher due to blood/protein. MRI demonstrates T1 and T2 signal similar to that of CSF, mildly brighter than CSF on fluid attenuated inversion recovery (FLAIR) sequence, and no enhancement; rarely they can show high T1 and low T2 signal. The most pathognomonic feature of epidermoid is restricted diffusion.7,8 Subtotal resection of the mass is often desired because of the non-malignant nature.2,6
Dermoid. Dermoid tumor is a congenital inclusion cyst of ectodermal elements. It is more common in males and may present from age 20–30. 6 They can be differentiated from epidermoid tumor because they follow fat signal on CT and MRI. The lesions are non-enhancing and hypodense on CT, with high T1 and T2 signal on MRI, and nulled signal with STIR and fat suppression techniques. Dermoid can be separated from RCC by identifying fat component. Dermoid tumors can rupture, causing chemical meningitis, with fat particle dispersion in the subarachnoid and intraventricular space, seen as T1 hyperintense foci, a pathognomonic finding. 6 Dermoid tumors are often suprasellar and parasellar, not intrasellar.
Arachnoid Cyst. Arachnoid cyst is a benign well-circumscribed non-neoplastic lesion filled with CSF. They are more common in males. Growth is rare and the majority of patients are asymptomatic. Lesions that lack communication to the subarachnoid space tend to be those that can enlarge and rarely cause obstructive hydrocephalus, cranial neuropathies, seizures, or headaches. Generally, on CT and MRI, the density and signal of the arachnoid cyst will mirror that of CSF.7,8 They are expansile, unilocular, and can cause osseous remodeling. 7
These can be located in the chiasmatic cistern or sella among and may rarely produce mass effect on the optic chiasm; more commonly, they are located in the middle cranial fossa. Arachnoid cysts can rarely have slightly bright FLAIR signal (in very large lesions) and never demonstrate restricted diffusion. Arachnoid cysts do not enhance, and tend to displace structures, while epidermoid tumors insinuate between them, a helpful differentiating feature. 4 Neurocysticercosis may mimick arachnoid cyst as clusters of racemose cysts in the cisternal space; however, neurocysticercosis should have parenchymal lesions as well.
Lipoma. Lipoma is an additional fatty benign lesion that can be found in the suprasellar cistern or interpeduncular region. It will appear more homogenous than a dermoid on imaging, as it is composed of fat.
Hypothalamic Hamartoma. A tuber cinereum hamartoma, or hypothalamic hamartoma, is a congenital lesion containing neural tissue and heterotopic hyperplastic gray matter. They are not true neoplasms but may grow over time. 4 Clinical symptoms are central precocious puberty or gelastic seizures. Lesions are well circumscribed, T1 and T2 isointense without enhancement, and following gray matter signal.7,10 They are isodense to gray matter on CT, and are frequently pedunculated. These features differentiate hamartomas from cystic/calcified craniopharyngioma or enhancing malignancies such as germinoma or astrocytoma.
Ectopic Pituitary. In pediatric patients, an ectopic posterior pituitary gland can mimic a mass, and was the most common stalk congenital lesion in a series by Mayo Clinic. 11 There may be a suprasellar or hypothalamic T1 bright spot, instead of at the normal site. There will be hormonal dysfunction. Pituitary stalk interruption syndrome is a rare entity, and imaging findings include ectopic posterior pituitary, thin or absent infundibulum, and absent/hypoplastic anterior pituitary (Figure 2(e)).
Inflammatory and granulomatous lesions
Langerhans Cell Histiocytosis. Langerhans cell histiocytosis (LCH) is caused by aberrant proliferation of specific dendritic cells belonging to the monocyte macrophage system. Peak presentation age is 1–3 years old and is more common in males. Most frequently present in the CNS with enhancement, mass-like thickening, and infundibular infiltration (Figure 2(f)). Loss of posterior pituitary bright spot is also a common finding. 13 Classically, LCH is known for osseous lytic lesions in the calvarium, skull base, or mastoids. If there is demyelination in the cerebellar white matter in the presence of infundibular mass, this is characteristic of LCH in the CNS (Figure 2(g)). 10 Biopsy of the stalk is not recommended if less than 7 mm thick. 13
Lymphocytic Hypophysitis. Lymphocytic hypophysitis is an autoimmune disease more frequently found in women, especially in pregnant or postpartum patients. 7 It should be considered if there are associated autoimmune conditions, such as thyroiditis or ipilimumab/drug-related disease. In a large case series, this entity was the most common cause of pituitary stalk pathology (25% of 209 cases).13,15 MRI may demonstrate symmetric enlargement of the pituitary gland and homogenous or centrally heterogenous pituitary enhancement. Pituitary gland destruction can occur. Other presentations include either smooth or mass-like infundibular thickening and enhancement (Figure 2(h)). The inflammation can efface the normal pituitary bright spot and may extend to the optic chiasm or cavernous sinuses. 10 Differential considerations include LCH, sarcoidosis, and metastasis.
Sarcoidosis. Sarcoidosis is a granulomatous inflammatory systemic and diffuse process that can involve the CNS. It typically involves young and middle-aged patients. Presenting symptoms include headaches, lethargy, polyuria, and polydipsia from diabetes insipidus. 10 CT can show pituitary stalk thickening. MRI can show uniformly thick or nodular stalk and pituitary enhancement. 11 The stalk may be T2 hypointense, as in other granulomatous lesions. Stalk thickening and enhancement may mimic lymphocytic hypophysitis; presence of enhancement in the cranial nerves, dura, or basal cistern leptomeninges is typical of sarcoidosis.7,15 Sarcoid was the second most common pituitary stalk pathology in a case series of 209 patients. 15
Other Pituitary Stalk Lesions. Rare inflammatory conditions associated with the pituitary stalk abnormality include Erdheim-Chester disease, Wegener hypophysitis, Xanthoma disseminatum, and lupus cerebritis. 11
Lateral parasellar space and masses
Introduction
The lateral parasellar area will be defined as the region between the lateral margin of the sella turcica (defined as the medial margin) and petroclival synchondrosis (defined as the lateral margin). Our discussion will be divided in two sections based on whether the abnormality’s epicenter is at the skull base or cavernous sinus.
Lateral parasellar masses commonly present with headache and cranial neuropathy. 16 Pathologies involving the central skull base include: chordoma, chondrosarcoma, plasmacytoma, metastasis, lymphoma, infection, and local extension from a primary sphenoid sinus, nasopharyngeal, or pituitary tumor. Lesions arising from or involving the cavernous sinus include meningioma, lymphoma, LCH, sarcoidosis, carotid-cavernous fistula, aneurysm, cavernous sinus thrombosis, perineural tumor, and infection. Tissue sampling and histopathologic evaluation is usually required for diagnosis due to imaging overlap between different pathologies. However, awareness of some key imaging features is useful in limiting the differential diagnosis or eliminating the need for biopsy in some cases. In this section, we will discuss entities that were not included in the previous sections.
Central skull base lesions - neoplasms
Chordoma. Chordoma, which originates from notochord remnant cells, is a rare midline mass with potential for local invasion that most commonly arises in the sacrum, cervical spine, and less commonly in the clivus. Average age of diagnosis is 55 years (range 40–75) with 1:1 gender distribution.2,17,18 In the skull base, it commonly arises from the spheno-occipital synchondrosis, and it typically extends into prepontine space. Bulk of the tumor is typically outside the bone, with smaller component involving the clivus.
19
Imaging features include intermediate/hypointense T1 signal, marked T2 hyperintensity (related to mucin and/or necrosis), and a component of lytic osseous destruction involving the adjacent bones (Figure 3(a) and (b)). “Lightbulb” bright T2 signal within the tumor and midline tumor location are characteristic findings, distinguishing this entity from other lesions.
19
The tumor demonstrates varying levels of enhancement and diffusion restriction. Cross-sectional angiography is useful in evaluation of adjacent vascular encasement or luminal narrowing and is important for surgical planning.
19
Local recurrence is common, necessitating the need for imaging surveillance following treatment.
20
Central skull base lesions. (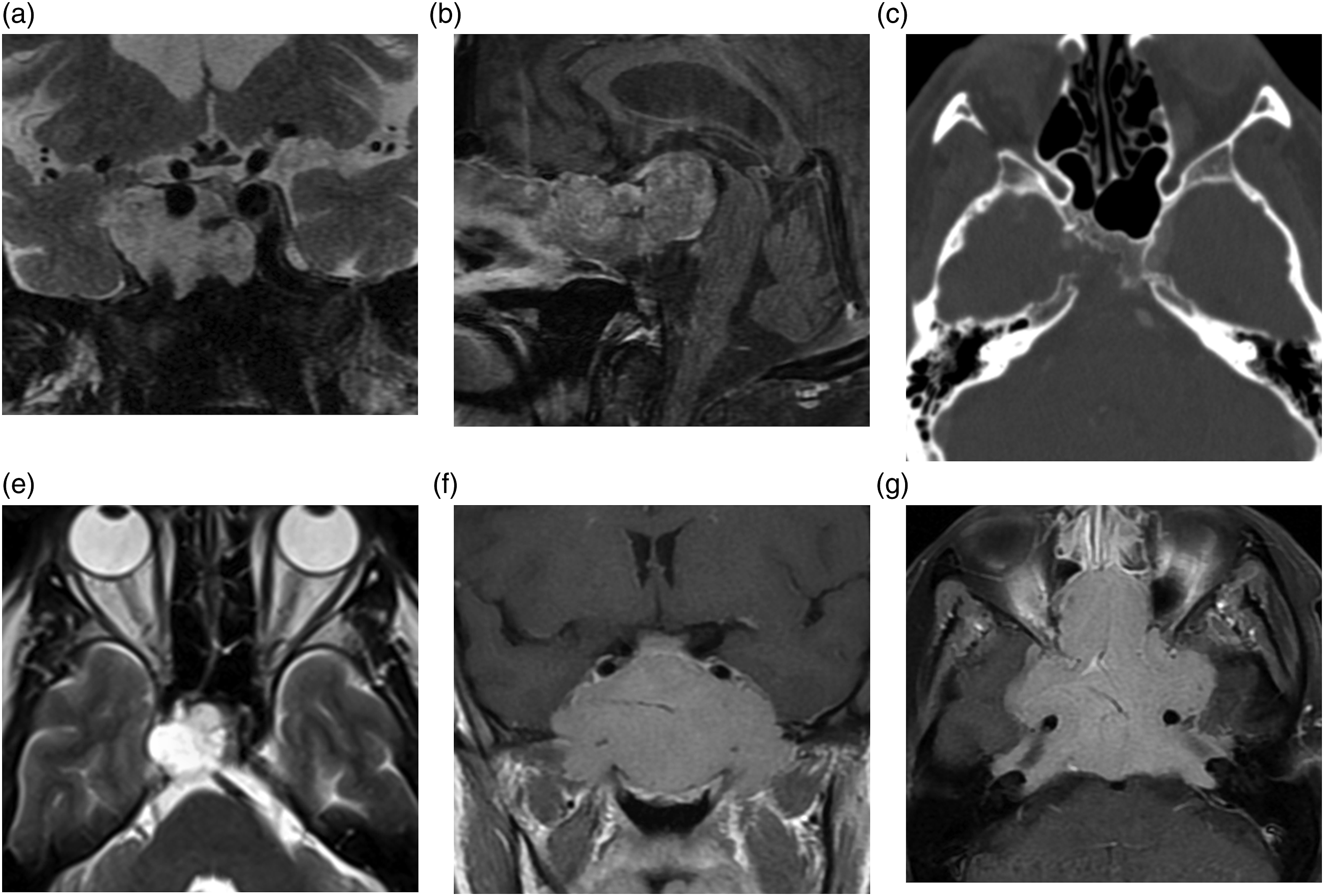
Chondrosarcoma. Chondrosarcoma is the second most common malignant bone tumor in general, occurs most commonly in adults (30–70 years). It accounts for approximately 5% of all skull base tumors.21,22 Imaging appearance of chondrosarcoma and chordoma overlap, both demonstrating bright T2 signal. 23 Key distinguishing feature is location of the tumor—chondrosarcoma is paramedian in location arising from the petro-clival synchondrosis, compared to classic midline location for chordoma (Figure 3(c) and (d)). Calcifications within chondrosarcoma are present approximately 41% of the time on CT.24,25 Because of the lateral location, ophthalmoplegia is a common presenting symptom. 26
Plasmacytoma. Plasmacytoma incidence rates are slightly higher in males, occur in adults (age range 20–80), and account for <1% of all head and neck tumors.27,28 They usually present with a cranial neuropathy. 29 CT demonstrates expansile lytic soft tissue mass. Compared to chordomas, plasmacytoma is centered within the bone. It has intermediate, gray T2 signal, which is related to higher cellularity and low water content. 2 In our experience, plasmacytoma can at times have mildly increased T1 signal on pre-contrast images, which is a helpful feature in pointing to the correct diagnosis when dealing with a destructive, enhancing skull base mass (Figure 3(e) and (f)). Lesions typically demonstrate heterogenous to avid enhancement. 30 When solitary plasmacytoma is diagnosed, additional imaging and laboratory analysis reveal occult multiple myeloma in approximately 40% of the patients. 28
Central skull base lesions - congenital/developmental
Encephalocele. Skull base meningocele and encephalocele are important considerations when evaluating a parasellar mass-like lesion, as they can mimic a neoplasm. Accurate diagnosis is important in order to avoid a potential biopsy. They most often develop as a sequela of previous trauma, surgery or complication of a long-standing idiopathic intracranial hypertension.31,32 If they involve the petrous apex or sphenoid sinus, they can extend into the central skull base. CT findings will demonstrate smooth bony expansion or bone gap in the central skull base, and MRI is helpful in making a definitive diagnosis. 31 If congenital, they tend to present in the first year of life in the pediatric population.33,34
Epidermoid Cyst. Discussed in the “Sellar Space and Masses” section.
Cavernous sinus lesions - neoplasms
Meningioma. Meningioma is discussed in the “Sellar Space and Masses” section. In the parasellar region, meningiomas are located along the surface of the clivus, sphenoid wing, cavernous sinus, and planum sphenoidale. Tumor extension to the cavernous sinus and sella turcica is common.
35
Parasellar meningioma often encases and causes stenosis of the cavernous or supra-clinoid internal carotid artery (Figure 4(a) and (b)).
36
Lateral parasellar lesions. (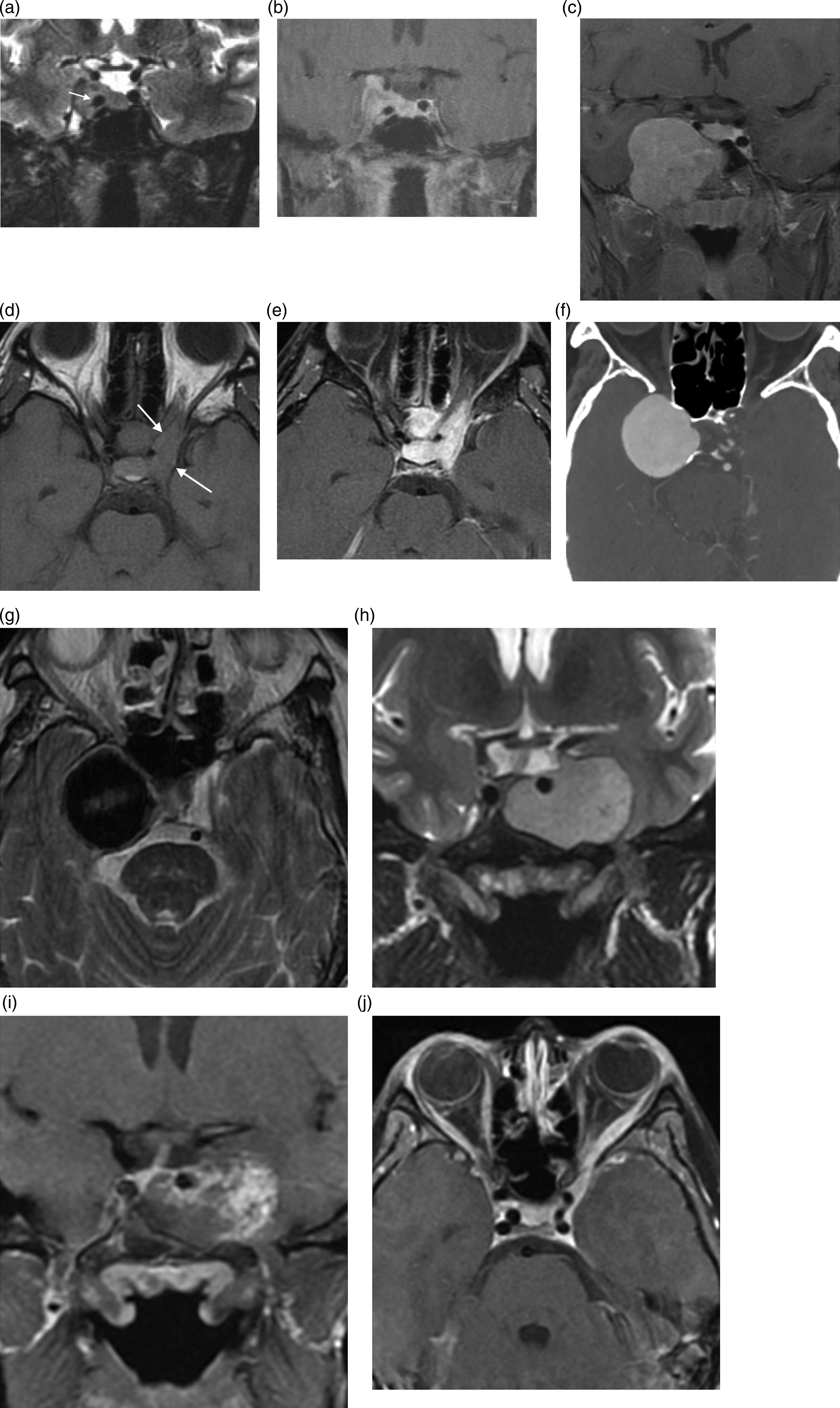
Metastasis. Systemic metastases or local extension of the head and neck cancer commonly involves central skull base and cavernous sinus. Breast and prostate cancer are the most common tumors to metastasize to the parasellar region. 37 Bone metastases demonstrate geographic marrow replacement on T1 and varying levels of diffusion restriction. Post-contrast fat saturation is helpful in delineating tumor margins.
Lymphoma. Parasellar lymphoma is rare and typically occurs in older adults. 38 Lymphoma can involve central skull base or cavernous sinus, and typically has pronounced diffusion restriction, which can offer a clue to the diagnosis. 39
Perineural Tumor. Primary head and neck mucosal and skin malignancies can extend to involve the cavernous sinus and skull base via perineural spread. 40 Perineural tumor spread is difficult to image; contrast-enhanced fat-supressed MR is superior to CT in the evaluation. 41
Schwannoma. Skull base and cavernous sinus schwannomas are rare benign slow-growing tumors. Trigeminal schwannoma accounts for 0.8–8% of intracranial schwannomas and typically occur in women between 38-40 years 42 In the parasellar region, most schwannomas originate from V1 and V2. 43 If V2 is involved at the skull base, the foramen rotundum classically demonstrates smooth, benign appearing expansion. 44 On CTA, schwannoma is seen as distinct from the carotid artery and the cavernous sinus is usually compressed and displaced medially, rather than infiltrated. 43 On MRI, schwannomas are well defined avidly enhancing lesions, T1 isointense, and T2 hyperintense (Figure 4(c)). 45
Langerhans Cell Histiocytosis. Parasellar involvement of LCH is included as examples (Figure 4(d) and (e)); otherwise imaging features are discussed in the “Sellar Space and Masses” section.
Cavernous sinus lesions - vascular
Aneurysm. Cavernous and parasellar aneurysms are not uncommon; general imaging features and diagnostic considerations are discussed in the “Sellar Space and Masses” section. Diagnosis in the cavernous sinus can be challenging in the setting of large, partially thrombosed aneurysms. Giant aneurysms can erode/remodel the skull base, and imaging is more complex due to altered intra-lesional flow, heterogenous T1/T2 signal, and partial enhancement related to peripheral thrombosis (Figure 4(f) and (g)). 46 CTA or transcatheter angiography may be necessary to establish the diagnosis and avoid potentially catastrophic biopsy consequences.
Carotid-Cavernous Fistula. Carotid-cavernous fistulas are usually a sequelae of trauma, and less frequently related to atherosclerotic ulceration or congenital intimal defects. 47 Useful MR findings include dilation of the ophthalmic vein and T2 flow channels related to arterialized venous flow, proptosis, and enlargement of the extra-ocular muscles. 48 Vascular flow within the cavernous sinus on non-contrast MRA is diagnostic of a fistula. 49 CTA may demonstrate asymmetric opacification of the expanded cavernous sinus with convex lateral wall. However, normal sized cavernous sinus with asymmetric enhancement on CTA is commonly seen and does not imply cavernous-carotid fistula, especially if other imaging or clinical findings are not present in a patient without history of significant trauma.
Cavernous Sinus Thrombosis. Cavernous sinus thrombosis is rare, least common among all dural venous sinus thromboses. 50 Dural venous sinus thrombosis is typically diagnosed in the early 3rd and 4th decade of life, and has a slight female predominance. 51 It typically presents with cranial neuropathy. Etiologies are usually secondary to systemic or adjacent inflammatory process (i.e., paranasal sinusitis, invasive fungal sinusitis), or external compression from bony trauma or tumor. 52 On CT, high-density bulk thrombus and cavernous sinus distention with filling defect on post-contrast imaging are typical. 53 Additional MRI findings include absent flow voids within the cavernous sinus and sinus expansion. If the thrombosis is related to tumor or adjacent infectious/inflammatory process, there should be some degree of enhancement within the thrombus.
Cavernous Sinus Hemangioma. Less than 1% of cavernous sinus masses are hemangiomas, typically in middle-age women. MRI findings include T1 hypointense, T2 hyperintense, and avid homogenous enhancement with gradual filling on dynamic imaging (Figure 4(h) and (i)). 54 Intraoperative blood loss results in high intraoperative mortality, approximately 12.5%. 55 Tagged red blood cell nuclear medicine imaging is also highly specific.
Cavernous sinus lesions - inflammatory
Tolosa-Hunt Syndrome. Tolosa-Hunt Syndrome is an idiopathic rare disease that involves cavernous sinus, with average age of onset 41 years and 1:1 gender ratio; pediatric cases are even rarer.18,56 Patients typically present with pain, and MRI demonstrates inflammatory change in the cavernous sinus extending to the orbital apex and T1/T2 iso-intensity with enhancement during active phase of disease (
Invasive Fungal Sinusitis. This is a life threatening rapidly progressive disease process that can involve cavernous sinus and skull base as an extension of the infection from the sinonasal cavity. 59 Complications include thrombosis of the cavernous sinus, vasculopathy, and thrombosis of the adjacent ICA.
Sarcoidosis. Discussed in the “Suprasellar Space and Masses” section.
Surgical approaches
Introduction
Surgical approaches for sellar and parasellar masses have drastically evolved since the first attempted bifrontal craniotomy approach for pituitary lesions. 60 Initial transcranial approaches by Sir Victor Horsley (1889)61,62 and Fedor Krause (1905) 63 were associated with significant morbidity due to frontal lobe retraction, prompting investigation of transsphenoidal approaches. In 1907, Hermann Schloffer 64 performed the first successful transsphenoidal approach and 3 years later Oskar Hirsh performed the approach without the disfiguring external rhinotomy incision.65-67 Halstead introduced the sublabial corridor 68 and Harvey Cushing continued to advance both transcranial and transsphenoidal approaches to the sella. 66 Even with improvements in mortality and cosmetic outcomes, early use of the transsphenoidal approach was limited by poor visualization, limited resection capabilities, and intraoperative complications.62,66,69,70
Early technological advances that improved the safety of the transsphenoidal approach included intraoperative fluoroscopy, which allowed for safe access into the sphenoid sinus,71,72 and the operative microscope, which significantly enhanced visualization and magnification.63,71 More recent advancements include high-resolution neuroimaging,73-75 surgical navigation, and high-definition endoscopy, all of which have further advanced the safety and efficacy of transsphenoidal approaches. As a result, the endoscopic endonasal approach is the most commonly used technique to access masses of the sellar, suprasellar, and parasellar regions.76,77
It is important to note, however, that endoscopic endonasal approaches have limitations. The endoscope requires mastery of specialized instruments and comfort working in a spatially limited region. 71 Lesions with significant lateral extension are inaccessible through this approach and endonasal surgery has higher risks of sinonasal morbidity and cerebrospinal fluid leak. Therefore, transcranial approaches are preferable for large extrasellar tumor extension, an inaccessible dural tail of a meningioma, and perhaps a dumbbell configuration of the tumor with an hourglass constriction at the level of the diaphragm sella.78,79 Additional indications for transcranial surgery include ectatic midline carotid arteries, co-existent aneurysm, 80 lateral cavernous sinus extension, 81 and indurated or very fibrous tumors.78,79,82
Therefore, the decision regarding endoscopic versus transcranial approaches depends on a variety of factors including lesion type, geometry and growth trajectory, risk profile, need for vascular control, patient preference, and surgeon comfort level, preference, and expertise. 81
Endoscopic endonasal approach
General background
Prior to performing EEA surgery, it is important to assess the anatomy of the target lesion, sella turcica, sphenoid sinus, and locations of the pituitary gland, optic chiasm, optic nerves, and carotid arteries. The sellar floor and sphenoid sinus are highly variable and should be carefully studied.81,83 Pre-operative assessment of the pituitary axis and visual function is standard. Intraoperative surgical navigation is invaluable and intraoperative imaging can be beneficial in particular skull base pathologies.84-88
The patient is placed in a semi-recumbent position to optimize venous outflow. The degree of head rotation and neck extension/flexion depends on the location and characteristics of the lesion. The nasal cavity is often prepped utilizing a nasal decongestant and aqueous antiseptic solution. The lateral thigh or abdomen is prepped for potential fat and/or fascial graft harvesting.
Transsphenoidal approach
The transsphenoidal EEA is often used to access lesions that primarily involve the sella turcica. The endoscope enters the nasal cavity and is navigated to identify the sphenoid ostium. A bilateral anterior sphenoidotomy is followed by a posterior nasal septectomy exposing the bony keel of the sphenoid rostrum. The bony rostrum and sphenoid sinus septations are removed to identify the sellar floor. The sellar floor is opened and exposed to span between the cavernous sinuses bilaterally and the superior and inferior intercavernous sinuses. The dura over the sella is incised and the sellar lesion is resected. Reconstruction is performed using a variety of possible techniques, including collagen grafts, fat and/or fascial grafts, structural repairs using bone, cartilage, or synthetic implants, and free or pedicled mucosal flaps.81,89 If a pedicled nasoseptal flap will be used, it must be prepared prior to the sphenoidotomy stage.81,90
Transsphenoidal EEA is the preferred surgical route for sellar and parasellar masses. 91 The widened surgical view allows for access to tumors with extension to the cavernous sinus and clivus.71,78 EEA should not be performed in patients with sinusitis until adequately treated. 79 A limited review demonstrated efficacy of EEA for sellar region tumors in an older (14–18 years) pediatric population, 92 but this approach may be limited in younger patients due to the narrow width of the piriform aperture and incomplete pneumatization of the sphenoid sinus prior to 10 years of age. 93
Transtuberculum/Transplanum approach
The TT/TP EEA is a rostral extension of the transsphenoidal EEA that provides access to the suprasellar space and prechiasmatic cistern. In addition to the bony resection of the sellar face, the tuberculum selle and posterior planum sphenoidale are also removed. 94 The optic canals serve as the lateral limits and the posterior ethmoidal arteries mark the anterior limits of this approach. 94 The dura is often incised at the midline to avoid injury to the optic nerves and supraclinoid carotid artery; the superior intercavernous sinus may need to be ligated. Suprasellar lesions are typically debulked prior to extracapsular dissection to allow for visualization of the following critical structures: optic nerves, supraclinoid carotid artery, superior hypophyseal artery, anterior cerebral artery complex, and the pituitary stalk.
Indications for the TT/TP EEA include suprasellar lesions such as tuberculum meningiomas, craniopharyngiomas, and select intrasellar lesions with significant suprasellar extension.94,95 The suprasellar region can be easily accessed via transcranial approaches as well (see below), and there are ongoing efforts to determine which lesions are best suited for the TT/TP EEA. For example, some have reported favorable outcomes using the TT/TP EEA for craniopharyngiomas96-99 and the transcranial approach may be superior for patients with planum and tuberculum meningiomas.100-102 Tumor characteristics, risk profile, patient preference, and surgeon experience often guide the choice of surgical approach to the suprasellar space. 103
Transclival approach
The transclival approach is a caudal extension of the transsphenoidal EEA that provides access to the prepontine and premedullary cisterns. The initial surgical approach is the same as the transsphenoidal approach, with the possible partial resection of the middle turbinates and elevation of a nasoseptal flap. Following sphenoid sinus exposure, the clivus is removed inferiorly towards the ventral foramen magnum. The extent of the bony resection depends on the size and location of the lesion and can be extended into the anterior arch of C1 and upper dens. 104 The dura is opened in the midline to avoid injury to the vertebral and basilar arteries as well as the abducens nerve at Dorello’s canals. After tumor removal, a fat graft and nasoseptal flap can be used to prevent post-operative CSF leak.
Common indications for the transclival approach include clival chordomas,105,106 petroclival meningiomas, 107 and chondrosarcomas. 108 This approach can also be used for odontoidectomy.109,110 Given the lateral exposure of this approach is limited by the eustachian tubes and parapharyngeal carotid arteries, this approach is best suited for midline infra- and retro-sellar, clival, and prepontine lesions. 106
Cranial approaches
General background
Transcranial approaches to the sella and parasellar regions are typically performed via anterior or anterolateral subfrontal corridors. These procedures differ from EEA in that the bony approach is through the convexity rather than the skull base and the initial intradural exposure is of brain tissue rather than lesion. Transcranial approaches require careful patient positioning to allow for gravity-assisted brain retraction and CSF drainage, the latter being achieved with opening of basal cisterns and/or placement of a lumbar drain.
Anterior approaches
Frontal craniotomy - subfrontal approach
The unilateral or bilateral subfrontal approaches were the earliest craniotomies used to access sellar lesions. The patient is placed in a supine position with the head extended and a bicoronal incision is made behind the hairline. A unilateral or bilateral frontal bone flap is elevated directly above or across the frontal sinus, based on surgeon preference (the latter requiring cranialization). The dura is opened in a low transverse fashion and the frontal lobes are gently retracted to allow for subfrontal access to the anterior skull base.
Common indications for the subfrontal approach include aneurysms, large suprasellar macroadenomas, olfactory groove meningiomas, tuberculum selle meningiomas, chiasmatic gliomas, and craniopharyngiomas. 81 An advantage of this approach is wide anatomic exposure; disadvantages include violation of the frontal sinuses and retraction injury to the frontal lobes.
Supraorbital craniotomy – subfrontal approach
The supraorbital craniotomy also allows for a subfrontal approach with a superior orbital rim osteotomy enhancing exposure and minimizing brain retraction. The patient is placed in a supine position with the neck extended. Head rotation is dependent on the characteristics of lesion. A similar bicoronal incision is performed, which stops at the contralateral superior temporal line. The supraorbital nerve is freed and a subfascial dissection mobilizes the temporalis muscle. A single burr hole is placed 1 cm behind the frontozygomatic suture and a bone cut is made from the lateral orbital rim above the zygoma traversing to the keyhole. A superior orbital roof osteotomy completes the bone flap removal. The dura is opened in a U-shaped fashion and frontal lobe elevation provides access to the optic nerve, carotid artery, and suprasellar region. An alternative incision is one made through the eyebrow or the upper eyelid crease followed by a minimally invasive “keyhole” craniotomy, which has been associated with improved cosmetic outcomes and patient satisfaction. 111
Common indications for this approach include large olfactory groove, planum sphenoidale, tuberculum sella, anterior clinoid process, and cavernous sinus meningiomas, pituitary adenomas, craniopharyngiomas, and vascular lesions.76,81,111 Importantly, posteriorly situated lesions with significant cranial extension may be difficult to access due to the limited vertical reach.
Anterolateral approaches
Pterional craniotomy
The pterional approach is a frontotemporal craniotomy surrounding the pterion. The patient’s head is elevated, extended, and rotated to position the malar eminence at the highest position. The scalp incision begins anterior to the tragus extending behind the hairline to cross the midline. The temporalis muscle can be elevated with the scalp or detached from the superior temporal line and reflected inferiorly as a separate flap. A “keyhole” burr hole is placed just behind the orbital rim, immediately superior to the frontozygomatic suture. 112 Additional burr holes often include one in the squamosa and one posteriorly below the superior temporal line. 112 A bone flap is raised, the sphenoid ridge is drilled flat, and additional bone is removed along the ridge to expose the superior orbital fissure. The dura is opened in a C-shaped fashion and reflected anteriorly. Opening the anterior limb of the sylvian fissure can facilitate retraction of the frontal and temporal lobes.
The pterional approach provides operative corridors in and around the suprasellar and paraclinoid spaces.113,114 An advantage of this approach is vascular control due to exposure of the proximal internal carotid artery. Common indications for the pterional approach include parasellar masses, lesions that extend into the cavernous sinus, parasellar lesions around the circle of Willis and optic apparatus, pituitary macroadenomas, and large intracranial meningiomas.81,115
Cranio-orbitozygomatic craniotomy
The cranio-orbitozygomatic (COZ) approach is a modification of the pterional approach with a superior and lateral orbital rim removal and zygomatic osteotomy. The head position and skin incision are the same. The temporalis fascia is reflected and subperiosteal dissection exposes the zygomatic arch and superior and lateral orbital rims. 116 The temporalis muscle is reflected inferiorly. Similar burr holes are placed, but additional osteotomies are made through the zygoma and orbital walls to elevate a single or two-piece bone flap. 117 In addition to the dural exposure, the COZ approach also exposes the periorbita and provides larger working angles.
Indications for COZ craniotomy include parasellar masses, interpeduncular fossa masses, and tumors with superior and/or laterally extension. 114 Additionally, this approach has been widely used for vascular and mass lesions in the cavernous sinus, paraclinoid, parasellar, interpeduncular, and upper paraclival regions.78,79
Footnotes
Author contribution
Bryan Lubomirsky, MD –
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.