
Abstract
We report in-vivo imaging of a constellation of arterial variants found incidentally on CT-angiography in a 23-year-old woman presenting with an ischaemic stroke. This extremely rare combination includes a common origin of both common carotid arteries, an abnormal origin of the right vertebral artery (VA) from the right common carotid artery and of the left VA from the aortic arch, associated with an aberrant right subclavian artery. This constellation, previously described in a female cadaver, has not been reported in-vivo. Awareness of this configuration is crucial for radiological diagnosis and when performing angiography and endovascular or surgical procedures in thorax, head and neck, to avoid complications.
Keywords
Introduction
Most of the cases of anatomic variations of the vertebral arteries (VA) are incidentally discovered during angiographic examinations. An origin of the right VA from the right common carotid artery (CCA) occurs only rarely and is frequently associated with an aberrant right subclavian artery (ARSA). 1
Here we report on the incidental finding of a rare constellation of these anatomic variants along with other variants of the aortic arch branches and seen on CT angiography (CTA).
Case report
A 23-year-old tobacco and cannabis consumer woman presented for transient diplopia. The CTA and brain MRI/MR angiography performed using a 3T scan did not show any arterial lesion of vascular malformation.
Nonetheless, CTA revealed a rare constellation of anatomy variants of the aortic arch branches with absence of brachio-cephalic artery: a common origin of both CCAs, a right VA arising from the right CCA, whereas the left VA originated from the aortic arch and a clinically silent retroesophageal ARSA originating distal to the left subclavian artery (Figure 1(a) and (b)). The ARSA crosses the midline between the oesophagus and the vertebral column to reach the right side (Figure 1(c)). Both VAs enter the transverse foramen of C5 (Figure 1(b)). CT angiogram (CTA) was performed using 320-slice Aquilion one system (Canon medical systems).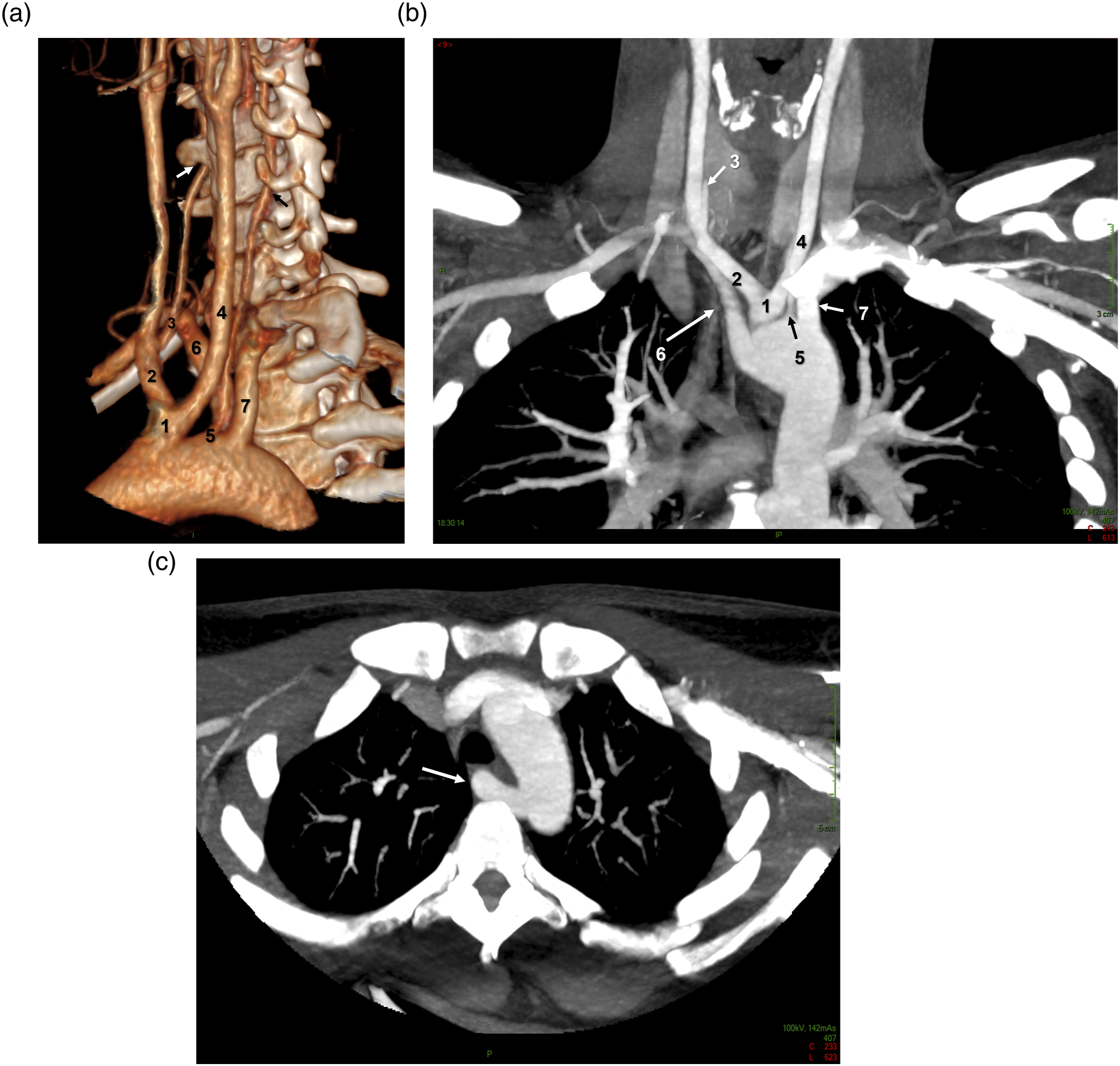
Discussion
An ARSA has been reported with an incidence of <1% and often coexists with other arteries variants. Tsai 1 et al found that 9.8% of patients with an ARSA had a concomitant anomalous right VA branching from the right CCA. Other studies have underlined that the origin of the VA from the CCA is a rare anomaly and that if the VA arises from the right CCA, there is also invariably an increased association with an ARSA. 2 Other studies reported anomalous regarding the VA origin and a common origin of both CCA, that is, a bicarotid trunk also known as truncus bicaroticus.1,3–5 Atypical origin of both VAs has been sporadically reported. A left VA of aortic origin with concomitant bicarotid trunk and ARSA has been found in only 2 out of 14,738 subjects of Lazaridis’ review. 6
Truncus bicaroticus with concomitant ARSA and VAs arising from the respective subclavian arteries has also been reported. 7 A multiple variant, quite similar to our case, including a truncus bicaroticus, an ARSA and a right VA originating from a right CCA has been previously reported on MR imaging. 3 Recently, Sharma 8 reported the association of bicarotid trunk with aberrant left SCA and direct VA origin from the right aortic arch, leading to four arch vessels, in a 7-month-old male infant presenting large ventricular septal defect (VSD). In a study based on a paediatric population undergoing cardiac catheterization, congenital heart disease (CHD) was associated with a truncus bicaroticus in 98.4% of cases, with VST being the most frequent. 9
The coexistence of a retropharyngeal ARSA and of a truncus bicaroticus could limit tracheo-oesophageal mobility. 10 Knowledge of the embryological development of the aortic arch is required for a complete awareness of these variations.4,7,10
We have reported here an extremely rare combination of a common origin of both CCA, an abnormal origin of the right VA from the right CCA and of the left VA from the aortic arch, associated with an ARSA. Although this constellation of variants has been recently reported in a cadaver case, 4 this is the first report of such association using in-vivo imaging to our knowledge.
Conclusion
The common origin of both CCA, abnormal origin of the right VA from the right CCA and of the left VA from the aortic arch, associated with an ARSA are an exceptional complex aortic arch anomaly. As other variants, careful reconstructions and cautious interpretation of CTA and/or MRA images are mandatory.
Awareness of this configuration is crucial for radiological diagnosis and when performing angiography and endovascular or surgical procedures in the thorax, head and neck, to avoid complications.
Footnotes
Author contributions
All authors attest that they meet the current International Committee of Medical Journal Editors (ICMJE) criteria for Authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article was written in accordance with local ethics policy.
Patient details
The authors declare that this report does not contain any personal information that could lead to the identification of the patient.
Informed consent
The authors declare that they obtained a written informed consent from the patient included in the article. The authors also confirm that the personal details of the patient have been removed.