
Abstract
Introduction
Traumatic brain injury (TBI) is a major public health concern in the U.S. Recommendations for patients admitted in the emergency department (ED) to receive head computed tomography (CT) scan are currently guided by various clinical decision rules.
Objective
To compare how a blood biomarker approach compares with clinical decision rules in terms of predicting a positive head CT in adult patients suspected of TBI.
Methods
We retrospectively identified patients transported to our emergency department and underwent a noncontrast head CT due to suspicion of TBI and who had blood samples available. Published thresholds for serum and plasma glial fibrillary acidic protein (GFAP), ubiquitin carboxyl-terminal hydrolase-L1 (UCH-L1), and serum S100β were used to make CT recommendations. These blood biomarker-based recommendations were compared to those achieved under widely used clinical head CT decision rules (Canadian, New Orleans, NEXUS II, and ACEP Clinical Policy).
Results
Our study included 463 patients, of which 122 (26.3%) had one or more abnormalities presenting on head CT. Individual blood biomarkers achieved high negative predictive value (NPV) for abnormal head CT findings (88%–98%), although positive predictive value (PPV) was consistently low (25%–42%). A composite biomarker-based decision rule (GFAP+UCH-L1)’s NPV of 100% and PPV of 29% were comparable or better than those achieved under the clinical decision rules.
Conclusion
Blood biomarkers perform at least as well as clinical rules in terms of selecting TBI patients for head CT and may be easier to implement in the clinical setting. A prospective study is necessary to validate this approach.
Keywords
Introduction
Traumatic brain injury (TBI) represents a major public health issue. Based on the 2016 Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), there were 27 million new cases of TBI and over 55 million prevalent cases in the world. 1 In the United States alone, over 2.5 million annual emergency department (ED) visits are prompted by TBI, resulting in approximately 282,000 hospitalizations and 56,000 deaths.2,3
A noncontrast head computerized tomography (CT) scan is typically the first imaging test used in the workup of patients suspected of TBI. 4 However, only a fraction of head CTs in patients suspected of TBI will show positive findings for TBI, 5 and different clinical decision rules have been developed to triage patients with suspected TBI and to maximize the yield of head CT in these patients. These rules include the Canadian CT Head Rule,6,7 the New Orleans Criteria,8,9 the National Emergency X-Radiography Utilization Study (NEXUS) II rule, 10 and the American College of Emergency Physicians (ACEP) clinical policy.11,12 While most TBI patients should receive the same head CT recommendation regardless of decision rule choice, there remains a fraction of patients for whom different rules will lead to conflicting decisions.13,14 There is no consensus on which clinical rule should be used. 15
Many recent studies have demonstrated the value of blood biomarkers in managing TBI. Among these blood biomarkers, S100β, 16 neurofilament light polypeptide (NFL), 17 glial fibrillary acidic protein (GFAP), 18 and ubiquitin carboxyl-terminal hydrolase-L1 (UCH-L1) 19 have been reported as most promising for diagnosing focal and diffuse brain injury, whereas neuron-specific enolase (NSE), 20 C-tau, 21 and spectrin breakdown products (SBDPs) 22 appear to be correlated with intracranial pressure. 23
The goal of this study was to compare the performance of clinical rules and blood biomarkers in terms of predicting a positive head CT in patients suspected of TBI.
Methods
Study population
We retrospectively enrolled patients transported to Stanford Health Care’s emergency department (ED) by ambulance or helicopter, for whom a trauma alert was triggered per established criteria (http://stan.md/2nw7pfD) and who underwent a noncontrast head CT scan due to suspicion of TBI, between December 2015 and April 2017. Stanford Hospital’s ED provides 24-h neurosurgery facilities and specialized intensive care to over 2500 TBI patients per year. Participant enrollment was limited to Mondays and Tuesdays due to research staff availability.
Patient eligibility was determined based on the following criteria: (1) at least 18 years old at admission, (2) presented to the ED with suspected TBI, and (3) have a blood draw as part of the standard of care. Non-English–speaking patients were excluded, as well as patients without the capacity to consent (including those with altered mental status and hearing impairments) if no legal authorized representative was available.
This study was approved by the Institutional Review Board at Stanford University. In accordance with the Helsinki Principles, research staff obtained written informed consent from patients or from their legal authorized representatives prior to enrollment.
Clinical information and clinical decision rules
Demographic and clinical characteristics were collected as part of their standard of care and extracted from our institution’s electronic health record system, including age, sex, mechanism of injury, Glasgow Comas Score at onset and at 2 h, clinical symptoms at presentation (alertness, general behavior, headache, vomiting, and seizure), alcohol use history, drug use history, and mortality status at hospital discharge. We also obtained records of other major extracranial traumatic injuries (OMEI) and other major intracranial non-traumatic injuries (OMII), for example, a stroke that would have caused the patient to get involved into a trauma.
We considered four commonly-used clinical decision rules for head CT in patients suspected of TBI—the Canadian CT Head Rule (Supplemental Table 1),6,7 the New Orleans Criteria (Supplemental Table 2),8,9 the NEXUS II rule (Supplemental Table 3), 10 and ACEP Clinical Policy (Supplemental Table 4).11,12 Based on each patient’s clinical characteristics, we then determined whether a head CT would be recommended under each rule.
Blood biomarkers
Approximately 25 mL of blood were drawn from and processed for each patient as part of their standard workup for trauma in the emergency room, and our IRB protocol allowed us to use any blood remaining after standard-of-care analyses. Blood samples were initially stored in ethylenediaminetetraacetic acid (EDTA) and serum-separating tubes (BD Vacutainer® Part No. 367861 and 367986, Becton Dickinson, Heidelberg, Germany) in a lightly refrigerated manner at 0–8°C within 30 min of the blood draw, for the period of the standard-of-care blood analyses. A previous study showed that blood biomarkers in lightly refrigerated blood of TBI patients are stable for at least 3 days after blood draw. 24 Subsequently, blood was processed into plasma and serum sample using centrifugation (3500 revolutions per minute for 10 min) and stored as plasma and serum aliquot samples (USA Scientific 2.0 mL self-standing screw cap tube, Part No. 1420-9705 and 1420-9706, USA Scientific, Ocala, FL, USA) at −80°C (900 Series −86°C Upright Ultra-Low Temperature Freezer, ThermoFisher Scientific, Waltham, MA, USA) for batch processing. Samples were shipped overnight on dry ice to a laboratory (Banyan Biomarkers, San Diego, CA) for subsequent proteomic analyses. Technicians were blinded to clinical data and CT results. A sandwich enzyme-linked immunosorbent assay (ELISA) was utilized to detect GFAP, UCH-L1, and their breakdown products, carried out as previously described. 25 An electrochemiluminescence immunoassay (ECLIA) designed for in-vitro diagnostic testing (Roche, Cobas 6000) was used to detect S100β, measured in the serum only. The lower limit of quantification (LLoQ) for GFAP was 3 pg/mL, and the limit of detection (LoD) was 0.8 pg/mL. The LLoQ of UCH-L1 was 14 pg/mL and the LoD was 6 pg/mL. The LLoQ for S100β was 20 pg/mL and the LoD was 5 pg/mL. 10% of GPAF samples were below the LoD. Samples with signals greater than those in the quantification range were diluted and re-assayed.
Head CT imaging review
Noncontrast head CTs were independently reviewed for TBI imaging common data elements 26 as defined by the National Institute of Health (NIH). Two experienced neuroradiologists assessed the presence/absence of closed head injuries including skull fracture, pneumocephalus, hemorrhage, mass effect, and brain parenchymal injuries. The volumes of each type of hematoma or contusion, as well as the extent of midline shift, were quantified as continuous variables, while the extent of subarachnoid hemorrhage, intraventricular hemorrhage, brain edema/swelling, cisternal compression, and hydrocephalus was characterized on ordinal scales.
Statistical analysis
Descriptive statistics were used to characterize the cohort, with categorical characteristics summarized as counts/percentages and continuous characteristics summarized as means with standard deviation (SD) or as median with interquartile range (Q1, Q3) for skewed distributions. Demographic, clinical, and injury severity characteristics were stratified by presence/absence of head CT findings, whether the clinical decision rules recommended a head CT, or whether blood marker values were above a certain threshold value. Thresholds for GFAP (22 pg/mL) and UCH-L1 (327 pg/mL) were taken from Bazarian et al.’s multicenter study for the prediction of intracranial injuries on head CT, 27 and the threshold for S100β (105 pg/mL) was taken from Welch et al.’s study on differentiating normal and abnormal head CT findings in patients with suspected mild or moderate TBI. 25
We presented cross-tabulations of whether a head CT was recommended under each of the four head CT decision rules with actual head CT findings (abnormal vs normal) and estimated measures of test accuracy (sensitivity, specificity, positive predictive value [PPV], and negative predictive value [NPV]). These steps were then repeated for blood biomarker-based decision rules in both the full study cohort and in a subcohort without OMEI and OMII. For the clinical decision rules, the number of rules recommending a head CT was also summarized by head CT status.
Finally, we used the methodology as described in Leisenring et al. 28 to compare PPV and NPV, as estimated under the composite GFAP + UCH-L1 and the four clinical head CT decision rules. For each decision rule pair, a logistic regression model was fitted in the generalized estimating equations (GEE) framework to relate log odds of abnormal imaging status to decision rule, with records restricted to positive decision rule outcomes when comparing PPV and to negative decision rule outcomes when comparing NPV. Statistical significance was assessed at the 0.05 alpha level, and all analyses were performed in the R statistical computing framework, version 3.6. 29
We repeated our analyses three times: (1) for all the study patients together, (2) for the patients with a GCS of 15 exclusively, and (3) for the patients with a GCS of 13 or 14 exclusively.
Results
Study population
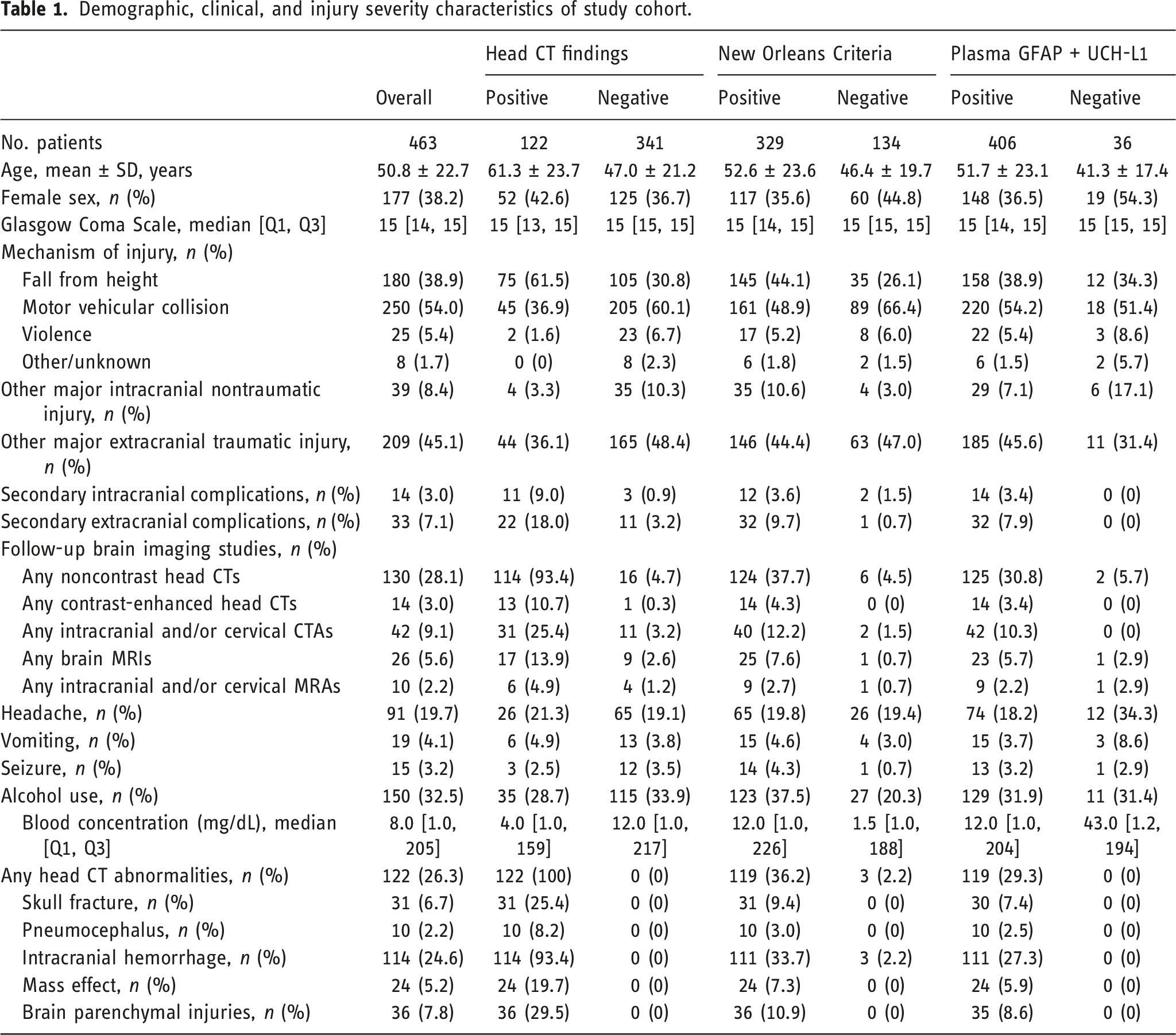
Demographic, clinical, and injury severity characteristics of study cohort.
Head CT imaging findings
Among the 463 patients considered, head CT was abnormal in 122 (26.3%). Classes of abnormalities consisted of skull fracture (6.7% of 463), pneumocephalus (2.2%), intracranial hemorrhage (24.6%), mass effect (5.2%), and brain parenchymal injuries (7.8%).
Clinical decision rules
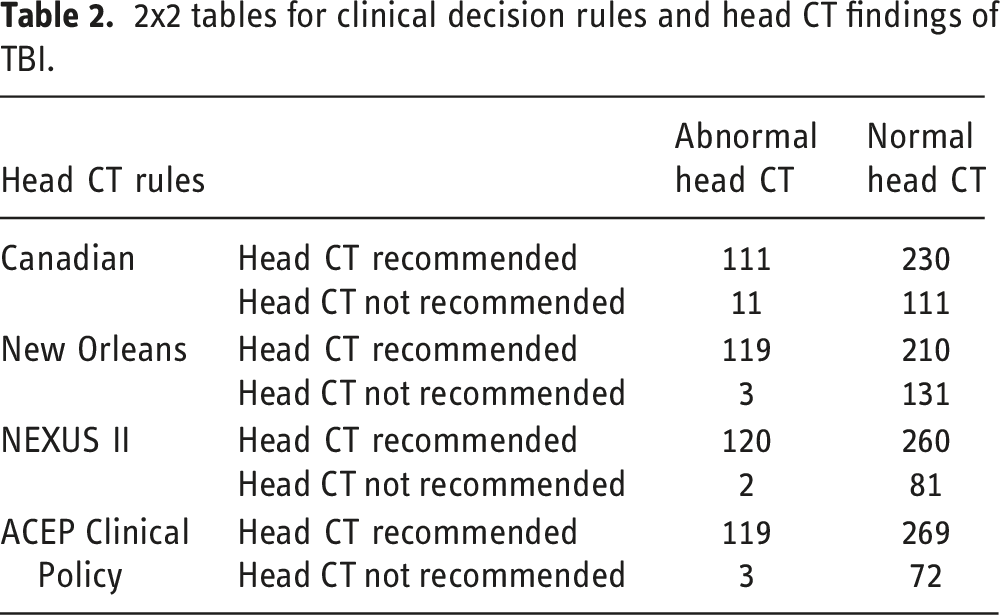
2x2 tables for clinical decision rules and head CT findings of TBI.
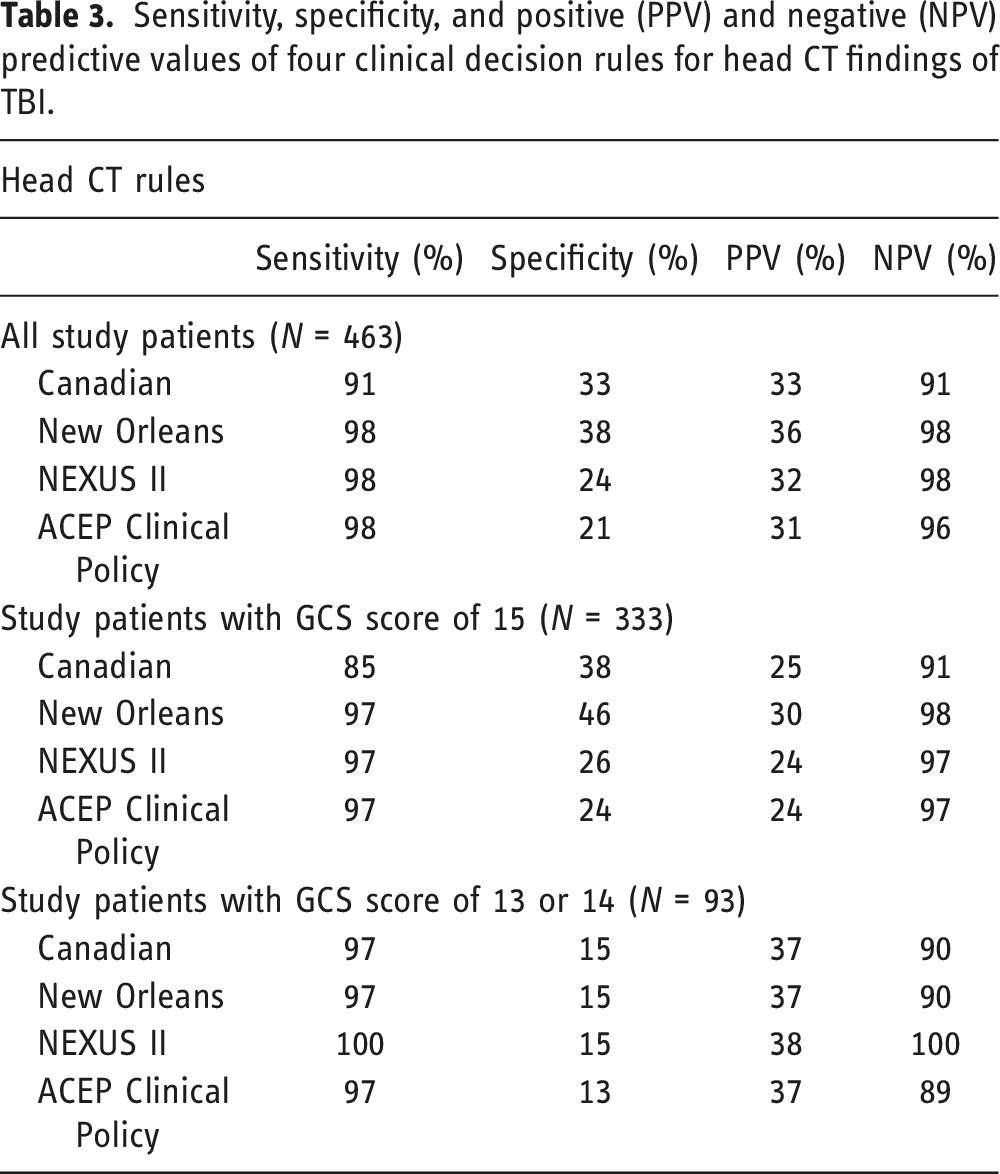
Sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values of four clinical decision rules for head CT findings of TBI.
Concordance of four clinical decision rules for head CT findings of TBI.
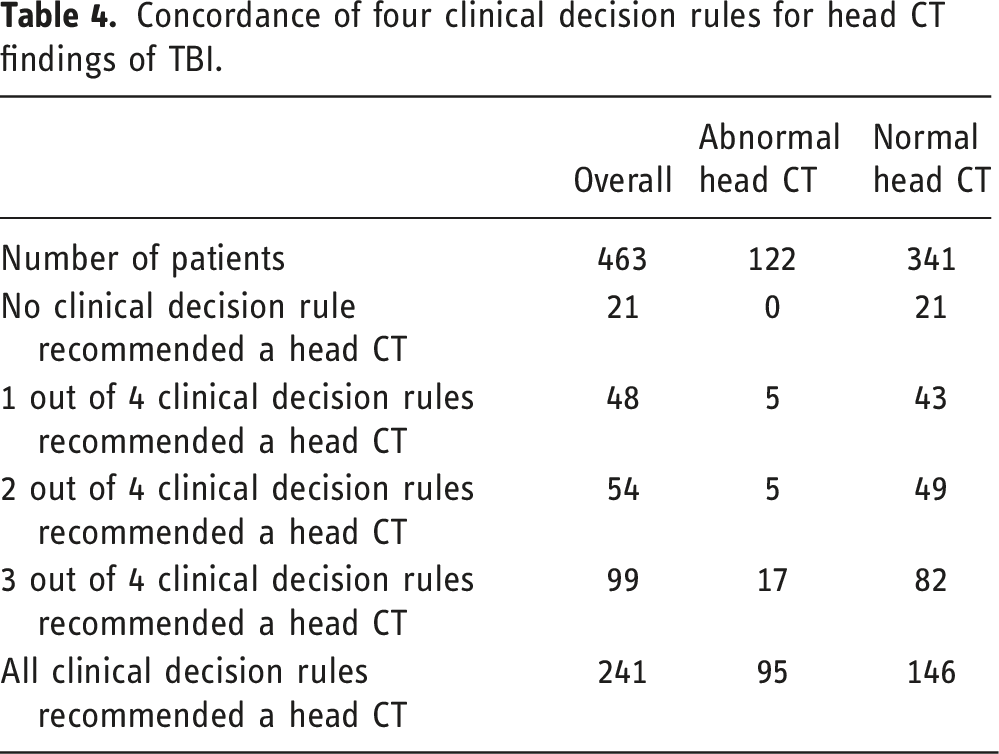
While no patient with positive CT findings would have been missed if all four clinical decision rules were applied together, 14 patients with positive CT findings would have been missed by one, two, or three clinical decision rules. These 14 patients showed the following injuries on CT: skull fracture (1 patient), intracranial hemorrhage (11 patients), nonhemorrhagic contusions (5 patients), and mass effect (1 patient) (the total number of injuries is higher than the number of patients, because several patients showed multiple injuries).
Blood biomarkers
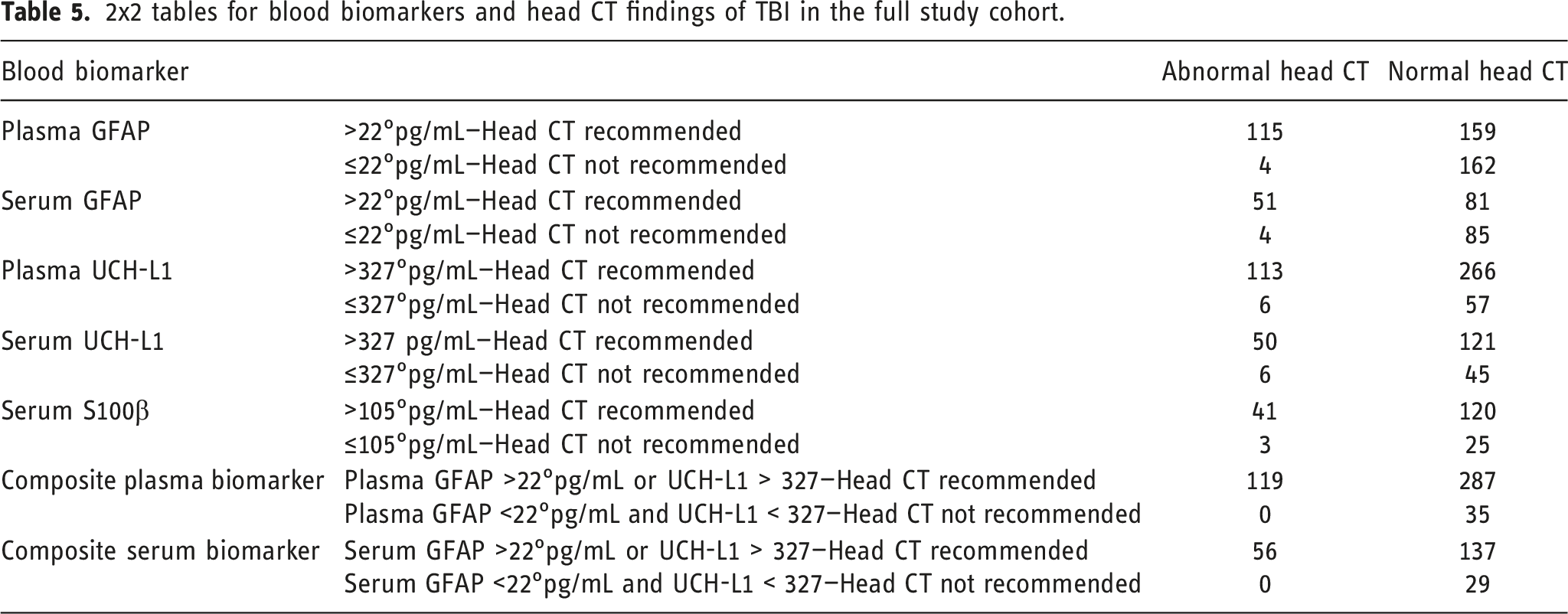
2x2 tables for blood biomarkers and head CT findings of TBI in the full study cohort.
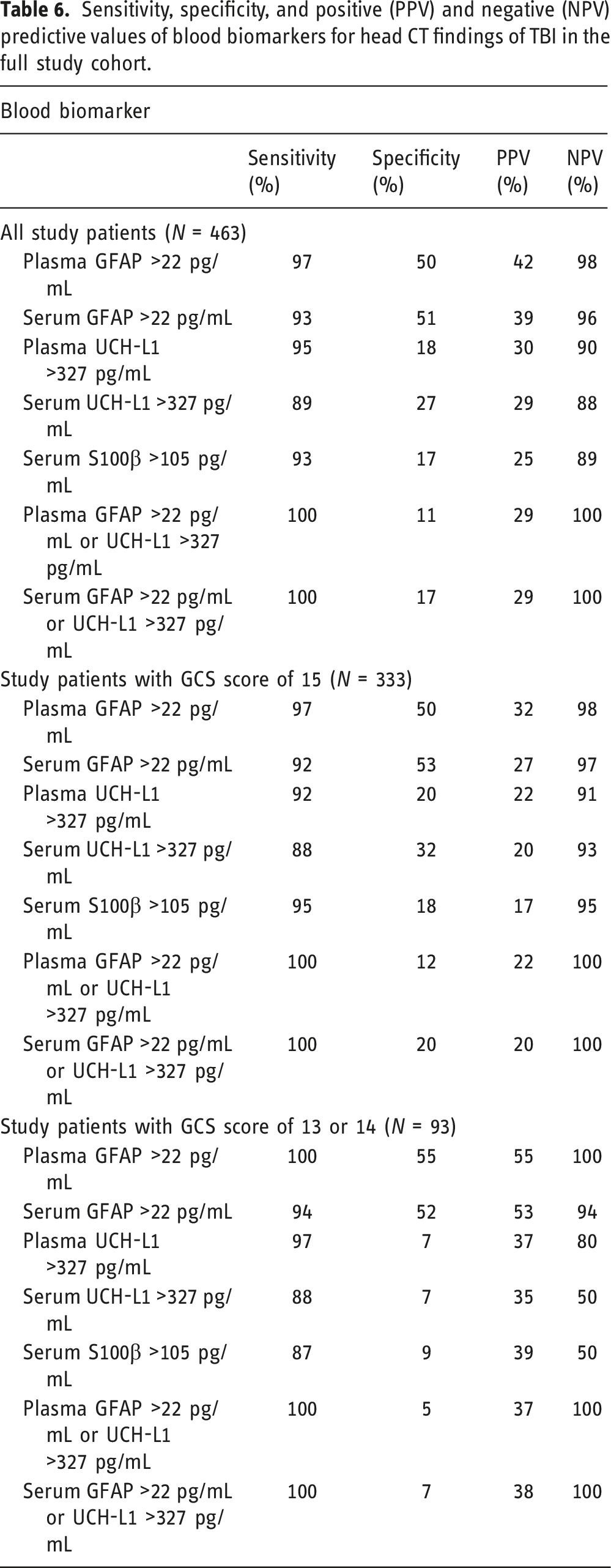
Sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values of blood biomarkers for head CT findings of TBI in the full study cohort.
Under the plasma GFAP + UCH-L1 composite biomarker decision rule, all patients with an abnormal head CT and 11% patients with a normal head CT would have been correctly triaged, respectively. In other words, none of the patients with TBI findings would have been missed for treatment, but 89% of normal patients would have been unnecessarily sent to the CT suite (Table 6).
Comparison of clinical decision rules and blood biomarkers
GEE-estimated a p-values for comparing positive and negative predictive values between composite biomarker and head CT decision rules.
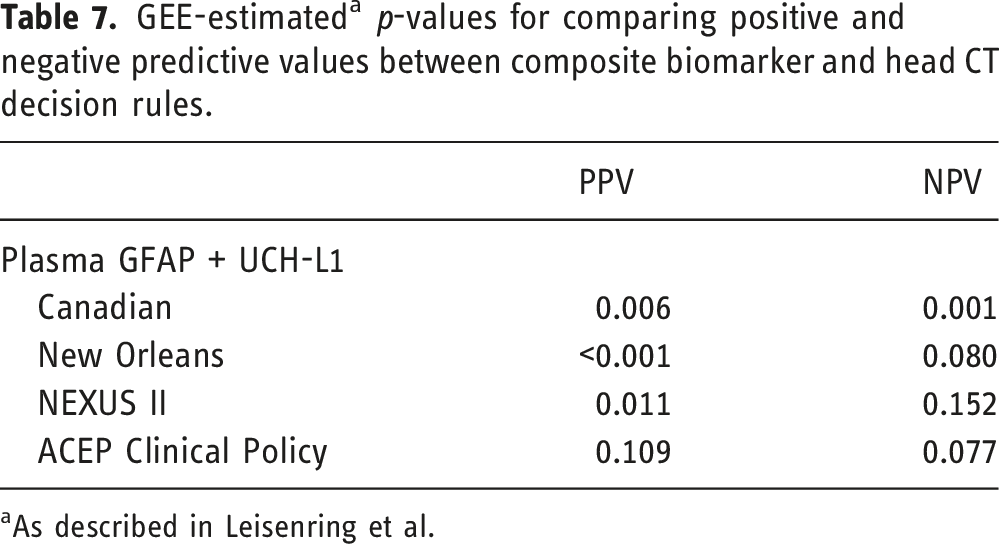
aAs described in Leisenring et al.
Discussion
In recent years, blood biomarkers for TBI have been investigated in multiple studies. Blood concentrations of GFAP, tau, and neurofilament light polypeptide (NFL) were found to be higher in patients with mild TBI compared to those of controls. 18 GFAP yielded an area under the curve (AUC) of 0.93, confirming its discriminatory power for distinguishing mild TBI from controls. 18 S100β and NSE had areas under the curve of 0.63 and 0.64, respectively, for detecting clinically important brain injury. 30 For predicting delayed recovery after mild TBI, top blood biomarker candidates included calpain-derived aII-spectrin N-terminal fragment, tau A, NFL, and ghrelin. 31
In this large prospective cohort, we primarily focused on GFAP, UCH-L1, and S100β. In our patients, plasma GFAP was shown to be the blood biomarker yielding the highest sensitivity (97%) and specificity (50%), which is consistent with previous studies.18,19 A composite blood biomarker test result was best at detecting CT abnormality, also consistent with an earlier study showing that combining tau, NFL, and GFAP achieved satisfactory discrimination (AUC 0.80, 95% CI 0.69–0.90) for detecting MRI abnormalities, even in patients with mild TBI with a normal CT. 18 This may be due that the different blood biomarkers peak at different times after the injury. 32 Depending on how long after the trauma the patient is admitted and blood drawn, one blood biomarker may perform better than the others. Therefore, a composite blood biomarker panel is more likely to detect an abnormality depending on the time from injury to ED admission/blood draw.
Previous research has shown a low compliance with the clinical rules to select TBI patients for head CT, ranging around 15–60%.33-36 Physicians are often either unaware of the clinical decision rules or ignore them in clinical practice due to their complexity.34,36,37 In agreement with past literature,6,9,38,39 our study found all four clinical decision rules to have excellent NPV but low PPV. We also noted that these clinical decision rules lacked consistency. Even the best clinical rule, the New Orleans Criteria, would have sent over 60% of the patients to the CT suite unnecessarily and missed 2.5% of patients with a positive head CT.
The NPV of the composite blood biomarker rule was significantly higher than that of the Canadian CT Head Rule, but was comparable to the other clinical decision rules in the study. Furthermore, the PPV of the composite plasma blood biomarker rule is similar to that of the ACEP Clinical Policy, slightly lower than the Canadian CT Head Rule and the NEXUS II rule, and significantly lower than the New Orleans Criteria.
Most of the clinical decision rules include a GCS threshold, reflecting the fact that they are meant to be used for patients with normal or almost normal GCS scores and that all patients with GCS less than 13 should undergo a head CT to assess for TBI. In our study, we conducted our analyses considering all patients together (including those with GCS less than 13 where a head CT would be recommended clinically) and also separately in patients with a normal GCS (15) and in patients with a GCS of 13–14. The results were the same in all three analyses, showing the high NPV and low PPV of clinical and biomarker rules.
We acknowledge several limitations to our study. All patients in our study underwent a head CT, which is indicative of more severe TBI that the clinical rules were originally developed for. Similarly, the rate of positive head CT (26%) is high, pointing to the same limitation. We tried to address this limitation by presenting a subanalysis focusing on patients with a GCS of 15, and another one for patients with a GCS of 13 or 14. Patients with blood samples may be victims of more severe TBI compared to those who did not get their blood drawn, and our cohort may not be representative of the general population admitted in the emergency room with a suspicion of TBI. We only tested three blood biomarkers. We applied the clinical decision rules retrospectively instead of these rules being applied by the clinicians treating the patients. Similarly, the blood biomarkers analysis was applied retrospectively. Finally, we did not compare the clinical decision rules to each other, only the blood biomarkers to the clinical decision rules.
In conclusion, our study shows that blood biomarkers perform at least as well as clinical rules in terms of selecting TBI patients for head CT and may be easier to implement in the clinical setting. A prospective study is necessary to validate this approach, which could have a significant impact in terms of reducing the number of unnecessary head CTs in patients’ victims of a trauma. Such a prospective study, and the use of blood biomarkers in general for patient screening, will be facilitated by the fact that GFAP and UCH-L1 are now available as point-of-care assay and can be obtained at the bedside.
Supplemental Material
Supplemental Material - Comparing blood biomarkers to clinical decision rules to select patients suspected of traumatic brain injury for head computed tomography
Footnotes
Author Contributions
1. Li: Methodology, Data collection, Data analysis, Manuscript drafting, and Manuscript editing. 2. Ding: Statistical Analysis, Manuscript drafting, and Manuscript editing. 3. Chen: Data collection, Data analysis, and Manuscript editing. 4. Zhu: Data collection, Data analysis, and Manuscript editing. 5. Jiang: Data collection, Data analysis, and Manuscript editing. 6. Boothroyd: Statistical Analysis and Manuscript editing. 7. Rezaii: Data collection, Data analysis, and Manuscript editing. 8. Bet: Data collection, Data analysis, and Manuscript editing. 9. Paulino: Methodology, Data analysis, and Manuscript editing. 10. Weber: Methodology, Data analysis, Manuscript editing. 11. Glushakova: Methodology, Data analysis, Manuscript editing. 12. Hayes: Study Design, Methodology, and Manuscript editing. 13. Wintermark: Study design, Project administration, Methodology, Manuscript drafting, and Manuscript editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.