
Abstract
Objective
The aetiologic diagnosis of non-traumatic acute myelopathies (AMs), and their differentiation from other mimicking conditions (i.e. ‘mimics’), are clinically challenging, especially in the emergency setting. Here, we sought to identify: (i) red flags suggesting diagnoses alternative to AMs and (ii) clinical signs and magnetic resonance imaging (MRI) features differentiating non-compressive from compressive AMs.
Materials and methods
We retrospectively retrieved MRI scans of spinal cord dictated at emergency room from January 2016 to December 2020 in the suspicion of AMs. Patients with traumatic myelopathies and those with subacute/chronic myelopathies (i.e. MRI scans acquired >48 h from symptom onset) were excluded from analysis.
Results
Our search retrieved 105 patients; after excluding 16 cases of traumatic myelopathies and 14 cases of subacute/chronic myelopathies, we identified 30 cases with non-compressive AMs, 30 cases with compressive AMs and 15 mimics. The presence of pyramidal signs (p = 0.012) and/or pain (p = 0.048) correctly identified 88% of cases with AMs. We failed to identify clinical indicators for distinguishing non-compressive and compressive AMs, although cases with inflammatory AMs were younger than cases with all the remaining conditions (p < 0.05). Different MRI patterns could be described according to the final diagnosis: among non-compressive AMs, inflammatory lesions were more often posterior or central; vascular malformation had a fairly widespread distribution; spine ischaemia was more often central. Anterior or lateral compression were more often associated with neoplasms and disc herniation , whereas hemorrhages and infections produced spine compression on all sides.
Conclusion
We propose a simple clinical indicator (i.e. pyramidal signs and/or pain) to distinguish AMs from their mimics in an emergency setting. Urgent spinal cord MRI remains essential to discriminate compressive and non-compressive aetiologies.
Introduction
Non-traumatic acute myelopathy (AM) refers to any pathologic process that involves the spinal cord with a sudden or rapid onset that worsens within hours or days.1,2
Incidence rates of AMs range from 1 to 11 cases per million population per year in European countries, with degenerative, inflammatory, neoplastic conditions more frequent than infections as compared with developing countries. 3 Timely recognition of an AM and its differentiation from other mimicking conditions bears relevant therapeutic and prognostic implications,4,5 but it is clinically challenging,6,7 especially in the emergency setting. 8 The first difficulty is to distinguish an AM from other neurological syndromes, and secondly to identify the correct aetiology.
Difficulty in diagnosis of AM (the so-called chameleons) arises with atypical or non-specific symptoms, especially in case of incomplete spinal cord syndrome and/or in the early stage of a spinal cord damage, when the spinal shock obfuscates upper motor neuron signs.9,10 The so-called mimics are non-myelopathic or even non-neurological conditions mimicking AMs because of real or apparent symptoms and clinical signs that wrongly suggest spinal cord involvement. 10
Magnetic resonance imaging (MRI) is the gold standard for spinal cord imaging as it allows accurate visualization of neural elements, demonstration of soft tissue pathology and discrimination between intrinsic and extrinsic spinal cord diseases.11,12
Here we sought to retrospectively correlate the early clinical and MRI features with the final diagnosis of patients admitted to a first-level emergency room (ER) for a suspected non-traumatic AM. We aimed at exploring: (1) the frequency of mimics in the emergency setting; (2) red flags suggesting diagnoses alternative to AMs and (3) clinical signs and MRI features differentiating non-compressive from compressive AMs.
Methods
Study design and participants
This is an independent, retrospective, real world, single-centre study conducted at the S. Camillo-Forlanini Hospital in Rome, Italy. Our hospital is an urban, 24/7-open, tertiary clinical care centre with a capacity of approximately 1000 beds, and a volume of over 35,000 admission per year for a catchment area population of two million inhabitants. 13
Eligible patients were identified through the hospital’s Radiology Information System-Picture Archiving and Communication System (RIS-PACS). Two Radiologists (AS and AP) retrieved all spine MRI scans consecutively dictated at our first-level ER between January 2016 and December 2020. Once obtained the demographic information of patients aged older than 18 years who underwent MRI scans, two Neurologists (CT and SH) – blinded to radiology report and final diagnosis – extracted relevant clinical data from the ER database. In January 2021, radiological and clinical data were merged to create an excel spreadsheet by a neurologist unaware of patients’ identity (LP).
To conform with our study purpose, we excluded patients with traumatic myelopathies, those with subacute or chronic myelopathies and those in whom a MRI scan of the spinal cord was not obtained within the first 48 hours from symptom onset. The final diagnosis of ascertained patients was based on the most recent international guidelines on the basis of a complete diagnostic work-up that included not only the MRI features but also other clinical and paraclinical tests as well as lumbar puncture (when applicable).
Our institutional ethical committee provided exemption of approval for retrospective data. An informed consent was obtained from each participant. In no way this study did interfere in the care received by patients and all medical information were sufficiently anonymized to avoid dissemination of confidential data belonging to identifiable individuals. Anonymized data presented in this article will be made available at the request of a qualified investigator; requests should be sent to Dr. Prosperini (luca.prosperini@gmail.com).
Clinical examination
Two neurologists (CT and SH), blinded to MRI data, collected the following demographic and clinical data from ER reports: age, sex, racial category, comorbidities and neurological presentation including temporal profile of symptom onset (hyperacute, i.e. ≤6 h; or acute, i.e. >6–48 hours), 14 presence or absence of asymmetric neurological symptoms, upper limb involvement, pain, limb weakness, pyramidal signs, sensory deficit and sphincter disturbances. We merged all types of pain (e.g. local, radicular and neuropathy) and different sensory deficits (including clinically detectable level or band-like hypoesthesia and leg numbness or paraesthesia) in order to avoid disproportionate granularity of data. Furthermore, we cannot ensure that detailed description of pain (radicular, local or neuropathic) was always available in the ER reports.
MRI acquisition
Imaging parameters used in spinal magnetic resonance imaging, applied to cervical, thoracic and epiconus-conus tracts.
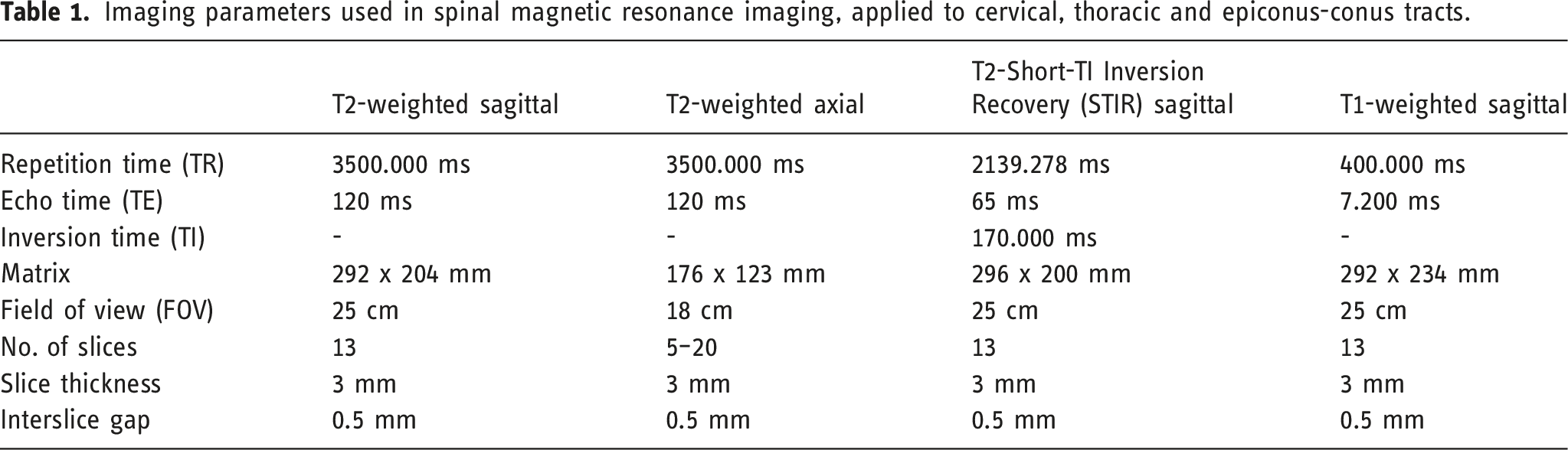
Image analysis
Lesions detected by MRI scanning were evaluated retrospectively according to the following features
11
: (1) location: cervical, cervico-thoracic, thoracic and conus-epiconus; (2) longitudinal extent, that is, < 3 or ≥3 vertebral bodies spanned; (3) contrast-enhancement: absent or present; (4) axial extent: anterior, central, posterior and total; (5) compression grade: we adopted a simplified version of the epidural spinal cord compression (ESCC) scale,
16
based on the obliteration of cerebrospinal fluid around the cord (incomplete or complete), corresponding to an ESCC score ≤2 and 3, respectively).
Image analysis was performed by consensus of two radiologists (VC and AS); disagreement was solved by the most experienced radiologist (AP).
Statistical analysis
Continuous data were modelled as two-level category variables by median-split.
The Fisher’s exact test explored between-group differences, including non-traumatic AMs versus mimics and non-compressive versus compressive AMs. To deal with multiplicity, the statistical significance was determined by the false discovery rate (FDR) correction for multiple testing according to the Benjamini-Hochberg procedure. 17
Clinical variables that resulted significant after FDR correction (i.e. two-sided p-values < 0.05) were entered in two binomial logistic models where we considered as outcomes: (i) the presence of a non-traumatic AM versus mimics and (ii) the presence of a compressive versus non-compressive AM. We were then able to estimate the percentage of patients correctly classified and the amount of variance explained (Nagelkerke pseudo-R2) by the models. When applicable, we finally provided diagnostic accuracy estimations 18 for those combinations of signs and/or symptoms that contributed to the fit of the model(s).
Results
Sample description
The initial inquiry of spine MRI scans dictated at ER and performed in the predefined timeframe (2016–2020) retrieved 105 exams corresponding to as many patients. We excluded from data analysis 16 cases of traumatic AMs and 14 cases of non-traumatic AMs who were admitted to the ER >48 hours after symptom onset (Figure 1). Therefore, we analysed 75 patients (41 men and 34 women) with a mean age of 51.7 (ranging from 18 to 85) years; their racial categories were White (n = 67), Asian (n = 5) and American Indian (n = 3). One or more already known comorbidities were present in 30 (40%) patients; the most frequent concomitant conditions were as follows: arterial hypertension (n = 10), coronary heart disease (n = 7), history of neoplasm (n = 7), type 2 diabetes mellitus (n = 6) and autoimmune disease (n = 3, namely, psoriatic arthritis, rheumatoid arthritis and systemic lupus erythematosus). Study flowchart.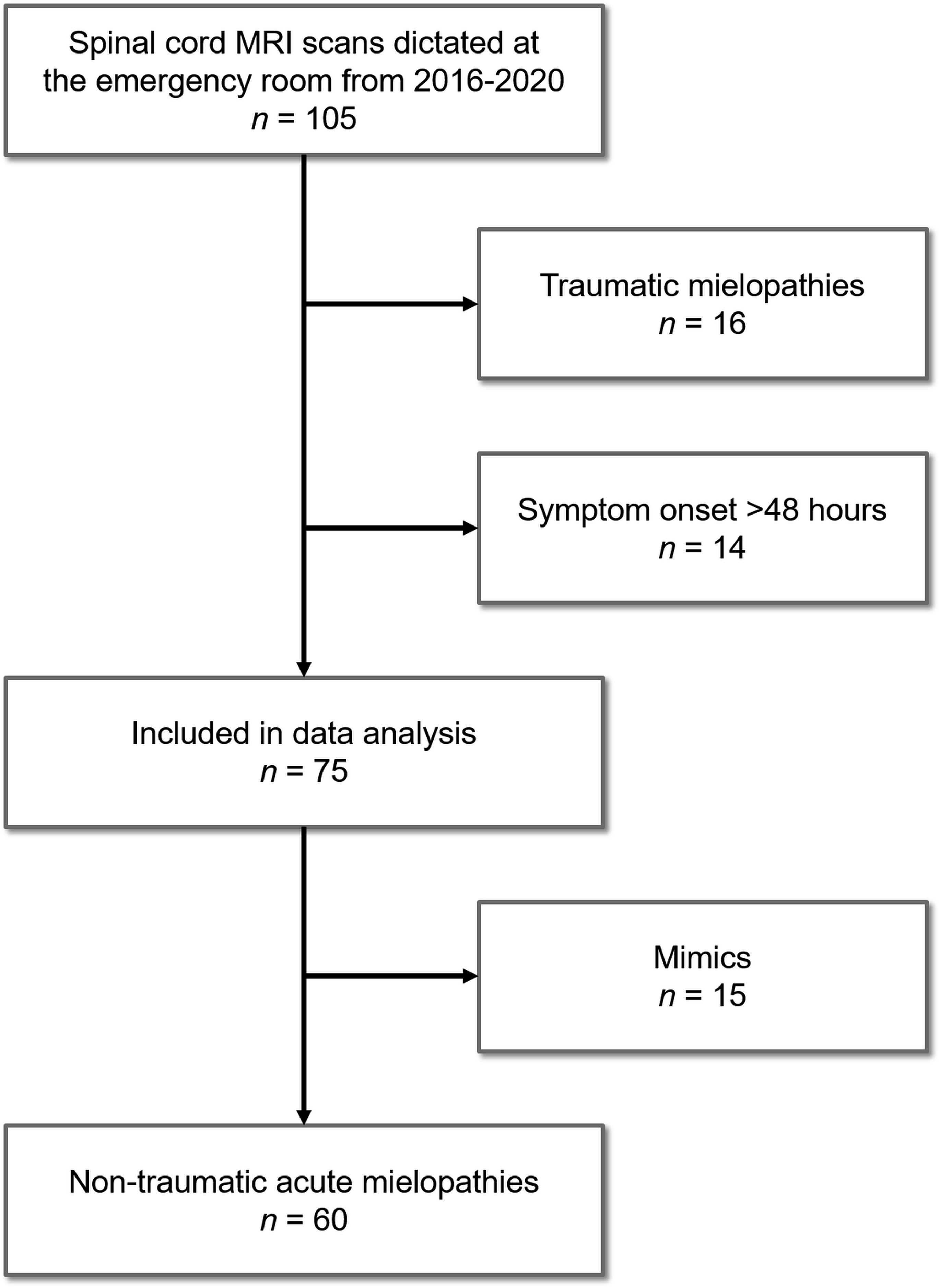
Clinical presentation
The time from symptom onset to ER admission was ≤6 hours (hyperacute presentation) in 37 (49%) patients and 6–48 hours in the remaining 38 (51%) patients. Leg weakness was present in 62 (83%) patients. Pyramidal signs were detected in 38 (51%) patients. Sensory deficits, including clinically detectable level, were described in 41 (55%) patients. A total of 43 (57%) patients complained pain, including dysesthesias, radicular or back pain. Sphincter disturbances were reported by 22 (29%) patients. Overall, the aforementioned neurological disturbances involved only lower limb in 48 (64%) patients, whereas upper limb involvement was also present in the remaining 27 (36%) patients. A clear asymmetry of neurological signs could be detected in 34 (45%) patients. Brown-Séquard or cauda equina syndromes were described in 9 (12%) and 7 (9%) patients, respectively; central cord syndromes were never reported.
Final diagnosis
Final diagnoses of patients’ sample (n = 105).
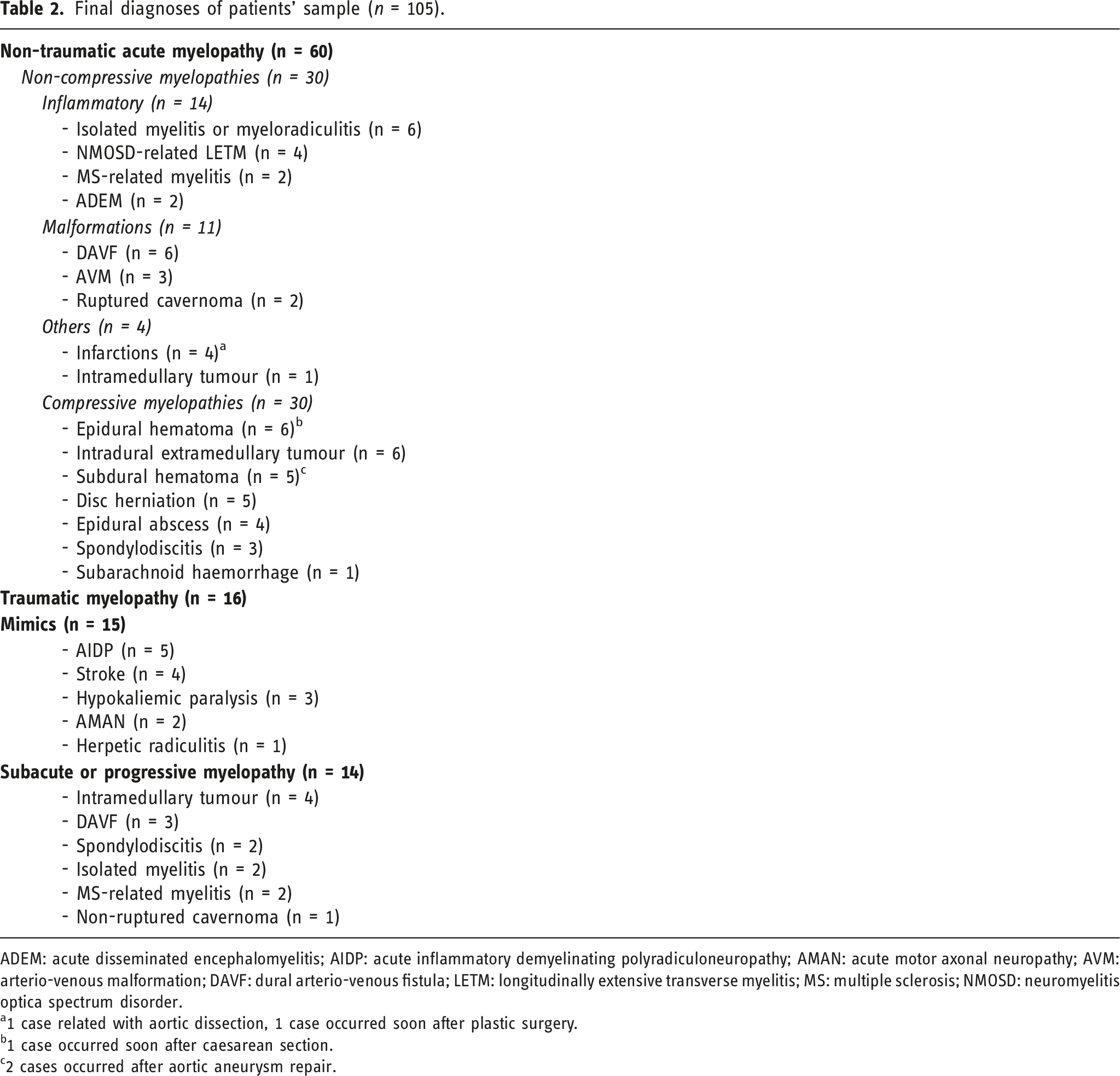
ADEM: acute disseminated encephalomyelitis; AIDP: acute inflammatory demyelinating polyradiculoneuropathy; AMAN: acute motor axonal neuropathy; AVM: arterio-venous malformation; DAVF: dural arterio-venous fistula; LETM: longitudinally extensive transverse myelitis; MS: multiple sclerosis; NMOSD: neuromyelitis optica spectrum disorder.
a1 case related with aortic dissection, 1 case occurred soon after plastic surgery.
b1 case occurred soon after caesarean section.
c2 cases occurred after aortic aneurysm repair.
We analysed data of 75 patients; of them, 15 (20%) were classified as mimics (bias-corrected and accelerated bootstrap 95% confidence interval: 13–28%), whereas the remaining 60 patients were affected by non-compressive (n = 30, 40%) and compressive (n = 30, 40%) AMs.
The most frequent non-compressive AMs were inflammatory disease (n = 14), including isolated myelitis or acute disseminated encephalomyelitis (ADEM) and first demyelinating events anticipating chronic condition, such as neuromyelitis optica spectrum disorders (NMOSDs) and multiple sclerosis (MS). In order of frequency, inflammatory conditions were followed by spine vascular malformation (n = 11), spine infarctions (n = 4) and intramedullary neoplasms (n = 1).
The most frequent compressive AMs were epidural, subdural or subarachnoid hemorrhages (n = 12), followed by infections such as epidural abscess or spondylodiscitis (n = 7), intradural extramedullary tumours (n = 6) and disc herniation (n = 5).
Non-traumatic AM versus mimics
Main characteristics of patients with acute myelopathies (n = 60) versus their mimics (n = 15).
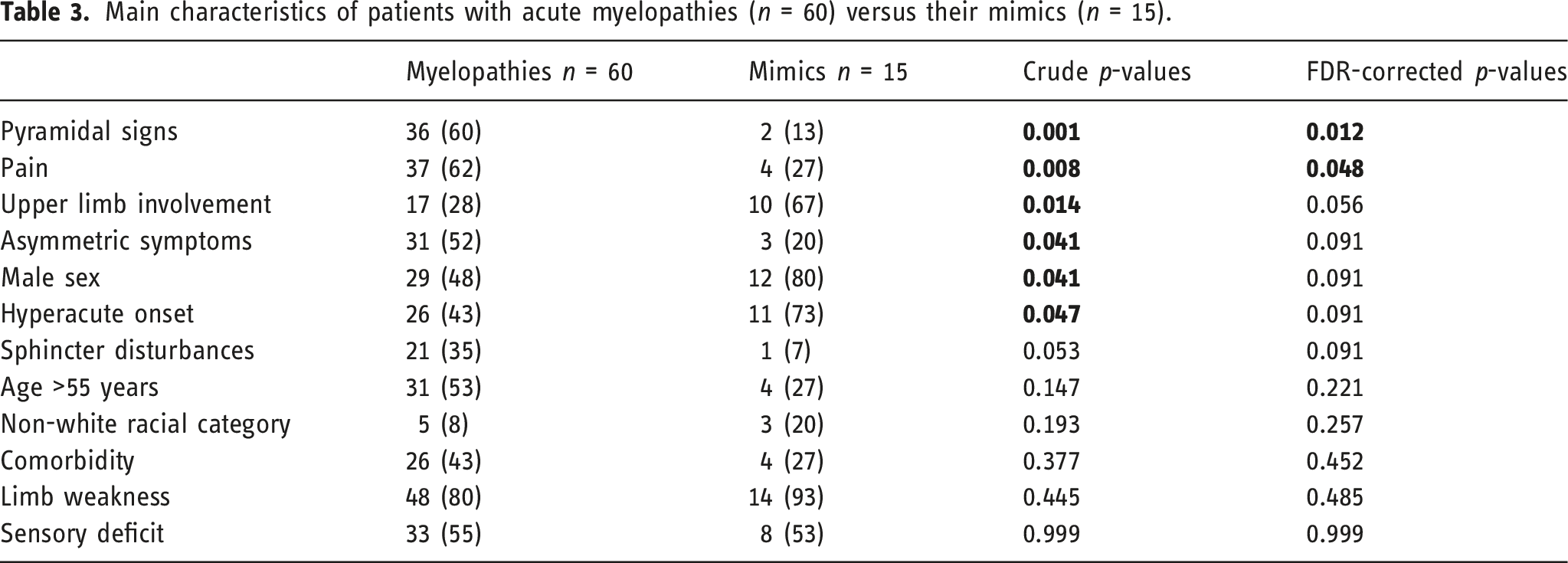
Pyramidal signs were found only in two patients with stroke in the anterior cerebral artery territory. Pain was reported by four patients affected by acute inflammatory demyelinating polyradiculoneuropathy (AIDP) who complained dysaesthesia and muscle pain in the extremities (n = 3) or radicular pain (n = 1).
Diagnostic accuracy values, with their 95% confidence intervals, of pyramidal signs and/or pain to confirm a diagnosis of non-traumatic acute myelopathy (n = 75).
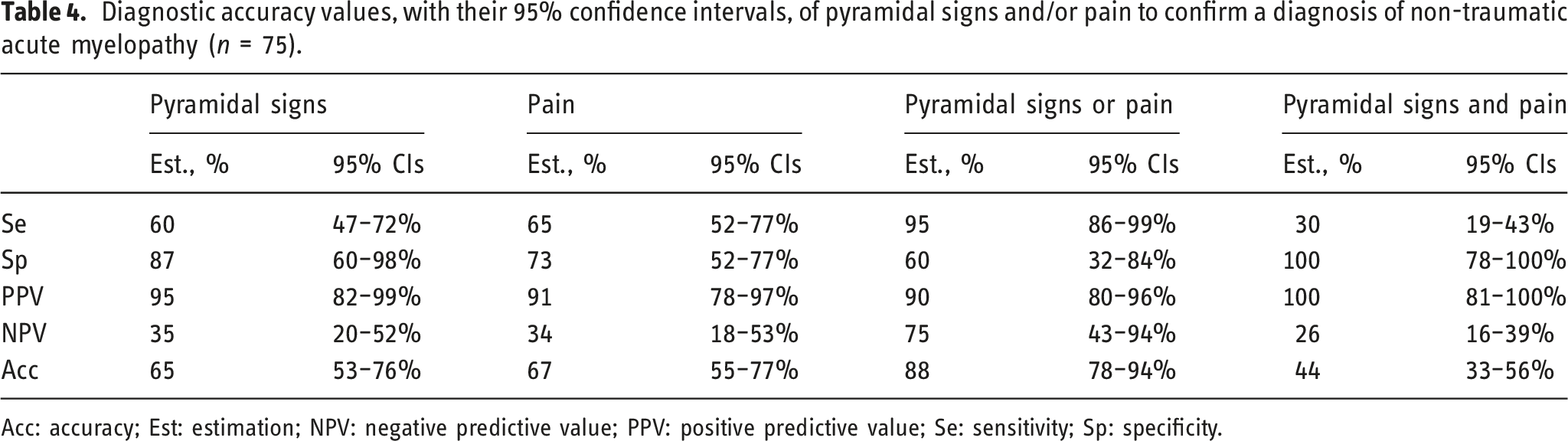
Acc: accuracy; Est: estimation; NPV: negative predictive value; PPV: positive predictive value; Se: sensitivity; Sp: specificity.
Non-compressive versus compressive AM
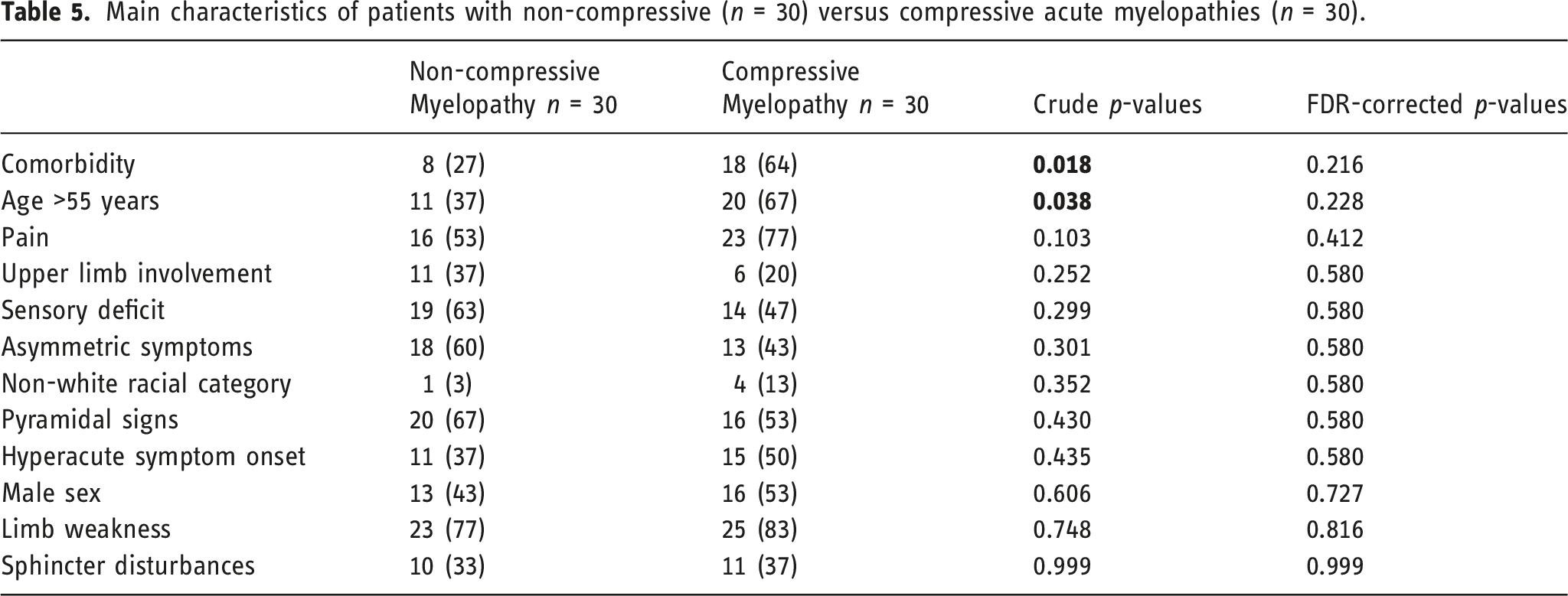
Main characteristics of patients with non-compressive (n = 30) versus compressive acute myelopathies (n = 30).
MRI features
Spine MRI scans were referred by a neurologist in 52 cases, by a neurosurgeon in 16 cases and by an ER doctor in 7 cases. According to the final diagnosis, MRI scanning did not detect spinal cord lesion in 15 cases; in three AIDP cases, gadolinium-enhancement on nerve roots of the cauda equina was observed. Out of 75 MRI scans, 49 were performed on the cervico-thoracic tract, 19 were limited to the thoracic-conus tract (including cauda equina) and the remaining 7 were limited to the cervical tract. Post-contrast MRI sequences were acquired in 47 cases; of these, 31 (66%) showed contrast-enhancement.
The Figure 2 shows the most relevant MRI pictures of non-compressive and compressive AMs. Magnetic resonance imaging examples of different acute myelopathies: (a) isolated myelitis: T2-hyperintense lesion (left) with contrast enhancement on T1-weighted sequence (centre) located in the in the posterior region of the upper cervical cord (right); (b) dural arterio-venous fistula: longitudinal extensive T2-hyperintense lesions of thoracic and conus regions (left), with diffuse axial involvement (right). (c) epidural abscess: extramedullary T2-hyso-/hyperintense mass (left) with a rim enhancement on T1-weighted sequence (centre), and posterior compression on thoracic cord (right); (d) spondylodiscitis: T2-hyperintense extramedullary signal and loss of vertebral boundaries, associated with posterior dislocation of the middle thoracic cord.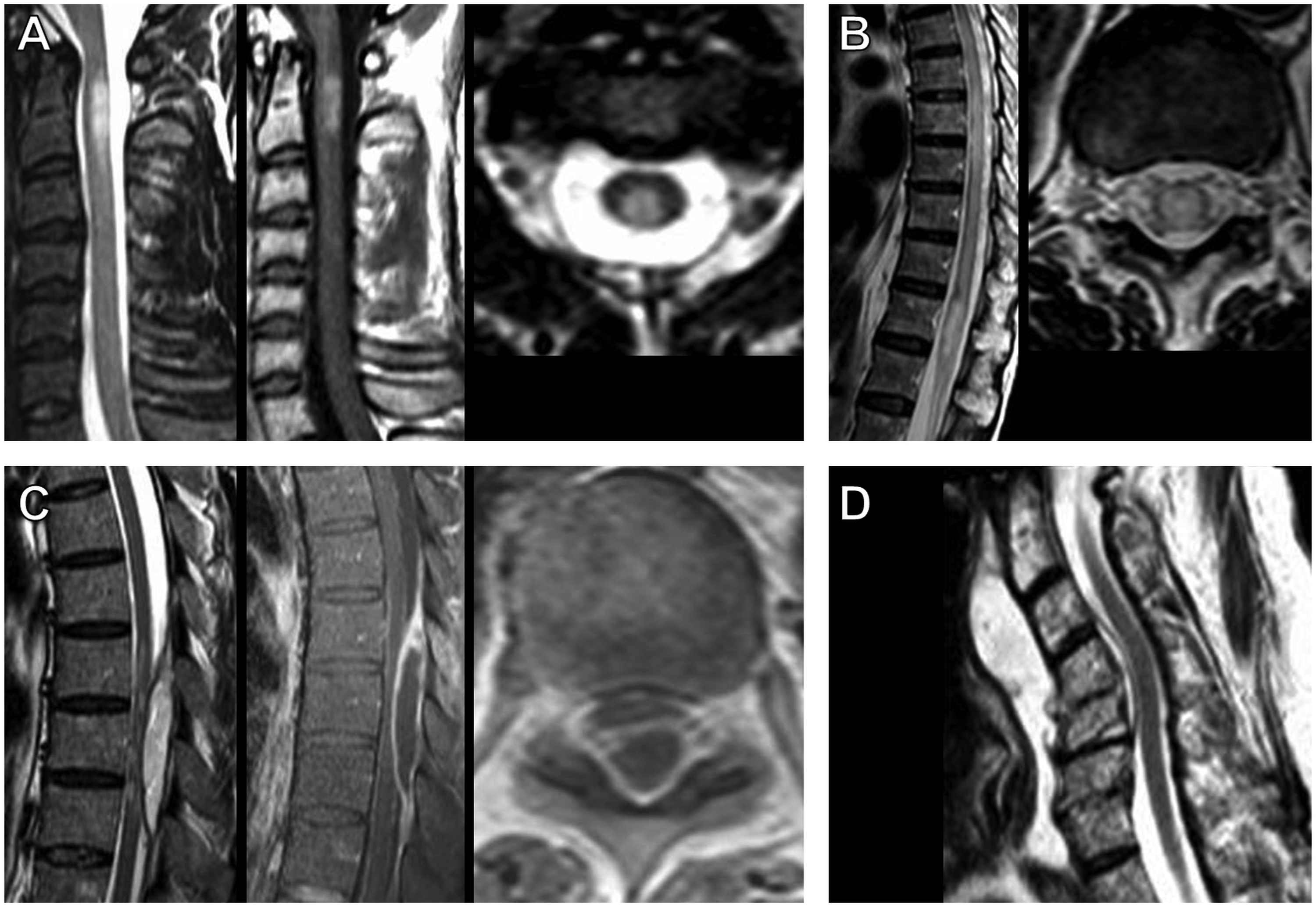
The most frequently involved sites of spinal cord were thoracic (n = 21, 35%), followed by thoracic-conus (n = 15, 25%), cervical (n = 15, 25%) and cervico-thoracic (n = 9, 15%) regions. The frequency of dorsal spine involvement was higher in compressive than non-compressive AMs (crude p-value = 0.03, p = 0.08 after FDR-based correction).
Gadolinium-enhancement was detected in 31 (52%) patients, without difference between compressive and non-compressive AMs.
Overall, longitudinally extensive AMs (i.e. ≥3 vertebral levels at MRI scan) were detected in 36 (60%) patients, 16 in the non-compressive AM subgroup and 20 in the compressive AM subgroup (p = 0.43).
Figure 3 shows the pattern of lesion distribution (axial view) according to the final diagnosis of AMs. Among non-compressive AMs, inflammatory lesions were more often posterior or central; vascular malformations had a fairly widespread distribution, including a complete involvement of spinal cord diameter; spine ischaemias were more often central. Among compressive AMs, intradural extramedullary neoplasms and disc herniations produced more frequently an anterior or lateral compression, whereas hemorrhages and infections produced spine compression on all sides. Frequencies of magnetic resonance imaging patterns of spinal cord involvement in acute non-compressive (a) and compressive (b) myelopathies. Footnotes: * including spine ischaemia (n = 4) and intramedullary neoplasm (n = 1); ** intradural extramedullary neoplasms.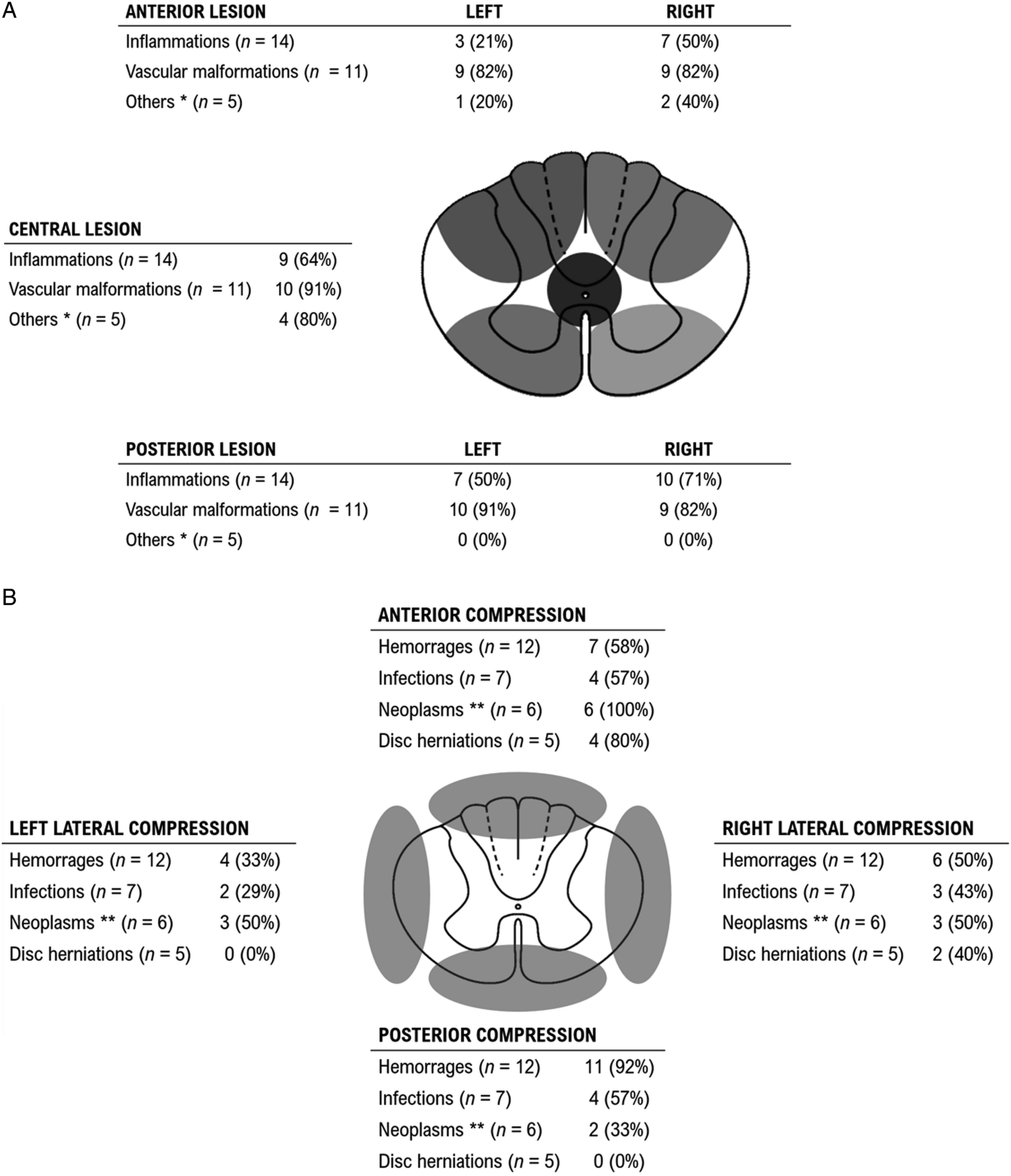
Discussion
In this study, we explored the clinical and MRI features of patients admitted to ER for suspected AMs with a two-fold purpose: (i) to identify red flags suggesting diagnosis alternative to AMs and (ii) to identify clinical signs and MRI features differentiating non-compressive from compressive AMs. Apart from cases obviously related to trauma, here we first retrospectively identified all MRI scans dictated at ER, and thereby we related neuroimaging features and neurological exams with their final diagnosis. Image analysis confirms the possibility of identifying different MRI patterns according to the aetiologic diagnosis with a fair approximation. 14
Timely and accurate diagnosis of AMs is of paramount to avoid missing or delaying recognition of pathologic conditions potentially causing devastating neurologic impairments.4,5 Non-compressive AMs, especially inflammatory conditions, require prompt pharmacological treatment with steroids or plasma exchange.19–21 Non-traumatic compressive AMs, regardless of aetiology, require urgent neurosurgical referral and possibly spinal decompression. 22 Finally yet importantly, several AM mimics may also require time-dependent pharmacological and/or invasive therapeutic procedures, for example, stroke, or prompt recognition as potentially life-threatening conditions, for example, AIDP. 23 Well-recognized spinal cord syndromes, such as Brown-Séquard and cauda syndromes, were described only in a minority of patients (12% and 9%, respectively), thus reinforcing the concept that the initial signs of AM are difficult to capture, 10 especially in the emergency setting. This difficulty gave us further motivation to explore possible combinations of early signs or symptoms that could be easily identifiable to guide a correct decision-making process.
We found approximately one in five patients initially misclassified as affected by an AM (i.e. ‘mimics’). The medical conditions mimicking AMs are mostly in line with literature data. 10 The presence of either pyramidal signs or pain had high sensitivity (95%) and acceptable specificity (60%) to confirm the diagnosis of AMs and, therefore, to rule out mimics. From a more pragmatic standpoint, this latter finding claims the need of more diagnostic work-up and imaging in patients with either pyramidal signs or pain at presentation. Accordingly, red flags suggesting alternative diagnosis were the absence of both pyramidal signs and pain.
In any case, we should consider that pyramidal signs can be as absent during the spinal shock phase,9,10 as present in some mimics such as stroke. 10 Likewise, pain can be present not only as result of spinal or radicular damage but also in peripheral nerve diseases. 24
Unfortunately, we did not find any reliable clinical indicator able to discriminate between non-compressive and compressive AMs, thus emphasizing the imperative need for urgent MRI scan in suspected AMs. Although patients with compressive AMs were on average older than those with non-compressive AMs, this difference did not survive the FDR correction and disappeared when patients with inflammatory conditions were excluded. Similar arguments can be made for comorbidities, which are strongly associated with advancing age.
Additionally, we confirmed previous MRI findings regarding the patterns of axial and longitudinal lesion distribution. Inflammatory conditions affected more frequently the postero-lateral spinal cord at cervical level. 12 Vascular malformations affected more frequently the anterior portion or the entire spinal cord at thoracic-conus level. 14 Posterior compressions of spinal cord were more frequently observed at thoracic or thoracic-conus levels, especially if driven by haematomas or abscesses. 25
This study is not without limitations, including the small sample size, ascertainment and recall biases.
The small sample size can be attributable to the condition under investigation itself, given its lower incidence as compared with other neurological emergencies, such as stroke, epilepsy and even AIDP.3,26–28
Regarding ascertainment bias, we cannot exclude that a number of patients with AMs were not submitted to an urgent MRI scan for several reasons, for example, misdiagnosis, overcrowding in ER and MRI scanner under maintenance.
Recall bias is mainly related with the retrospective study design; we should consider indeed that some clinical information could be missed in the neurological report likely because of time and space constraints at the ER. In this regard, it is notably both the unfeasibility to better detail the quantity and quality of pain and the lack of information on recent infections or vaccinations suggesting post-infectious myelitis or AIDP. Another example concerns patients with hypokaliaemic paralysis who underwent MRI scan before obtaining laboratory data to exclude electrolyte abnormalities.
In spite of these limitations, we are confident that our study has also some strengths. While there are numerous literature reviews, observational real world data on myelopathies are scarce. The few published articles were mainly focused on inflammatory or idiopathic myelitis, spinal infarction or compression.14,22,29–31 Moreover, to our best knowledge, only another study explored the early clinical presentation of AMs in the emergency setting. 22 Another strength of the present study is the adoption of a standardized MRI protocol and homogeneous diagnostic work-up to affirm the final diagnosis according to the most recent international guidelines or expert recommendations.
Conclusion
Hopefully, our study can add valuable insights in the decision-making process of suspected AMs, as much of the existing literature is based on traumatic spinal injuries or provides only limited value in the emergency setting being focussed on specific causes rather than their initial clinical presentation.14,30,32 In conclusion, we confirm that the approach to AMs in the ER is clinically challenging and almost always requires urgent MRI scanning. While some clinical features, namely, pyramidal signs and pain, may help to distinguish AMs from their mimics, spinal cord imaging is essential to discriminate compressive and non-compressive aetiologies.
Footnotes
Acknowledgements
This article is in the memory of the head of Neurosurgery Unit Dr. Agazio Menniti who died prematurely on 29 April 2021.
Author contributions
LP, SH, FRP, CT, AM and CG were responsible for collecting clinical data; AS, AP, VC, EP and EC were responsible for collecting MRI data; AS and LP were responsible for extracting and analysing data; EC, AM and CG were responsible for supervising the manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.