
Abstract
The severe acute respiratory syndrome coronavirus disease 2019 (COVID-19) pandemic, became rapidly recognised by variable phonotypic expressions that involve most major body organs. Neurological complications of severe acute respiratory syndrome coronavirus disease are increasingly encountered in patients with COVID-19 infection, more frequently in patients with severe infection, and develop as a consequence of the neurotropic potential of this virus, secondary cytokine storm and acquired syndrome of COVID-19 coagulopathy. Spinal cord involvement after COVID-19 more commonly includes infectious transverse myelitis, para and post infection myelopathy and, rarely, spinal cord ischaemia related to increased coagulopathy with thromboembolic consequences. We herein report a COVID-19-positive patient with increased coagulopathy and vertebral artery thrombosis leading to posterior circulation and subsequent spinal cord infarction.
Keywords
Introduction
Acute spinal cord ischaemia syndrome (ASCIS) is rare, accounting for approximately equal to 5–8% of all acute myelopathies and 1–2% of all vascular neurological pathologies. 1
In the study of Nedeltchev et al., in their cohort of patients the most prevalent origin of ASCIS was atherosclerosis (33.3%), followed by aortic pathologies with or without surgery (15.8%) and degenerative spine disease (15.8%). Cardiac embolism, systemic hypotension and epidural anaesthesia were rare causes of spinal cord ischaemia, and in 17 patients (28%), the cause remained unclear. 1
Other rare causes of ASCIS include trauma, intervertebral disc fibrocartilaginous embolism, decompression sickness from scuba diving, coagulopathy, haematological disorders (e.g. sickle cell disease), spinal arteriovenous malformations, vasculopathy (radiation-induced vasculopathy, cocaine) and procedure related (spinal anaesthesia, sympathectomy, esophagectomy).2,3
Different patterns of neurological impairment of ASCIS with much variability in description are presented in the literature. The majority of patients develop abrupt symptomatology within 12 hours in more than 50% of patients and within 72 hours for the vast majority of patients, 2 and can sometimes be preceded by transient ischaemic attacks often of the same neurological distribution. 3
Common clinical presentations include: anterior spinal artery (ASA) infarct (bilateral motor deficit with spinothalamic sensory deficit below the level of involvement), anterior unilateral infarct/pseudopoliomyelitic form (hemiparesis with contralateral spinothalamic sensory deficit), posterior spinal artery infarct (bilateral motor and lemniscal sensory deficit), posterior unilateral infarct (hemiparesis with homolateral lemniscal sensory deficit), central infarct often with cardiac arrest or prolonged hypotension (bilateral spinothalamic sensory deficit without motor deficit) and transverse infarct, often embolic (bilateral motor and complete/all modality sensory deficit). Less common presentations include: man-in-the-barrel syndrome (painful bilateral brachial diplegia) with cervical central spinal cord infarct, progressive distal amyotrophy due to chronic lesions of the anterior horns, sulcal artery syndrome (partial Brown–Séquard syndrome) and cauda equina syndrome due to infarction at the level of the conus medullaris.2,3
The gold standard in imaging of the spinal cord is magnetic resonance imaging (MRI) because of its capability to confirm the diagnosis and exclude other causes of acute myelopathy and cord impairment due to compression. The hallmark of spinal cord infarction on MRI is the presence of an intramedullary increase in the T2-weighted imaging signal, the pattern of which will depend on the territory affected, cord swelling and diffusion-weighted imaging (DWI) diffusion restriction in the acute phase.2,3
The severe acute respiratory syndrome coronavirus disease 2019 (COVID-19) pandemic became rapidly recognised by widely variable phonotypic expressions that involve most major organs, and are commonly associated with the acquired syndrome of COVID-19 coagulopathy involving venous, arterial and microcirculatory systems, distinct from other viral illnesses, and more commonly encountered in critically ill patients with acute respiratory distress syndrome (ARDS) and intensive care unit admission. 4
Case report
We report the case of a 41-year-old male patient, with an unremarkable past medical history, who presented to the emergency department with fever, vomiting, dizziness, headache and right-sided weakness. Urgent computed tomography (CT) of the brain (not shown) was performed and showed right cerebellar and right-sided medulla oblongata ill-defined hypodensity, suggestive of acute right posterior circulation stroke which was further confirmed by magnetic resonance imaging (MRI) of the brain performed on the same day with corresponding restricted diffusion on diffusion-weighted sequence (DWI) and high signal on fluid-attenuated inversion recovery (FLAIR)-T2 sequence, and occlusion of the distal right vertebral artery (VA) (Figure 1) on three-dimensional time of flight cranial magnetic resonance angiography (MRA). On admission he had moderate respiratory symptoms, with 95% oxygen saturation, his chest X-ray showed patchy areas of pneumonic consolidations, and his COVID-19 polymerase chain reaction tested positive. Since then the patient was started on hydroxychloroquine, aspirin, clopidogrel, esomeprazole and subcutaneous enoxaparin.
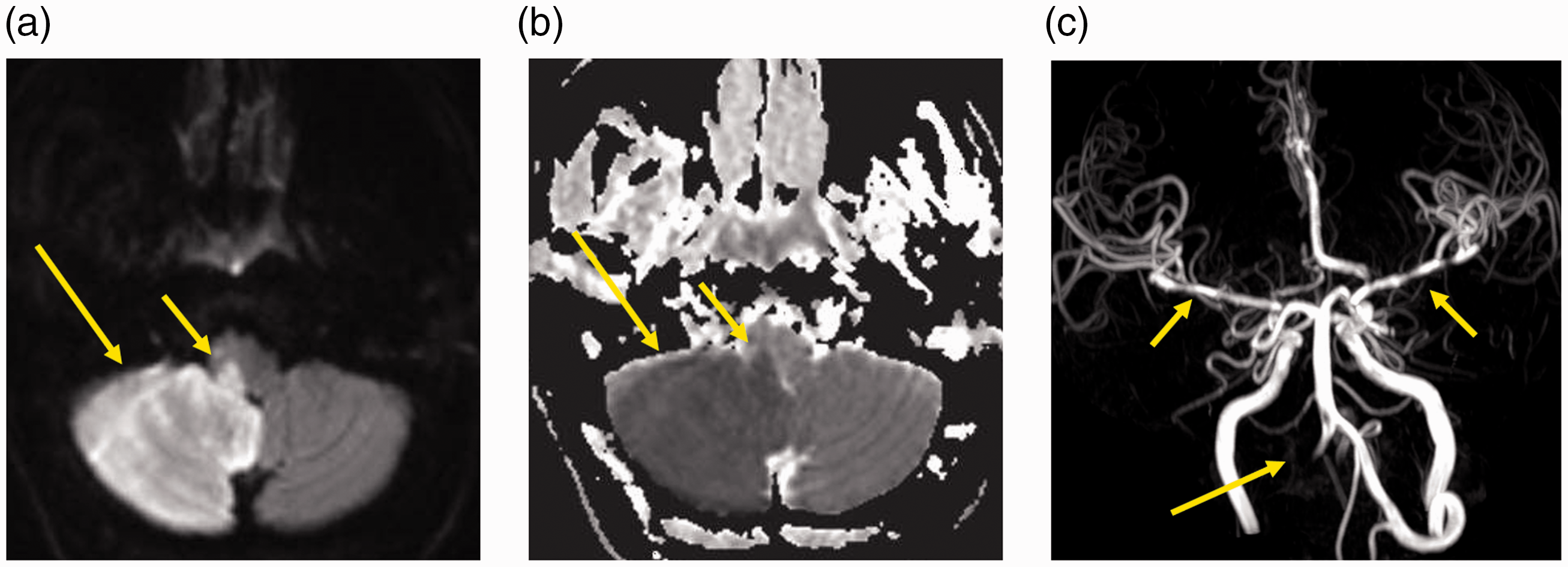
(a) Axial diffusion-weighted imaging b 1000 showing diffuse right cerebellar and right lateral medulla oblongata bright signal intensity (SI); and (b) Corresponding ADC map low SI (long and short arrows, respectively) denoting diffusion restriction due to recent subacute right-sided posterior circulation stroke; (c) Cranial magnetic resonance angiography showing complete occlusion of the intracranial segment of the right vertebral artery with retrograde flow from the contralateral side filling its distal aspect, note bilateral middle cerebral arteries mural irregularities (long and short arrows, respectively). b value: degree of diffusion weighted image applied; ADC: Apparent diffusion coefficient.
On the following day his oxygen saturation dropped further to less than 90% and he was intubated. Five days later he developed weakness in all four limbs lower more than upper. MRI of the spinal cord showed increased T2 signal intensity on T2-weighted imaging and diffusion restriction on DWI at the cervical and dorsal levels consistent with spinal cord infarcts (Figure 2). A few days later he progressed to ARDS and had tracheostomy for airway protection. One week later he started to improve; he became stable after 3 weeks and was transferred to a rehabilitation unit. To our knowledge this is the first reported case of spinal cord ischaemia in a COVID-19-positive patient.
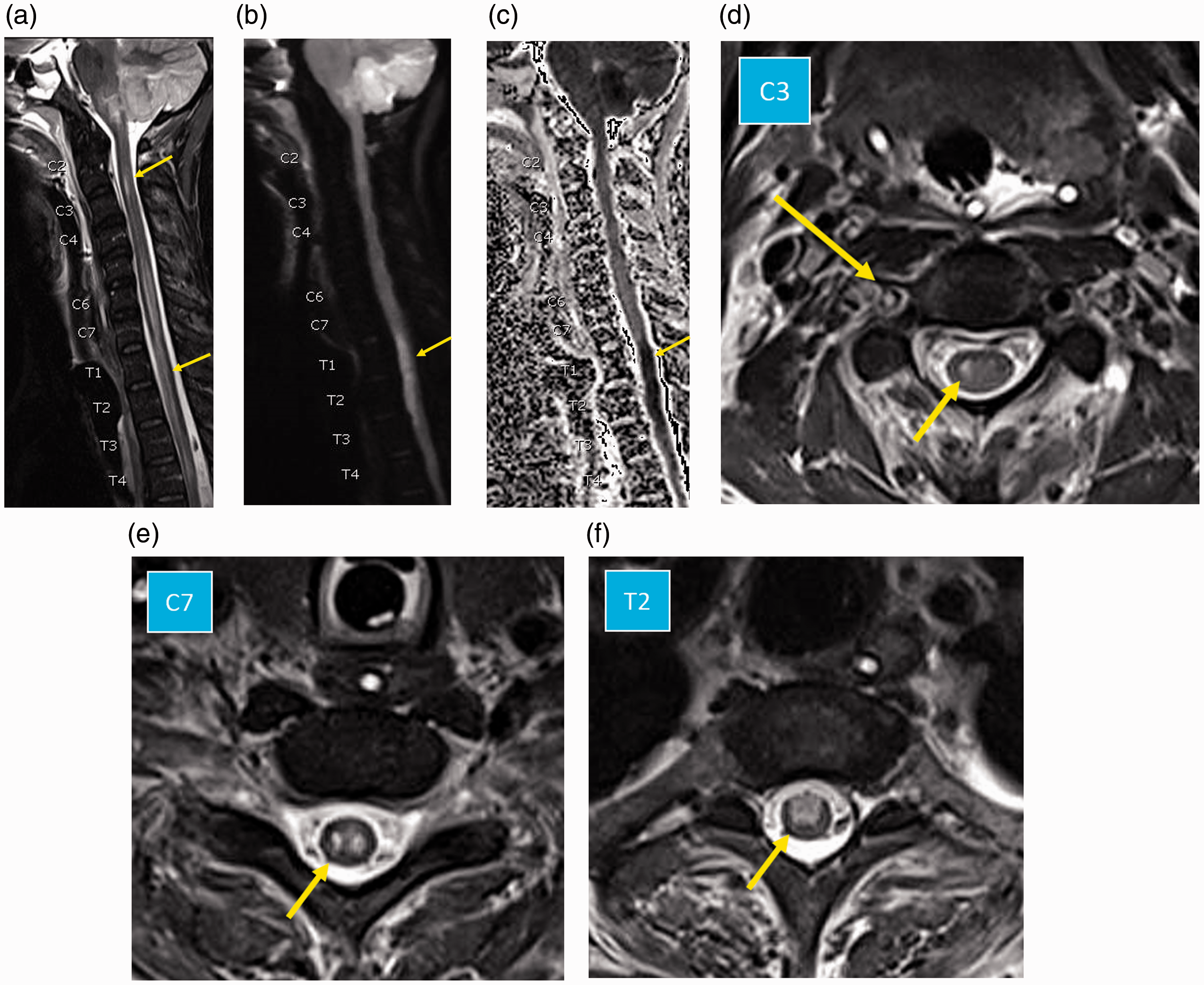
Sagittal magnetic resonance imaging (MRI) of the spinal cord; (a) T2-weighted imaging showing diffuse intermediary bright signal intensity and mild swelling involving cervical and upper dorsal levels of the spinal cord; (b) diffusion-weighted imaging (DWI) b 800; and (c) ADC map showing spinal cord recent ischaemic changes (diffusion restriction) with intramedullary bright and low signal intensity, respectively, involving dorsal D1 to D3 levels (arrows in (a), (b) and (c)). Axial MRI of the spinal cord at the C2 cervical level (d); lower cervical C6 level (e); and upper dorsal T2 level (f); showing variable ischaemic changes at these levels, with unilateral involvement of right anterior deep grey matter at C2, ‘owl eye’ appearance due to symmetric involvement of deep grey matter at C6, and more diffuse involvement of central grey matter and anterior white matter at the T2 level (arrows in (d), (e) and (f)), note loss of signal void in thrombosed right vertebral artery in the right transverse foramen (long arrow in (e)). b value: degree of diffusion weighted image applied; ADC: Apparent diffusion coefficient.
Discussion
The typical vascular supply of the spinal cord is by the midline ASA and two paramedian posterior spinal arteries (PSAs), these arteries originate from the intracranial (V4) segment of the VA and extend down to the level of the conus. These arteries are typically not longitudinally continuous structures but rather a longitudinal network of arterial structures that are reinforced by radicular arteries at multiple levels.3,5
Our index case demonstrates lower cervical and upper thoracic spinal cord infarction following thrombosis of the intracranial V4 segment of the VA with posterior circulation stroke, followed a few days later by extension of thrombosis more proximally to involve the V3 and V2 cervical segments of the VA. VA artery occlusion implicated in spinal cord infarction is often due to dissection, whereas VA thrombosis due to a hypercoagulable state is a rare recognised cause of spinal cord infarction. 5
Etgen and Höcherl reported a case of cervical spinal cord ischaemia associated with extracranial VA thrombosis which was treated by repeated thrombolysis. 6 Suzuki et al. reported cervical cord infarction caused by dissection of the intracranial V4 segment of the VA. 7 Hsu et al. 8 described a patient with combined brain and spinal cord infarction following VA dissection. The authors also performed a systematic review of published reports on this topic and found that the most common regions affected were at the V1 or proximal V2 segments, and spinal cord infarction occurred most often at the C2 spinal level (65%), followed by the C3–C5 levels (41–59%) and C6–T3 levels (12–24%), and the vascular territory involved was the PSA in 29% of patients, spinal sulcal artery in 42% and ASA in 29%, moreover 29% had additional brain posterior circulation infarcts. 8
VA occlusion involving the V1 segment can also result in haemodynamic/watershed ischaemic changes at the upper thoracic (T1–T4) region which represents a crossover of two regions of two radicular arterial supply, as was encountered in our case. 9
MRI is the imaging modality of choice for ASCIS; it can show T2 hyperintensities with associated spinal cord cytotoxic oedema, these T2-weighted imaging changes, however, can take hours to days to develop and its sensitivity is therefore low in the acute setting. Conversely, recent advances in DWI techniques of the spine applying a reduced field of view and high spatial resolution, combined with distortion reduction techniques and homogeneous fat saturation allowed the identification of acute ischaemic changes as a diffusion restriction-related signal in the small-sized spinal cord.2,10
As in our index case, involvement of the ASA represents the majority of cases where the anterior and central portions of the spinal cord are involved, most frequently bilaterally. In many instances, however, the anterior horn cells are primarily involved resulting in pencil-like T2-weighted imaging hyperintensities extending over multiple spinal levels on sagittal images and two bright dots – the ‘owl eye’ appearance on axial images. Central involvement can be more extensive, involving not only the grey matter but also the deep white matter, sparing only a thin rim of surrounding peripheral white matter, and sometimes unilateral patterns can also be encountered (Figure 2(e), (d) and (f)). Moreover, it is also possible to have unclassifiable patterns which can be related to ischaemic changes involving cross territories of several spinal arteries.2,3,11
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.