
Abstract
Soft tissue aneurysmal bone cysts (STABCs) are rare neoplasms histopathologically identical to aneurysmal bone cysts. These benign lesions are characterized by thin, peripheral ossification and no skeletal continuity. STABC may be difficult to distinguish from myositis ossificans (MO) and malignant entities from imaging and fine needle aspiration, due to rarity and overlapping features. We present a case of a STABC occurring in the paraspinal cervical muscles. The imaging, histopathology, molecular analysis, and treatment are discussed. Four other published cases of STABC of the head and neck are reviewed.
Introduction
Aneurysmal bone cysts (ABCs) are benign osteolytic lesions of the bone found in isolation or associated with adjacent osseous neoplasms. 1 Approximately two-thirds of ABCs occur in long bones, predominantly in the metaphysis. 1 Once believed to be a purely reactive lesion, the identification of rearrangement of ubiquitin-specific peptidase 6 (USP6) gene located at chromosome 17p13 in isolated tumors has substantiated the classification of this entity as a neoplasm. 2
First described in 1972 by Salm and Sissons, soft tissue aneurysmal bone cysts (STABCs) are rare neoplasms with no skeletal continuity but histopathologically identical to ABCs.3–5 Over half of STABCs occur in the lower extremities, while 19% occur in the arm, and 15% in the shoulder area. 2 Head and neck cases are particularly unusual, with only four reported cases to date: two in the periclavicular area,4,6 one involving the carotid bifurcation, 7 and a fourth laryngeal ABC with no apparent connection to the cricoid perichondrium. 8 Additionally, three other ABCs involving the larynx have been reported,9–11 but these are related to laryngeal cartilage ossification and are not considered soft tissue in origin.
Here, we report a case of an STABC of the cervical paraspinal muscles, with a review of the relevant literature. Recognition of this rare entity by neuroradiologists can facilitate earlier intervention as compared to other benign ossifying processes that are routinely observed. The imaging characteristics, treatment considerations, histopathological features, and molecular analysis of STABCs are described in detail.
Case report
A 53 year-old, otherwise healthy, female presented with a 5-month history of a progressively enlarging left neck mass associated with severe posterior neck pain and associated tension headaches. She had no prior neck trauma or surgery. Examination revealed a large firm, tender, and mildly mobile mass involving the left posterior neck, largely confined to level V, with no overlying skin changes. She had no motor or sensory deficits, though some restriction in head rotation to the ipsilateral side was noted secondary to guarding and mass effect. Written informed consent was obtained from the patient for participation in this report and publication of pictures. MRI with contrast at presentation demonstrated a 3.1 × 2.4 cm multicystic mass at the level of C2-3. The mass appeared to displace the adjacent levator scapula, longissimus capitis, and semispinalis capitis. The mass was isointense to muscle on T1-weighted images and with multiple internal septations and fluid-fluid levels on T2-weighted images. There was no apparent atrophy of the ipsilateral paraspinal muscles. Both the mass and surrounding soft tissues demonstrated avid enhancement. Five months prior to presentation, outside MRI and CT angiogram demonstrated a 2.5 × 2.1 cm mass, isointense to muscle on T1-weighted images, enhancing, and without ossification. On F-18 Fludeoxyglucose (FDG) PET/CT, the mass showed marked FDG avidity consistent with ongoing metabolic activity, though small areas of hypometabolism were present centrally. Egg-shell mineralization of the mass periphery was noted on CT angiography. The medial margin of the mass closely approximated, but did not abut, the left vertebral artery. Prior outside biopsy revealed skeletal muscle and was inconclusive.
The patient was evaluated by otolaryngology – head and neck surgery, endocrinology, orthopedic spine surgery, neuroradiology, and radiation oncology teams. Fluorescence in situ hybridization (FISH) of the prior neck mass biopsy was performed and positive for USP6 gene rearrangement; USP6 gene rearrangement was also evident on repeat biopsy following consultation. This finding and imaging characteristics were compatible with either myositis ossificans (MO) or STABC. To assess maturity of the ectopic skeletal mass and optimize timing of surgical resection, bone alkaline phosphatase levels were assessed and a nuclear medicine (NM) bone scan with technetium Tc-99m medronate was performed. These demonstrated a downward trend with normalization of bone alkaline phosphate levels and low blood flow suggestive of near-maturity of the mass. Due to persistent growth of the lesion to 5.2 × 4.8 cm and continued pain 4 months following presentation, surgical resection was recommended. The patient underwent CT angiogram due to the proximity of the vertebral artery to the mass; the vertebral artery was uninvolved, and coil embolization was performed preoperatively after adequate balloon occlusion testing.
Left neck exploration and resection of the paraspinal mass was performed by otolaryngology and orthopedic spine surgery teams. A horizontal neck incision was made extending from near midline to the occiput. Neck dissection was performed with identification and preservation of spinal accessory nerve in neck levels IIb and V. The mass was found to be well-circumscribed in the paraspinal muscles with limited involvement of surrounding structures. The great vessels were dissected superiorly to the skull base to ensure they were uninvolved by the mass. The mass was then resected with sharp dissection and coblation from levels IIb and Va. A segment of the embolized vertebral artery was clipped, transected, and included with the specimen.
The pathology specimen was consistent with an STABC. The patient had a significant improvement in her neck pain postoperatively. She received 3000 cGy radiation to the operative bed in 15 fractions beginning 5 weeks after surgery. She had no recurrence clinically 8 months following the completion of radiation therapy. Her pain resolved; however, she did report residual neck stiffness, for which she was undergoing physical therapy, and lymphedema as a result of her treatment.
Discussion
This case exemplifies the imaging characteristics of an STABC, a neoplasm infrequently encountered in the head and neck. The imaging features seen in this case, though striking, are non-specific and are shared by more sinister entities. As such, such lesions typically required tissue sampling to rule out more aggressive malignancies.
For example, extraskeletal osteosarcomas are characterized by a variable amount of ossification. In contrast to STABCs, the observed ossification is usually centrally located and lacks well-defined peripheral mineralization on CT imaging. 12 However, some extraskeletal osteosarcomas—classically telangiectasia osteosarcomas—demonstrate intralesional fluid-fluid levels, similar to those seen in this case. 3
MO, like STABC, can also demonstrate substantial peripheral ossification. A form of heterotopic ossification (HO), MO is a benign process which can be present on CT imaging with coarse peripheral ossification and often with a history of prior trauma or surgery in the affected area.3,13 For the neuroradiologist, a few features would support a diagnosis of STABC over MO: thin peripheral mineralization on CT, a multilocular cyst with septations, and fluid-fluid levels on MRI. 3 These features, while not always present, support intervention compared to MO, a classic “do not touch” lesion. Additionally, one should consider the expected evolution of MO with increasing thickness of the ossified shell, cessation of growth around 2 months, and possible involution over 6 months. 3 Continued eggshell-thin peripheral mineralization and growth would be more suggestive of STABC on follow-up imaging, though the natural history of STABC has not been thoroughly elucidated. In our case, growth was demonstrated 4 months following initial presentation (and 9 months following initial imaging), prompting surgical intervention.
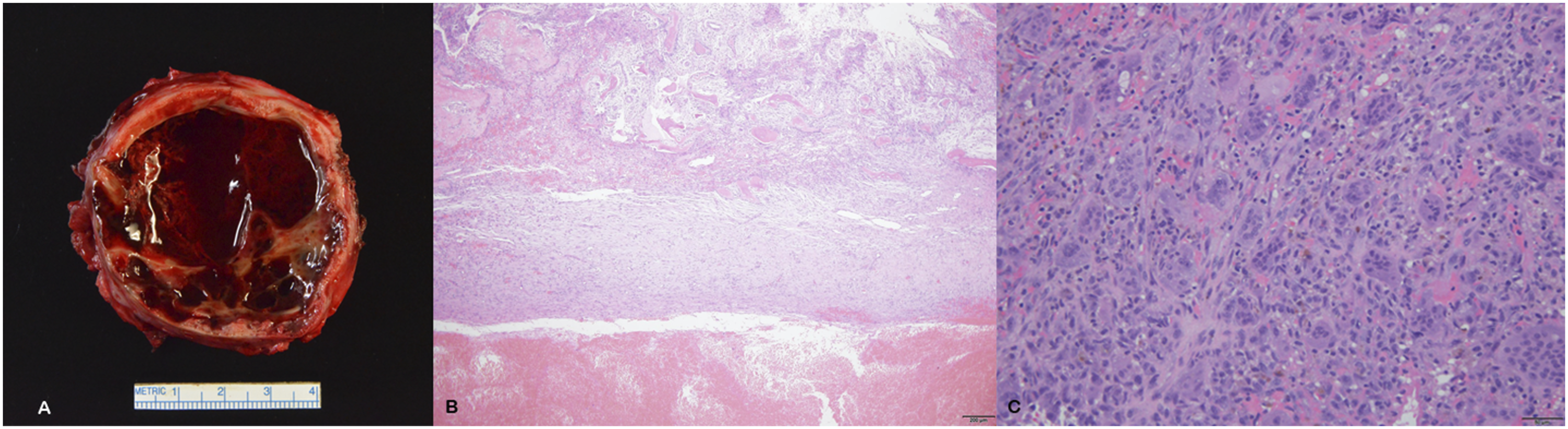
STABC and MO can most definitively be distinguished on histopathology. Macroscopically, STABCs have a multilocular cystic appearance and are filled with hemorrhagic debris. Microscopically, the fibrous septa and cyst wall consist of a cellular mixture of blood vessels, inflammatory cells, multinucleated osteoclast-type giant cells, and red blood cells that can mimic inflammatory granulation tissue (Figures 1–3). A shell of reactive bone is usually present at the inner surface of the lesion.
14
In comparison, MO demonstrates a characteristic zonal pattern with a central soft tissue area corresponding to immature fibroblasts, myofibroblastic tissue, and hemorrhage; an osteoid intermediate layer; and a hard peripheral ossified shell. The outermost layer consists of mature bone, with the amount and thickness corresponding to the age of the lesion.
15
In this case, a diagnosis of STABC was made on histopathology due to the gross multilocular hemorrhagic appearance, lack of strictly demarcated zonation pattern, and presence of osteoclast-type multinucleated giant cells. Preoperative imaging evaluation of cervical calcified mass. At the time of presentation, the 3.1 x 2.4 cm left cervical T1 isointense mass demonstrated avid enhancement of both the mass and surrounding soft tissue on post-gadonlinium T1-weighted images (a). Intralesional fluid-fluid levels (white arrows) were evident on T2 sequence (b). On subsequent CT angiography (c), thin mineralization consistent with ossification was noted along the periphery of the lesion, which closely approximated the left vertebral artery (black arrow). Peripheral ossification of the mass was confirmed on AP cervical spine X-ray (d) at the levels of C2-3. NM bone scan displayed low-level intralesional blood flow (e) and blood pooling (f) tracer uptake, with intense peripheral tracer uptake on delayed-phase images (g). A small focus of tracer near the right clavicle was felt to be related to injection artifact (curved white arrows; e andf). Surgical findings in wide local excision of paraspinal STABC. Intraoperative view (A) of left neck level V demonstrating the mass in situ (*). Prior to excision of the mass, the vertebral artery was ligated and divided (v and v’) (B). scm, sternocleidomastoid muscle; ejv, external jugular vein; tr, trapezius muscle; lo, lesser occipital nerve; tp, transverse process of C2. Pathological and genetic evaluation of STABC. (a) Macroscopic picture of the sectioned specimen, revealing an outer osseous rim and a central cavity filled with sanguineous fluid and fibrous septae. (b) Hematoxylin and eosin (H&E) low-power microscopic image showing the blood-filled cavity (*) and the fibro-osseous wall of the cyst (†). (c) Hematoxylin and eosin (H&E) high-power microscopic image showing multinucleated osteoclast-type giant cells (white arrows) intermixed with spindle cells in a fascicular conformation (black arrows), along with red blood cell pooling.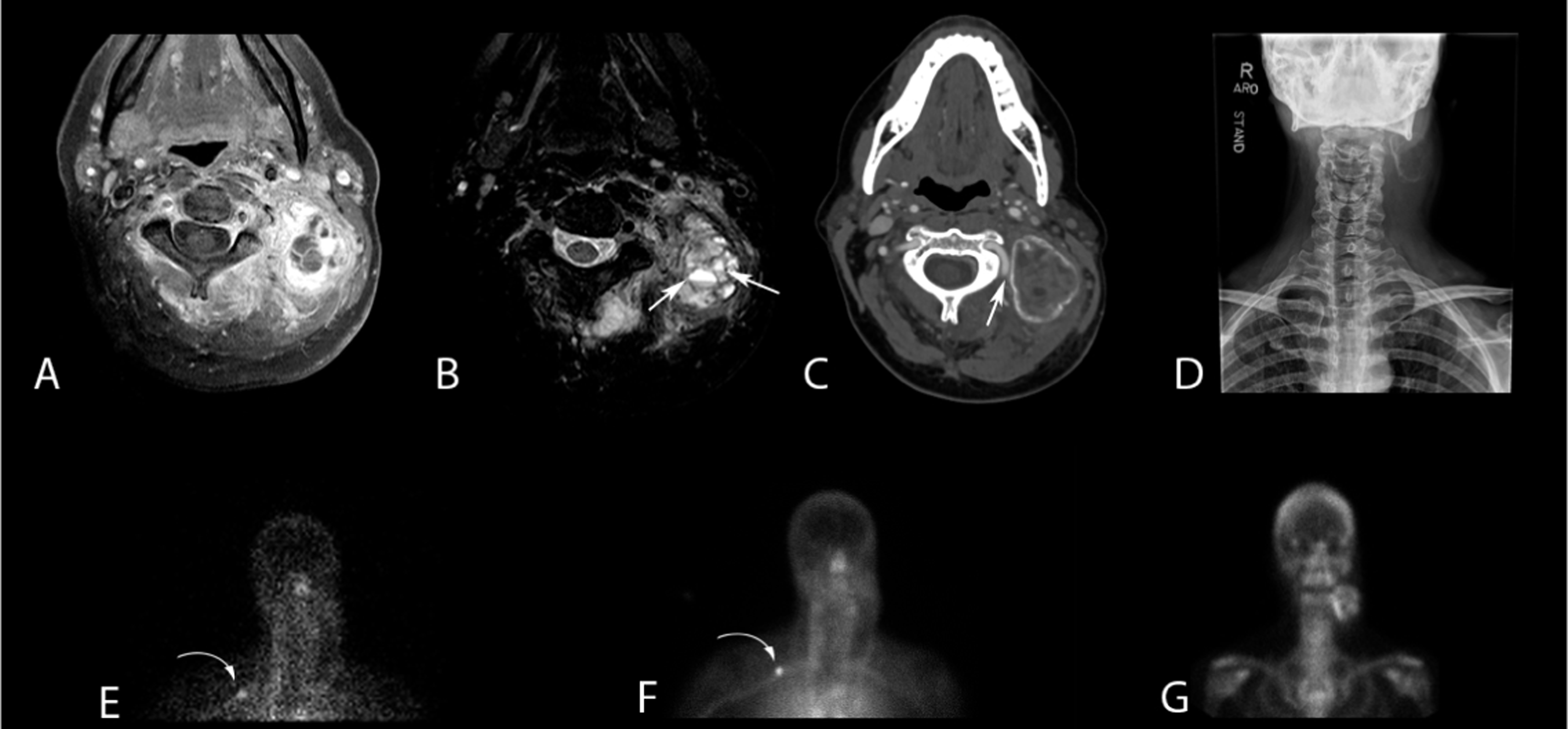

The distinction of MO and STABC is important, as the primary management for MO is watchful waiting. 3 The natural history of MO suggests maximum size occurs after 2 months, and lesion maturation occurs over 5–6 months, with possible involution. 4 Fine-needle aspiration or core biopsy may facilitate histopathologic and molecular analyses, though this may not be specific. 2 Rearrangement of USP6 has been found in ABC, STABC, MO, and nodular fasciitis.2–4,16 Ten of eleven STABCs undergoing next-generation sequencing or RNA sequencing in the literature had a fusion of USP6 and COL1A1 (collagen alpha 1 polypeptide chain), a gene implicated in Ehlers-Danlos, osteogenesis imperfecta, and other inherited disorders of bone metabolism.3,4,17 In the remaining case, a novel fusion of USP6 and ANGPTL2 (angiopoietin-related protein-2), a pro-inflammatory, and pro-angiogenic gene was identified. 4 The promoter regions of COL1A1 and ANGPTL2 are likely responsible for the upregulation of USP6, 4 which transcribes matrix metalloproteinase and promotes inflammation, angiogenesis, and matrix degradation. 16 Both cases of head and neck STABC undergoing USP6 FISH testing were positive for rearrangement, and fusion with COL1A1 was identified in the only case analyzed with RNA sequencing. 4 COL1A1-USP6 fusion genes have also been found in MO, though DH11 and MYH9 are the most common USP6 fusion partners in skeletal ABC and nodular fasciitis, respectively.3,18 Thus, neither the discovery of USP6 rearrangement on FISH nor USP6-COL1A1 fusion is helpful in distinguishing STABC and MO.
STABC management guidelines, especially in the head and neck, are limited due to its low incidence. Given the infrequent differentiation of STABC from MO and HO preoperatively, HO management recommendations are salient when considering treatment options for STABC. Most authors recommend waiting until maturation of the calcified lesion before intervention occurs in an effort to reduce the risk of recurrence. 13 Shebab et al. describe the ideal surgical candidate with HO fulfilling the following criteria: functional limitation (e.g., reduction in joint range of motion); lack of swelling, fever, or erythema suggestive of ongoing lesion activity; normal serum alkaline phosphatase; and normal or near-normal bone scan findings. 19 However, in the presence of intolerable symptoms, functional deficits, or uncertainty regarding the diagnosis, earlier intervention can be considered. Maturity can be assessed by resolution of perilesional edema on MRI 3 and decrease in flow and blood-pool activity on NM bone scan. 19 Though alkaline phosphatase levels are not reliable predictors of maturity of HO, a normal value can be supportive of maturity and helpful in timing surgical intervention. 19
Management of STABC is biased towards surgical resection, as the definitive diagnosis usually follows open resection. 2 Indeed, with a mean size of 5.3 cm (range 2–12 cm) among 43 reported cases,3,4 surgical resection is likely indicated due to impact on function or cosmesis. Surgical planning should include preoperative imaging. STABC of the head and neck may require angiography to assess involvement of vasculature—as in the current case and that of Petrik et al. 7 —or upper aerodigestive evaluation. 8 With the present case, preoperative embolization of the vertebral artery by interventional radiology and multidisciplinary surgery teams were critical in navigating the spine and surrounding neurovascular structures. The tumor itself involved the surrounding paraspinal muscle but was not adherent to nerves or vessels, though involvement of critical structures in the head and neck has been reported.7,8 Physical therapy should be initiated in the postoperative period for tumors with significant cervical musculature involvement.
Recurrence of surgically resected STABC is low, with 2 of 36 (5.5%) cases in the literature experiencing recurrence. 3 Both of these recurrences followed initial incomplete excision. Nonetheless, radiation therapy has shown efficacy in local control of ABC with local recurrence rates ranging from 9 to 45% for surgery alone compared to 0%–17% for surgery with adjuvant radiation therapy. 20 Radiotherapy alone can be used successfully in the treatment of ABC not amenable to surgical resection. Recurrence rates for radiotherapy doses of 26–30 Gy range from 0 to 10%.20–23 However, use of radiotherapy, either primary or in the adjuvant setting, must be weighed against the side effects of radiation therapy. Recurrence did not occur in any of the five head and neck STABC reviewed (mean follow-up, 13 months), with only the current case receiving radiation therapy.
Conclusion
STABCs are rare, soft tissue neoplasms containing peripheral ossification and must be distinguished from both MO and extraskeletal osteosarcoma. The overlapping radiologic, histopathological, and molecular features between STABC and MO make these entities particularly challenging to differentiate. Neuroradiologists should consider STABC in the differential of ossifying soft tissue lesions with eggshell-thin peripheral ossification, multicystic appearance with fluid-fluid levels on MRI, and continued growth beyond 2 months. Surgical resection may be indicated for suspected STABC, compared to initial observation for MO.
Footnotes
Author contributions
Drafting of original manuscript: SAC, JCB, MAN, KC, and KMV. Review and acquisition of pathology images: JJG, KC, and KBG. Critical review and revisions: SAC, JCB, MAN, KC, JJG, KBG, LMG, RAW, RJP, PSR, and KMV.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.