
Abstract
Introduction
Traumatic brain injury (TBI) is a leading cause of disability and mortality worldwide, with epidural hematoma (EDH) being a severe consequence. This study focuses on identifying factors predicting EDH volume changes in TBI patients and developing a machine learning (ML) model to predict EDH expansion.
Methods
The study includes patients with traumatic EDH between 2019 and 2021. Data were gathered from CT scans performed at the time of admission and 6 hours later, and subsequently analyzed. The data was divided into three cohorts: all cases, adults, and pediatrics. To predict EDH volume changes, we used Logistic Regression (LR), Random Forest (RF), XGBoost, and K-Nearest Neighbors (KNN) models. Data was divided into an 80% training set and a 20% test set. Through a rigorous process of parameter optimization and K-fold cross-validation, focusing on the area under the receiving operating curve (AUROC), we identified the best models in all cohorts. The best models were evaluated on the test sets, reporting AUROC, recall, precision, and accuracy using the youden index threshold.
Results
Results show that age, initial EDH volume, swirl sign, intra-hematoma air bleb, contusion, otorrhagia, subarachnoid hemorrhage, location, and other side extra-axial hematoma have significant effects on changing EDH volume. Based on test AUROC, the best models were RF for adults (82.4%), KNN for pediatrics (90%), and LR for all cases (81.6%).
Discussion
In this study, we identified key features for predicting EDH expansion as well as developing ML models. Using high sensitive models, can assist clinicians in identifying high-risk patients early. This allows for enhanced monitoring and timely intervention, improving patient outcomes by facilitating quicker decisions for follow-up imaging or treatment.
Introduction
Traumatic brain injury (TBI) is one of the most common causes of disability and mortality and a major public health and social problem in most countries. 1 Epidural hematoma (EDH) is a significant consequence of traumatic brain injury. 2
EDH is a life-threatening situation with high mortality rates which requires urgent intervention. 3 It occurs in approximately 10% of the patients with TBI who need hospitalization. 4 An EDH can be caused by different traumatic mechanisms such as motor vehicle accidents, falling down, and assault trauma. 4 It occurs in approximately 8% of the patients with TBI. 5
The incidence of EDH is higher in adolescents and young adults, and it occurs more frequently in males compared to females. The average age of the patients is from 20 to 30 years, and infrequently it occurs in people older than 50 to 60 due to the adherence of the dura to the cranial bone. 4
If an EDH suddenly develops, patients’ conditions can deteriorate quickly, potentially leading to severe neurological complications or even death. 6 Observation of a new EDH or an increase in size during the subsequent computerized tomography (CT) compared to the findings of the initial CT indicates the presence of progressive EDH (PEDH) which warrants surgical interventions. 7 On the other hand, sometimes, the EDH volume reduces, and the patient is managed conservatively.
Several radiologic and clinical features are known to have significant effects on EDH volume changes.7–13 These features assist in predicting EDH volume changes after the initial CT scan. Although previous studies have been designed to predict hematoma volume changes, none specifically focused on EDH.14,15 Given the specific behavior and management of EDH, the lack of studies aiming to predict its volume changes is notable.
This study aims to determine the predicting factors for an EDH volume change evident in the brain CT images of TBI patients. Additionally, it seeks to build a machine learning (ML) model to predict EDH changes based on radiologic and clinical features.
Method
Study population
All patients with traumatic EDH between 2019 and 2021, considering the inclusion and exclusion criteria were included in this study. Patients followed-up 6 h after hospital admission to detect hematoma expansion. All enrolled cases were imaged just after admission and 6 h after hospitalization.
Inclusion and exclusion criteria
The inclusion criterion was the radiologic evidence of EDH in the brain CT images that was confirmed by a neurosurgeon.
The exclusion criteria were patients who expired in the emergency department (ED) before a CT scan and those who needed the operation based on the first CT scan or clinical conditions. Operation indications were volume >30 mL, focal neurological deficit which can be due to EDH, GCS <9 with midline Shift ≥5 mm or thickness ≥15 mm, and increasing intracranial pressure for all types of EDHs (single, multiple, ipsilateral, and bilateral EDH). Also, if GCS decreased, CT scan repeated and if hematoma expanded, patient went to operation room and exclude from study.
Ethical considerations
Permissions and a code of ethics were obtained from the ethics committee of Isfahan University of Medical Sciences before the study onset (ethical code: IR.MUI.MED.REC.1399.864). The objectives of the study were explained to the patients and their families (in the cases of unconsciousness), and written informed consent was obtained from all participants.
Data collection and imaging analysis
Each patient was evaluated after an initial CT scan and neurological exams. A control CT scan was performed 6 h after the first CT scan. All of the images were collected and finally assessed by a neurosurgeon, and the dimensions of the hematoma in each CT scan were recorded. In the following as described by Kothari et al., to calculate the volume of an intracranial hemorrhage (ICH), one can utilize the following formula: A, which represents the maximum length in cm, B, which denotes the width perpendicular to A on the same head CT slice, and C, which signifies the number of slices multiplied by the slice thickness; the ABC/2 equation was used to calculate the hematoma volume with ml unit of measurement. Hematoma volume changes were defined as a proportional increase or decrease of more than 1 mL. 16 After these steps, patients were divided into two groups: one group with an increase in hematoma volume after 6 h, requiring neurosurgical intervention, and another group where the hematoma volume either decreased or remained unchanged, managed conservatively.
Statistical analysis
For analytical purposes, the data is divided into three cohorts: all cases, adults (patients aged 18 years and older), and pediatrics (patients under 18 years of age). Given the fact that all CT scans were reviewed by an expert neurosurgeon and also, the clinical variables were both easily obtainable and essential for completing the initial records, no missing data was identified. Finally, the data were analyzed using the SPSS software (version 24) at a significance level of 0.05. Kolmogorov–Smirnov test was used to assess data normality. Results were presented as frequency (percentage) or mean ± standard deviation. For quantitative variables, two tests were applied. In the first instance, the Kruskal-Wallis test was used. In the second instance, the quantitative variable was categorized, and then the Chi-square or Fisher’s test was performed on the categorized data. Categorical variables were analyzed using Chi-square or Fisher’s test.
Machine learning model
In this study, we utilized Logistic Regression (LR), Random Forest (RF), Extreme Gradient Boosting (XGBoost), and K-Nearest Neighbors (KNN) to predict changes in hematoma volume in all three cohorts. Cases were divided into an 80% training set and a 20% test set. To address the class imbalance, the Synthetic Minority Over-sampling Technique (SMOTE) was applied on the training set. Separate models were developed for each cohort to address physiological and clinical differences that could influence outcomes related to hematoma expansion. Each cohort was analyzed using a tailored set of ML algorithms, with model parameters optimized through grid search to best fit the distinct characteristics of each group. The efficacy of each algorithm was assessed through K-fold cross-validation (CV) (5-fold-CV for all cases and adults cohorts models, and 3-fold-CV for pediatric cohort models), focusing on the area under the receiver operating characteristic curve (AUROC). After identifying the most effective model, the optimal decision threshold was established based on the youden’s index. The best models were then evaluated on the test set, and their performance metrics were compiled.
The model incorporated a range of features, including patient age, sex, coagulation status (have impaired PTT or INR, using antiplatelet or anticoagulation drugs, thrombocytopenia), mechanism of injury, presence of cerebral contusion, Glasgow coma scale (GCS) score at admission, hematoma location, initial hematoma volume (ml), presence of a swirl sign, intra-hematoma air bleb, subarachnoid hemorrhage (SAH), presence of extra-axial hematoma on the other side (EDH, subdural hemorrhage and intraparenchymal hematoma not SAH due to low pressure effects), and otorrhagia on the same side (which suggests a fracture of the petrous bone) as the EDH. These features were aimed at predicting the primary outcome: the change in hematoma volume after 6 h.
Results
Characteristics of the patients
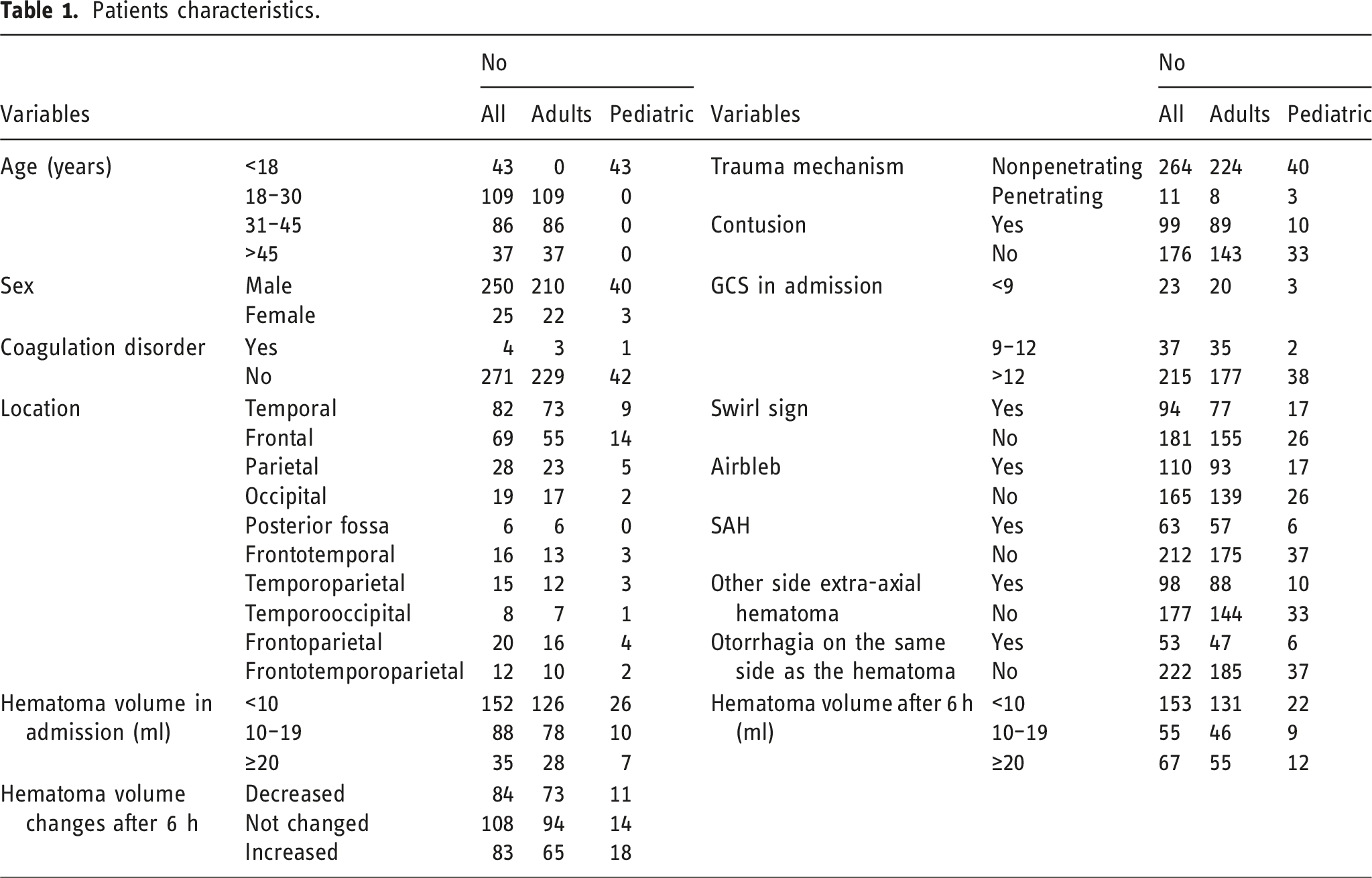
This study examined 275 cases of traumatic intracranial EDH. The mean age of the patients was 30.51 ± 13.37 years, and median age was 29 years, ranging from 2 to 69 years. 90.9% of the patients were male. Initial EDH volume was 9.47 ± 7.66 mL (range: 1–45 mL), and it increased to an average of 12.98 ± 14.74 mL (range: 0–90 mL) after 6 h.
Patients characteristics.
Prognostic factors
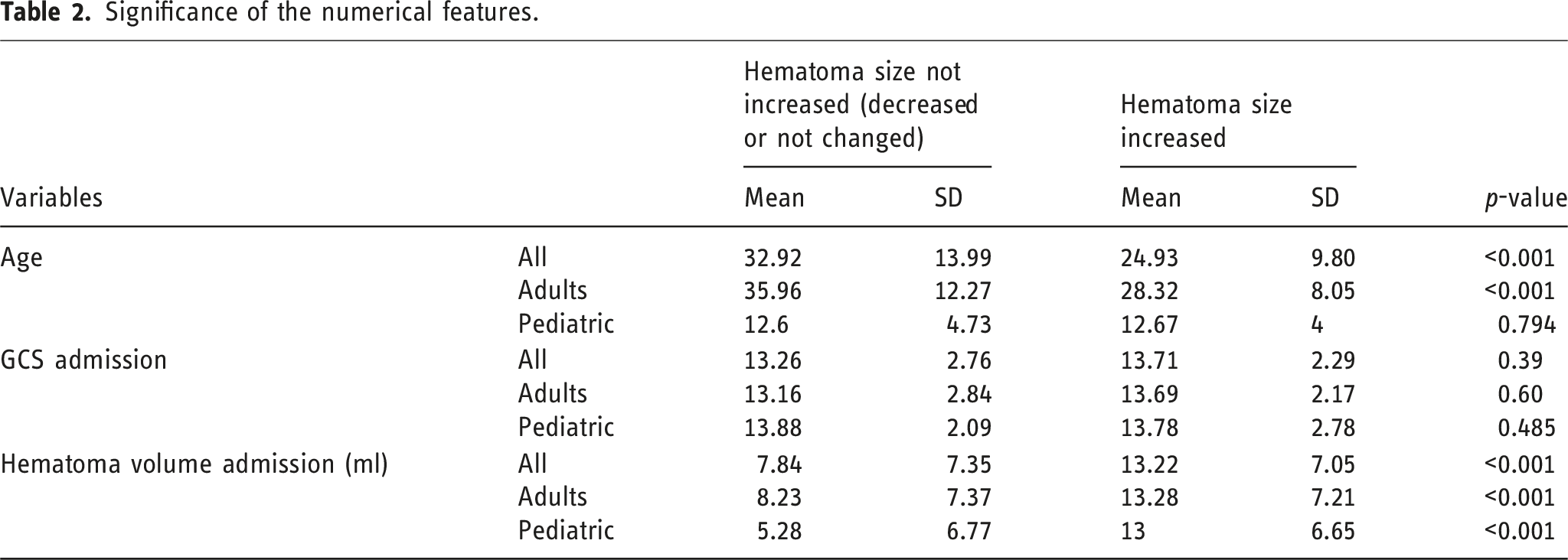
Significance of the numerical features.
Significance of the categorical features.
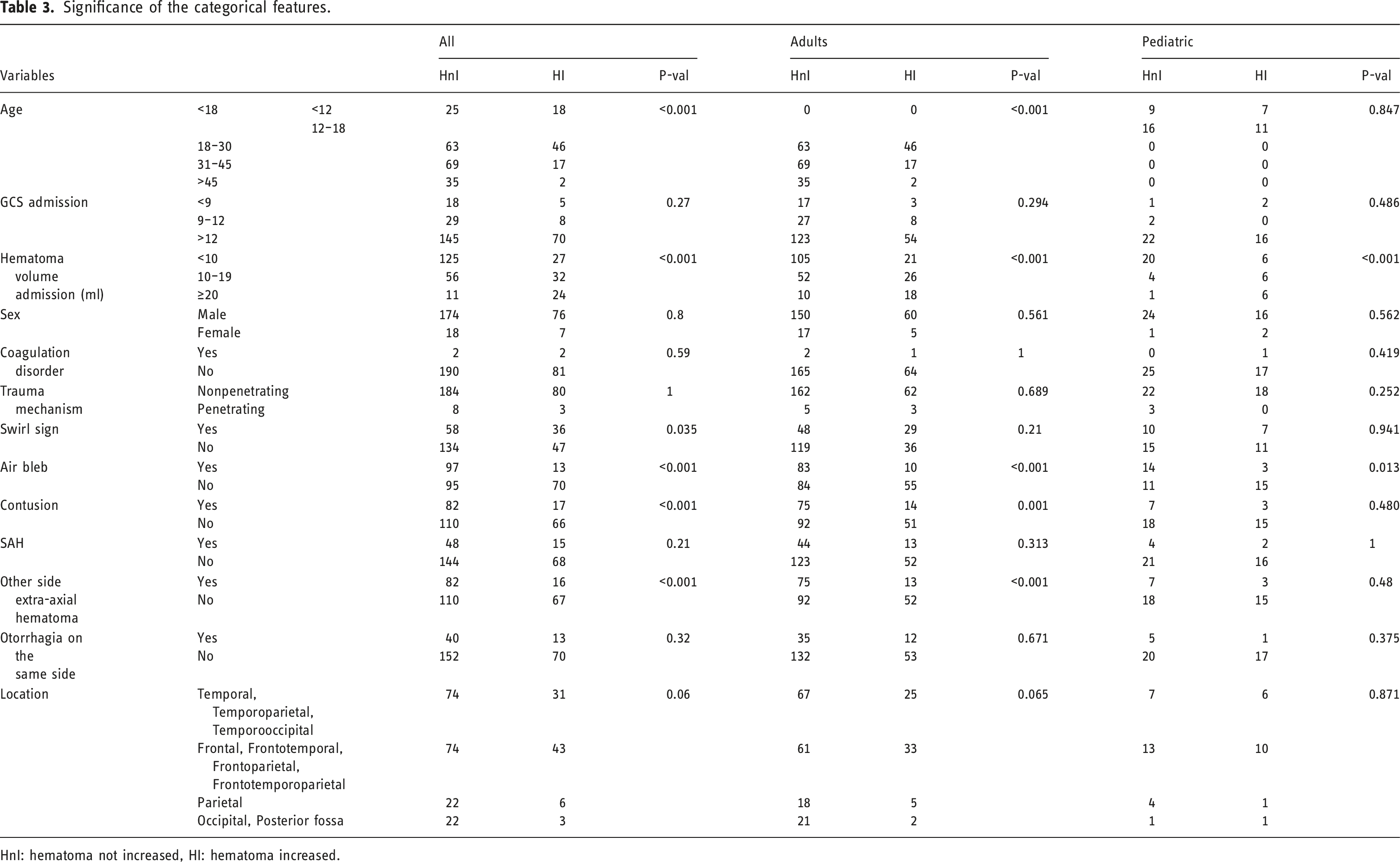
HnI: hematoma not increased, HI: hematoma increased.
In terms of other variables, no statistically significant differences were observed in EDH size changes across different sexes (p = .80, .561, .562), in patients with coagulation disorders (p = .59, 1, .419), or in those with varying mechanisms of trauma (p = 1.00, .689, .252). Similarly, SAH and otorrhagia on the same side were not significantly associated with changes in EDH size, with p-values of .21, .313, 1 for SAH and .32, .671, .375 for otorrhagia on the same side respectively. Also, the study did not find significant differences in EDH size changes when considering the location of the hematoma (p = .06, .065, .871).
To assess the impact of various factors on reducing EDH volume, we divided the data into two groups: one where the EDH size decreased and another where it remained the same or increased. Our analysis showed that older age was significantly associated with a greater reduction in EDH volume in the overall cohort and adult cohort (p = .019, .017). Also, lower GCS in all cases cohort have significant effect on EDH volume reduction (p = .024). Additionally, the presence of variables such as air blebs (p < .001), contusions (p < .001, .001), SAH (p = .016, .046), contralateral extra-axial hematoma (p < .001), and ipsilateral otorrhagia (p < .001, .004) were significantly associated with a reduction in EDH volume in both the overall cohort and adult group. Hematoma location also showed a significant correlation with volume changes in the overall and pediatric cohort (p = .024, .038). Additional details are provided in Supplemental Tables 1 and 2.
Prediction of EDH size change
Machine learning model results.
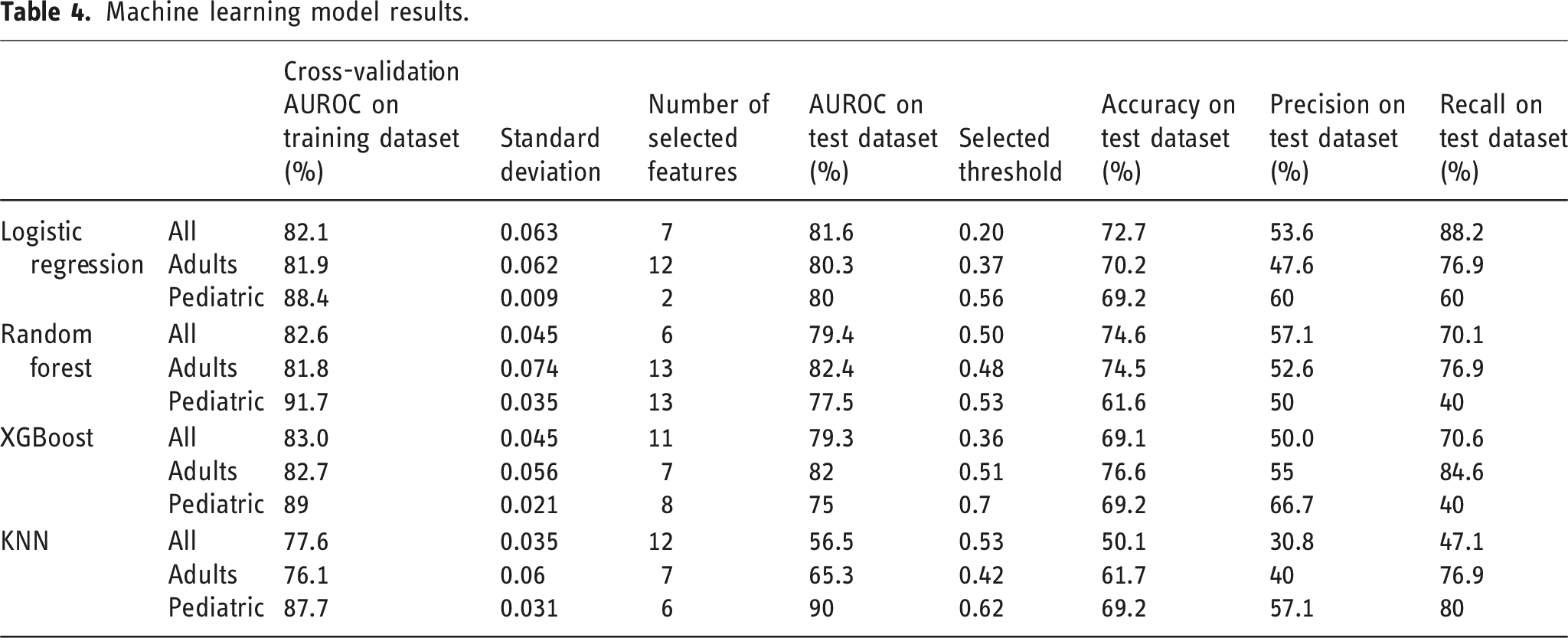
The RF model demonstrated the best performance for adult cohort, achieving a CV AUROC of 81.8% and a test AUROC of 82.4%, using 13 selected features. XGBoost also performed well, with a CV AUROC of 82.7% and a test AUROC of 82.0%, using 7 features. Notably, the standard deviation of the CV AUROC for XGBoost was lower compared to RF (0.056 vs 0.074). LR and KNN showed test AUROCs of 80.3% and 65.3%, respectively, with LR using 12 features and KNN using 7 features.
For pediatric cohort, the KNN model was the best performer, achieving a test AUROC of 90% with 6 selected features. The model’s CV AUROC was 87.7% with a standard deviation of 0.031, indicating stable performance. In comparison, the LR, RF, and XGBoost models achieved test AUROCs of 80%, 77.5%, and 75%, respectively, using 2, 13, and 8 features.
For the overall patient cohort, LR emerged as the top-performing model, with a CV AUROC of 82.1% and a test AUROC of 81.6%, using 7 selected features. The model’s CV standard deviation was 0.063. In comparison, RF, XGBoost, and KNN achieved test AUROCs of 79.4%, 79.3%, and 56.5%, respectively, with 6, 11, and 12 selected features.
Finally, based on test AUROC, best model for all cases, adults and pediatrics cohorts were LR, RF, and KNN.
Discussion
This study of 275 patients with EDH, showed that patients with lower age, higher hematoma volume after first CT scan, swirl sign in CT scan had more chance of increasing hematoma volume in the second CT scan after 6 h. Patients with higher age, lower hematoma volume after first CT scan, air bleb, otorrhagia on the same side as the hematoma, contusion, other side extra-axial hematoma, significantly had more chance of decreasing EDH volume.
In previous studies, various features have demonstrated significant effects on the expansion of EDH. For instance, Basamh et al. found that younger age and coagulation disorders are critical factors influencing the surgical approach for patients with EDH. EDH volume is not significantly different between surgery and no surgery groups which may cause a lack of adequate patients and heterogeneity in two groups (surgery: 14 patients, no surgery:111 patients). 8 In contrast, our study highlights that EDH initial volume significantly correlates with an increased likelihood of hematoma volume expansion. Chen, Hao et al. showed that skull fracture, time from injury to first CT, coagulopathy, and hypotension were significant variables that correlate with PEDH. 7 In our study, we considered coagulopathy as a variable which didn’t have significant effect on EDH volume; however, due to imbalanced data, the related results to this feature are not reliable. Kang et al. showed that the time interval between the trauma and the initial CT, as well as increasing blood pressure, were significantly associated with increasing EDH volume. 9 Wang, Ren et al. show skull fracture and Time from injury to first CT significant effects on EDH progression and it showed that EDH predominantly progresses within the first 6 h post-injury (60%); however, in 40% of cases, it transpires beyond the 24-h. 10 However, skull fracture and time from injury to CT variables were not included in our dataset, limiting our ability to directly compare these findings with our results. Additionally, the swirl sign’s presence in CT scans has been repeatedly shown in various studies to have a significant impact on patient prognosis.11,12 Existence of intradural air is correlated with hematoma volume expansion in pediatric patients. 13 Both the swirl sign and intra-hematoma air bleb significantly affected EDH volume in our results. The swirl sign was associated with an increased likelihood of EDH expansion. In contrast, the presence of intra-hematoma air bleb was linked to a reduced risk of EDH expansion. These factors collectively underscore the importance of early and repeated imaging in managing traumatic brain injuries, especially for tailoring individualized treatment strategies and improving patient outcomes.
This study identifies key effects of otorrhagia on the same side as the hematoma (which suggests a fracture of the petrous bone) on reducing EDH volume. Several hypothetical mechanisms may explain these correlations. The presence of a fracture, especially in the petrous bone, might allow blood to drain from an EDH, thus reducing its size. This is inferred from otorrhagia, indicating a possible escape route for blood. Additionally, air within the hematoma suggests a potential link between the brain and the outside, possibly through a fracture, leading to decompression of the EDH. These trauma-induced changes, including enhanced clot formation and altered intracranial pressure, could also contribute to the reduction in EDH volume. However, these are theoretical insights and warrant further research for confirmation.
In light of the discovery of multiple predictive variables for changes in the size of EDH and the significance of these changes on patient prognosis, it appears that predicting EDH size variations could be highly effective in patient management.
Predictive model
Previously, several articles have used ML models to predict hematoma expansion, but to the best of our knowledge, none specifically focused on EDH.14,15 Moyer JD et al. built an ML model to predict the need for emergency neurosurgery within 24 h after moderate and severe head injuries. Their dataset included 2159 cases, with 42% requiring neurosurgical intervention within 24 h, achieving an AUROC of 81% using the CatBoost technique. 17 In another study, Karabacak M and Margetis K used an ML model to predict in-hospital mortality of EDH patients, achieving AUROC values ranging from 0.874 to 0.956. This study also predicted non-home discharges (AUROC range: 0.776–0.798), prolonged length of stay (LOS) (AUROC range: 0.737–0.758), prolonged ICU-LOS (AUROC range: 0.712–0.774), and major complications (AUROC range: 0.674–0.733). 18
In our study, in adults cohort, RF model was the best predictor of EDH expansion, achieving a test AUROC of 82.4% and a CV AUROC of 81.8% with a standard deviation of 0.074 across 13 selected features. Although its performance was strong, the higher CV standard deviation than other models and inclusion of numerous features limit its clinical applicability. Additionally, some of these selected features appeared to have minimal relevance based on the results of previous statistical analysis in our study (Tables 2 and 3). While RF achieved the highest test AUROC, the XGBoost model may be more clinically valuable due to its use of fewer features and higher recall (76.9% vs 84.6%), enabling early detection and improved monitoring of high-risk patients.
For pediatric cohort, the KNN model performed well with a test AUROC of 90% and a CV AUROC of 87.7% using 6 selected features. However, the limited pediatric dataset (43 cases) reduces the reliability of these findings, necessitating further validation.
Overall, for all cases cohort the LR model was determined to be the optimal choice across all cases due to its superior test AUROC and recall metrics, along with an acceptable cross-validation AUROC and standard deviation. The model’s selected feature was robust, with all selected features showing significant associations with EDH volume changes (p-value <.05) based on the previous results in our study (Tables 2 and 3), supporting its clinical efficacy. With a recall of 88.2%, the LR model demonstrated excellent capability in identifying high-risk patients, making it a reliable option for early detection and intervention.
We support the implementation of models resembling these after undergoing additional refinement and external validation, using larger datasets in EDs. In this way we can identify high-risk patients for increased surveillance and expedited follow-up imaging, facilitating the early detection of EDH volume escalation without the need for additional interventions.
Despite the promising utility of ML models in this context, we maintain that they should not replace the need for a second CT scan. CT imaging remains the gold standard for assessing EDH and other pertinent conditions. Nonetheless, ML models, by forecasting changes in EDH volume, offer a valuable tool for identifying patients who are at elevated risk, thereby enabling more focused monitoring and earlier scheduling of subsequent CT scans. The integration of our ML model could support medical professionals in swiftly recognizing patients at increased risk, facilitating quicker intervention for EDH progression.
Limitations
The study’s single geographic area may limit the generalizability of the findings. Additionally, our dataset lacked certain key features, such as the time between injury and the first CT scan, which have been shown in previous studies to significantly impact EDH expansion. Future studies should include a larger, more diverse population and incorporate these variables to enhance the model’s predictive power.
Conclusion
The study identified key predictive factors for EDH volume changes in TBI patients and demonstrates the feasibility of using a ML model to aid in predicting these changes. The findings emphasize the role of early and repeated imaging in managing TBI and the potential of ML in enhancing patient care. This approach can assist clinicians in making more informed decisions regarding the management of patients with EDH, potentially improving outcomes in TBI cases.
Supplemental Material
Supplemental Material - Predicting epidural hematoma expansion in traumatic brain injury: A machine learning approach
Supplemental Material for Predicting epidural hematoma expansion in traumatic brain injury: A machine learning approach by Mohammad Hasanpour, Danial Elyassirad, Benyamin Gheiji, Mahsa Vatanparast, Ehsan Keykhosravi, Mehdi Shafiei, Shirin Daneshkhah, Arya Fayyazi, and Shahriar Faghani in The Neuroradiology Journal.
Footnotes
Declaration of conflicting interests
The authors declare that the article content was composed in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Ethical statement
AI assistant tools
In this article, ChatGPT-4 was employed to assess grammar and enhance the textual content. Subsequently, the authors thoroughly examined and edited the content as required, assuming complete responsibility for its accuracy and quality.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.