
Abstract
Disappearing intracranial aneurysms are rare and have not been extensively reported in the literature. They are often small or partially thrombosed and carry a significant risk of recurrence. We discuss a unique case of a 65-year-old woman who presented in 2006 with a subarachnoid hemorrhage and was found to have a ruptured posterior communicating artery and an unruptured P1 aneurysm. Follow-up angiography and imaging showed no changes in the size of a left P1 aneurysm for 11 years (2006–2017). However, in 2021, 15 years after initial presentation, no aneurysm was seen on magnetic resonance angiography, and subsequent digital subtraction angiography in 2022 showed almost complete disappearance of the unruptured P1 aneurysm. Literature review reveals only six reported cases during which a small, unruptured anterior circulation aneurysm disappeared, or regressed on follow-up imaging and no reported cases in the posterior circulation.
Introduction
Intracranial aneurysms are relatively common and present in up to 3% of the general population. 1 30% of patients with one aneurysm will be found to have multiple. 2 Aneurysms are classically found within the circle of Willis, with a preference for the anterior circulation compared to the posterior one. Although consensus regarding a size-based classification of aneurysms is still lacking, aneurysms that are <5 mm are considered small with a low annual risk of rupture, approximately 0.36% per year.3–5 The International Study of Unruptured Intracranial Aneurysms reported that the 5-year cumulative risk of rupture in anterior circulation aneurysms was 0% in aneurysms less than 7 mm, and the corresponding rupture rate for similar aneurysms in the posterior circulation was 2.5%. 5 Disappearance of intracranial aneurysms has been previously reported; however, this often occurs in the ruptured setting or in the setting of giant aneurysms. It is thought to be related to spontaneous thrombosis of the aneurysm. The spontaneous shrinking or disappearance of a small unruptured aneurysm is extremely uncommon. 6 We present a case of a small, unruptured, intracranial aneurysm that was stable across 11 years of follow-up yet spontaneously regressed on all follow-up imaging at year 15. A waiver for consent was obtained and all patient information de-identified.
Case presentation
A 65-year-old woman with a medical history of hypertension and hyperlipidemia presented in 2006 with aneurysmal subarachnoid hemorrhage (SAH) from a ruptured right posterior communicating (PCOM) artery aneurysm. She underwent endovascular embolization of the PCOM aneurysm and during digital subtraction angiography (DSA) was noted to have a small, left P1 aneurysm in addition to the PCOM aneurysm.
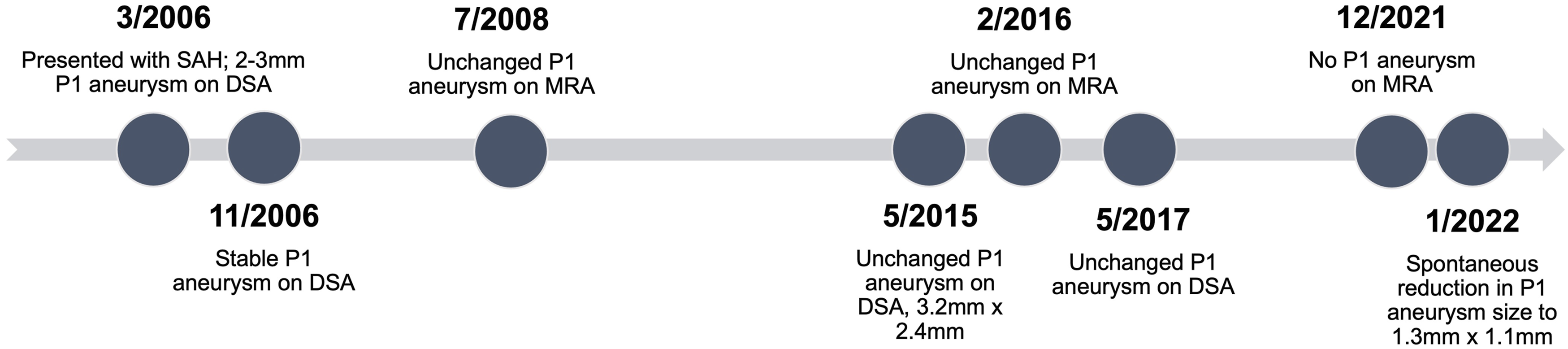
A remnant of the embolized PCOM aneurysm and the P1 aneurysm were both were seen on follow-up angiography at 7 months (Figure 1(a)) and on 3-D time-of-flight (TOF) MRA at 16 months (Figure 1(b)). Both studies described stability of the left P1 aneurysm which measured 2–3 mm. The patient did not receive any follow-up until May 2015 when she underwent angiography which demonstrated the previously documented P1 aneurysm (Figure 1(c)). This aneurysm was oval-shaped, superoposteriorly projecting and incorporating the proximal left P1 segment (Figure 1(d)). It was measured to be 3.2 mm × 2.4 mm with a wide neck. Of note, the previously seen ruptured PCOM aneurysm remnant was enlarged compared to prior imaging and decision was made to place a flow-diverting stent across the recurrence of the PCOM aneurysm. The aneurysm was unchanged during DSA on September 2015, 3-D TOF MRA on February 2016, and DSA on May 2017 (Figure 2). (a) Digital subtraction angiography (DSA) from 2006 of the left vertebral artery showing P1 aneurysm with an arrow indicating a posterior thalamo-perforator originating from the proximal neck of the aneurysm sac. (b) 3-D time-of-flight (TOF) contrast-enhanced magnetic resonance angiography (MRA) from 2008 demonstrating superiorly projecting 2–3 mm left P1 aneurysm. (c) DSA of left vertebral artery from 2015 confirming stable oval-shaped P1 aneurysm. (d) TOF MRA from 2016 showing 3 mm long P1 aneurysm with 2.3 mm neck, unchanged from previous exams. Timeline summarizing the left P1 aneurysm appearance on follow-up imaging between initial diagnosis after subarachnoid hemorrhage (SAH) in 2006 and last follow-up in 2022. All imaging was completed either on 3-D time-of-flight (TOF) contrast-enhanced magnetic resonance angiography (MRA) or digital subtraction angiography (DSA).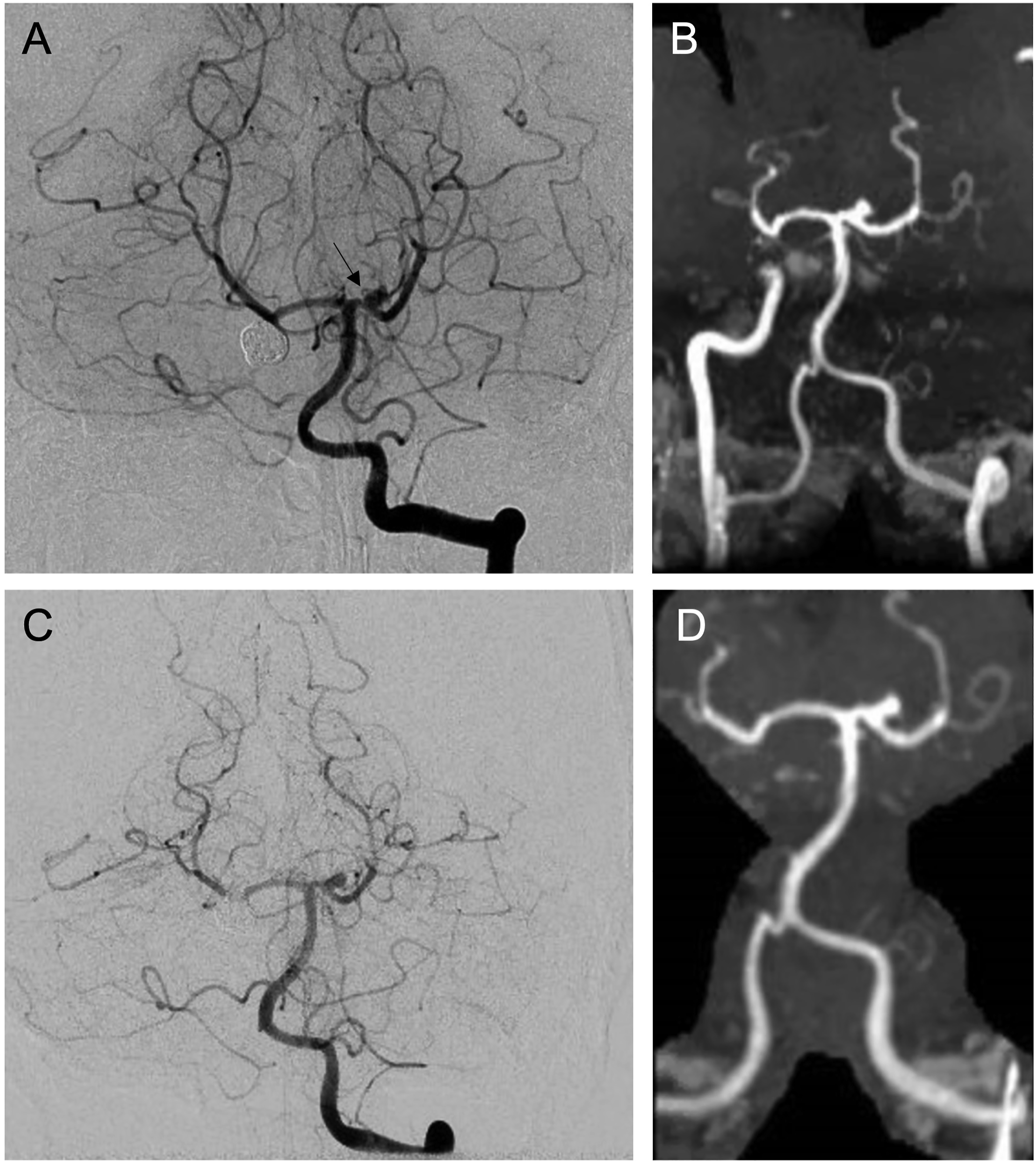
In December 2021, she underwent follow-up 3-D TOF MRA which demonstrated no evidence of left P1 aneurysm (Figure 3(a)). Formal angiography was planned for January 2022 and showed almost complete disappearance of the left P1 aneurysm, now measuring 1.3 mm × 1.1 mm (Figure 3(b)). (a) 3-D time-of-flight (TOF) MRA time-of-flight from 2021 with previous left P1 aneurysm not identified. (b) DSA of left vertebral artery from 2022 showing significant spontaneous reduction in the size of the previously seen left P1 aneurysm, now almost completely occluded, measuring 1.3 mm × 1.1 mm.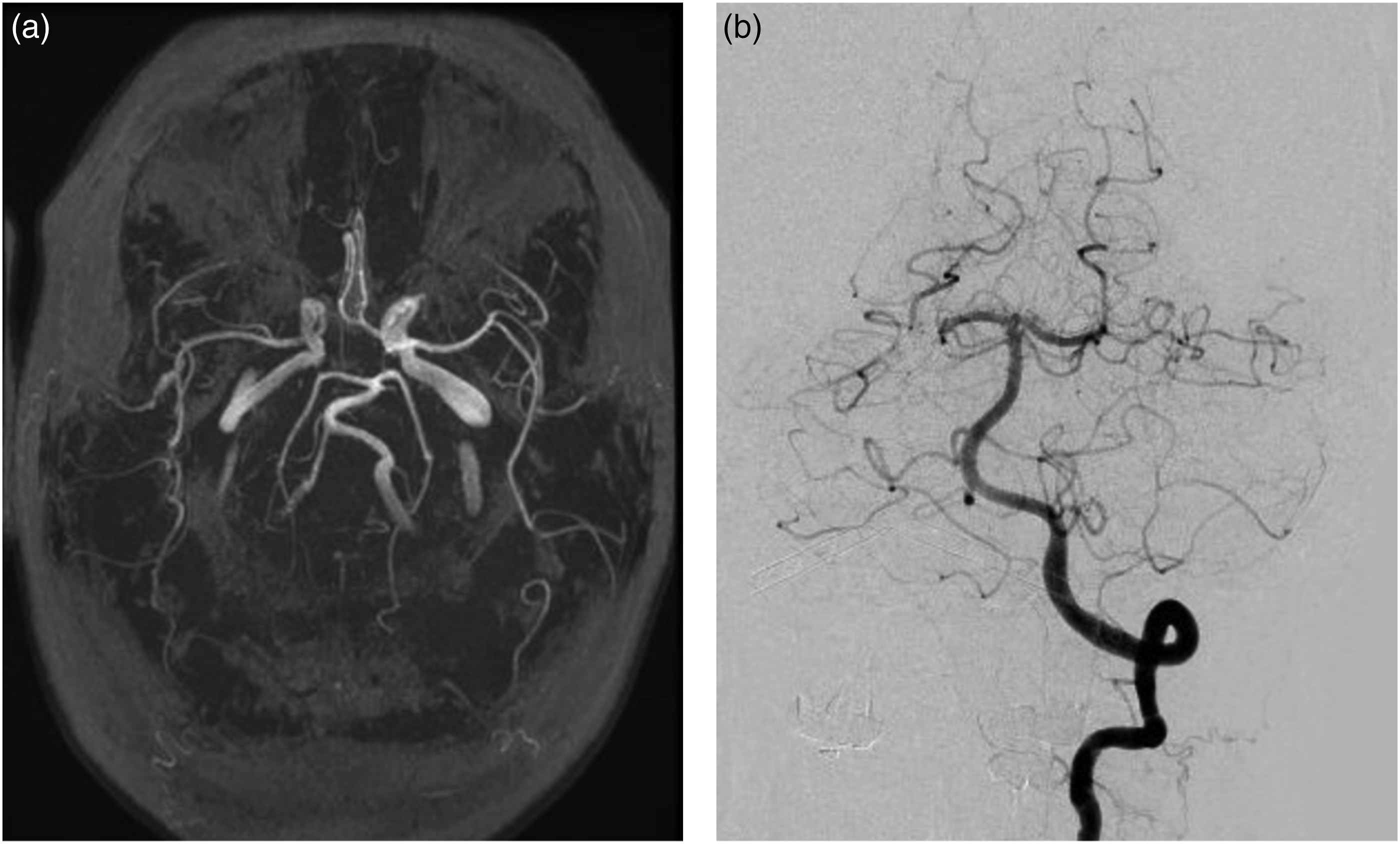
Discussion
Spontaneous resolution of an aneurysm is thought to be associated with thrombosis of the aneurysm sac. Thrombosis of both ruptured and unruptured aneurysms has been previously reported in the literature with an incidence of 1–3%. 7 It most commonly occurs in the setting of subarachnoid hemorrhage after aneurysm rupture, in giant aneurysms, or in partially thrombosed aneurysms. Thrombosis is associated with giant cerebral aneurysms due to the size of the aneurysm dome creating slow and turbulent blood flow that leads to stasis and thrombosis. When thrombosis occurs, imaging findings can mimic intra-axial neoplasms and patients may undergo oncologic workup with attempted resection of the lesion. 8
Factors associated with thrombosis are reflective of classic risks for coagulation and include arterial wall damage, vasospasm of the parent vessel, and relative hypotension. Thrombosed aneurysms are best diagnosed on MRA or CTA as these modalities can image the vessel wall, rather than with DSA which can only characterize the lumen, if patent. Ruptured aneurysms are naturally unstable with endothelial disruption occurring at the time of injury that increases the potential for thrombosis. The spontaneous resolution of intracranial aneurysm has also been reported with flow related aneurysms in the setting of treated arteriovenous malformations.9,10 Changes in hemodynamic flow are thought to lead to spontaneous regression of aneurysms, if shear forces on the vessel wall no longer maintain intra-aneurysm blood flow and allow for stasis.11,12
Reported cases of spontaneous disappearance of a small, unruptured, intracranial aneurysm.
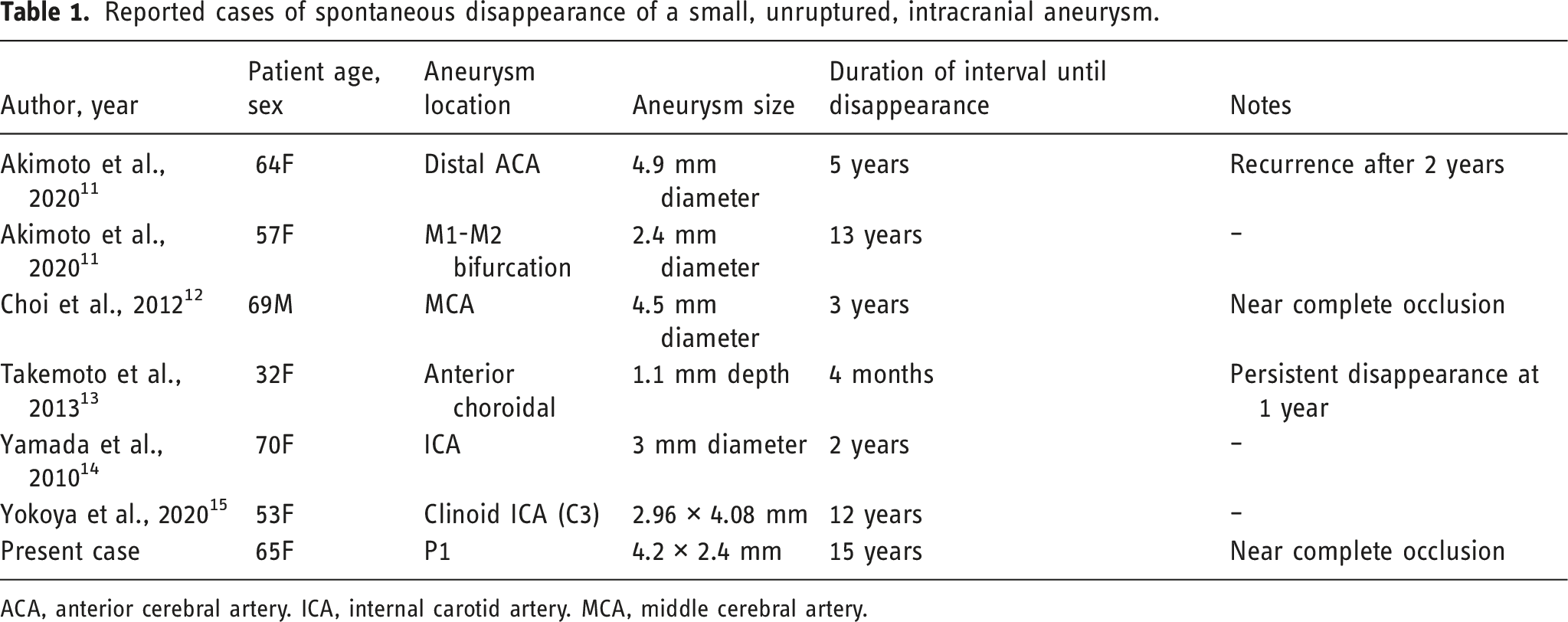
ACA, anterior cerebral artery. ICA, internal carotid artery. MCA, middle cerebral artery.
The proposed etiology of small, unruptured aneurysm disappearance is thought to be linked to spontaneous thrombosis, as it is with giant aneurysms, although the factors that encourage thrombosis in these small sacs are less understood.11,12 Small aneurysms have less potential for stasis, although this is increased in aneurysms with large diameters and narrow necks. Since unruptured aneurysms are not subjected to the endothelial injury associated with rupture, other factors must trigger the coagulation process. Although these aneurysms were all untreated, they did use of formal angiography with intra-arterial contrast injections to monitor growth. It has been proposed that angiographic procedure could contribute to the spontaneous thrombosis and regression via the introduction of turbulent flow, vasospasm, or pro-thrombotic materials. 12 Therefore, the risk of recanalization could remain high after treatment if the return to previous hemodynamic forces encourages thrombolysis and aneurysm regrowth. Patients with spontaneous disappearance of intracranial aneurysms should be followed with a combination of invasive (angiography) and non-invasive monitoring (MRA, CTA) to monitor changes in aneurysm size and risk of future rupture. Given that the patient described in this report went over 4 years without imaging follow-up prior to the documented regression of her aneurysm, it is impossible to know if the spontaneous reduction happened slowly or acutely within that period. This further supports the need for consistent follow-up in these patients which could improve our understanding of the aneurysm regression process.
Conclusion
While intracranial aneurysms are prevalent, the spontaneous disappearance of non-giant and unruptured aneurysms is rare and infrequently described. This report discussed a case of a small, unruptured left P1 aneurysm that remained stable throughout 11 years of follow-up but demonstrated spontaneous and near-complete resolution in the 15th year. A literature review found only six similar cases of disappearing and unruptured intracranial aneurysms <5 mm, with our case uniquely describing a disappearance in the posterior circulation. The unknown etiology in these clinical scenarios warrants the need for continued close observation and follow-up of patients given the risk of recurrence after disappearance. Data collection from follow-up of such patients will be crucial in further understanding the underlying nature of such disappearing aneurysms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.