
Abstract
Objective
This systematic review aimed to evaluate the published cases with miliary brain lesions and their etiological factors, clinical manifestations, diagnostic procedures, and outcomes.
Methods
A comprehensive search of PubMed, Scopus, Embase, and Google Scholar was conducted using the specified search strategy. Eligibility criteria included cases with miliary lesions in the brain confirmed through neuroimaging and various diagnostic procedures. The PRISMA guidelines were followed, and the PROSPERO registration number for the protocol is CRD42023445849.
Results
Data from 130 records provided details of 140 patients. Tuberculosis was the primary cause in 93 cases (66.4%), malignancies in 36 cases (25.7%), and other causes accounted for the remaining 11% cases. Tuberculosis patients averaged 35.7 years old, while those with malignancies averaged 55.44 years. Tuberculosis symptoms primarily included fever, headache, and altered sensorium, whereas malignant cases often exhibited progressive encephalopathy, headache, and specific neurological deficits. Distinctive indicators for CNS tuberculosis were choroidal tubercles and paradoxical reactions. Additionally, 63 tuberculosis patients showed miliary lung shadows and 49 had abnormal CSF findings. For the malignancy group, 13 exhibited miliary lung lesions, and 8 had CSF abnormalities. Regarding outcomes, a significant mortality disparity was observed, with 58.3% in the malignancy group, compared to 10.8% in the tuberculosis group and 27.3% in other cases.
Conclusion
Miliary brain lesions are a crucial imaging abnormality that necessitates prompt work up. In an immunocompromised state, diagnostic possibilities of miliary brain lesions are more varied and often pose a bigger challenge.
Introduction
The term “miliary” is derived from the resemblance of these small lesions, measuring 1–5 mm, to millet seeds, especially when viewed on a chest X-ray throughout the lung parenchyma. In the brain, the miliary pattern is characterized by multiple small, nodular, or ring enhancements, with monomorphic lesions less than 3 mm in diameter. Miliary brain lesions can have myriad of causes, with tuberculosis being the most frequent one.1,2
When miliary lesions in the brain are identified in neuroimaging, especially in the absence of a clear clinical scenario, these lesions pose a serious diagnostic challenge. Therefore, a systematic diagnostic approach is essential to prevent unnecessary invasive procedures like brain biopsies. Proper diagnosis is vital for delivering timely and suitable treatments. 3
Most of the data about miliary brain lesions are available as isolated case reports and case series. The principal objective of our systematic review is to evaluate the range of causes behind miliary lesions in the brain. We also tried to make a diagnostic algorithm that can obviate the need for invasive brain biopsy. Nevertheless, on occasion, an early brain biopsy becomes indispensable, when early diagnosis becomes crucial for decision-making. We also evaluated the indications when brain biopsy becomes inevitable.
Methods
This systematic review adheres to the guidelines outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement, as detailed in the PRISMA checklist. Our review has been registered with PROSPERO (registration number- CRD42023445849). 4 Approval by the Institutional Ethics Committee to conduct this systematic review was not needed and no human subjects were enrolled.
Search strategy
The databases of PubMed, Scopus, Embase, and Google Scholar were searched for relevant literature. The first 50 pages of the Google Scholar database were searched for pertinent articles. When searching databases, there are no restrictions based on language. The use of a “Google translator” was used to convert articles written in languages other than English into English. The search strategy we used was “(((Miliary brain lesions) OR (Miliary brain metastasis)) OR (Miliary brain tuberculosis)) OR (Miliary brain fungal lesions).” The date of the last search was 27 July 2023.
Eligibility criteria
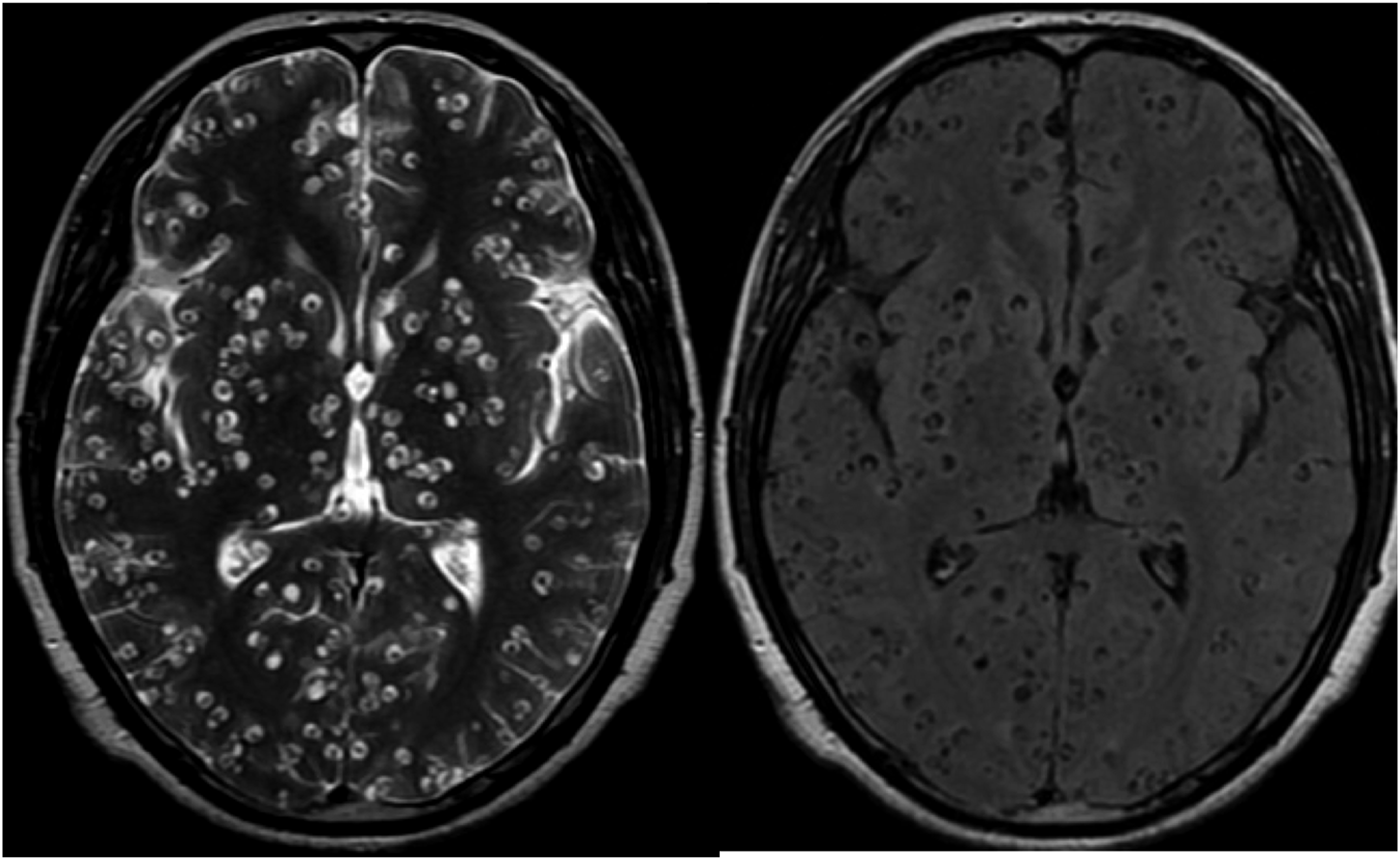
We reviewed the cases exhibiting miliary lesions in the brain. These included patients whose neuroimaging revealed multiple/numerous small, ring, or nodular-enhancing lesions, each measuring less than 3 mm in diameter. (Figures 1 and 2) Magnetic resonance imaging brain shows miliary brain lesions. T2 and FLAIR Magnetic resonance imaging brain shows miliary neurocysticercosis lesions.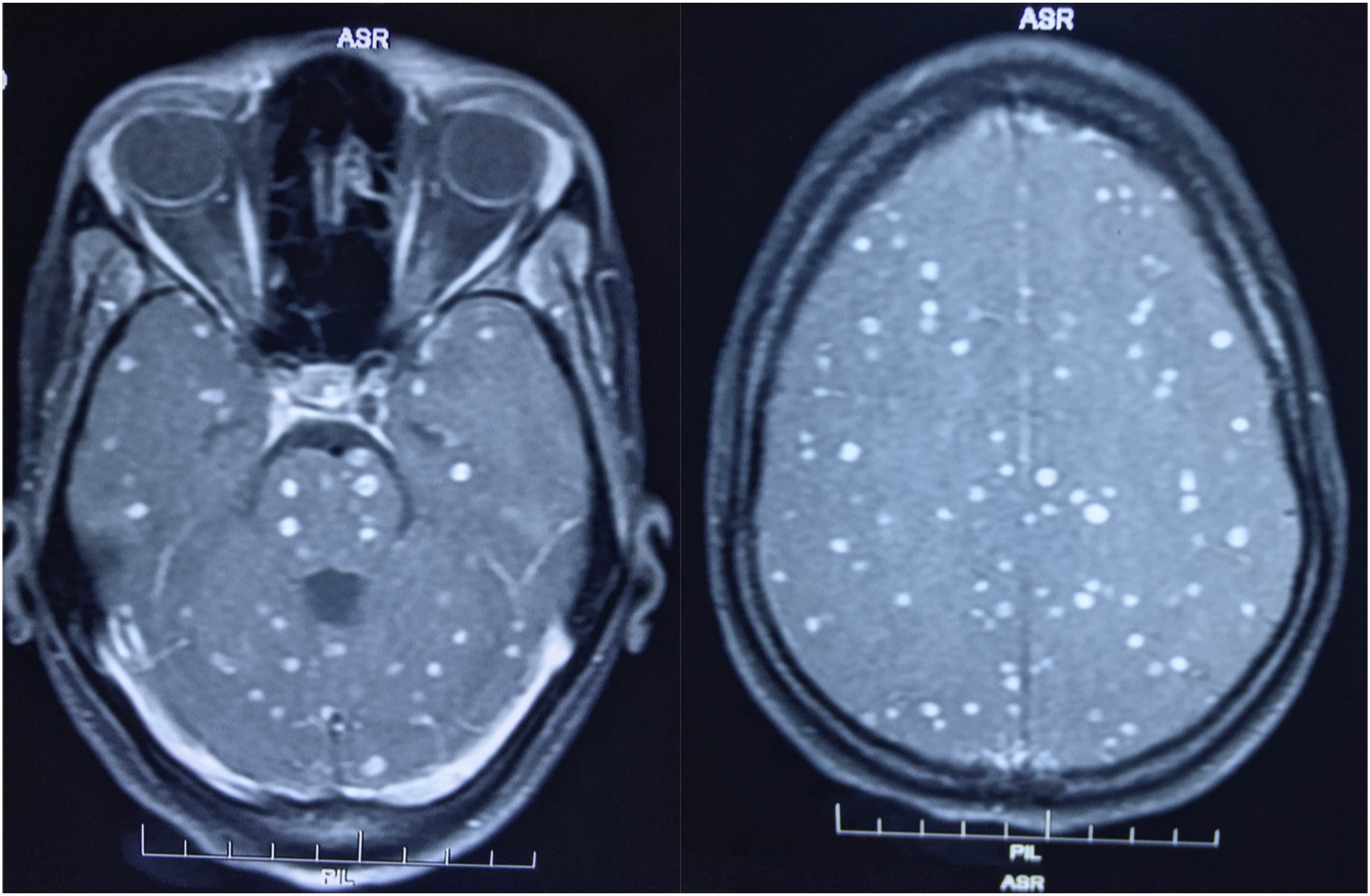
Paradoxical manifestations
In individuals with tuberculous meningitis, a paradoxical reaction refers to the enlargement of the existing tuberculous lesions or the appearance of new brain lesions even after an initial positive response to anti-tuberculosis therapy. 5
Study selection
Case reports, case series, and observational studies were included, if they provided individual patient details and had undergone brain biopsy or autopsy. These must have confirmed diagnoses through histopathological examinations. Moreover, cases where the diagnosis was ascertained in the cerebrospinal fluid (CSF) using alternative methods, such as serology, genetic testing, or smear analysis, were also considered.
Exclusion criteria
Excluded articles encompassed editorials, remarks on prior published cases, and literature reviews. We also did not take into account conference summaries.
Data extraction
The review process was conducted in a two-step approach. First, we assessed the titles and abstracts of the articles. Subsequently, we reviewed the full texts of the shortlisted articles to ensure they met the predefined inclusion criteria. In cases of differing opinions, consensus was reached through discussion.
The EndNote 21 software (Clarivate, Philadelphia, PA, USA) was employed to manage duplicate entries. Any discrepancies or issues that arose were resolved with consensus. A PRISMA flow diagram was also prepared, illustrating the count of records acquired and assessed at every stage. This PRISMA flow chart was prepared with the aid of the EndNote 21 tool.
Quality of reports
Each case had been scrutinized based on four key criteria: selection, ascertainment, causality, and reporting, as detailed by Murad MH et al. 6 Specifically, the chosen cases had encompassed the entire clinical experience, with diagnostic verification through histopathology from biopsied or autopsied brain samples and additional confirmation in the cerebrospinal fluid (CSF) using techniques like serological, genetic, or smear tests. Moreover, a thorough account of the disease’s progression had been essential, with detailed case descriptions that allowed other medical professionals to infer based on their encounters. Using Della Gatta et al.’s standards, a case report that met all these criteria had been termed “good quality,” three domains warranted a “fair quality” designation, and meeting only one or two criteria resulted in a “poor quality” label. 7
Data analysis
The demographic details, clinical features, comorbid conditions including HIV status, type and number of brain enhancements, diagnostic procedures, final diagnosis, treatment, and outcomes of patients were recorded in a Microsoft Word file. The consolidated data was then depicted in tables, showcasing the respective numbers and percentages.
Results
Our review resulted in 130 records describing 140 patients. Among 130, 84 records (93 patients) dealt with tuberculous etiology. Thirty-five records (36 patients) described malignancy and remaining 11 records (11 patients) described etiologies other than tuberculosis and malignancy. Figure 3 shows the PRISMA flowchart for our systematic review. Out of 140 cases evaluated, 130 (92.9%) were classified as having good or fair quality, while the remaining 10 cases were considered to be of poor quality (Supplementary item- 1). The PRISMA checklist has been provided as supplementary item 2. PRISMA flow diagram of the study depicts the procedure of selecting articles for the systematic review.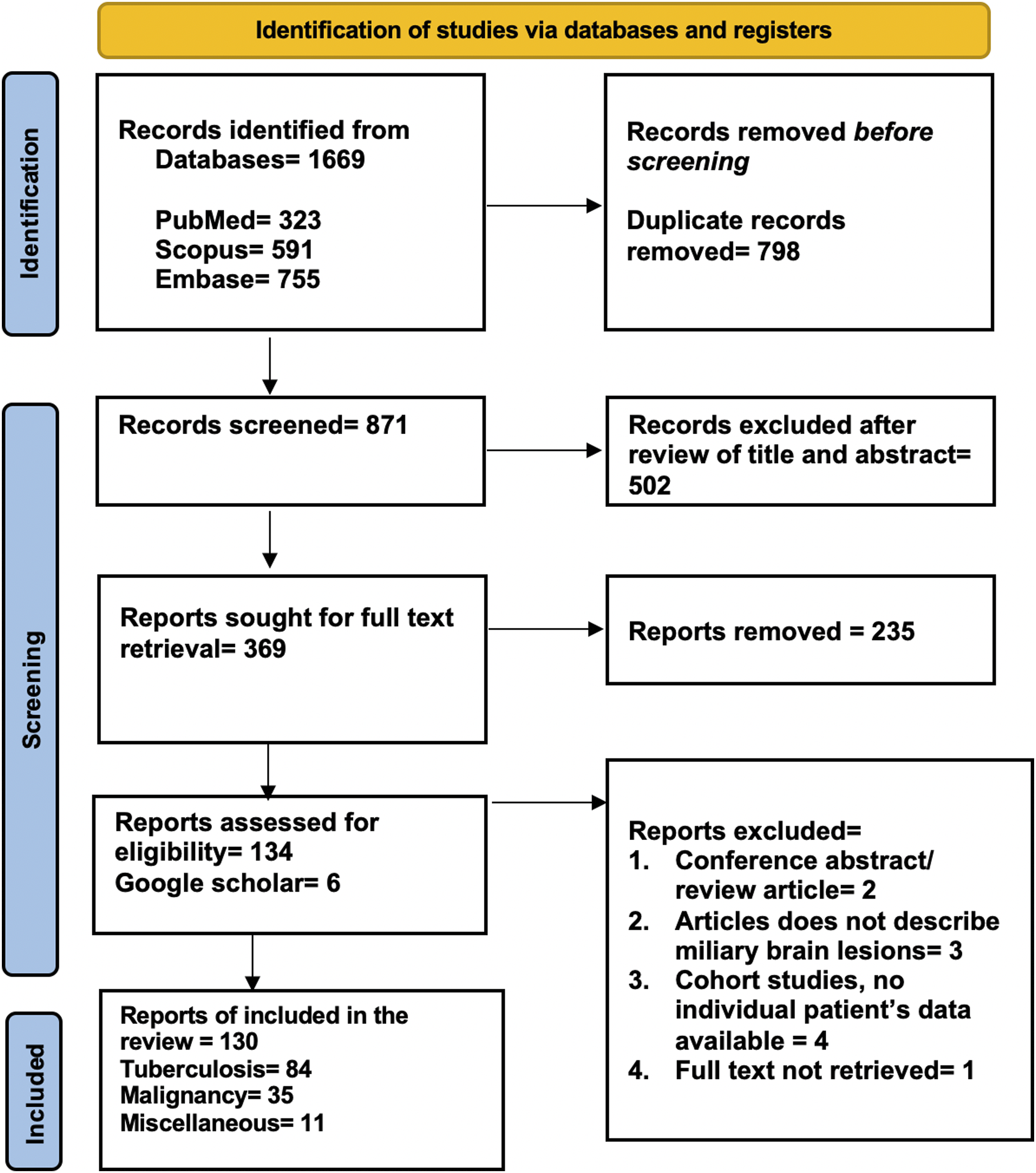
Epidemiological characteristics, clinical features, imaging findings, histopathology of brain lesions, and outcome of patients with miliary lesions of the brain (n = 140).
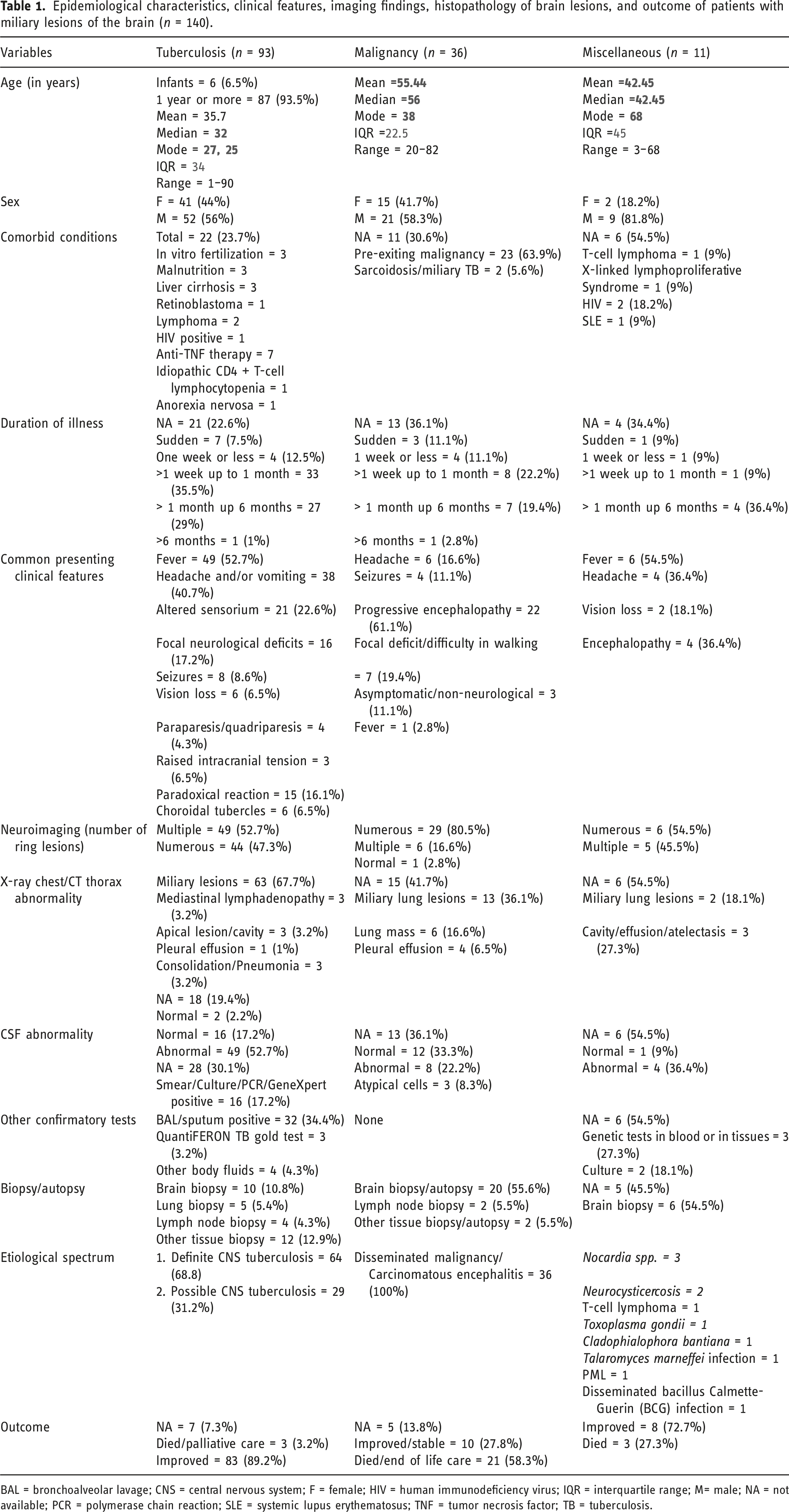
BAL = bronchoalveolar lavage; CNS = central nervous system; F = female; HIV = human immunodeficiency virus; IQR = interquartile range; M= male; NA = not available; PCR = polymerase chain reaction; SLE = systemic lupus erythematosus; TNF = tumor necrosis factor; TB = tuberculosis.
In the tuberculosis group, fever, headache, altered sensorium, and focal neurological deficits were the most frequent presenting clinical manifestations. In addition, 15 (16.1%) patients had paradoxical manifestations and in 6 patients, ophthalmological examination revealed choroidal tubercles. In the malignant group, progressive encephalopathy, headache, and focal neurological deficits were dominant clinical manifestations. The proportion of patients having encephalopathy was more frequent in the malignancy group (61% vs 22%). In the miscellaneous group, fever, headache, and encephalopathy were the most frequent presenting clinical manifestations (Table 1) (Supplementary item- 3).
In the tuberculosis group, 22 (24%) of patients had pre-existing illnesses. Anti-TNF therapy, in vitro fertilization, and malnutrition were three dominant reasons predisposing disseminated tuberculosis/CNS tuberculosis. In cases of malignant miliary brain lesions, around 64% of patients (23/36) had a history of systemic cancer, most commonly lung cancer. Within the miscellaneous group, three patients with either acquired or inherited immunodeficiency (Table 1).
Thoracic imaging showed that in the group with tuberculosis, a majority of patients (63/93; 67.7%) had miliary shadows in their lungs. In the group with malignancy, miliary lung lesions were observed only in 36.1% (13 out of 36) of the patients. In 6 patients, a lung mass was demonstrated. In the miscellaneous group, only 2 patients out of 11 had miliary lung shadows (Table 1) (Supplementary item- 3).
For the group with tuberculosis-related miliary brain lesions, CSF analysis showed abnormalities in over half of the patients (49/93). In contrast, in the group with malignant miliary brain lesions, only 22% (8/36) exhibited CSF abnormalities. In 16 patients, CSF smear/Culture/PCR/GeneXpert tests confirmed the presence of Mycobacterium tuberculosis. In the malignant group, 3 (out of 36) showed the presence of atypical cells. Smear/Culture/PCR/GeneXpert tests in sputum or gastric lavage fluid confirmed the presence of Mycobacterium tuberculosis in 34% (32/93) of patients (Table 1) (Supplementary item- 3).
Brain biopsy/brain autopsy data more frequently confirmed the presence of malignant cells in the brain parenchyma in 55.6% (20/39) patients while in the tuberculosis group, among 10 (1.8%) patients brain biopsy confirmed the presence of Mycobacterium tuberculosis in the brain. In the miscellaneous group, in more than 50% of cases, brain biopsy helped in confirming the definitive diagnosis. In the tuberculosis group, in 29 (31.2%) cases, diagnosis of CNS tuberculosis remained presumptive as Mycobacterium tuberculosis could not be identified. In the miscellaneous group, in the majority (9/11) of cases, an immunocompromised state leading to CNS infection caused miliary lesions of the brain (Table 1) (Supplementary item- 3).
The prognosis was grim for patients having disseminated malignancy as the majority died (58.3%) while in tuberculosis and miscellaneous groups, majority (89.2% and 72.7%, respectively) improved (Table 1) (Supplementary item- 3).
Discussion
In this systematic review, we analyzed cases presenting with miliary brain lesion, the majority of patients were affected by tuberculous etiology, followed by malignancy, and a minority by other causes. Those with tuberculosis typically exhibited fever and neurological issues, with some presenting paradoxical symptoms. Patients with malignancy more frequently had encephalopathy. A notable portion of the tuberculosis group had other pre-existing illnesses, and a significant portion of those with malignancy also had a history of systemic cancer. Thoracic imaging often showed miliary lung patterns among tuberculosis patients, to a lesser extent in the malignancy group. Abnormalities in CSF were common in the tuberculosis group, with Mycobacterium tuberculosis often being identified. Brain biopsies or autopsies generally confirmed malignancy. The outlook was particularly poor for patients with disseminated malignancy, leading to a high death rate, whereas most patients with tuberculosis or other causes generally showed improvement. A diagnostic algorithm, describing an approach to a case of miliary brain lesions, has been prepared (Figure 4). An algorithmic diagnostic strategy for evaluating a patient with miliary brain lesions. Thoracic imaging is one of the most valuable tests in these patients.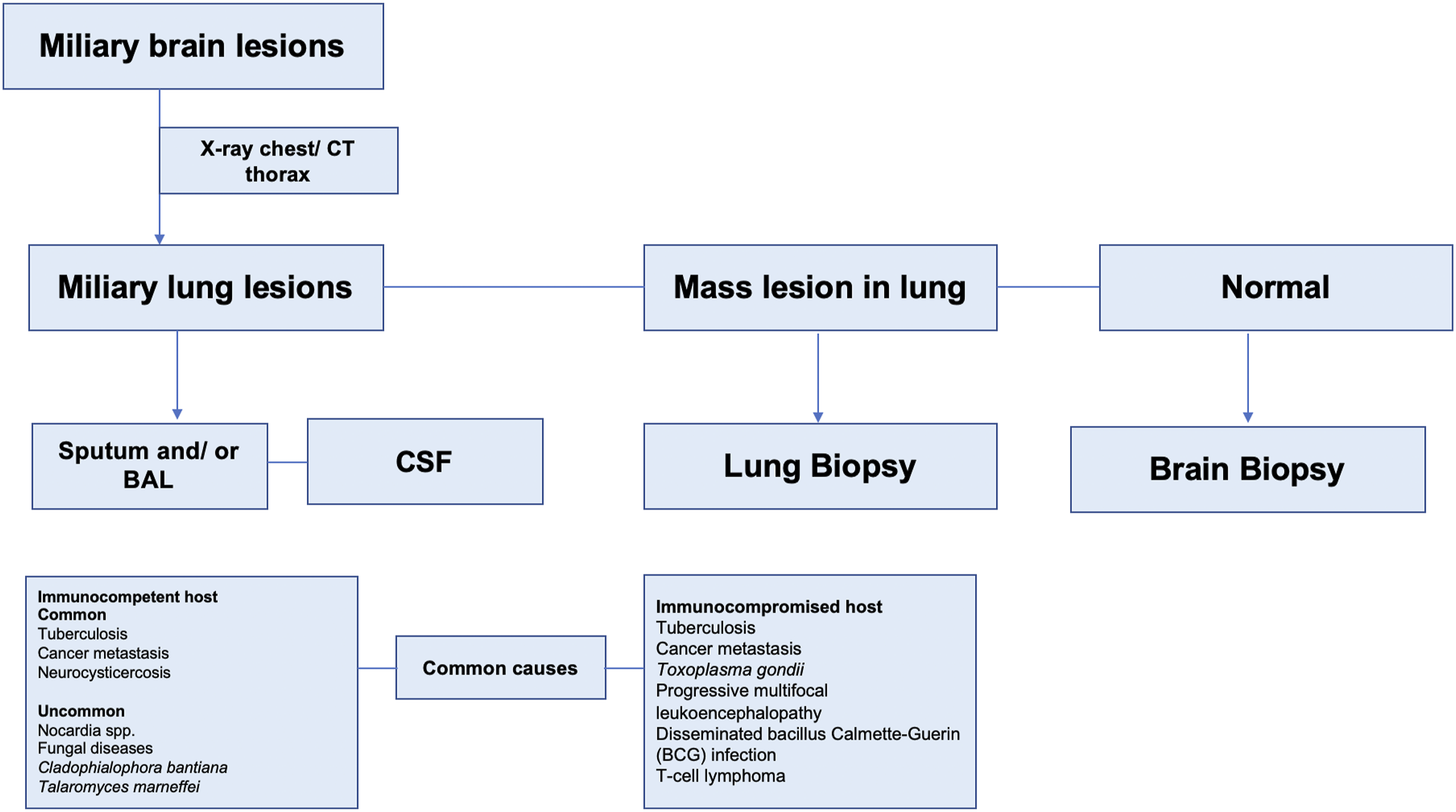
While commonly associated with the lungs, miliary mottling can also be observed in the brain when tuberculosis disseminates, affecting the CNS. We noted that in approximately two-thirds of cases, tuberculosis was established as a cause of miliary lesions of the brain. Imaging of the chest showed that miliary patterns in the lungs in the two-thirds of cases. Similar to our findings in a Chinese study involving 177 patients with pulmonary miliary lesions, contrast-enhanced MRI revealed a miliary pattern in the brains of 157 (89%) patients. 8 In a retrospective study of 32 pediatric patients with tuberculous meningitis, a significant 88% of patients displayed miliary brain lesions. 9 In patients with miliary brain lesions, fever, headache, and miliary lesions in the lungs indicate CNS tuberculosis. Miliary CNS tuberculosis typically coexists with tuberculous meningitis. A prospective study explored the co-occurrence of miliary tuberculosis and tuberculous meningitis in immunocompetent adults. Out of 53 patients with miliary pulmonary tuberculosis, approximately 23.5% were diagnosed with definitive tuberculous meningitis. 10 A study suggested that brain imaging in miliary tuberculosis patients might be beneficial due to the high occurrence of cerebral involvement even in the absence of clinical symptoms or CSF abnormalities. 11
One of the challenges with miliary tuberculosis in the brain is its neuroimaging appearance, which can often resemble miliary metastatic brain cancer. Miliary brain metastases are a form of carcinomatous spread throughout the brain. This condition is frequently termed “carcinomatous encephalitis.” The term carcinomatous encephalitis was first described by Madow and Alpers in 1951. 12 In our review, miliary brain metastases constitute the second common cause of miliary brain lesions. Miliary brain metastases typically arise at an advanced stage of a primary disease, often lung carcinoma, due to its easy access to the systemic arterial circulation. Generally, these patients present with progressive encephalopathy, although many may have minimal findings despite multiple lesions. Nevertheless, the definitive diagnostic method remains histopathologic examination. Certain markers, like thyroid transcription factor 1 (TTF-1), help pinpoint the pulmonary origin of adenocarcinomas. Differentiating miliary metastatic brain lesions from non-neoplastic lesions remains a challenge. Incorrect diagnoses can lead to unnecessary treatments, underscoring the importance of accurate identification. 13
For example, Harrower and co-workers described a 50-year-old woman with a history of tuberculosis exposure displaying neurological symptoms and brain lesions, initially suspected to be tuberculosis-related. Her condition deteriorated following treatment with dexamethasone, which led to the initiation of tuberculosis therapy. However, a brain biopsy 3 months later identified the issue as metastatic papillary adenocarcinoma, likely from the lungs, despite no detected primary lesion. Her smoking history supported this diagnosis. Ultimately, the focus of treatment shifted from actively treating tuberculosis to providing palliative care; however, she succumbed to her illness shortly thereafter. 14
In addition to lung cancer, breast malignancy is another reported source of miliary malignant brain lesions. In a retrospective study encompassing 546 patients with brain metastasis originating from primary breast cancer, in 21 (3.8%) cases, miliary malignant brain lesions were identified. For magnetic resonance imaging, miliary malignant brain lesions were defined as the presence of 20 or more lesions per imaging slice on at least two non-contiguous slices. In contrast, for computed tomography scans, miliary malignant brain lesions were recognized when 10 or more lesions were observed per slice, on at least two non-contiguous slices. Additionally, the criteria included the requirement for bilateral lesions located in both the supratentorial and infratentorial compartments of the brain. 15
In an interesting case, a 72-year-old female who was first thought to have renal cell carcinoma that had spread to her brain and lungs was unexpectedly diagnosed with miliary tuberculosis affecting multiple organs, following investigations that included bronchoalveolar lavage, transbronchial lung biopsy, and renal biopsy. The patient had an excellent response to antituberculous treatment. 16 This case highlights the possibility of diagnostic challenges when miliary brain lesions are encountered. Distinguishing between miliary brain tuberculosis and miliary brain carcinoma is vital, especially when both the lungs and brain are simultaneously affected. Miliary tuberculosis is more common in younger individuals and in patients with HIV positivity, whereas carcinoma is often found in older people and may frequently associated with known malignancy. Clinically, patients with miliary brain tuberculosis often present with basal meningitis, while those with miliary brain carcinoma manifest with progressive encephalopathy. Unique to patients with miliary brain tuberculosis is the presence of choroidal tubercles in the eyes. Furthermore, magnetic resonance spectroscopy for tuberculosis reveals an increased lipid peak and an absence of the N-acetyl-aspartate peak, contrasting with miliary brain carcinoma which shows an increase in choline and a decrease in creatine peaks. Diagnostic confirmation for tuberculosis often involves CSF, bronchial wash, and transbronchial biopsy showing caseating granulomas, whereas miliary brain carcinoma is often diagnosed on autopsy. The paradoxical appearance of new brain lesions is common in CNS tuberculosis. Miliary brain metastases often signify advanced cancer. 17
Our review has several limitations. The heterogeneous nature of the included case reports and series could affect the findings’ reliability and generalizability. The study’s observational nature, primarily based on case reports and series, limits establishing causality. Diagnostic inconsistencies across studies due to the lack of standardized definitions for clinical presentations could skew results. Additionally, there may be a bias in publication since negative or inconclusive results could be less frequently reported. Going forward, there should be a focus on conducting prospective cohort studies to gain a clearer understanding of causality.
Miliary brain lesions are an uncommon but crucial imaging abnormality that necessitates prompt attention. In an immunocompromised state, diagnostic possibilities of miliary brain lesions are more varied and often pose a bigger challenge.
Supplemental Material
Supplemental Material - The etiological spectrum of miliary brain lesions: A systematic review of published cases and case series
Supplemental Material for Estimating a The etiological spectrum of miliary brain lesions: A systematic review of published cases and case series by Ravindra Kumar Garg, Vimal Paliwal, Swastika Suviriya, Hardeep Singh Malhotra, and Anoop Verma in The Neuroradiology Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.