
Abstract
Arteriovenous malformations (AVMs) are abnormal connections of arteries and veins without intermediate capillary components. As such, AVMs can remain asymptomatic or have a variety of clinical presentations ranging from mild headaches to severe symptoms like seizures, hemorrhage, and subsequent coma. Papilledema and increased intracranial pressure without hydrocephalus or hemorrhage are rare forms of presentations of cerebral AVM. The mechanism of intracranial hypertension accompanying brain AVMs is not entirely understood, and the right treatment strategy is controversial. Here, we present the treatment and outcomes of four patients with unruptured AVMs who presented with intracranial hypertension accompanied by visual symptoms, papilledema, and without evidence of hydrocephalus. In cases of AVMs accompanied by intracranial hypertension, AVM treatment should be considered the main target of management.
Introduction
Although frequently asymptomatic, arteriovenous malformations (AVMs) may present with a broad variety of symptoms ranging from nonspecific headaches to intracerebral hemorrhage resulting in severe neurologic deficits. 1 Increased intracranial pressure, as a result of hemorrhage and hydrocephalus, is a common presentation of such malformations. However, clinical manifestation with papilledema in the absence of cerebral hemorrhage and hydrocephalus, similar to benign intracranial hypertension, is very rare. No definitive etiology has ever been reported for this kind of presentation and the suggested treatment strategies include medical therapy, CSF diversion shunts, or endovascular embolization and/or surgical resection of the lesion.1–3 In this article, we present four patients with visual presentations and symptoms of increased intracranial pressure who underwent endovascular treatment and provide a literature review of previous case.
Case series
Case 1
A 35-year-old male presented with intermittent headaches and blurred vision. On ophthalmologic examination, he had bilateral Papilledema. Computed Tomography (CT) 4 and Magnetic Resonance Imaging (MRI) revealed an arteriovenous malformation (AVM) in the left frontal lobe without evidence of bleeding and venous thrombosis. Subsequent Digital Subtraction Angiography (DSA) showed a small AVM with a compact high-flow nidus in the left frontal lobe fed by multiple branches from the left anterior cerebral artery (ACA) and middle cerebral artery (MCA). The AVM drained through four dilated and tortuous cortical veins into superior sagittal sinus as well as into the straight sinus (Grade 3 Spetzler–Martin). A diagnostic lumbar puncture revealed an opening pressure of 38 cm H2O. The patient had no predisposing factors for intracranial hypertension. Based on these findings, the embolization of the AVM was considered treatment option. Complete occlusion of the nidus using Onyx glue was achieved in one session. One-week post intervention, the patient reported significant improvement of headache and blurred vision and intracranial pressure was 28 cm H2O with lumbar puncture assessment. At the 1-month follow-up, bilateral pupil edema disappeared and intracranial pressure was 21 cm H2O.
Case 2
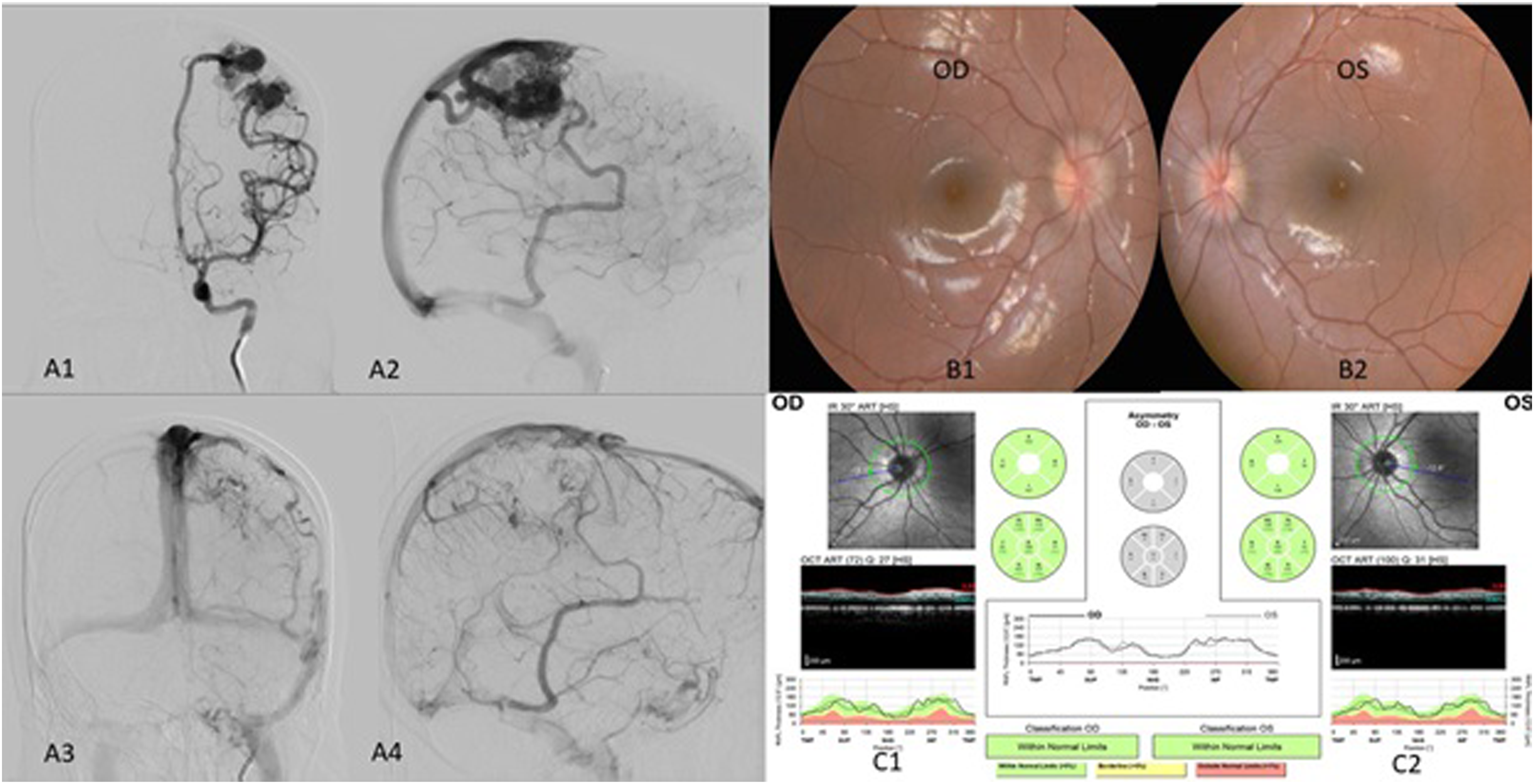
A 15-year-old female patient was referred to our center with a history of headache, bilateral orbital pain, intermittent blurred vision, and right hand tingling. A brain MRI revealed multiple superficial flow voids in the left parietal lobe just posterior to the hand-area on the motor cortex. A DSA showed a large high-flow nidus AVM involving two compartments that were fed by the left MCA and ACA. It also contained two large intranidal aneurysms and had multiple draining veins to the superior sagittal sinus (SSS) and the left transverse-sigmoid sinus junction (Grade 3 Spetzler–Martin). Due to the bilateral papilledema and visual disturbance on ophthalmic exam, a lumbar puncture was performed and showed a pressure of 33 cm H2O. Three days after admission, complete endovascular embolization of the AVM could be achieved at one session. The patient’s symptoms improved and intracranial pressure decreased to 27 cm H2O after 1 week. At the 1-month follow-up examination, the bilateral papilledema was resolved and the intracranial pressure was 19 cm H2O.
Case 3
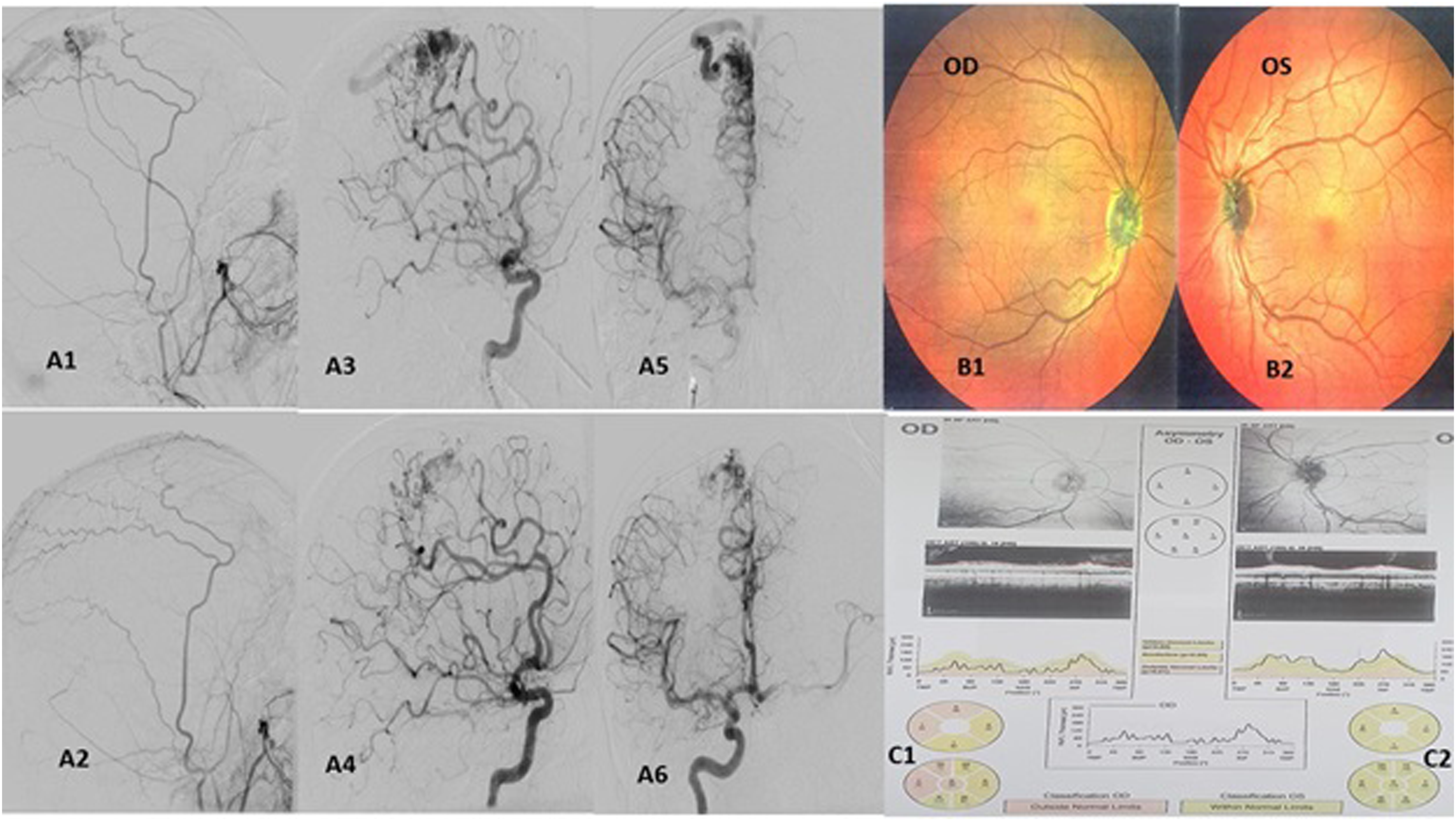
A 39-year-old male patient presented with history of headache, intermittently blurred vision, and progressive visual acuity decrease in the right eye (best corrected visual acuity: 20/40). An ophthalmic examination showed right optic nerve atrophy and a normal left eye. A brain MRI revealed flow voids in the right posterior frontal lobe in close proximity to the leg motor cortex. A DSA showed an AVM nidus at the medial posterior of superior frontal gyrus, fed by multiple branches derived from the right ACA as well as right external carotid artery via the right middle meningeal artery. The AVM drained via cortical veins into the SSS (Grade 3 Spetzler–Martin). A lumbar puncture revealed an opening pressure of 31 cm H2O. Because of the proximity of the AVM nidus to the motor cortex and en-passage feeder to the motor cortex, a partial AVM embolization with Onyx was performed and observation was considered. Lumbar CSF pressure decreased to 29 cm H2O after 1 week and azetazolamide 250 mg was prescribed to treat the headaches and elevated ICP. After 1 month, the lumbar puncture showed that pressure decrease to 27 cm H2O. Two months later, the lumbar puncture rose to 30 cm H2O and the patient complained about headaches and azetazolamide intolerance. Another stage of embolization was considered for this patient. At second stage, near complete occlusion of the AVM nidus with preservation of en-passage artery could be achieved. The patient experienced no new neurological deficit and the headaches resolved. A subsequent lumbar puncture showed that the pressure normalized to 24 cm H2O without medication. For complete occlusion, additional radiotherapy was performed. At the 6-month follow-up, bilateral papilledema disappeared and intracranial pressure was decreased.
Case 4
A 38-year-old female presented with history of chronic headaches and intermittent blurred vision that recently worsened with progressive visual disturbance and a right side visual field defect (right nasal quadrianopia). The fundoscopic examination showed bilateral optic disc edema. A brain MRI revealed flow voids in the right occipito-parietal region suspicious of an AVM nidus. The patient refused lumbar puncture for pressure measurement. A DSA showed a large high-flow AVM nidus fed by right MCA and posterior communicating artery (PCA) branches. The AVM had multiple draining veins into SSS and transverse-sigmoid junction (Grade 3 Spetzler–Martin). A near complete Onyx occlusion could be achieved in one session. The headache and visual disturbance improved and bilateral papilledema had resolved at the 1-month follow-up examination.
Discussion
In rare cases, unruptured AVMs can present with visual symptoms that are clinically and radiologically compatible with intracranial hypertension.1–3 Although the definition of benign intracranial hypertension may not be correct in the presence of cerebrovascular lesions, a coexistence of these two processes is possible.1,2 Abnormal drainage of cortical veins due to arterialization may be the underlying mechanism. A subsequent high pulse pressure in the subarachnoid space leads to increased cerebral pressure without affecting CSF resorption or cerebral blood volume.2,3,5 The prompt treatment response in our patient population supports this hypothesis.
Literature review and treatment strategies
Summary of recent studies concerning intracranial hypertension and papilledema secondary to cerebral AVM in the worldwide.
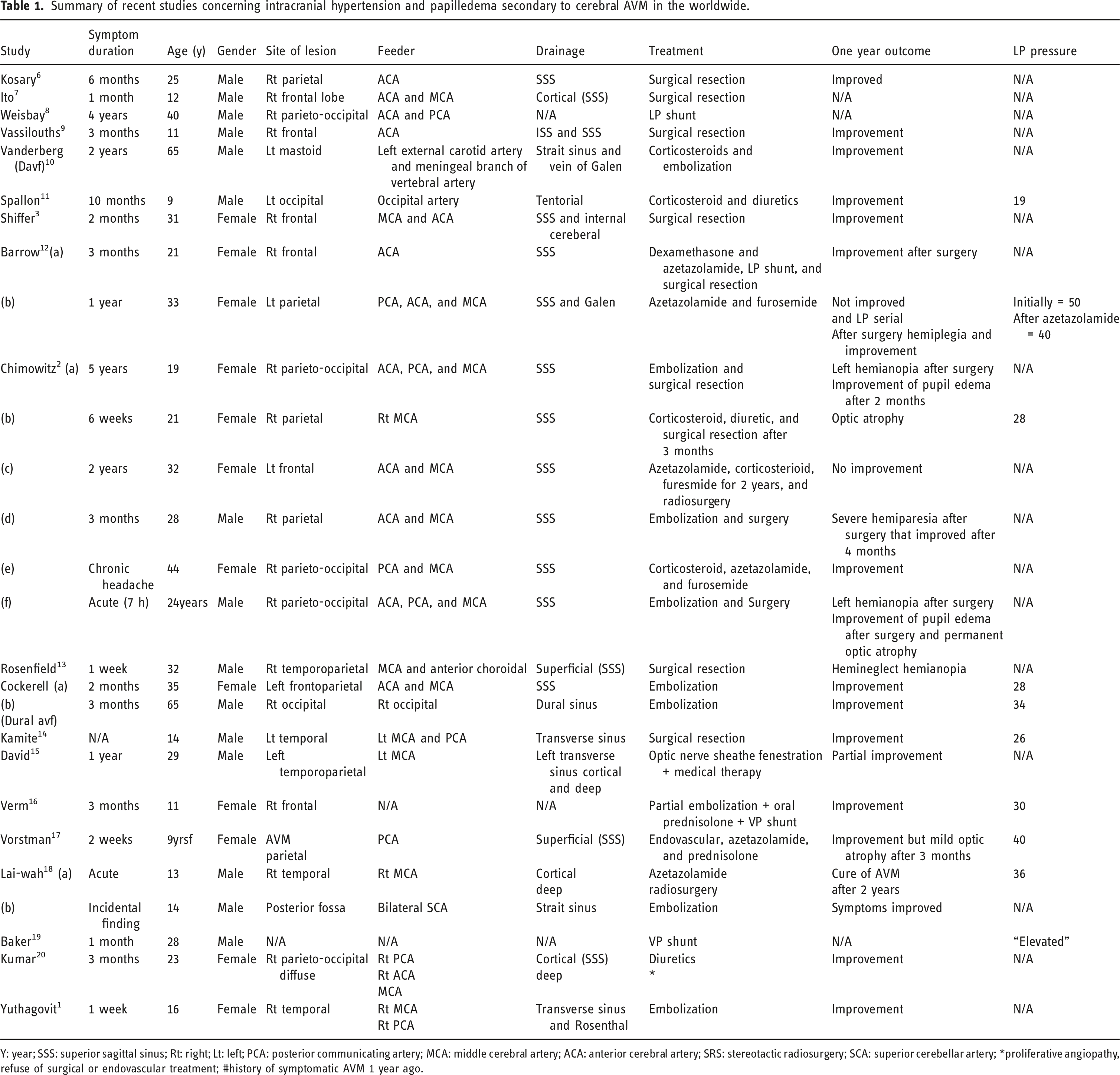
Y: year; SSS: superior sagittal sinus; Rt: right; Lt: left; PCA: posterior communicating artery; MCA: middle cerebral artery; ACA: anterior cerebral artery; SRS: stereotactic radiosurgery; SCA: superior cerebellar artery; *proliferative angiopathy, refuse of surgical or endovascular treatment; #history of symptomatic AVM 1 year ago.
Overall, three case reports described good response to medical treatment while six cases required additional surgical intervention including CSF diversion, optic nerve sheath fenestration, or surgical resection of the AVM.2,12,15,21 The outcome after CSF diversion was superior to medical treatment, but one patient required surgical resection of the AVM despite good functional CSF diversion. However, despite well controlled ICP, severe optic atrophy was associated with poor visual outcomes. 12
Surgical resection of the lesion
The majority of reported surgical treatments in patients with intracranial hypertension and an unruptured AVM were reported before the advent of curative endovascular AVM treatment.3,6,7,9,13,14
Endovascular treatment
Due to recent technologic advances, endovascular therapy may be used as the first line treatment in certain cases. The important point for this method is the selection of partial or complete vascular lesion treatment. Although partial embolization sufficiently treats intracranial hypertension in some cases, supplementary treatments, surgical resection, or radiosurgery are required in other cases Optionally, initial endovascular treatment can be used for pre-operative embolization. 2
Based on these findings, we chose to recommend endovascular embolization as the option if feasible. Response to the endovascular treatment was fast and effective in our case series. Clinical improvement could be observed as early as the first postoperative day. After 1 week, the opening pressure on lumbar puncture was significantly reduced, indicating a decreased ICP.
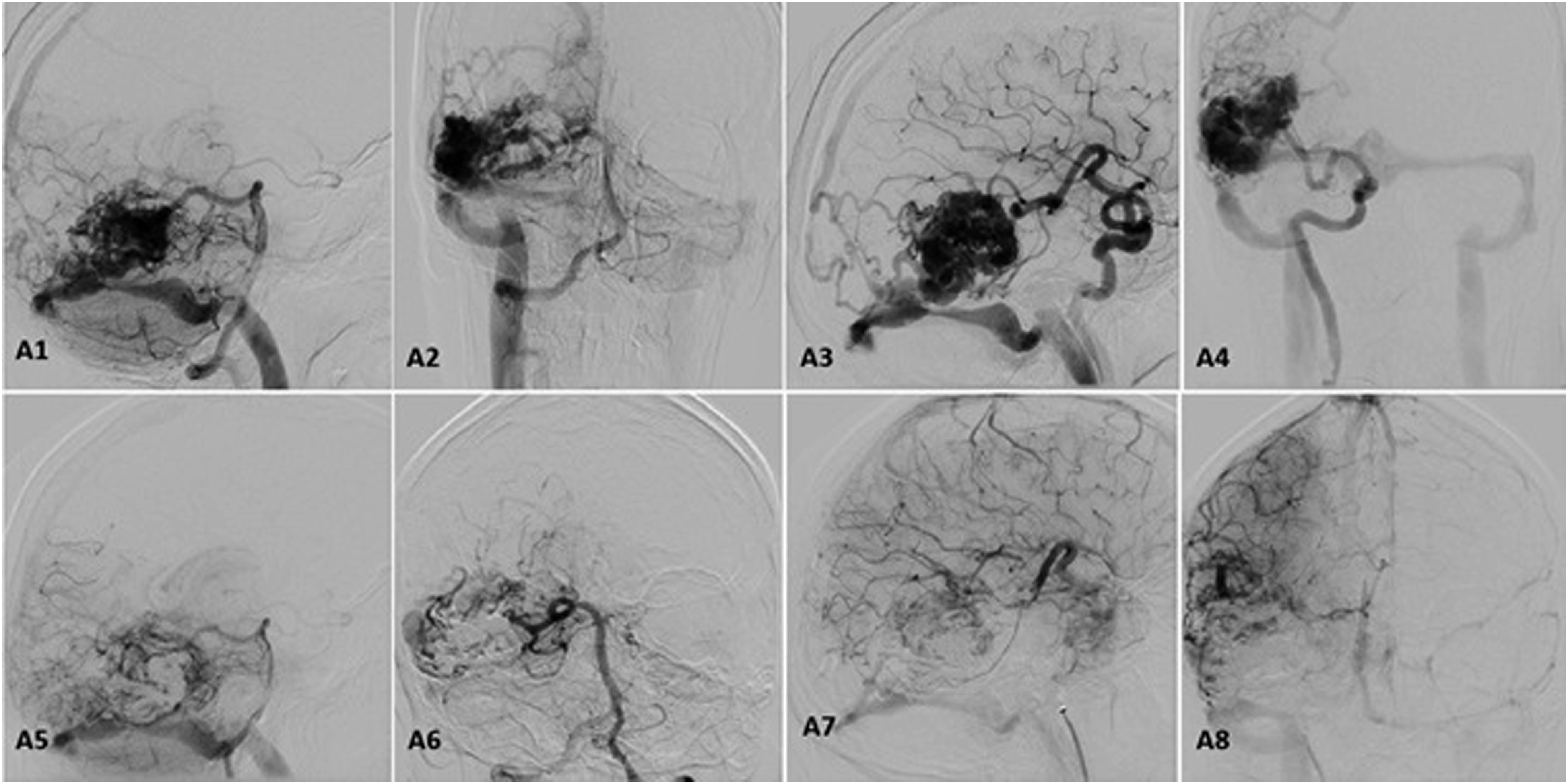
In cases with complete AVM embolization, the outcome was excellent and did not require the adjustment of long-term medical treatment. Partial embolization was associated with partial resolution of symptomatology (Figures 1–4). {Case1}: A1 left ICA lateral view pre-embolization, A2 left ICA AP view pre-embolization, A3 left ICA Lateral view post-embolization, A4 left ICA AP view post-embolization, B1 right eye papilledema pre-embolization, B2 left eye papilledema pre-embolization, B3 right eye resolved papilledema 1-month post-embolization, B4 left eye resolved papilledema 1 month post-embolization, C1 right eye OCT 1-month post-embolization, and C2 left eye OCT 1-month post-embolization. {Case2}: A1 left ICA AP view pre-embolization, A2 left ICA lateral view pre-embolization, A3 left ICA AP view post-embolization, A4 left ICA Lateral view post-embolization, B1 right eye papilledema pre-embolization, B2 left eye papilledema pre-embolization, C1 right eye OCT resolved papilledema 1-month post-embolization, and C2 left eye OCT resolved papilledema 1-month post-embolization. {Case 3}: A1 right ECA lateral view pre-embolization, A2 right ECA lateral view post-embolization, A3 right ICA lateral view pre-embolization, A4 right ICA lateral view post-embolization, A5 right ICA AP view pre-embolization, A6 right ICA AP view post-embolization, B1 right eye optic atrophy pre-embolization, B2 left eye normal pre-embolization, C1 right eye OCT 1-month partial optic atrophy post-embolization, and C2 left eye OCT 1-month normal papilla post-embolization. {Case 4}: A1 right VA lateral view pre-embolization, A2 right VA AP view pre-embolization, A3 right ICA lateral view pre-embolization, A4 right ICA AP view pre-embolization, A5 right VA lateral view post-embolization, A6 right VA AP view post-embolization, A7 right ICA lateral view post-embolization, and A8 right ICA AP view post-embolization.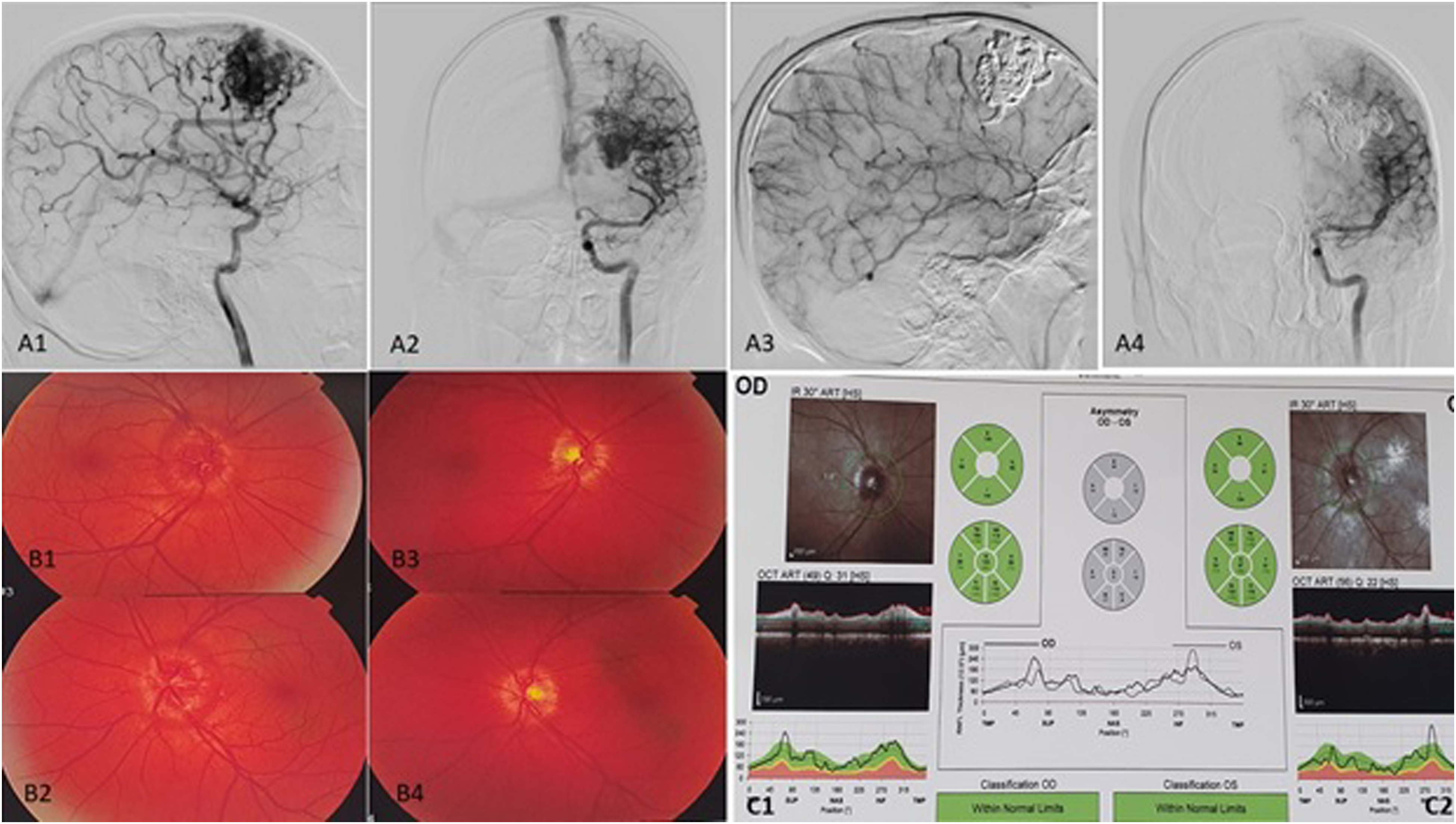
Conclusion
Our case series as well as a review of the literature indicated that intracranial hypertension might occur as a sequel of an unruptured supratentorial AVM. Increased ICP and papilledema without hydrocephalus may therefore be an indication for AVM treatment. Any delay in the treatment of such lesions may result in irreversible damages to the optic nerve. In these patients, endovascular treatment can be used safely as primary treatment if complete or near complete AVM occlusion can be achieved. However, if complete endovascular occlusion is not possible, complementary radiosurgery or primary surgical resection might be required.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.