
Abstract
Primary spinal cord high-grade gliomas, including those histologically identified as glioblastoma (GBM), are a rare entity in the pediatric population but should be considered in the differential diagnosis of intramedullary lesions. Pediatric spinal cord high-grade gliomas have an aggressive course with poor prognosis. The aim of this case report is to present a 15-year-old female adolescent with histopathologically confirmed spinal cord GBM with H3F3A K27 M mutation consistent with a diffuse midline glioma (DMG), H3 K27-altered, CNS WHO grade 4 with leptomeningeal seeding on initial presentation. As imaging features of H3 K27-altered DMGs are non-specific and may mimic more frequently encountered neoplastic diseases as well as demyelinating disorders, severe neurological deficits at presentation with short duration, rapid progression, and early leptomeningeal seeding should however raise the suspicion for a pediatric-type diffuse high-grade glioma like DMG, H3 K27-altered.
Keywords
Introduction
Glioblastoma (GBM) is a very rare entity in children.1–5 Compared to adults, less than 3% occur in the pediatric population. 1 Although high-grade gliomas (CNS WHO grade 3 and 4) are the most common class of central nervous system malignancies in pediatric patients, high-grade gliomas histologically defined as GBM account for only up to 4.6% of all primary pediatric tumors of the central nervous system.2–4 The vast majority of histologically confirmed pediatric GBMs are intracranial in location with only about 7% occurring in the spinal cord. 1 A subset of infiltrating gliomas in midline structures harbor mutations in histone H3-encoding genes which is diagnostic of a diffuse midline glioma (DMG), H3 K27-altered, CNS WHO 4. 6 Due to its rarity, there is still a limited though growing corpus of literature dealing with pediatric spinal cord DMG, H3 K27-altered.5,7–16 The aim of this case report is to present a 15-year-old female with histopathologically confirmed spinal cord GBM with molecular findings of H3F3A K27 M mutation consistent with a DMG, H3 K27-altered.
Case report
History
A 15-year old female presented with a 1 year history of pain in her left shoulder and 2-month history of worsening and new symptoms of weakness in the right arm and progressive inability to raise her right arm. In addition, significant neck pain, left sided dysesthesia, and mild numbness in parts of her right foot and hand were found. She was referred to our quaternary hospital for additional diagnostic work up and subsequent treatment of a spinal cord lesion found on neuroimaging in an outside hospital.
Neurological examination
On examination, the patient was found to have an intention tremor in her left hand and a tremor when attempting pronator drift testing. She had nearly full strength in the left arm. In the right arm, the deltoid and biceps muscle were scored 1/5 on the Medical Research Council scale of muscle strength, the triceps muscle: 4/5, the wrist extension: 3/5, the grip: 4+/5, and the hand intrinsic muscles: 4/5, respectively. In both legs, strength was normal. The biceps and triceps deep tendon reflexes were normal and symmetrical; the knee and angle jerk reflex were hyperactive without clonus on both sides. There was a dysesthetic feeling in the left hemibody.
Neuroimaging
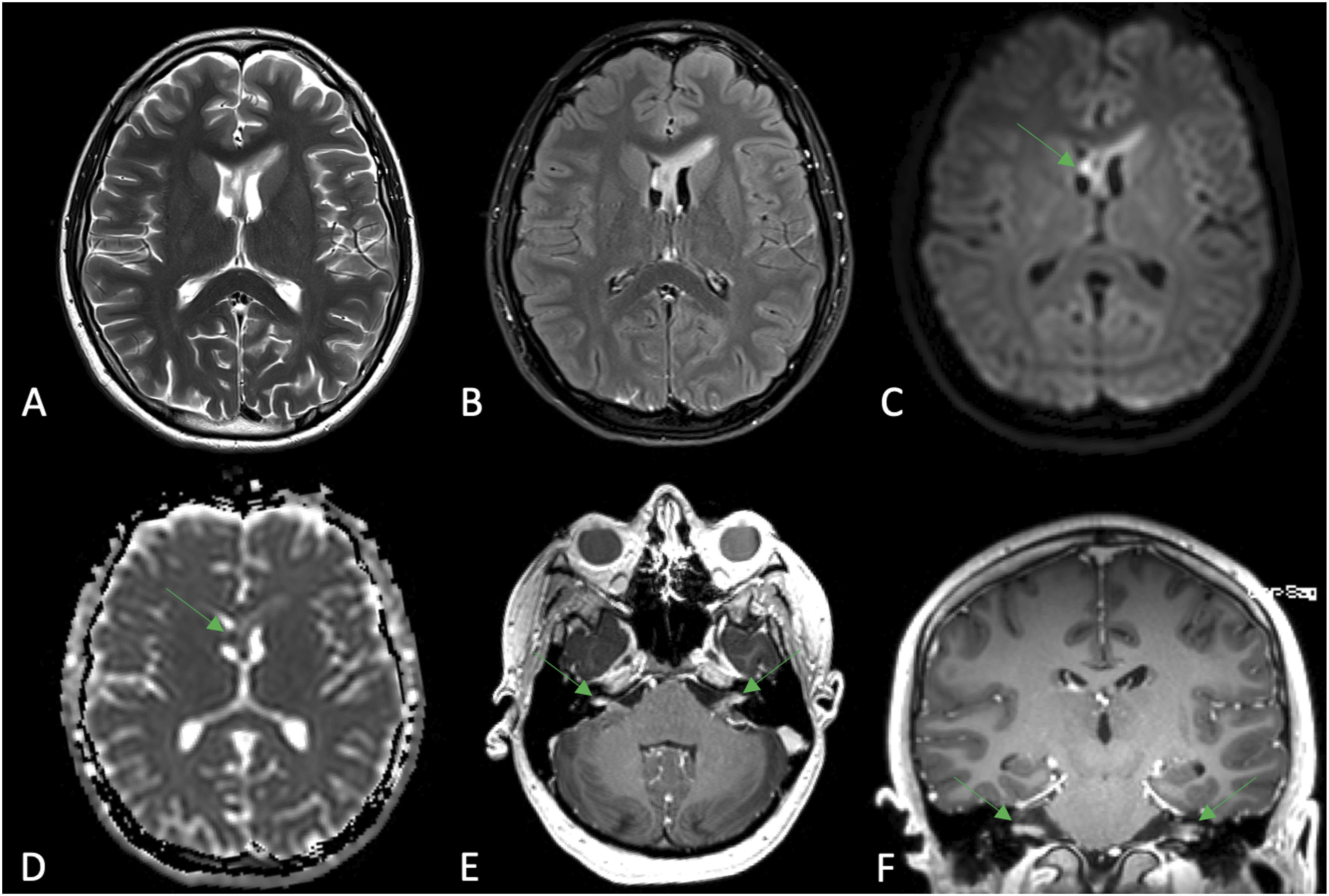
On spinal magnetic resonance imaging (MRI) (Figure 1), an approximately 1.6 × 0.8 × 5.5 cm (length × width × height) intramedullary mass lesion within the cervical spinal cord extending from the level of the base of the dens at C2 down to near the bottom of the C5 vertebral body was found. The lesion was T2W hyperintense and showed some ring contrast enhancement at the superior aspect of the lesion. On axial imaging, right side pronounced narrowing of the perimedullary cerebrospinal fluid space was found. In addition, a contrast enhancement along the surface of the entire spinal cord and the nerve roots of the cauda equine with slightly irregular appearance was noted. In conclusion, imaging was consistent with a neoplastic process within the cervical spinal cord with extensive leptomeningeal carcinomatosis. Brain MRI (Figure 2) showed extensive leptomeningeal spread with multiple focal T2W hyperintensities along the surface of the brain and ependymal surfaces of the ventricles. Some of the lesions showed abnormal fluid-attenuated inversion recovery signal, some showed diffusion restriction, and some showed focal contrast enhancement. Spinal cord diffuse midline glioma, H3 K27-altered with extensive leptomeningeal spread in a 15-year-old female adolescent. Sagittal (A) and axial (B) T2-weighted images showing an eccentric T2W hyperintense intramedullary mass centered in the right hemicord extending from C2 to C5. Sagittal (C) and axial (D) contrast enhanced T1-weighted images demonstrate focal ring-enhancement at the superior aspect of the lesion (arrow in C and D). Sagittal (E) and axial (F) contrast enhanced T1-weighted images show diffusely enhancing leptomeningeal carcinomatosis in both the ventral and dorsal aspect of the spinal cord including the conus medullaris (arrow in E and F). Additionally, clumping of the cauda equina nerve roots with abnormal enhancement at the L4 level (arrow in G and H) seen on sagittal (G) and axial (H) contrast enhanced T1-weighted imaging are demonstrated. Intracranial leptomeningeal dissemination of a spinal cord diffuse midline glioma, H3 K27-altered in a 15-year-old female adolescent. Axial T2-weighted (A) and axial fluid-attenuated inversion recovery (FLAIR; B) images demonstrating a T2W/FLAIR hyperintense mass involving the anterior column of the fornix and the genu of the corpus callosum (left greater than right) in conjunction with an adjacent intraventricular nodular lesion in the right frontal horn of the lateral ventricle without associated hydrocephalus. The nodular lesion in the right frontal horn demonstrates internal restricted diffusion with hyperintense signal on diffusion-weighted imaging (DWI; C) and corresponding low signal on apparent diffusion coefficient (ADC) map (arrows in C and D). Axial (E) and coronal (F) contrast enhanced T1-weighted images showing enhancing leptomeningeal carcinomatosis within both internal auditory canals (arrows in E and F).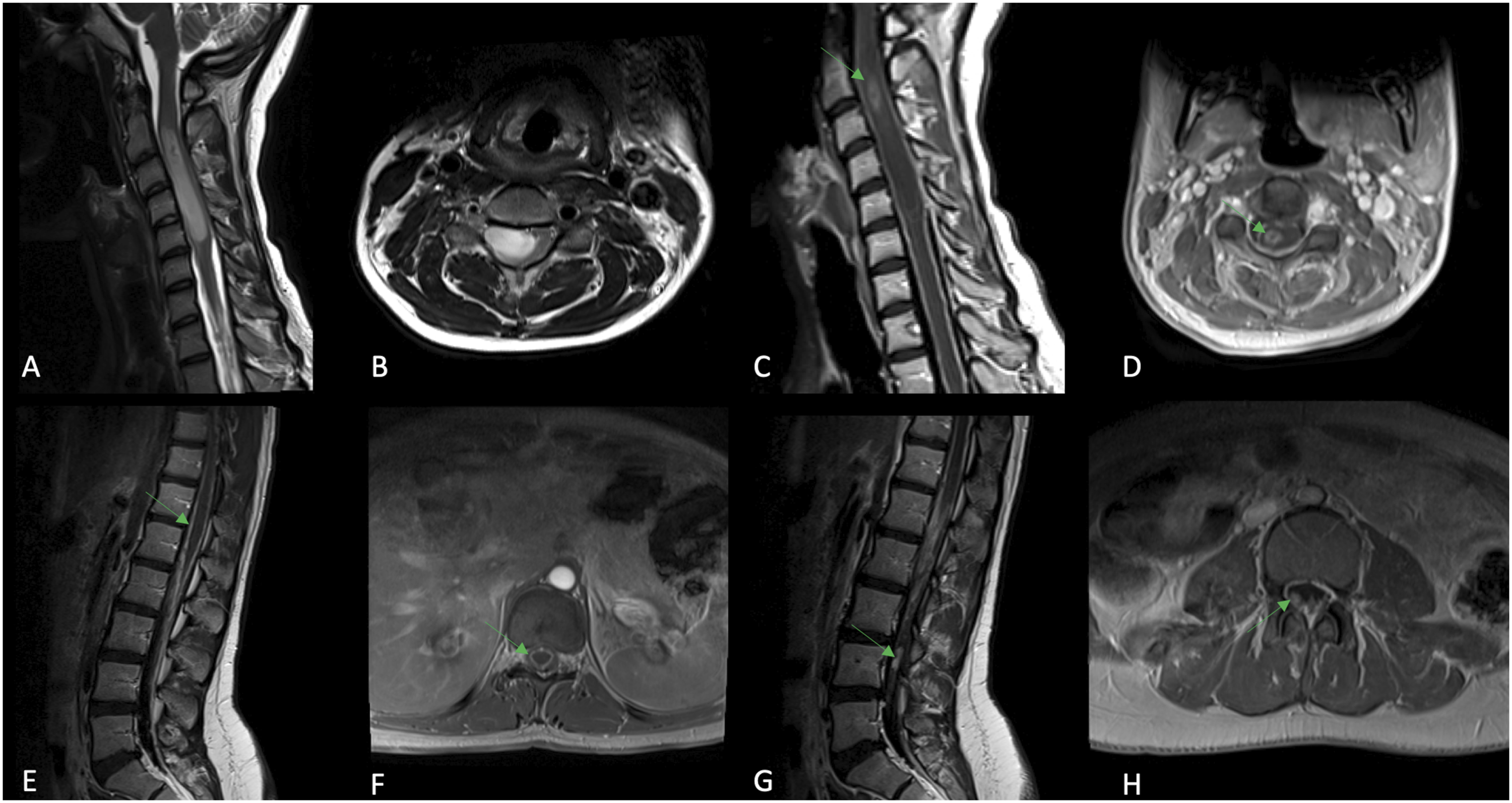
Operation and histopathology
Cervical 3–5 laminectomy was performed with the attempt to carry out a tumor resection. Due to swelling of the spinal cord and an ill-defined tissue plane between tumor and spinal cord, only a biopsy could be carried out (Figure 3). Histopathology showed a high-grade poorly differentiated neoplasm with predominant small blue cell features (Figure 4). The tumor showed florid anaplasia, moderate pleomorphism, endothelial proliferation, and frequent mitosis with elevated proliferation index of about 80%, as measured by Ki-67 positive count. Tumor cells were immunoreactive for GFAP consistent with astrocytic lineage. Tumor cells were negative for synaptophysin and showed retained nuclear staining for INI-1 (integrase interactor 1). Immunostain for p53 immunostain was strong and widely positive in about 70% of tumor cells consistent with a TP53 mutation. These histologic features were consistent with a histologic diagnosis of GBM, small cell subtype. Molecular analysis revealed an H3F3A K27 M mutation by pyrosequencing. These histologic and molecular features of this tumor are consistent with a DMG, H3 K27-altered, CNS WHO grade 4. MGMT (O-6-methylguanine-DNA methyltransferase) promoter was unmethylated. Intraoperative photographs demonstrating the procedure of tissue sampling. (A) After initial bone removal, the dura appears swollen and enlarged. (B) After initial dural opening, we see the spinal cord that is swollen with tumor and edema. (C) After mobilization of the spinal cord, the ventral lateral tumor is biopsied. Histologic sections show a high-grade poorly differentiated neoplasm with predominant small blue cell features with florid anaplasia, moderate pleomorphism, frequent mitosis, and endothelial proliferation (A and B). Tumor cells are immunoreactive for GFAP (C) and the Ki-67 proliferation index is elevated (D). Tumor cells show diffuse strong immunoreactivity for p53 (E).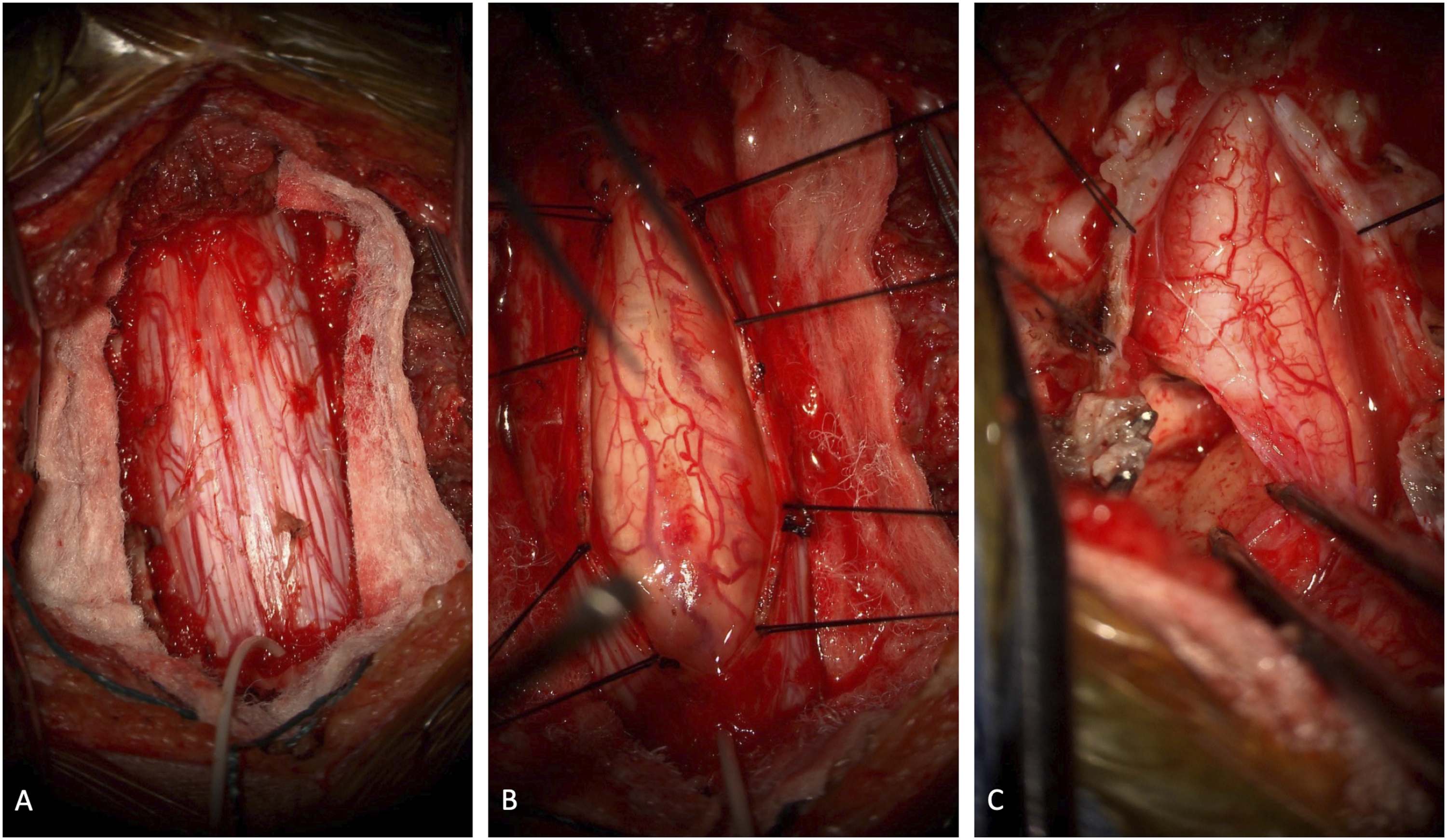

Therapy and outcome
The patient received craniospinal irradiation with proton therapy to a dose of 3960 cGy in 22 fractions. This was followed by a boost to 5400 cGy to the gross disease in the brain and boosts to 45 Gy to the gross disease in the cervical cord, thoracic cord, and cauda equina. Chemotherapy (temozolomide) was not administered. To date, there is no convincing data on the benefits of temozolomide in the management of pediatric high-grade gliomas. 17 She developed severe and worsening headaches with nausea and vomiting. Because of suspected elevated intracranial pressure, an external ventricular drain and subsequent ventriculoperitoneal shunt was placed. After shunt placement, she was able to be discharged from the hospital with significantly improved symptoms from hydrocephalus. She completed the planned course of proton therapy, but a general and neurological deterioration was noted and the therapy regimen was changed to palliative comfort care treatment.
Discussion
Spinal cord DMG, H3 K27-altered is a very rare entity in children.5,7–16 In the past decades, there have been several changes in the structuring and nomenclature of (pediatric) high-grade gliomas, reflecting the incorporation of molecular features and its advances into integrated tumor diagnoses with combined histopathological and molecular characteristics.6,18,19 Histologically GBMs are defined as malignant infiltrating astrocytomas with necrosis and/or microvascular proliferation. DMG may present as a high-grade glioma, including GBM, or they may have histological features of an infiltrating low-grade glioma. The presence of H3 K27 M mutation in an infiltrating glioma of a midline structure is graded as CNS WHO grade 4, regardless of histopathologic features. 20 DMGs, H3 K27-altered occur in midline structures (brainstem, thalamus, and spinal cord) with about 6–13% located within the spinal cord.7,8,15
Neuroimaging, especially MRI, plays an important role in narrowing the differential diagnosis. While DMGs, H2 K27-altered have highly variable imaging features,7,8 spinal cord GBMs, even though not specific, have been described as eccentrically located expansile T1W-hypointense and T2W-hyperintense intramedullary lesions with various degrees of irregular and poorly defined contrast enhancement.21,22 In the pediatric population, differential diagnosis includes the more frequently encountered neoplastic diseases such as low-grade diffuse astrocytoma, ganglioglioma, and ependymoma as well as spinal cord demyelinating disorders such as, for example, neuromyelitis optica, acute disseminated encephalomyelitis, or multiple sclerosis. A central location within the spinal cord, the presence of a cleavage plane, and a homogeneous enhancement are imaging features in favor of an ependymoma, while an eccentric location, ill-defined boarders, and patchy enhancement favor intramedullary astrocytomas. 22 However, since neuroimaging and symptoms may be non-specific, a biopsy or surgical sampling should be performed to provide the final diagnosis. 5
Pediatric spinal cord DMG, H3 K27-altered has an aggressive course with poor prognosis; median survival time is about 11 months. 15 To date, there is no consensus or standard of care treatment.10,23,24 The available treatment options include surgery (gross total resection or subtotal resection), (neo-)adjuvant radio- and/or chemotherapy or, if a resection is not possible, radio- and or chemotherapy.23,25
Like in our patient, the cervical spinal cord is most commonly involved in high-grade gliomas, followed by the thoracic spinal cord, cervicothoracic spinal cord, and conus medullaris. 23 Depending on the location, frequently reported presenting symptoms are extremity weakness, sensory disturbances, back pain, and bladder and bowel disturbances. 23
There is emerging evidence of the heterogeneity of high-grade gliomas with age-specific molecular and genetic subgroups.26–28 The H3F3A gene is among the genes encoding the histone protein H3. 27 The H3F3A K27 M mutation, as detected in our patient, is found in a subset of pediatric high-grade gliomas. 27 The presence of this mutation in a diffuse glioma occurring in a midline structure (e.g., brainstem, thalamus, and spinal cord) is consistent with a DMG, K27-altered, CNS WHO grade 4 6 and carries a dismal prognosis.9,10,12,16 In line with the literature, our patient did not exhibit IDH1 or IDH2 (isocitrate dehydrogenase enzyme 1 and 2) mutation. H3F3A K27 M mutation is mutually exclusive with IDH1/2 mutations which are found in a subset of primarily adult GBMs and are extremely rare in pediatric high-grade gliomas.27,28
Our patient presented with intracranial and spinal leptomeningeal dissemination. Leptomeningeal spread is a severe complication of high-grade gliomas including GBM and DMG, H3 K27-altered, and can be seen in up to 58% of high-grade gliomas of the spinal cord.26,29–31 The median survival from the time of leptomeningeal spread diagnosis to death is 3–4 months 32 Different risk factors such as age, gender, location, and molecular subtyping have been associated with a greater risk of leptomeningeal spread in patients with high-grade gliomas.5,26,32,33 Among these, young age, spinal cord location, H3F3A K27 M mutation and high Ki-67 proliferative index, were present in our patient.32,33 DMG, H3 K27-altered should especially be considered if leptomeningeal seeding is noted on initial presentation. 30 In general, leptomeningeal spread is rare in low-grade gliomas and extremely uncommon at tumor diagnosis.34–36
The MGMT promotor in our patient was unmethylated with a methylation rate of MGMT <20%. An unmethylated status is associated with an adverse prognosis as they seem to be less sensitive to the alkylating cytostatic drug temozolomide. 37 A better understanding of molecular and genetic subgroups of high-grade gliomas and their resulting prognostic and therapeutic features are the prerequisite for the development of targeted and more effective treatment strategies.
Conclusion
Diffuse midline glioma, H3 K27-altered, CNS WHO grade 4 is a very rare entity in the pediatric population but should be considered as differential diagnosis of intramedullary lesions.5,7–16 Imaging features are non-specific and may mimic more frequently encountered neoplastic diseases as well as spinal cord demyelinating disorders. The following conditions should however raise the suspicion for a high-grade glioma: severe neurological deficits at presentation with short duration and rapid progression and early leptomeningeal seeding. The current case is an example for a high-grade glioma histologically confirmed as GBM with H3F3A K27 M mutation consistent with a DMG, K27-altered, CNS WHO 4. Spinal cord DMGs, H3 K27-altered have a dismal prognosis.9,10,12,16 In recent years, there is a growing body of literature dealing with the considerable heterogeneity of high-grade gliomas with age-specific molecular and genetic differences.26–28 A better understanding of molecular and genetic subgroups of high-grade gliomas and their resulting prognostic and therapeutic features are the prerequisite for the development of targeted and more effective treatment strategies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All human studies in this paper are retrospective reviews and approved by the Baylor College of Medicine Institutional Review Board under IRB protocol H-40,231. Informed consent was waived for this purely retrospective manuscript.