
Abstract
Keywords
Introduction
Brachiocephalic steal is a rare phenomenon that can occur in patients with steno-occlusive disease of the proximal brachiocephalic artery, resulting in hemodynamic insufficiency of downstream carotid and vertebral arteries, as well as the peripheral arteries of the arm. The development of clinical symptoms suggests advanced steno-occlusive disease, with luminal stenosis exceeding 50%. 1 The presence of neurological symptoms depends on multiple factors including functional demand, presence of functional collaterals, and comorbid cerebrovascular disease. 2 In contrast to subclavian steno-occlusive disease, which primarily affects ipsilateral vertebral artery flow, brachiocephalic disease additionally impairs hemodynamics of the ipsilateral carotid artery. In fact, severe brachiocephalic disease may drive retrograde flow through the carotid artery into the peripheral arterial system, resulting in hemodynamic insufficiency of the right hemisphere and increased risk of subsequent infarction. Flow deceleration or complete reversal puts patients at risk for both hemispheric and posterior fossa events. 3
Brachiocephalic artery stenosis, however, rarely results in right hemispheric infarction, with few cases reported of successful treatment. 4 Medical management of atherosclerotic brachiocephalic disease generally targets prevention of cardiovascular disease progression by following guideline-directed therapy of atherosclerosis and risk factor modification. Endovascular or surgical treatment may be indicated in symptomatic patients refractory to medical therapies. The main transthoracic surgical approach to revascularization is the placement of a prosthetic extra-anatomic bypass graft. 5 The indications for such interventions are controversial, with studies demonstrating that many patients with radiographic evidence of stenosis do not require treatment. Individualized treatments focusing on hemodynamic data are therefore critical in tailoring treatment approaches. Impaired cerebral blood flow as measured by quantitative magnetic resonance angiography (QMRA) has been shown to be a predictor of recurrent stroke in patients with intracranial atherosclerotic disease. 6 In our case, we used various hemodynamic imaging techniques, including QMRA, single-photon emission computed tomography (SPECT), and CT perfusion to understand the local and tissue level hemodynamics in a patient with brachiocephalic and middle cerebral artery (MCA) occlusion. 2 This multimodal imaging approach, along with collaboration across multiple medical specialties, allowed for a precise and targeted treatment plan.
Case presentation
A 61-year-old right-handed woman who is an active smoker, with a medical history of hypertension, hyperlipidemia, and right extracranial internal carotid artery (ICA) stenosis was evaluated in the emergency department for acute left facial droop upon awakening. The patient also reported a chronic history of intermittent right arm weakness, which was exacerbated by overhead activities at work, and was found to have a systolic blood pressure discrepancy of 46mmHg between her upper extremities. There was no prior history of strokes or transient ischemic attacks. On admission, neurological exam was unremarkable other than left facial droop (National Institutes of Health Stroke Scale (NIHSS) of 1). CT head did not demonstrate early ischemic changes. CT angiogram revealed a right MCA M1 occlusion and critical stenosis of the proximal brachiocephalic artery (Figure 1, Image A). CT perfusion demonstrated a Tmax >6 s delay of 41 mL and hypoperfusion intensity ratio (HIR) of 0, suggestive of robust leptomeningeal collaterals (Figure 1, Image B).7,8 The patient was out of the window for tenecteplase administration and thrombectomy was deferred due to a low NIHSS. Diffusion-weighted magnetic resonance imaging (DWI) of the brain showed a right putamen and corona radiata infarction (Figure 1, Image C). Digital subtraction angiography (DSA) demonstrated crossed collateralization across the anterior cerebral artery (ACA), as well as robust right ACA-MCA and posterior cerebral artery (PCA) to MCA leptomeningeal collaterals and retrograde filling of the brachiocephalic and right common carotid artery via the right vertebral artery (Figure 1, Images D, E). These findings were supported by QMRA, which revealed decreased blood flow in the right ICA, increased flow in the right A2 and left A1, and retrograde right vertebral flow indicative of a brachiocephalic steal phenomenon (Figure 1, Image F). Pre-operative QMRA also confirmed the absence of flow in the right MCA. Pre-operative SPECT with acetazolamide challenge demonstrated markedly diminished activity in portions of the right temporal, frontal, and parietal lobes following acetazolamide administration, indicative of very poor cerebrovascular reserve and intracerebral steal phenomena in the distribution of the right ICA (Figure 2, Image A). The patient’s neurological exam remained stable throughout her pre-operative hospital course. The patient did not develop any new symptoms, including signs of vertebrobasilar insufficiency, at any time during the hospital stay. (a) CT angiogram showing right MCA M1 occlusion. (b) CT Perfusion. (c) DWI showing right putamen and corona radiata infarct. (d) Left ICA injection showing robust leptomeningeal and crossed collaterals. (e) Left vertebral injection demonstrating robust retrograde filling of right vertebral artery and subsequent filling of brachiocephalic and right common carotid artery. (f) Quantitative MRA supporting robust collateralization and brachiocephalic steal phenomenon. (a) Pre-Operative SPECT demonstrating diminished flow in the right hemisphere. (b) Post-STA-MCA bypass SPECT revealing improved flow in the right hemisphere.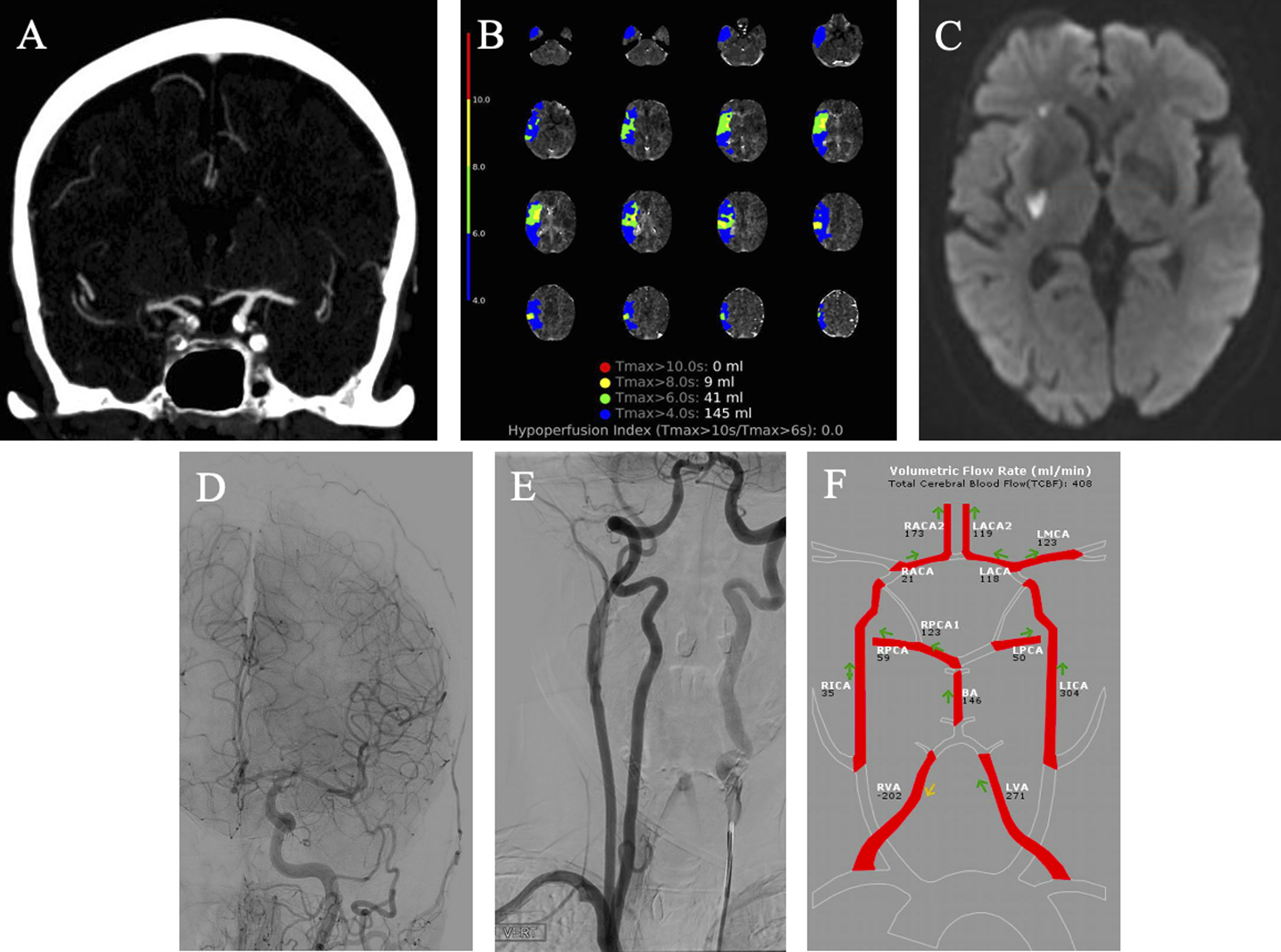
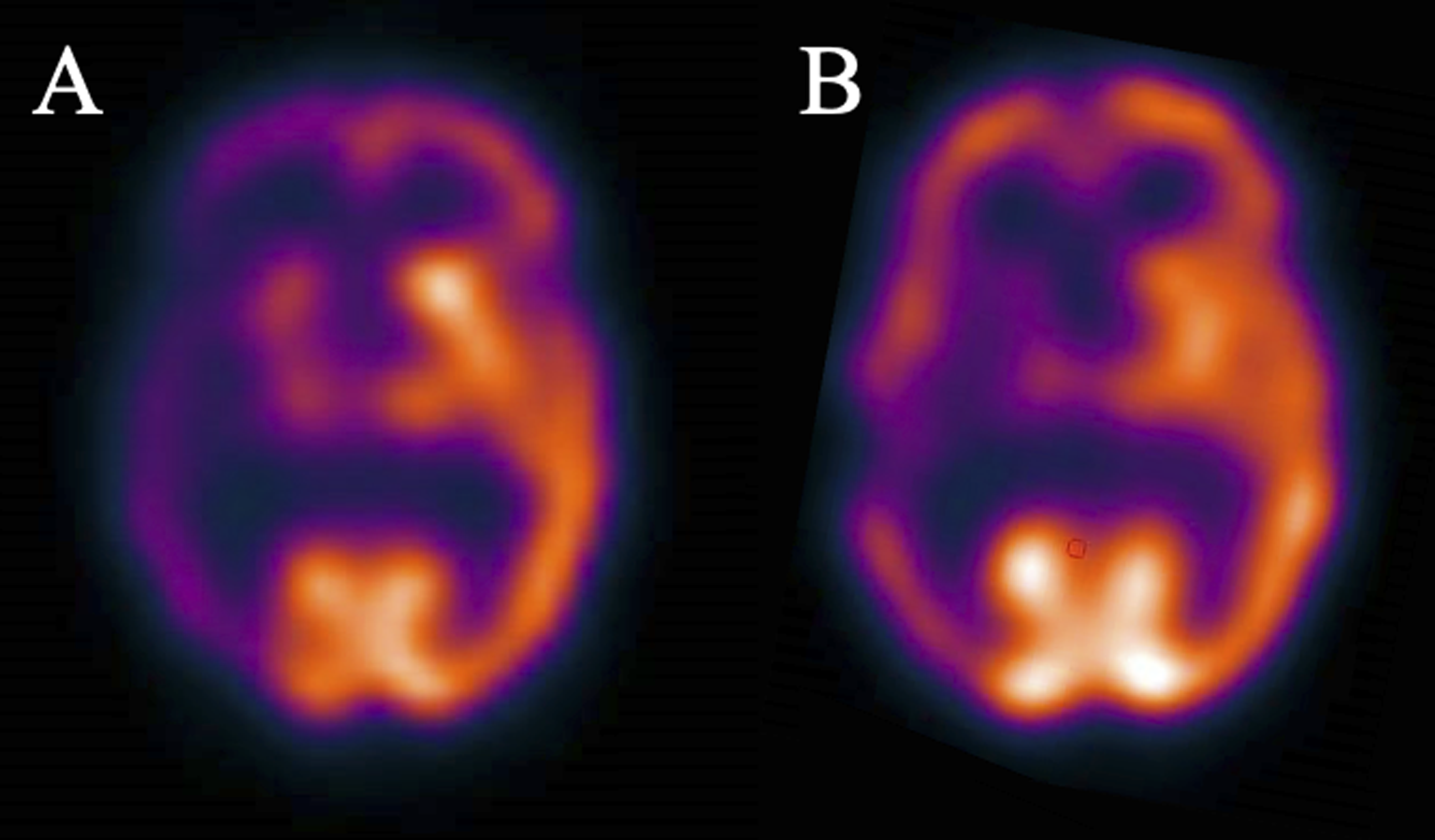
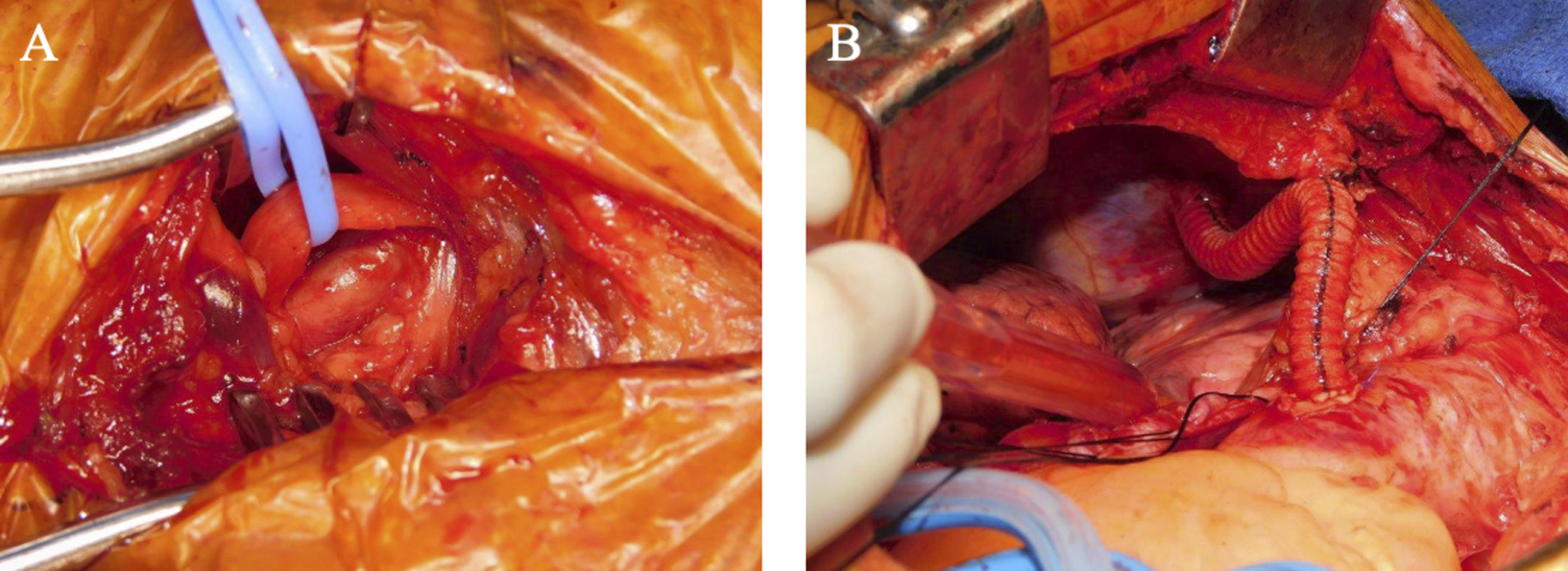
Given the symptomatic nature of this patient’s brachiocephalic stenosis, resulting in arm weakness and claudication, as well as radiographic evidence of hemodynamic insufficiency and poor cerebral vascular reserve, the decision was made to forego conservative management with dual antiplatelet therapy and risk factor modification and instead, two staged bypass procedures were planned. To protect against subsequent ischemic stroke, and hemodynamic insufficiency that may be provoked by the anticipated brachiocephalic procedure, she first underwent a right superficial temporal artery (STA) to right MCA bypass. Post-operative QMRA demonstrated bypass patency with a flow velocity of 20 mL/min and improved flow signal in the right MCA M1 and M2 branches (Figure 3, Image B). Post-operative SPECT revealed improved flow in the right hemisphere (Figure 2, Image B). Nine days later, the patient received a synthetic bypass from the aorta to the right subclavian artery (Figure 4). Post-operative QMRA demonstrated that right ICA flow increased from 35 mL/min to 251 mL/min (Figure 3, Image C). Pre-operative right carotid flow had been significantly diminished due to primary blood supply originating from retrograde flow in the right vertebral artery. Right external carotid artery flow also increased post-subclavian bypass, further improving flow through the STA-MCA bypass to 39 mL/min (Figure 3, Image C). We expect flow through the bypass to continue to improve over the upcoming months. (a) Pre-Operative Quantitative MRA supporting robust collateralization and brachiocephalic steal phenomenon. (b) Quantitative MRA post-MCA-STA bypass. (c) Quantitative MRA post-subclavian-aorta bypass. (a) Nerve bundle looped and right subclavian vein retracted inferiorly, exposing the right subclavian artery. (b) View of aorto-right subclavian bypass through the right chest, with enough laxity to allow for lung expansion.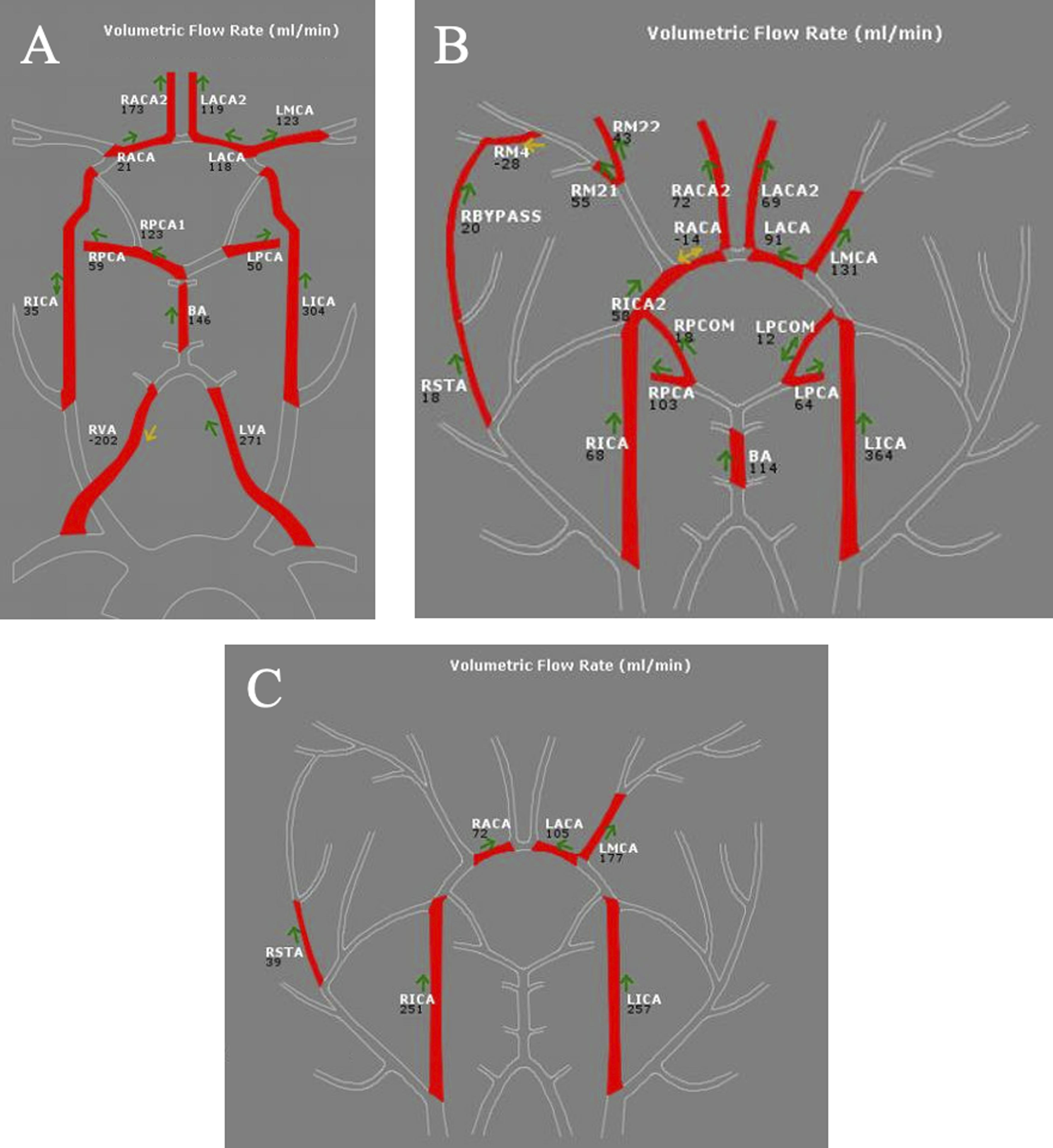
Eleven days after the aorta-right subclavian bypass, the patient underwent a cranial wound revision with debridement of scalp and subcutaneous necrosis. The patient recovered well from the scalp reconstruction, and post-operative course was otherwise unremarkable. Other than mild left facial droop, she did not experience any neurological or upper extremity symptoms between the day of her initial presentation and discharge. The patient was discharged seven days after her scalp reconstruction.
Discussion
Brachiocephalic steal is a rare phenomenon that presents with various hemodynamic abnormalities. Clinical presentation in symptomatic patients ranges from right arm weakness on exertion to recurrent TIAs and cerebrovascular insufficiency. 9 This report highlights a unique case of minimal neurological symptoms in the setting of brachiocephalic steal with concurrent MCA occlusion. Case reports have demonstrated concurrence of brachiocephalic occlusion with additional extracranial occlusion. 10 However, to our knowledge, performing two staged bypass procedures for brachiocephalic stenosis with concomitant intracranial occlusion has not yet been reported.
In this case, STA-MCA bypass was performed prior to aorta-right subclavian bypass. There are no current guidelines or evidence regarding the most efficacious order in which extracranial-intracranial and thoracic bypasses should be performed. For our patient, STA-MCA bypass was performed first to supplement cerebral perfusion and decrease the likelihood of a hypoperfusion event during the aorta-right subclavian bypass surgery.
Initial management of complex steal phenomena involves imaging focused on cerebral perfusion, as stroke prevention is the primary focus of treatment. QMRA has emerged as an important tool in risk stratification and evaluation of hemodynamics. The Vertebrobasilar Flow Evaluation and Risk of Transient Ischemic Attack and Stroke (VERiTAS) study demonstrated significantly increased stroke risk in patients with low flow states distal to the site of stenosis on QMRA. 11 However, this study focused on vertebrobasilar circulation. Further research is necessary to elucidate the impact of decreased flow on QMRA on stroke risk in steal phenomena.
Regarding its use in the evaluation of hemodynamics, QMRA has demonstrated potential as a valuable diagnostic tool. Nevertheless, more studies are required to better characterize its role in understanding cerebral flow dynamics and guiding treatment. 7
Operative management of brachiocephalic stenosis is highly dependent on operator experience. 12 In this case, a bypass graft was successfully used; however, many reports have found success with endovascular approaches. Percutaneous transluminal angioplasty (PTA) has been shown to have a success rate above 90%, with complication rates under 4%. 13 However, patency rates 2 years after PTA have been demonstrated to be as low as 67% in patients without stent placement and 83% in patients with stent placement. 14 Meanwhile, carotid-subclavian bypass for brachiocephalic stenosis has shown patency rates as high as 100% at 5 years, when arterial transposition is used. 15 Overall, it is important to consider patient characteristics, institution resources, and operator experience when determining management.
The major limitations of this report include its poor external validity and the lack of accepted thresholds defining hemodynamic compromise. This patient had a highly unique presentation of concurrent right MCA and proximal brachiocephalic occlusion. Due to the hemodynamic variability in patients with steal phenomena, surgical management of these patients is often heavily individualized.
Conclusions
We report a patient who presented with very mild symptoms and clinical stability despite severe concomitant occlusion of the right MCA M1 and proximal brachiocephalic artery, likely caused by ischemic conditioning related to chronic hypoperfusion. Through the use of STA-MCA bypass and aorta-right subclavian bypass, the patient had successful restoration of intracranial and extracranial hemodynamics, as demonstrated on QMRA and SPECT. Further research to elucidate the role of perfusion imaging and surgical management in mildly symptomatic patients with complex steal phenomenon and multi-vessel atherosclerosis is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.