
Abstract
An adult patient was admitted to our emergency department for a first episode of generalized tonic-clonic seizure. Computed tomography scan and magnetic resonance imaging showed a temporal intracranial hemorrhage and parenchymal edema caused by a dural arteriovenous fistula (DAVF), whose angioarchitecture was better understood through the DSA which showed as intriguing and rare vascular anomaly the origin of the posterior inferior cerebellar artery (PICA) from the middle meningeal artery (MMA). The endovascular treatment of the DAVF was then successfully performed.
This case describes the first case of a PICA arising from the MMA in the literature and highlights as an accurate knowledge of vascular anatomy and its variations is essential for the endovascular treatment of the cerebrovascular diseases.
Introduction
The embryologic and phylogenetic development of the cerebral vascular system illustrates a complex network of arterial connections that play a critical role in both normal physiology and clinical interventions. Understanding these connections is especially important in endovascular procedures, where accidental embolic complications can occur if the vascular anatomy is not well known.
The external carotid artery (ECA) primarily supplies the face and neck but also has important collateral connections to the intracranial circulation. These anastomoses typically occur where cranial nerves exit the skull, such as the foramen ovale or foramen spinosum, allowing branches of the ECA to connect to the internal carotid artery (ICA).
One underreported significant aspect of this vascular network is the relationship between the middle meningeal artery (MMA) and the posterior cerebral circulation, that is, the aim of our paper.
Case report
An adult patient presented with a first episode of generalized tonic-clonic seizure. At the admission at the ER, neurological examination revealed aphasia. The EEG showed a non-specific global slowdown in brain activity. CT scan and MRI disclosed parenchymal edema in the temporal lobe with a small subcortical hematoma. CT-angio highlighted an engorgement of the pial veins in the temporal region which raised the suspicion of dural arteriovenous fistula (DAVF). The DSA confirmed and better defined the angioarchitecture of the DAVF.
The DAVF was located in the pterional region (Figure 1(a) and (b)) and was fed by a meningeal branch raising from the pre-bifurcation segment of the left MMA (Figure 1(c)), by transdiploic branches of the left superficial temporal artery (STA) (Figure 1(d)), and by tiny dural feeders from the ipsilateral maxillary artery (MA). The DAVF drained into few temporal veins directed both in the sphenoparietal sinus and into the left basal vein. The petrous branch of the MMA was hypertrophic despite not feeding the DAVF; it coursed over the petrous bone, then downward on the retro mastoid occipital region until entering the subarachnoid space (g) and supporting the posterior inferior aspect of the left cerebellar hemisphere (i.e., PICA territory). Super selective angiograms better demonstrated that the telovelotonsillary segment of the PICA arose from the MMA (Figure 1(e) and (f)). Selective left vertebral artery injection confirmed the agenesis of the PICA and the absence of the left posterior meningeal artery (PMA) (Figure 1(h)). Lateral (a) and frontal (b) angiograms demonstrate the angioarchitectures of the DAVF. The superselective angiogram of the maxillary artery (c) better shows the short dural feeder arising from the MMA (red arrow), the transdiploic feeders from the STA (d), and the point fistula (yellow arrows). Lateral (e) and frontal (f) superselective angiograms of the petrous branch of the MMA disclose the origin of the PICA from the petrous branch. Axial XperCT MIP reconstruction (g) shows the emergence of the PICA from the petrous branch of the MMA. Lateral (h) angiogram of the left vertebral artery shows agenesis of the PICA and the absence of the tributary vascular territory.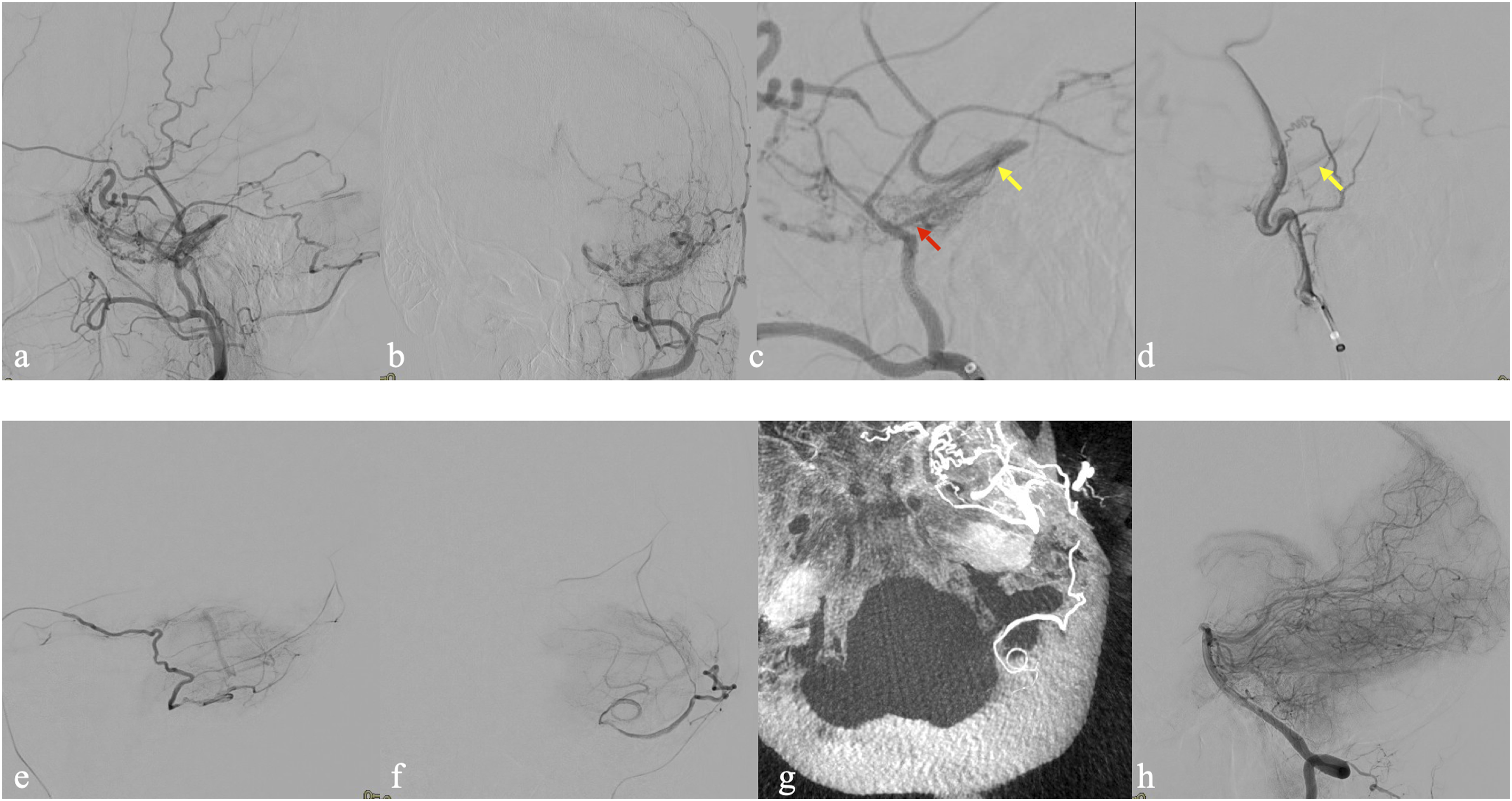
The procedure was performed in general anesthesia. Bilateral femoral approach was performed. Using a right-side triaxial system, an intermediate catheter was advanced into the proximal segment of the STA; an EVOH-compatible microcatheter Headway DUO (Microvention, Tustin, CA, USA) was then delivered into one of the arterial feeders in the proximity of the point of fistula to inject Squid 12 (Balt, Montmorency, France) (Figure 2(a)). A left-side bi-axial system was used to deliver a double-lumen balloon microcatheter Scepter XC (Microvention, Tustin, CA, USA) at the origin of the meningeal feeder arising from the left MMA (Figure 2(b)). The balloon microcatheter was alternatively inflated (not more than 3 minutes per inflation) during the injection of the embolic agent to avoid retrograde reflux and thus preserve the patency of the MMA and the PICA. Two ml of Squid 12 (Balt, Montmorency, France) was injected in 33 minutes to achieve complete occlusion of the DAVF (Figure 2(e) and (f)). The left petrous branch of MMA and the related PICA remained patent at the end of the procedure (Figure 2(f)). Endovascular treatment of the DAVF. An EVOH-compatible microcatheter was delivered into one of the arterial feeders of the STA (yellow arrows) near the point of the fistula in order to inject the EVOH embolic agent (a). Subsequently, a double-lumen balloon microcatheter (red arrows) was positioned at the origin of the meningeal feeder (white arrowheads) arising from the left MMA (b). Frontal and lateral unsubtracted images were obtained prior to the injection of the embolic agent (c), (d). The balloon microcatheter was alternately inflated during the injection of the embolic agent to prevent retrograde reflux and thus preserve the patency of the MMA. The final unsubtracted lateral angiogram (e) shows the cast of the embolic agent and the occlusion of the point of the fistula. The lateral angiogram (f) demonstrates complete occlusion of the DAVF while maintaining the patency of the petrous branch of the MMA and the related PICA.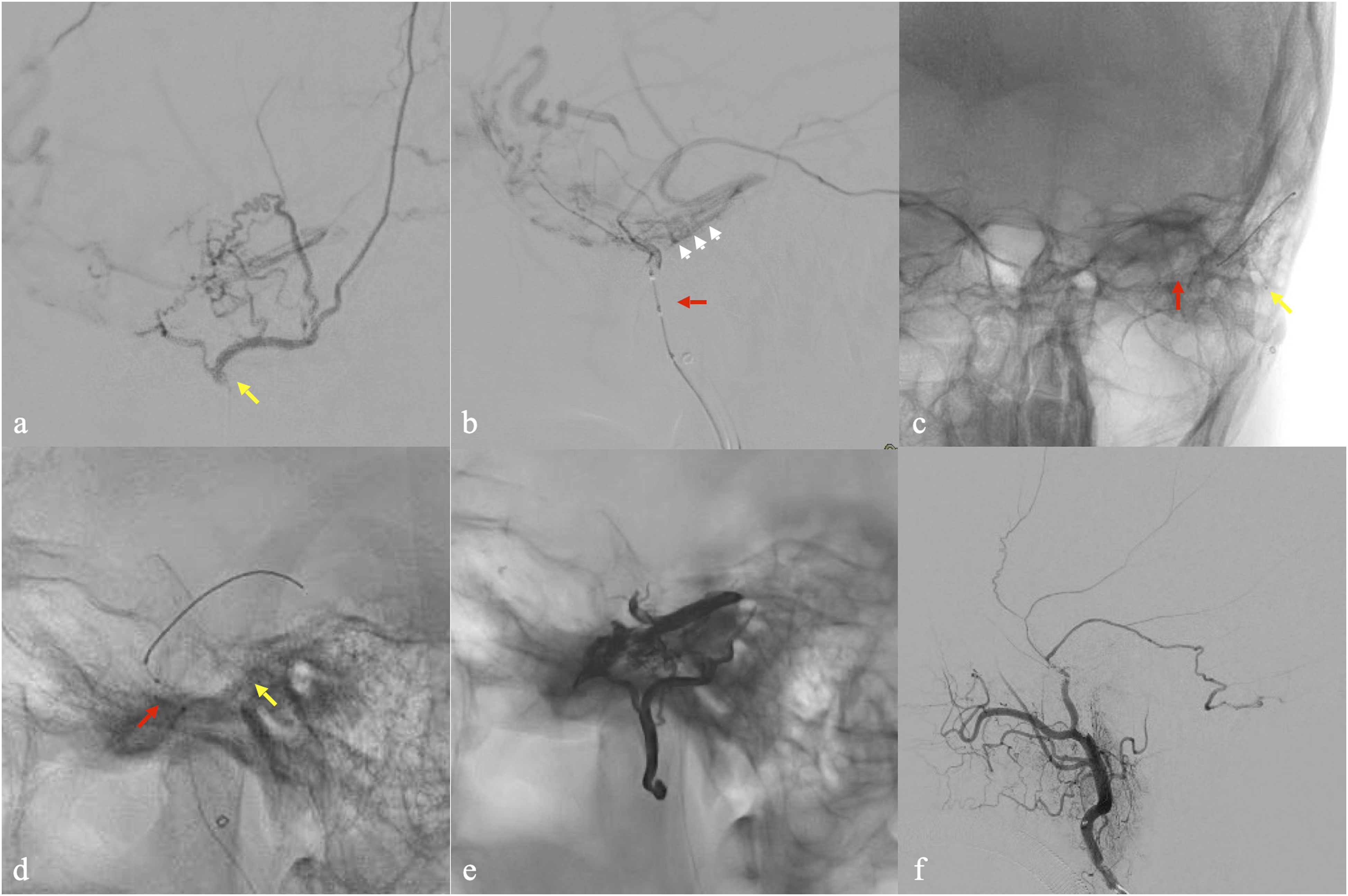
No additional deficit was recorded after the procedure. The CT scan excluded ischemic or hemorrhagic complications. At 3-month FUP the patient completely recovered without any remaining deficit (mRS 0).
Discussion
Cerebral DAVFs are acquired abnormal arteriovenous connections between an arterial feeder and a dural venous sinus or leptomeningeal vein that account for 10%–15% of all intracranial vascular malformations. 1 Endovascular therapy with liquid embolic agents is currently the gold standard for the treatment of these acquired vascular malformations. 2 An accurate DSA is essential to define DAVF angioarchitecture, to plan the more appropriate endovascular strategy and to rule out dangerous anastomosis with the intracranial circulation, in order to avoid unexpected brain ischemic injuries. 3 In our case, the PICA originated from the petrous branch of the MMA. PICA has the most complex and variable course of the cerebellar arteries. Equally, the location of PICA’s origin is highly variable. It can arise extradurally below the foramen magnum, from the basilar artery or more rarely from ECA branches, as the occipital artery. 4 To the best of our knowledge, this is the first case described in the literature of a PICA arising from MMA. On the contrary, the origin of MMA from the posterior circulation has been described, highlighting the intimate relationship between pial and meningeal vessels.5,6 MMA can origin from the basilar artery or from a lateral pontine artery. Two distinct embryologic explanations are postulated by investigators to explain this anatomic variation: it could be the consequence of anastomosis in the gasserian region between the basilar remnant of the trigeminal artery and the persistent stapedial artery. Alternatively, it can originate from an enlarged lateral pontine artery developing during embryologic life and anastomosing with the stapedial artery. 5 One case of MMA originating from the PICA was described from Kuruvilla et al. They postulated that the internal auditory artery might have originated from the PICA during fetal development and possibly its close relationship to stapedial artery during embryogenesis might explain the anomalous origin of the MMA. 6 The PMA is the largest vessel supplying the dura mater of the posterior fossa. It typically arises from the vertebral artery, although other origins have been seen, such as from the ascending pharyngeal artery or from the occipital artery. Tanohata et al. reported two cases of anomalous origin of the PMA from the lateral medullary segment of the PICA. Their explanation for this anomalous origin was the persistence of one of the pre-existing anastomotic channels between the primitive vessels of the future PICA and the future PMA. 7 This close relationship is supported by the case report of Ogawa et al. in which an origin of the PICA from the PMA was described. 8 In our case, a possible explanation could be a pre-existing PICA origin from the PMA, followed by a regression of the first segment of PMA. In this setting, due to the rich anastomoses between dural arteries, the MMA may have taken over the supply of the PMA and PICA territories. This case underlines how the thorough knowledge of intracranial/extracranial connections and an accurate pre-treatment DSA are mandatory to avoid inadvertent embolization of arteries supplying normal brain tissue during endovascular procedures.
Footnotes
Author Contributions
EL: project development, data collection and management, data analysis, and manuscript writing/editing. SS: project development and data collection and management. PT: data analysis and manuscript writing/editing. AP: project development, data collection and management, data analysis, and manuscript writing/editing. VD: project development and data collection and management. FS: project development, data collection and management, and data analysis. LB: project development and data collection and management. AP: project development and manuscript writing/editing. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.