
Abstract
Purpose
Cartilage cap resurfacing is a method to seal a superior semicircular canal dehiscence. The purpose of this study was to evaluate the detection of new bone formation after surgical placement of a cartilage cap over a dehiscent semicircular canal.
Methods
In this retrospective review, two neuroradiologists blinded to each other’s interpretation reviewed the temporal bones of 20 patients, five of which had a pre-operative computed tomography (CT) exam which was interpreted as unilateral superior semicircular canal dehiscence and with new bone formation following repair on follow-up CT. There were also 15 control subjects. Each neuroradiologist was blinded to history, including post-operative changes, and asked to determine if there was a dehiscence or no dehiscence.
Results
Out of the 15 controls, there was 100% inter-observer agreement. On the five post-operative patients, there was agreement in 4/5 that there was no dehiscence post-operatively and 1/5 agreement of dehiscence post-operatively, but ectopic bone adjacent to the dehiscence.
Conclusion
Our results indicate that new bone formation can be seen at the site of cartilage cap placement over the dehiscence and be interpreted as bony closure of the dehiscence.
Introduction
A syndrome of vestibular symptoms induced by sound or by changes in middle ear or intracranial pressure due to superior semicircular canal dehiscence (SSCD) was first described in 1998. 1 Classically, patients with SSCD present with Tullio phenomenon—vestibular symptoms such as vertigo, imbalance, and oscillopsia induced by loud sounds. Patients may also present with conductive hearing loss, autophony, pulsatile tinnitus, and hyperacusis. 2 Most symptomatic patients with SSCD can be treated conservatively. Those with debilitating symptoms may be considered for surgery. Plugging of the dehiscence involves placing fascia, bone wax, or bone dust into the lumen of the superior semicircular canal, thereby closing the canal, but can leave the patient with significant disequilibrium. On the other hand, conchal or tragal cartilage cap resurfacing seals the defect and preserves, anatomically and functionally, the superior semicircular canal.2,3
Most patients have significant improvement or resolution of symptoms after cartilage cap placement surgery and no further imaging is necessary. 3 Clinical concern for rare complications such as fistula or pneumolabyrinth may prompt computed tomography (CT) evaluation. Also, patients with bilateral SSCD are sometimes imaged after surgery on one side, to follow progression of the contralateral side, thus providing an opportunity to visualize the cartilage cap side. The purpose of this study is to assess radiographic evidence of new bone formation after surgical placement of a cartilage cap over a dehiscent semicircular canal.
Methods
This retrospective study was approved by the institutional review board. We used 5 subjects whose pre-operative CT temporal bone exam was interpreted as unilateral SSCD and with new bone formation following repair on follow-up CT (3 males and 2 females, ranging from 38 to 79 years old, 3 with tragal source cartilage and 2 with conchal source cartilage); both the pre-operative and post-operative images were to be reviewed by the neuroradiologists. For our control set, we obtained 15 subjects with temporal bone CT exams—12 with no SSCD, 2 with bilateral SSCD, and 1 with bilateral SSCD and surgery on one side (4 males and 11 females, ranging from 16 to 78 years old). These CT exams were obtained on Siemens helical CT scanners (Sensation, Definition Edge, Definition Flash) using a 16 × 0.6 mm, U30 ultrahigh resolution kernel. Individual right and left reformats were created as follows: axial and coronal, 1.0 × 0.5 mm, parallel and perpendicular to the superior semicircular canal, 0.8 × 0.2 mm, and display field of view 18 cm. All images were of adequate and similar quality for review, confirmed by our physicists.
Next, we deidentified images of the bilateral otic capsules, perpendicular and parallel to the superior semicircular canal for each of the 20 subjects for a total of 80 sets. Each set of images was cropped using Analyze 12.0 (Biomedical Imaging Resource, Mayo Clinic, Rochester, MN), and visualization and analysis software for medical imaging, to eliminate evidence of prior surgery.
Two fellowship trained neuroradiologists with certificate of added qualification (CAQ) in neuroradiology, one 14 years post-fellowship and the other 13 years post-fellowship were blinded to each other’s interpretation and independently reviewed all 80 sets. Each neuroradiologist was asked to draw conclusions, as if reading in real time, and indicate if there was a dehiscence or no dehiscence. Interpretations were then compared for inter-observer agreement.
Results
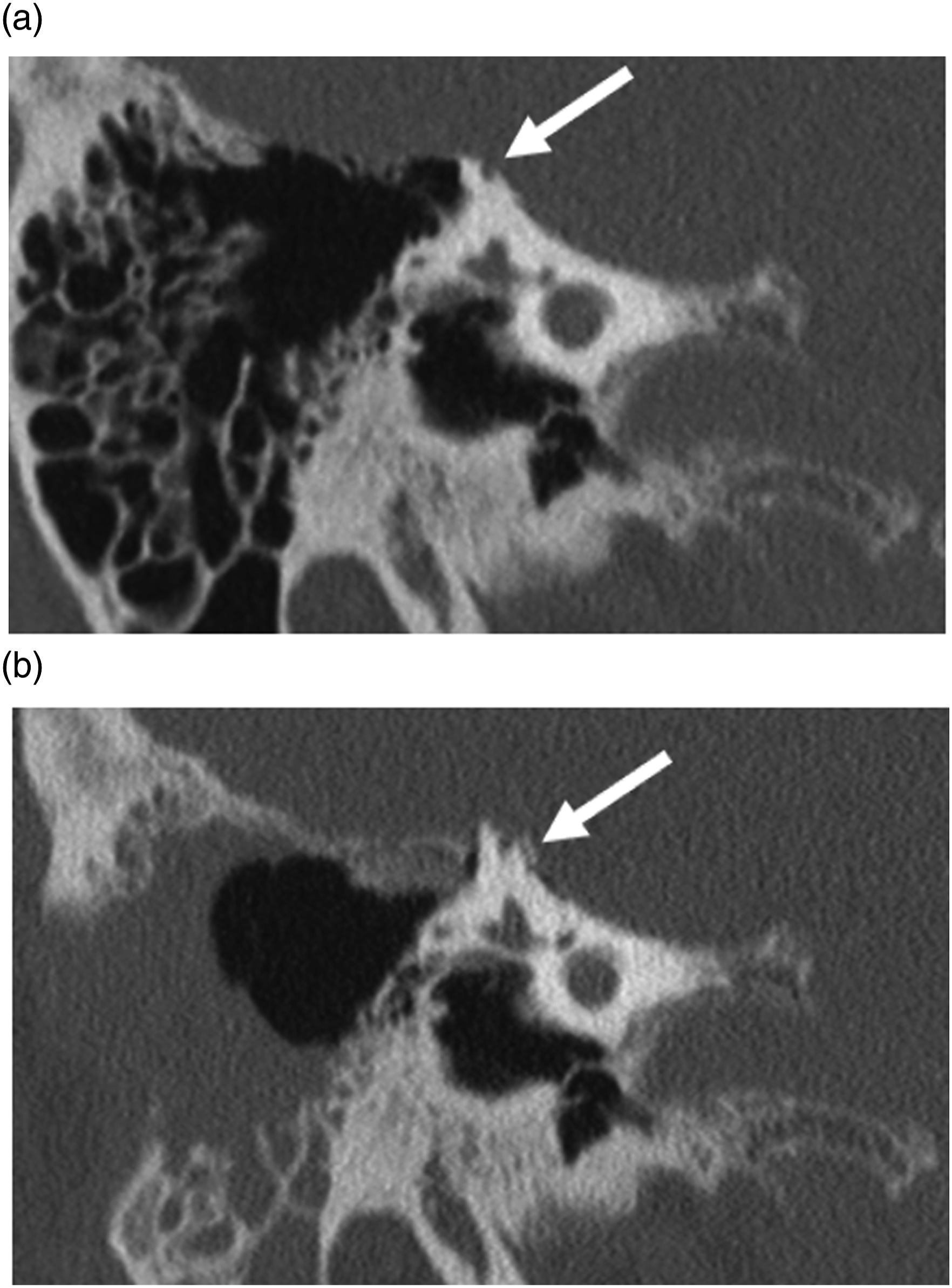
There was 100% inter-observer agreement in the 15 control subjects, both sides. In the five post-operative patients, all had their pre-operative CT read as dehiscence, and agreement in 4/5 cases that no dehiscence was present post-operatively (example given in Figure 1). The remaining 1 case had agreement there was dehiscence post-operatively, but ectopic bone adjacent to the dehiscence (Figure 2). Average months post-operatively that bone formation was seen was 30 months, and as early as 20 months. 63-year-old male with superior semicircular canal dehiscence (a). Follow-up imaging approximately 38 months after cartilage cap resurfacing surgery demonstrates osseous coverage of the dehiscence (b). 38-year-old female with dehiscence of the superior semicircular canal (a). Follow-up imaging approximately 20 months after cartilage resurfacing surgery demonstrates new bone formation adjacent to the dehiscence (b).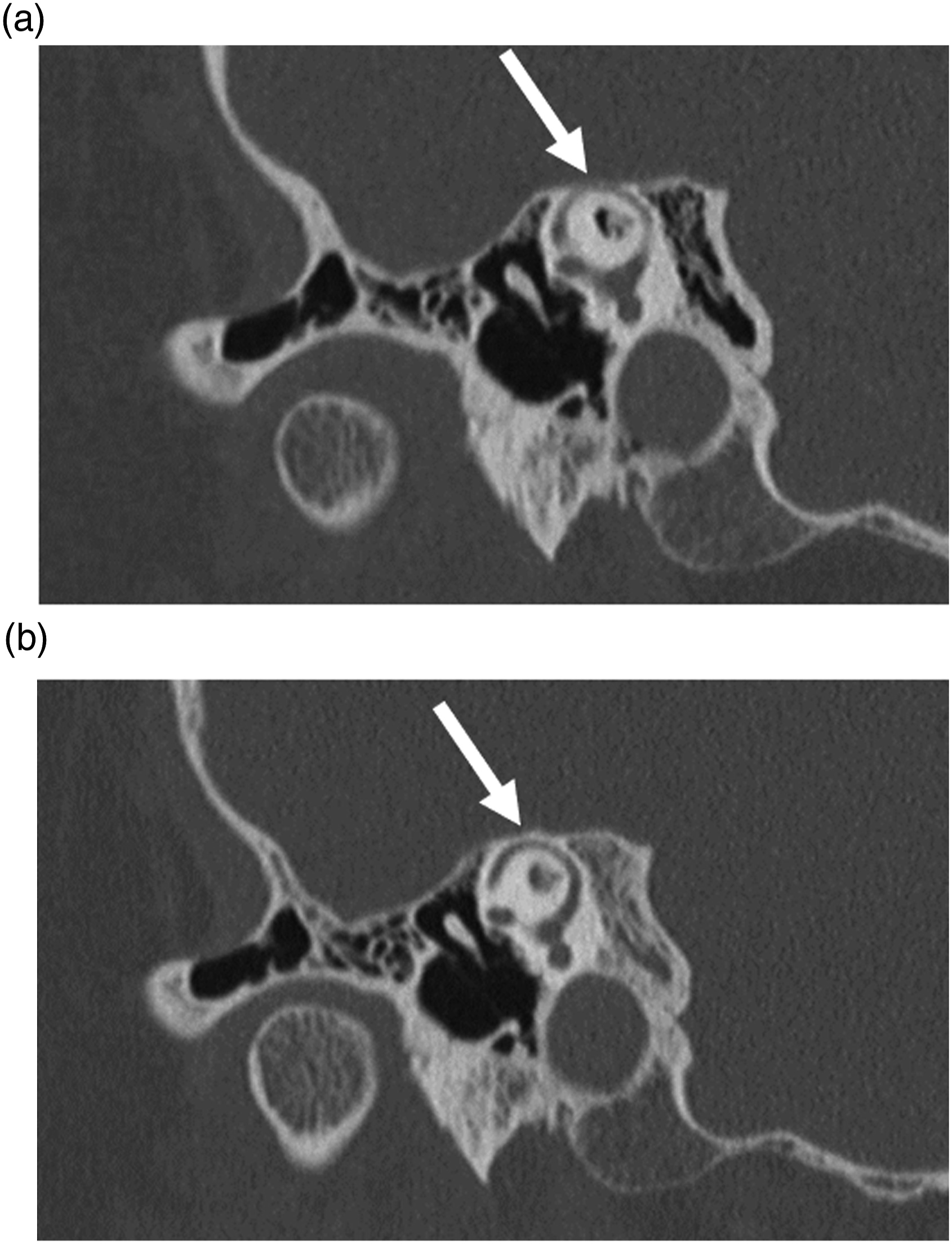
Discussion
Most patients with SSCD can be conservatively treated. Surgery can be considered for patients that have debilitating symptoms such as primary sound-induced vertigo and chronic severe disequilibrium. There are two primary surgery options: plugging and resurfacing. Plugging involves placing fascia, bone wax, or bone dust into the lumen of the superior semicircular canal at the dehiscence, thereby closing the dehiscence and preventing abnormal transmission of sound energy. However, normal function of the semicircular canal is sacrificed, and patients may have persistent disequilibrium. The second surgery option, which is used at our institution, is resurfacing of the dehiscence without plugging using conchal or tragal cartilage, which conforms to the undulating surface of the floor of the middle cranial fossa and does not block or plug the lumen of the canal. This latter method seals the defect and preserves the physiologic function of the semicircular canal.2,3
Most patients have significant improvement or resolution of symptoms after cartilage cap placement surgery and therefore, undergo no further imaging. As a result, very little is reported in literature about the post-operative appearance of SSCD resurfacing and is an inherent limitation of this study; clinical concern for rare complications such as fistula or pneumolabyrinth may prompt CT examination. Our study demonstrates that new bone formation can be seen at the site of cartilage cap placement over the dehiscence, as early as 20 months post-operatively, and be interpreted as bony closure of the dehiscence. One of our patients showed ectopic bone adjacent to the dehiscence, suggesting the beginnings of complete osseous coverage.
The mechanism of bone formation and if the cartilage itself ossifies or provides a scaffold for new bone growth is unclear.4,5 Many patients do not have osseous coverage (1 used in our control data set) and symptoms have resolved. Therefore, it is important to remember the absence of bone formation does not imply failure of surgery. Expected lag time for development of osseous coverage over the dehiscence has yet to be elucidated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.