
Abstract
Introduction
Platelet function testing using serial VerifyNow P2Y12 platelet reactivity units (PRUs) is established for guiding clopidogrel antiplatelet therapy in cerebral aneurysm stenting procedures. However, for ticagrelor, the impact of serial PRU testing and the identification of safe PRU ranges remains unexplored.
Methods
Flow diversion stenting (n = 232) and stent-assisted coiling procedures (n = 83) performed 05/2017–12/2021 were reviewed. Out of these, 31 flow diversion and 18 stent-coiling procedures were performed on 44 patients using ticagrelor. Baseline demographics, ticagrelor PRUs, and clinical outcomes were assessed.
Results
Collectively, 257 ticagrelor P2Y12 PRUs were obtained. PRUs were <100 in 192/257 (74.7%) tests. Only 11/257 (4.3%) PRUs were >200. The overall median ticagrelor PRU was 38 (IQR 11–101). Among the 49 procedures, median PRUs before the procedure (25, IQR 10–67), on the day of the procedure (68, IQR 44–117), and on the day after the procedure (37, IQR 21–79) did not show the significant differences between the groups. A total of seven thromboembolic complications occurred. Median PRUs surrounding the thromboembolic complications (median 182, IQR 148–235) were significantly higher than preprocedural (p < .001), day of surgery (p < .01), and postprocedural PRUs (p < .01). All seven procedures harbored demographic, anatomic, or procedural features increasing the risk for thromboembolic complications.
Discussion
The majority of periprocedural ticagrelor PRUs were <100. PRUs at the time point of thromboembolic complications were >120. Despite procedure-complicating features in each thromboembolic case, it raises the question whether safe ticagrelor PRU levels might be lower than those commonly applied for clopidogrel.
Introduction
Dual antipatelet therapy (DAPT) with aspirin and clopidogrel represents the most common antithrombotic regimen for patients undergoing intracranial stenting procedures such as stent-assisted coiling and flow diversion stenting.1,2 Guided antiplatelet therapy with platelet function testing has been shown to reduce thromboembolic complications due to identification of clopidogrel hypo- and non-responders. 3 Platelet function testing using VerifyNow™ quantifies P2Y12 platelet reactivity units (PRUs). Traditionally, platelet inhibition with clopidogrel was considered sufficient with PRUs <230s but post-hoc analyses lead to more conservative upper PRU limits. Per manufacturer, PRU levels among patients without antithrombotic medication range between 182 and 335. Therefore, conservative upper PRU levels for patients with platelet inhibitors are as low as 182. Additionally, intracranial stenting procedures may be safer with tighter than usual PRU ranges although study findings remain inconsistent.4–11 The choice of P2Y12 inhibition medication and monitoring through platelet function testing varies considerably among U.S. centers.12,13 Ticagrelor has emerged as a valuable alternative to clopidogrel since it should render further platelet function testing dispensable. Only a few cases of ticagrelor hypo- or non-response have been reported among patients undergoing flow diversion for cerebral aneurysms.14–16 We previously reported a case series of flow diversion and stent-assisted coiling procedures performed under ticagrelor in which serial VerifyNow P2Y12 PRUs were obtained. We raised the question whether safe ticagrelor PRUs might differ from safe clopidogrel PRUs. 17 Here, we seek to extend our institutional experience with ticagrelor and explore the association of ticagrelor PRU values and complications surrounding cerebral aneurysm stenting procedures.
Methods
This retrospective study was approved by the local institutional review board (#2022-0160). Consecutive cerebral aneurysm patients treated between May 2017 and December 2021 at two North American academic centers part of the same healthcare system were reviewed from a prospectively maintained case database. In the study period, a total of 232 flow diversion stenting (FDS) and 83 stent-assisted coiling (SAC) procedures were identified. We identified 49 procedures (31 FDS, 18 SAC) in which patients were on periprocedural ticagrelor as P2Y12 inhibitor (Figure 1). Chart review of patients undergoing cerebral aneurysm treatment with intracranial stenting for stent-assisted coiling (SAC) or flow diversion stenting (FDS) was performed. The treatment period consists of the preprocedural phase with dual antiplatelet therapy initiation up to 30 days before the treatment and up until 6 months post-procedure. The preprocedural time period was counted as the day 1 to 30 prior to the procedure day (displayed as negative count −30 to −1 in Figure 2). The day of the procedure was displayed as day 0. The postprocedural period was counted as day 1 to day 180 after the procedure date. Baseline demographics, aneurysm characteristics, treatment variables, antithrombotic regimen, complications, and outcome at 6 months after stenting were reviewed. Routinely, elective patients were initiated on aspirin 325 mg/d and clopidogrel 75 mg/d with follow-up platelet function testing according to the institutional pharmacy-mediated antiplatelet management protocol. VerifyNow P2Y12 platelet reactivity unit (PRU) testing per manufacturer manual was performed 1 week after clopidogrel initiation, on the day of procedure, on day one after the procedure, and then 1 week, 1 month, and 3 months after the procedure. In case dose adjustments are required, additional testing is performed. Clopidogrel P2Y12 platelet reactivity units (PRUs) in a range of 60–210 were considered therapeutic during the study period.
6
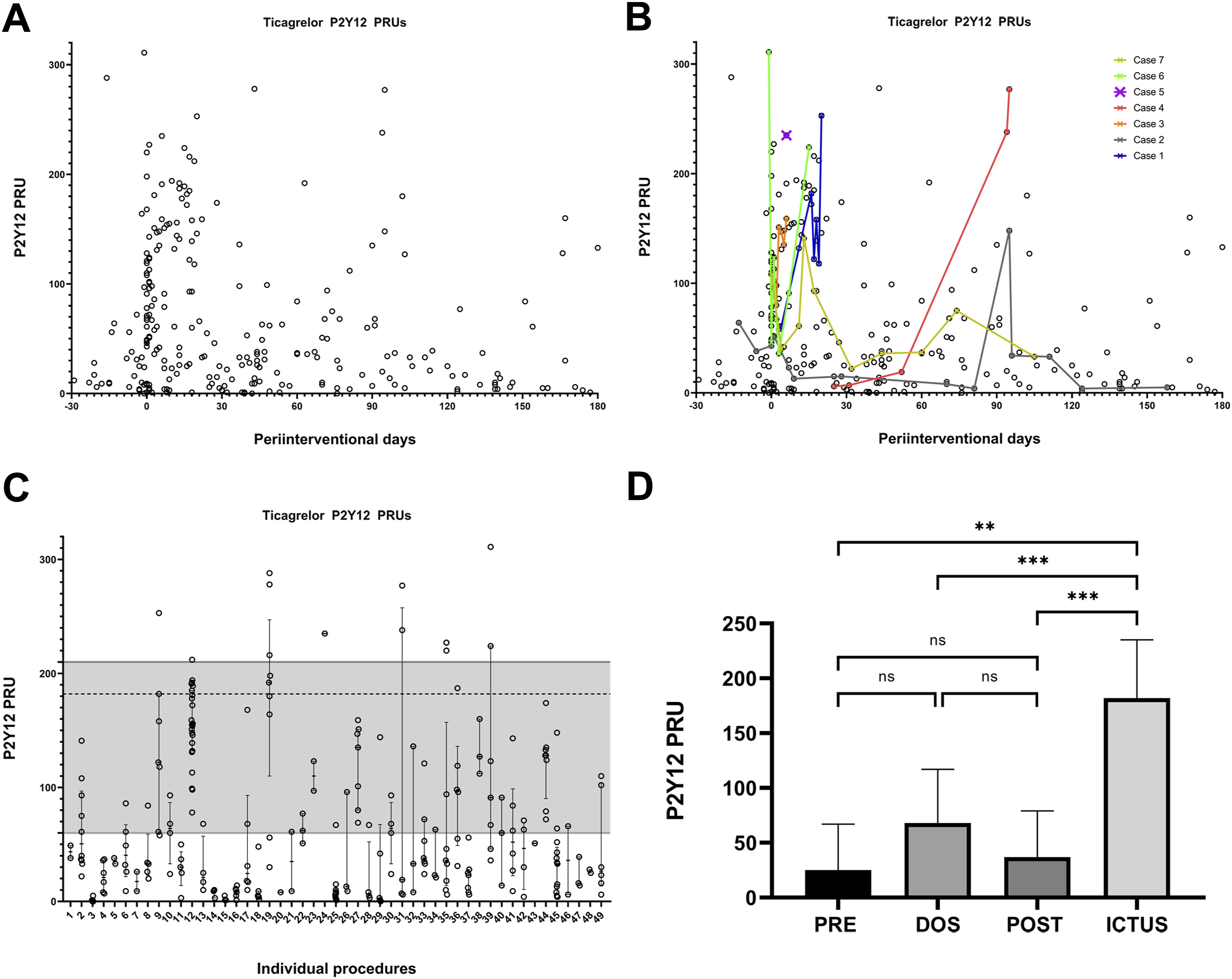
Patients were considered clopidogrel hyper-responders when the standard dose of 75 mg daily induced PRUs <60 and subsequent clopidogrel dose reduction was required. Patients were considered clopidogrel hypo-responders requiring transitioning to ticagrelor when clopidogrel loading doses of 300–600 mg and a daily 150 mg dose did not induce PRUs <210. Based on physician discretion, a subset of patients was initiated on aspirin and ticagrelor. Other patients were switched to ticagrelor because clopidogrel dose adjustments did not facilitate constant achievement of target PRUs 60–210.18,19 Platelet function testing intervals and protocol deviations based upon physician discretion with respect to case individual criteria. Thromboembolic complications were defined as all clinically apparent ischemic complications that were associated with the intracranial stent placement including stent occlusion, subocclusive in-stent thrombosis, and thromboembolism in the stent’s respective vascular territory. Decision on medical management with or without neurointervention was based on the imaging findings (CTA, MRI, and DCA) and stroke severity. Ictus PRUs were obtained in the acute setting prior administration of additional antithrombotic medications. Intracranial hemorrhage was defined as any CT or magnetic resonance imaging positive for intracranial hemorrhage. Extracranial hemorrhagic complications were defined as all bleeding complications that required medical attention, hospitalization, or intervention. Flow diagram representing studied cohort. (a) Individual ticagrelor P2Y12 PRUs obtained in the periprocedural phase. (b) In seven cases, thromboembolic complications occurred and the corresponding PRUs are colored. The case counts correspond to the details in Table 2. (c) Ticagrelor P2Y12 PRU values obtained per procedure. The therapeutic PRU 60–210 window is colored gray. The dotted line at PRU 182 indicates the upper threshold for conservative PRU limits. (d) Comparison of ticagrelor P2Y12 PRU values obtained in the preprocedural, day of surgery, and postprocedural phase and compared to values obtained on day of thromboembolic complication. PRE versus DOS (p = .058), PRE versus POST (p = .218), DOS versus POST (p = .068), PRE versus ICTUS (p = .001), DOS versus ICTUS (p < .001), and POST versus ICTUS (p < .001).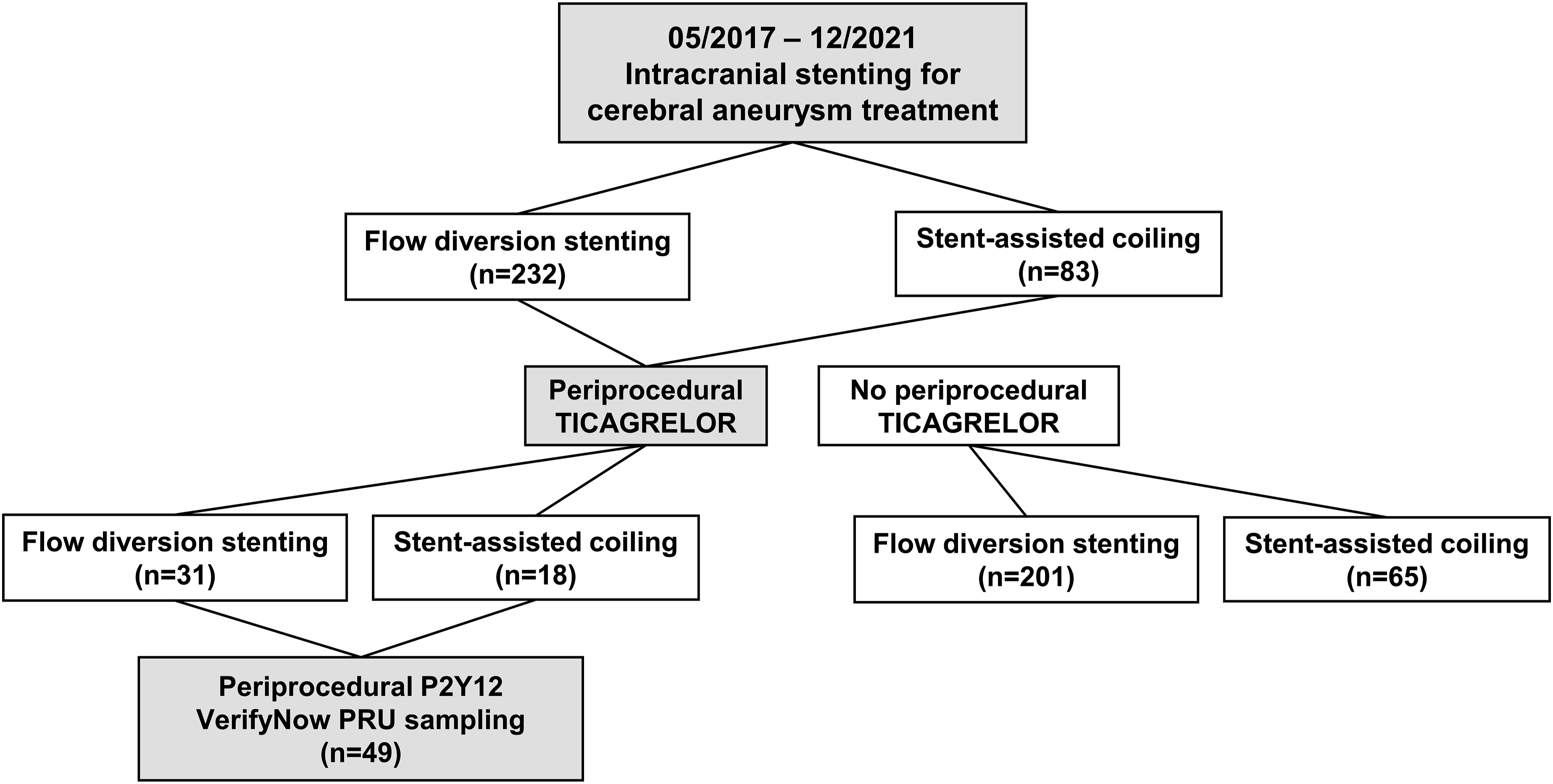
Statistical analysis
Categorical variables are stated as frequency and percent. Continuous variables are presented as the median and interquartile range (IQR). Number of PRU tests per individual and time point differed throughout the study period. Therefore, Mann-Whitney U test was used to compare PRU values for the preprocedural, day of procedure, and postprocedural phase. p-values of <0.05 were considered statistically significant. IBM SPSS version 25 and GraphPAD Prism 8 were used for analysis.
Results
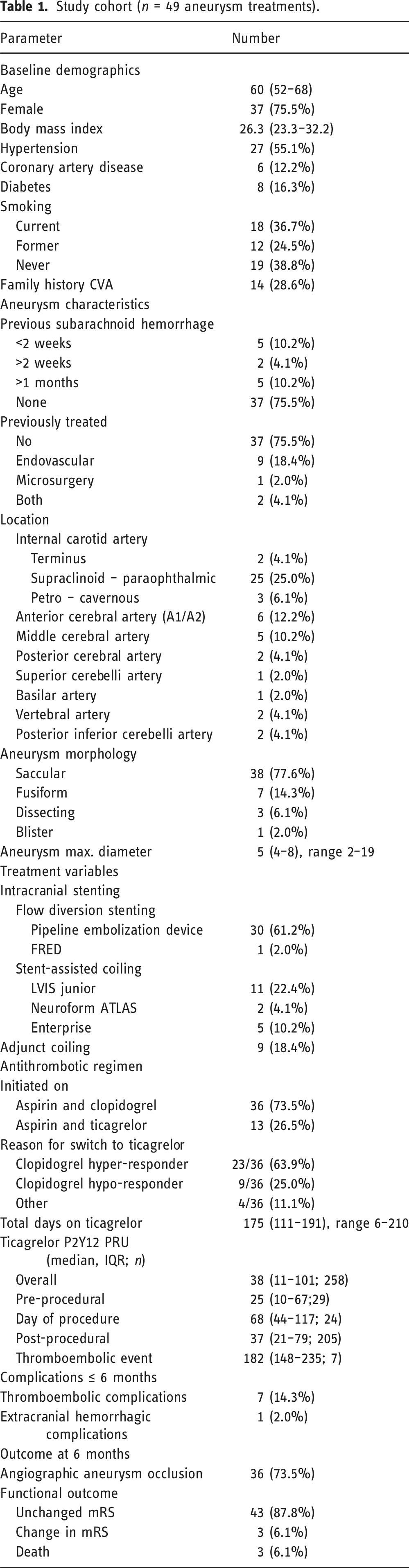
Study cohort (n = 49 aneurysm treatments).
Ticagrelor PRUs
Overall, the median length of ticagrelor intake per case was 175 days (IQR 111–191), with a range of 6 to 210 days. A total of 257 ticagrelor P2Y12 PRUs were obtained (Table 1, Figure 2(a)) and 148/257 (57.6%) PRUs were <60, 192/257 (74.7%) PRUs were <100, and 237/257 (92.2%) PRUs were <182. Only 11/257 (4.3%) PRUs were >200. The overall median ticagrelor PRU was 38 (IQR 11–101). In 7 cases, thromboembolic complications occurred and individual P2Y12 PRUs are highlighted in Figure 2(b) for each case. Individual PRU ranges per case are depicted in Figure 2(c). Median PRUs prior to the procedure (25, IQR 10–67), on day of the procedure (68, IQR 44–117), and the day after the procedure (37, IQR 21–79) were similar (p = .058–0.218) (Figure 2(d)) but significantly lower compared to those PRUs on day of thromboembolic complication (p < .01–p < .001) (Figure 2(d)). Eight individuals had at least one individual PRU ≥182 (Figure 2(b)).
Complications
Specifics of patients who suffered complications.
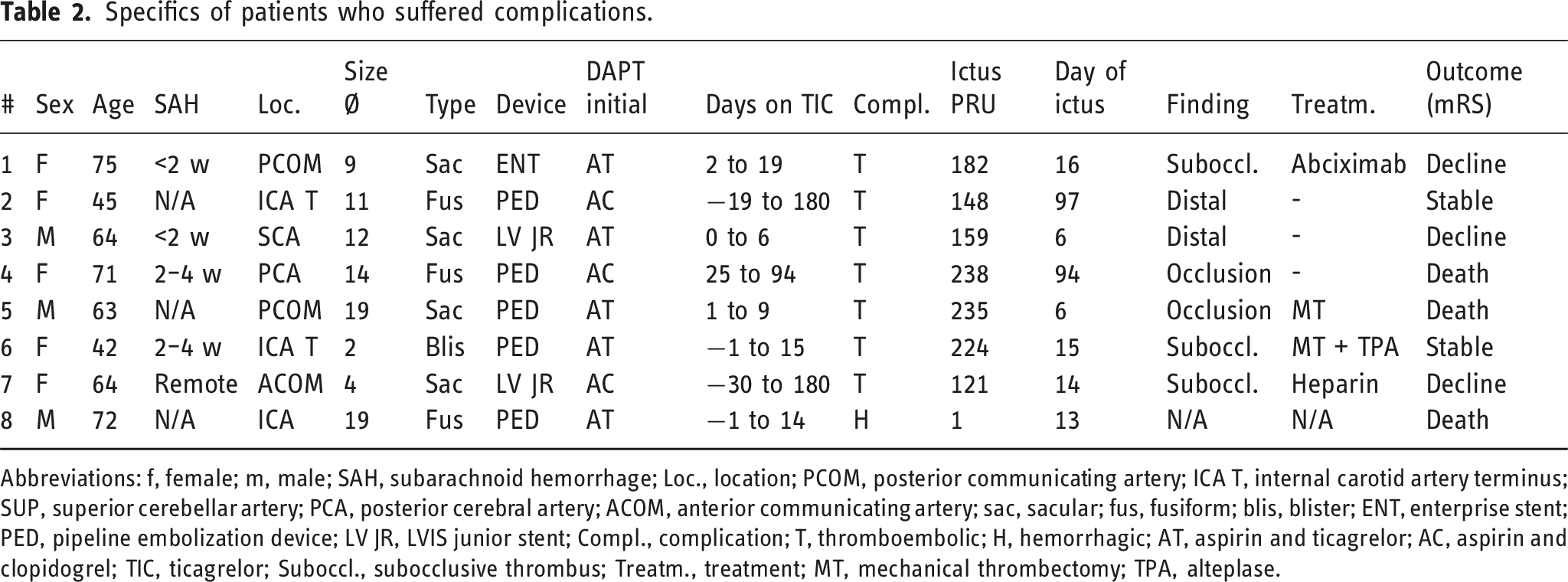
Abbreviations: f, female; m, male; SAH, subarachnoid hemorrhage; Loc., location; PCOM, posterior communicating artery; ICA T, internal carotid artery terminus; SUP, superior cerebellar artery; PCA, posterior cerebral artery; ACOM, anterior communicating artery; sac, sacular; fus, fusiform; blis, blister; ENT, enterprise stent; PED, pipeline embolization device; LV JR, LVIS junior stent; Compl., complication; T, thromboembolic; H, hemorrhagic; AT, aspirin and ticagrelor; AC, aspirin and clopidogrel; TIC, ticagrelor; Suboccl., subocclusive thrombus; Treatm., treatment; MT, mechanical thrombectomy; TPA, alteplase.
Discussion
The key finding of this study was that in all seven patients with thromboembolic events, PRUs on day of ictus were significantly increased compared to the average periprocedural PRUs obtained in the entire cohort. While more than 90% of all obtained ticagrelor PRUs were <100, all seven patients with a thromboembolic complication had a PRU >120 on the day of ictus. Notably, in four of these seven patients, PRUs on day of ictus were ≤182 which per manufacturer is generally considered therapeutic. However, to date, PRU target ranges are established for the P2Y12 inhibitor clopidogrel but not ticagrelor. This raises the question whether therapeutic PRU ranges differ between clopidogrel and ticagrelor. Importantly, in this case series, all seven procedures harbored distinct complicating features that could have contributed to the risk of ischemic complications outside insufficient platelet inhibition.
To date, only few studies have reported serial VerifyNow P2Y12 platelet reactivity units in cerebral aneurysm patients treated with ticagrelor surrounding stent-assisted coiling or flow diversion stenting. DeGrote et al. reported 29 patients who received ticagrelor and aspirin after Pipeline Embolization Device placement. In their hands, no patient suffered from thromboembolic nor hemorrhagic complications within 6 months. A total of 61 ticagrelor PRUs were obtained in 28 patients. Median PRU was 53 (IQR 15–84) and 78.7% of PRUs were <100. The ticagrelor PRU values were similar to our observations. 20 However, the baseline demographics of their cohort were fundamentally different in terms of risk factors for ischemic complications with flow diversion stenting.21–24 In recent analyses, ticagrelor performed equally safe and effective when compared to clopidogrel surrounding flow diversion procedures.25–27 Overall, ticagrelor hypo- or non-response among patients undergoing intracranial stenting procedures for cerebral aneurysms is rarely reported.14–16 Associating elevated ticagrelor PRUs to clinical events remains controversial. The dose and timing of last P2Y12 inhibitor intake to testing is a critical determinant of the PRU value obtained. 28 Additionally, per manufacturer, GP IIb/IIIa inhibitors interfere with VerifyNow P2Y12 PRUs, which might be overlooked by the neurointerventionalist who intraprocedurally administers bridging agents such as eptifibatide, tirofiban, or abciximab. 29 While studies support the notion that PRU-driven clopidogrel treatment is beneficial surrounding flow diversion stenting, 8 other authors report the contrary. Particularly, determinants of procedural complexity such as longer fluoroscopy time, adjunctive coiling, and post-stent balloon angioplasty were identified as predictors of thromboembolic complications.4,9,10 In the presented study, each of the seven cases with thromboembolic complications also had certain features that increased case complexity and thereby could have been the primary source for the thromboembolic complication outside insufficient platelet inhibition. Since the majority of patients in our system are treated with clopidogrel, the subset of patients presented in this study is subject to selection bias. Patients with higher risk of periprocedural thromboembolic complications and more urgent need of platelet inhibition were more likely to be initiated on ticagrelor by physician discretion. Next, the heterogeneity of treatment related characteristics such as aneurysm size, location, and morphology confounds interpretation of the causality of thromboembolic events. Additionally, the small cohort consisted of patients who underwent flow diversion stenting as well stent-assisted coiling, two procedures that have stenting of the parent vessel in common, but critically differ in metal coverage as well as other procedural aspects. Since the matter of safe ticagrelor PRU ranges is not yet elucidated, further investigation is required to understand whether therapeutic—and with that safe—PRU ranges differ between ticagrelor and clopidogrel.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.